
Men’s Positive and Negative Experiences Following Acute Myocardial Infarction

 ,
, 
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Participants
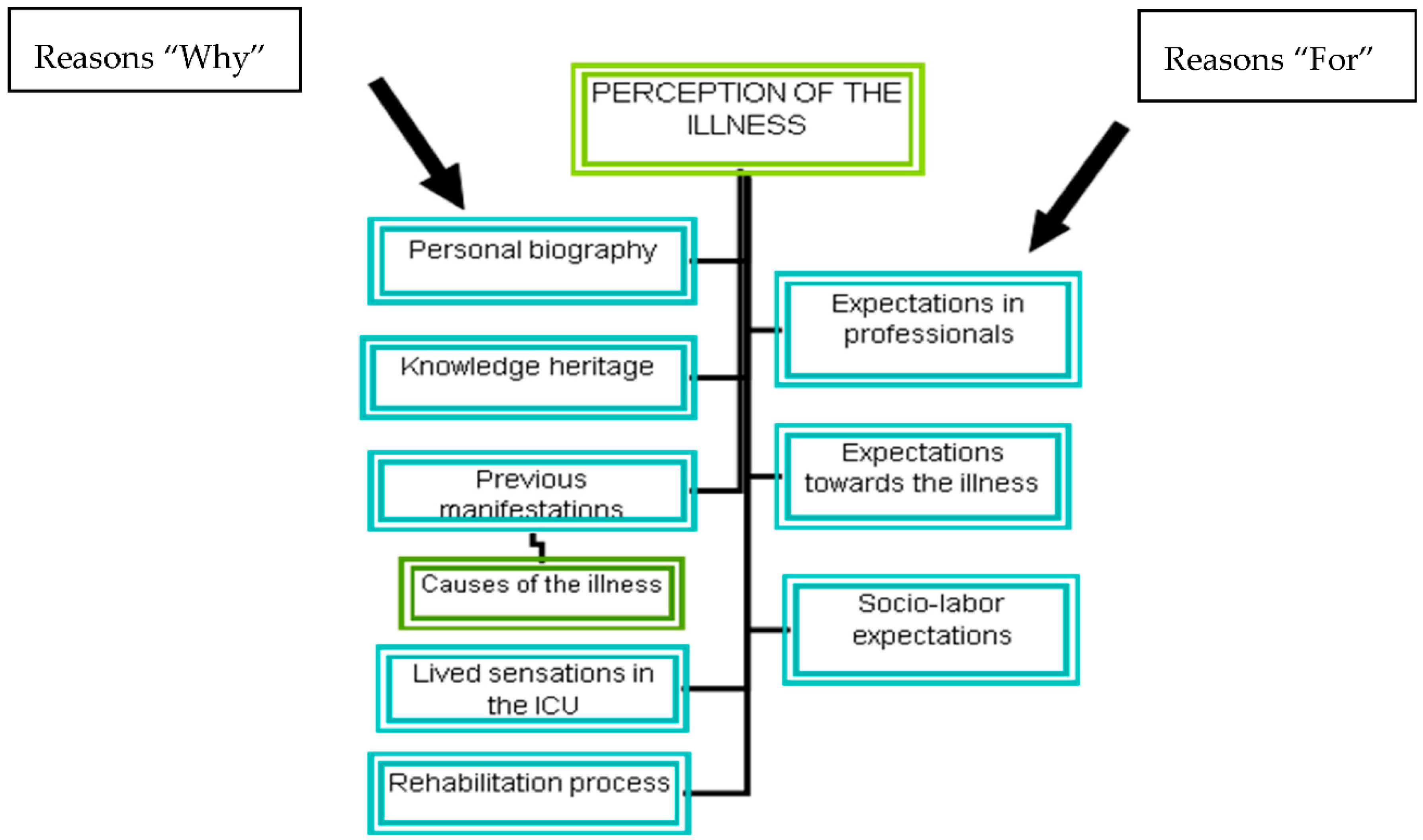
3.2. Reasons “Why” of the Myocardial Infarction Sufferers
“A month before, I walked out of work, I couldn’t stand it there any more, I just couldn’t, I sat down, I knelt, as if I was out of it, I lay on my back. Then I blamed it on stress and it never occurred to me that it might have been a heart attack ….”(D13)
“Everything is coming out now, I’ve worked a lot, I’ve had to work in the fields and the suchlike since I was 11, I’ve worked so much my whole life, so very, very much”(D3)
“My life in general was really crazy, I mean, I’ve always liked partying although I don’t think I partied to excess and I’ve always liked know going out and disappearing for two or three days, and making the party last all weekend”(D2)
“I smoked since I was 12 or 13 until last year”. “I ate a lot of salt, a lot of fat. I never cared”(D12)
“When I was in the ICU I cried a lot because I was afraid that I was already dead”(D4)
“I knew someone who had a heart attack and it’s like I say sometimes, (…) it’s precisely those who have had a heart attack that die from one”(D5)
3.3. Reasons “For” of the Myocardial Infarction Sufferers
“When I got home, I was afraid and we’ve been back to the hospital twice”(D14)
“Before myocardial infarction, I had decided to change my 100 m2 home to 150 m2, or change my car, after, I thought about it. I said to myself that I am all running around for a better life, if I am to be bed-ridden, does it really make any difference if my home is 100 or 150 m2 or if my car is a Peugeot or Elegance Mercedes”(D12)
“I was given that information in the corridor and I… I was really scared, it’s not that I don’t want more information but I thought that they should be the ones to tell me how I should live my life from now on”(D7)
“Now I drive less, before we didn’t used to go out a lot but we did go away at Christmas”(D1)
“I get very tired, the stairs kill me and if not them, the hills, I can’t manage the hills, I’m a pensioner now”(D6)
“Life has changed me a lot. Life has no meaning when you are sick, let alone having a painful heart. You will value life when you get sick, even if you have the world, it will be valueless”(D5)
4. Discussion
4.1. Study Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Reveals Leading Causes of Death and Disability Worldwide: 2000–2019. Available online: https://www.who.int/news/item/09-12-2020-who-reveals-leading-causes-of-death-and-disability-worldwide-2000-2019 (accessed on 9 December 2020).
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Ferrerira-González, I. Epidemiología de la enfermedad coronaria. Rev. Esp. Cardiol. 2014, 67, 139–144. Available online: http://www.revespcardiol.org/es/epidemiologia-enfermedad-coronaria/articulo/90267578/ (accessed on 14 October 2016). [CrossRef]
- Orozco-Beltran, D.; Cooper, R.; Gil-Guillen, V.; Bertomeu-Martinez, V.; Pita-Fernandez, S.; Durazo-Arvizu, R. Tendencias en mortalidad por infarto de miocardio. Estudio comparativo entre España y Estados Unidos: 1990–2006. Rev. Esp. Cardiol. 2012, 65, 1079–1085. Available online: http://www.revespcardiol.org/es/tendencias-mortalidad-por-infarto-miocardio-/articulo/90165277/ (accessed on 14 October 2016). [CrossRef]
- Moran, A.; Odden, M. Tendencias de la mortalidad por infarto de miocardio en España y Estados Unidos: ¿una carrera cuesta abajo o cuesta arriba en el siglo XXI? Rev. Esp. Cardiol. 2012, 65, 1069–1071. Available online: http://www.revespcardiol.org/es/tendencias-mortalidad-por-infarto-miocardio/articulo/90165274/ (accessed on 14 October 2016). [CrossRef] [PubMed] [Green Version]
- Dreyer, R.P.; Pavlo, A.J.; Hersey, D.; Horne, A.; Dunn, R.; Norris, C.M.; Davidson, L. “Is My Heart Healing?” A Meta-Synthesis of Patients’ Experiences after Acute Myocardial Infarction. J. Cardiovasc. Nurs. 2020. [Google Scholar] [CrossRef]
- Salminen-Tuomaala, M.; Åstedt-Kurki, P.; Rekiaro, M.; Paavilainen, E. Coping experiences: A pathway towards different coping orientations four and twelve months after myocardial infarction—A grounded theory approach. Nurs. Res. Prac. 2012. Available online: https://www.hindawi.com/journals/nrp/2012/674783/ (accessed on 14 October 2018). [CrossRef]
- Baldacchino, D. Myocardial infaction: A turning point in meaning in life over time. Br. J. Nurs. 2011, 202, 107–114. [Google Scholar] [CrossRef]
- Fredriksson, U.; Alsén, P.; Karlson, B.W.; Brink, E. Fatigue two months after myocardial infarction and its relationships with other concurrent symptoms, sleep quality and coping strategies. J. Clin. Nurs. 2015, 24, 2192–2200. [Google Scholar] [CrossRef] [PubMed]
- Junehag, L.; Asplund, K.; Svedlund, M. A qualitative study: Perceptions of the psychosocial consequences and access to support after an acute myocardial infarction. Intens. Crit. Care Nurs. 2014, 30, 22–30. [Google Scholar] [CrossRef]
- Andersson, E.K.; Borglin, G.; Willman, A. The experience of younger adults following myocardial infarction. Qual. Health Res. 2013, 23, 762–772. [Google Scholar] [CrossRef] [Green Version]
- Fors, A.; Kertin, D.; Ekman, I. Life is lived forwards and understood backwards—Experiences of being affected by acute coronary syndrome: A narrative analysis. Int. J. Nurs. Stud. 2014, 51, 430–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schutz, A. El problema de la Realidad Social. Escritos I. Buenos Aires; Amorrortu: Madrid, Spain, 2008. [Google Scholar]
- Schutz, A. Estudios Sobre Teoría Social. Escritos II. Buenos Aires; Amorrortu: Madrid, Spain, 2003. [Google Scholar]
- Jesus, M.C.; Capalbo, C.; Merighi, M.A.B.; Oliveira, D.; Tocantins, F.; Rodrigues, B.; Ciuffo, L.L. The social phenomenology of Alfred Schütz and its contribution for the nursing. Rev. Esc. Enferm. USP 2013, 47, 736–741. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0080-62342013000300736&lng=en (accessed on 7 April 2017). [CrossRef] [Green Version]
- Merighi, M.A.B.; Jesus, M.C.; Domingos, R.F.; Oliveira, D.M.; Baptista, P.C.P. Being a nursing teacher, woman and mother: Showing the experience in the light of social phenomenology. Rev. Latino-Am. Enferm. 2011, 19, 164–170. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692011000100022 (accessed on 14 October 2017). [CrossRef] [PubMed] [Green Version]
- Delgado, J.M.; Gutierrez, J. Métodos y Técnicas Cualitativas de Investigación en Ciencias Sociales; Síntesis: Madrid, Spain, 2007. [Google Scholar]
- Parga Nina, L. Estudo das Informações não Estruturadas do ENDEF e de sua Integração com os Dados Quantitativos; PUC-RJ: Rio de Janeiro, Brazil, 1978. [Google Scholar]
- Merighi, M.A.B. Professional trajectory of obstetric nurses from the University of São Paulo College of Nursing: A focus on social phenomenology. Rev Latino-Am Enferm. 2002, 10, 5. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692002000500004 (accessed on 19 October 2013).
- Araújo, B.; Rodrigues, B. Mothers’ experiences and perspectives regarding their premature infant’s stay at the Neonatal Intensive Care Unit. Rev. Esc. Enferm. USP 2010, 44, 865–872. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0080-62342010000400002&lng=en (accessed on 7 April 2017). [CrossRef]
- Eriksson, M.; Asplund, K.; Svedlund, M. Patients’ and their partners’ experiences of returning home after hospital discharge following acute myocardial infarction. Eur. J. Cardiov. Nurs. 2009, 8, 267–273. [Google Scholar] [CrossRef]
- Hassani, P.; Ardeshir, A.; Masoude, F.K. Perceived positive effects of illness following acute myocardial infarction. Int. J. Nurs. Midwif. 2009, 1, 1–5. [Google Scholar]
- Solano, M.C.; Siles, J. Las vivencias del paciente coronario en la unidad de cuidados críticos. Index Enferm. 2005, 51, 29–33. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1132-12962005000300006 (accessed on 18 October 2014). [CrossRef]
- Ramírez, C.A.; Parra, M. Percepción de los comportamientos del cuidado de enfermería en la unidad de cuidados intensivos. Av. Enferm. 2011, 29, 97–108. [Google Scholar]
- Gómez, M.J.; Casajús, G.; Gómez, C.; Martínez, A. Percepciones y experiencias vividas por el paciente con un primer infarto, e impacto en su entorno social, familiar y laboral. Enferm. Cardiol. 2012, 55–56, 67–75. Available online: https://www.enfermeriaencardiologia.com/wp-content/uploads/55_56_10.pdf (accessed on 18 October 2014).
- Brink, E.; Brändström, Y.; Cliffordsson, C.; Herlitz, J.; Karlson, B.W. Illness consequences after myocardial infarction: Problems with physical functioning and return to work. J. Adv. Nurs. 2008, 64, 587–594. [Google Scholar] [CrossRef] [PubMed]
- López-Medina, I.; Gil-García, E.; Sánchez-Criado, V.; Pancorbo-Hidalgo, P.L. Patients’ Experiences of Sexual Activity Following Myocardial Ischemia. Clin. Nurs. Res. 2016, 25, 45–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassen, T.A.; Nordrehaug, J.E.; Hanestad, B.R. A qualitative study of the infomations needs of acute myocardial infarction patients, and their preferences for follow-up contact after discharge. Eur. J. Cardiov. Nurs. 2005, 4, 37–44. [Google Scholar]
- Stolic, S.; Michtell, M.; Wolllin, J. Nurse-led telephone interventions for people with cardiac disease. A review of the research literature. Eur. J. Cardiov. Nurs. 2010, 9, 203–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solano, M.C.; Siles, J.; Fernades, G. Vivencias de las esposas cuyas parejas han sufrido un infarto de miocardio. Index Enferm. 2008, 17, 7–11. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1132-12962008000100002&lng=es (accessed on 7 April 2018).


{kind=link}
| Prior Illnesses |
|---|
| Antecedents, risk factors |
| Diagnosis, dates, therapies |
| Prior hospital admissions |
| Social and family support |
| Beliefs (religion…) |
| Current |
| Changes in lifestyle, work, sexuality, partnerships |
| The emotional situation |
| Feelings and meaning of the illness. |
| Participants | Age | Marital Status | Current Employment Status | Level of Education | Socio-Economic Level | Prior Record of Illnesses |
|---|---|---|---|---|---|---|
| D-1 | 61 | married | Pensioner | Primary | Mid-high | No priors |
| D-2 | 50 | married | Active | Primary | Mid | * AMI-2008 |
| D-3 | 58 | married | Pensioner | Primary | Mid | ** IDDM |
| D-4 | 62 | married | Active | Secondary | Mid | No priors |
| D-5 | 60 | separate | Unemployed | Secondary | Mid-low | No priors |
| D-6 | 41 | single | Pensioner | Primary | Low | AMI 2014 chest pain |
| D-7 | 52 | married | Active | Secondary | Mid | AMI 2000 |
| D-8 | 46 | separate | Active | Higher | Mid-high | No priors |
| D-9 | 57 | separate | Active | Primary | Low | High blood pressure |
| D-10 | 66 | married | Pensioner | Higher | Mid | Int. Claudication |
| D-11 | 61 | separate | Sick leave | Primary | Low | Prior infarctions |
| D-12 | 53 | married | Sick leave | Primary | Low | No priors |
| D-13 | 46 | separate | Sick leave | Primary | Low | No priors |
| D-14 | 54 | married | Sick leave | Primary | Low | No priors |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solano-Ruiz, M.; Freitas, G.F.d.; Ugarte-Gurrutxaga, M.I.; Gómez-Cantarino, S.; Siles-González, J. Men’s Positive and Negative Experiences Following Acute Myocardial Infarction. Int. J. Environ. Res. Public Health 2021, 18, 1053. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031053
Solano-Ruiz M, Freitas GFd, Ugarte-Gurrutxaga MI, Gómez-Cantarino S, Siles-González J. Men’s Positive and Negative Experiences Following Acute Myocardial Infarction. International Journal of Environmental Research and Public Health. 2021; 18(3):1053. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031053
Chicago/Turabian StyleSolano-Ruiz, MCarmen, Genival Fernandes de Freitas, M. Idoia Ugarte-Gurrutxaga, Sagrario Gómez-Cantarino, and José Siles-González. 2021. "Men’s Positive and Negative Experiences Following Acute Myocardial Infarction" International Journal of Environmental Research and Public Health 18, no. 3: 1053. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031053