
Health Advertising during the Lockdown: A Comparative Analysis of Commercial TV in Spain




Abstract
:1. Introduction
Contextualization of the Study
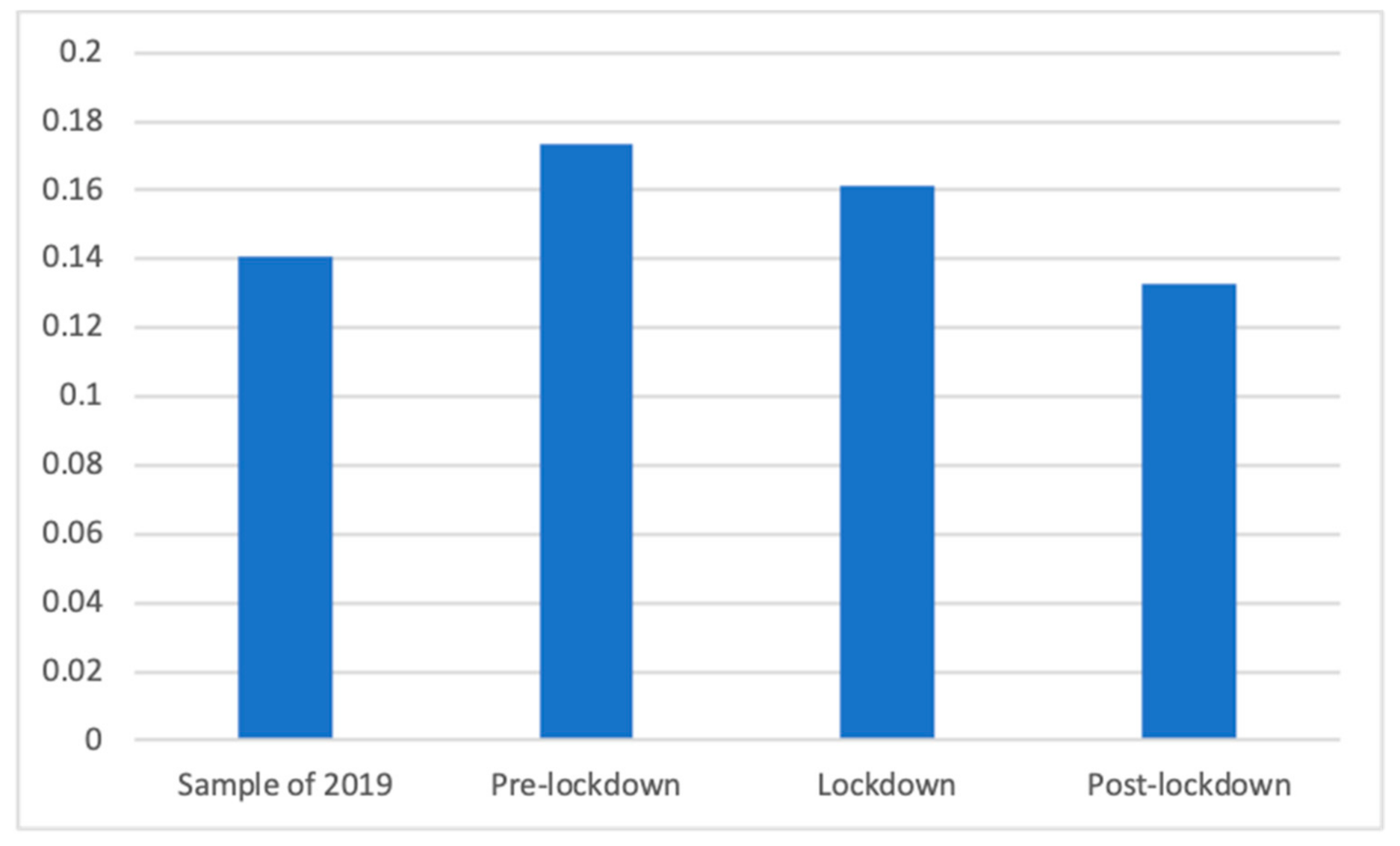
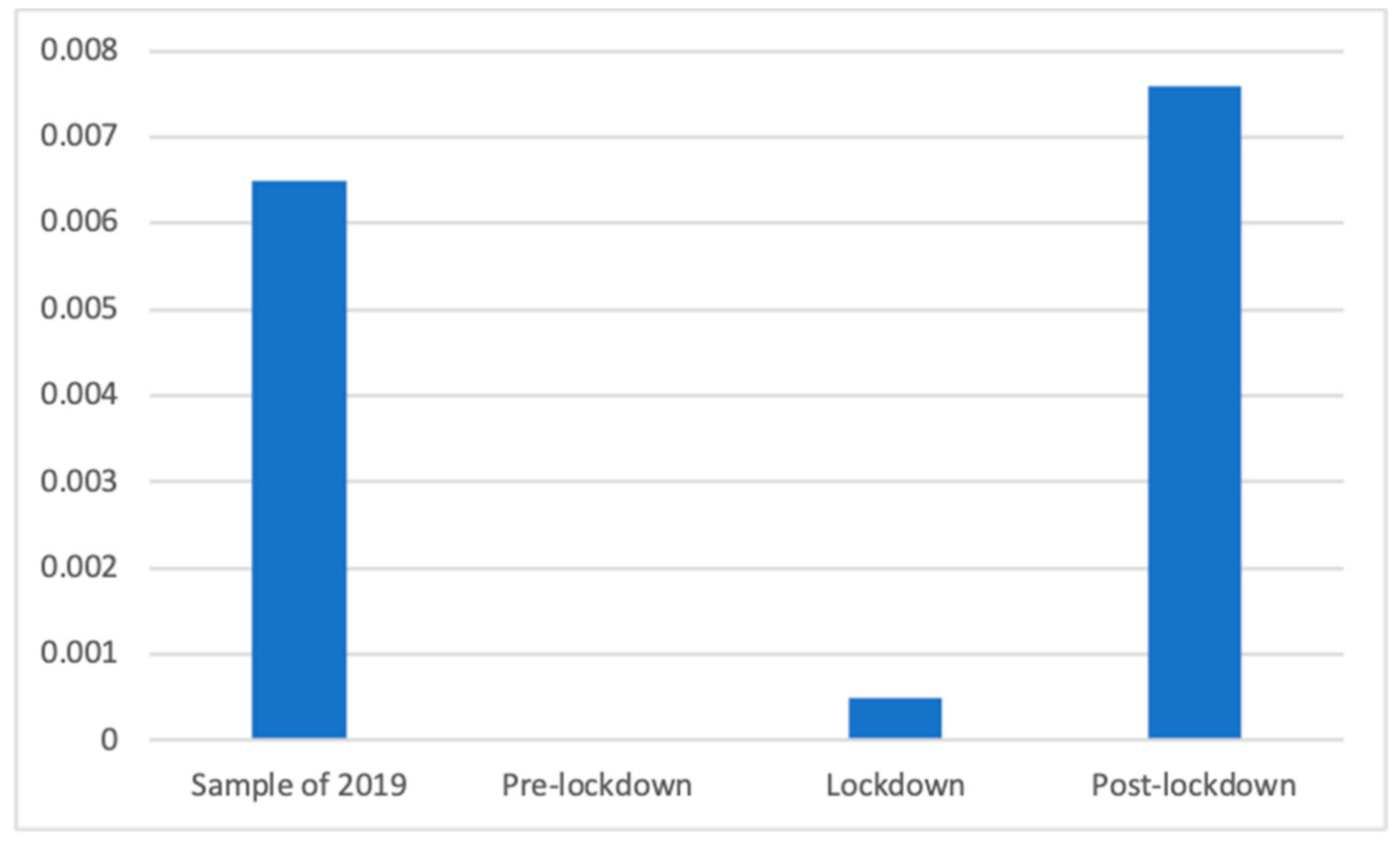
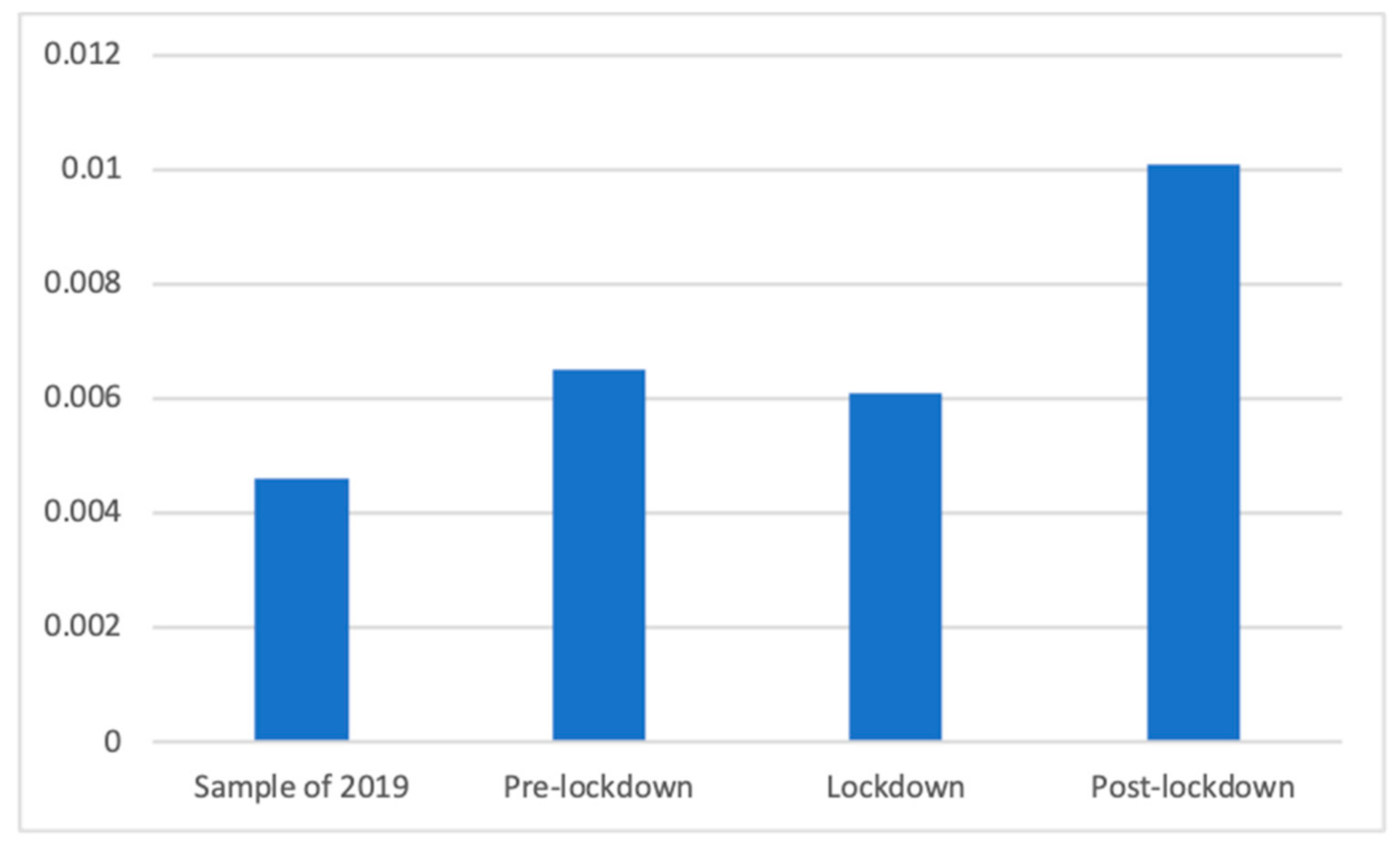
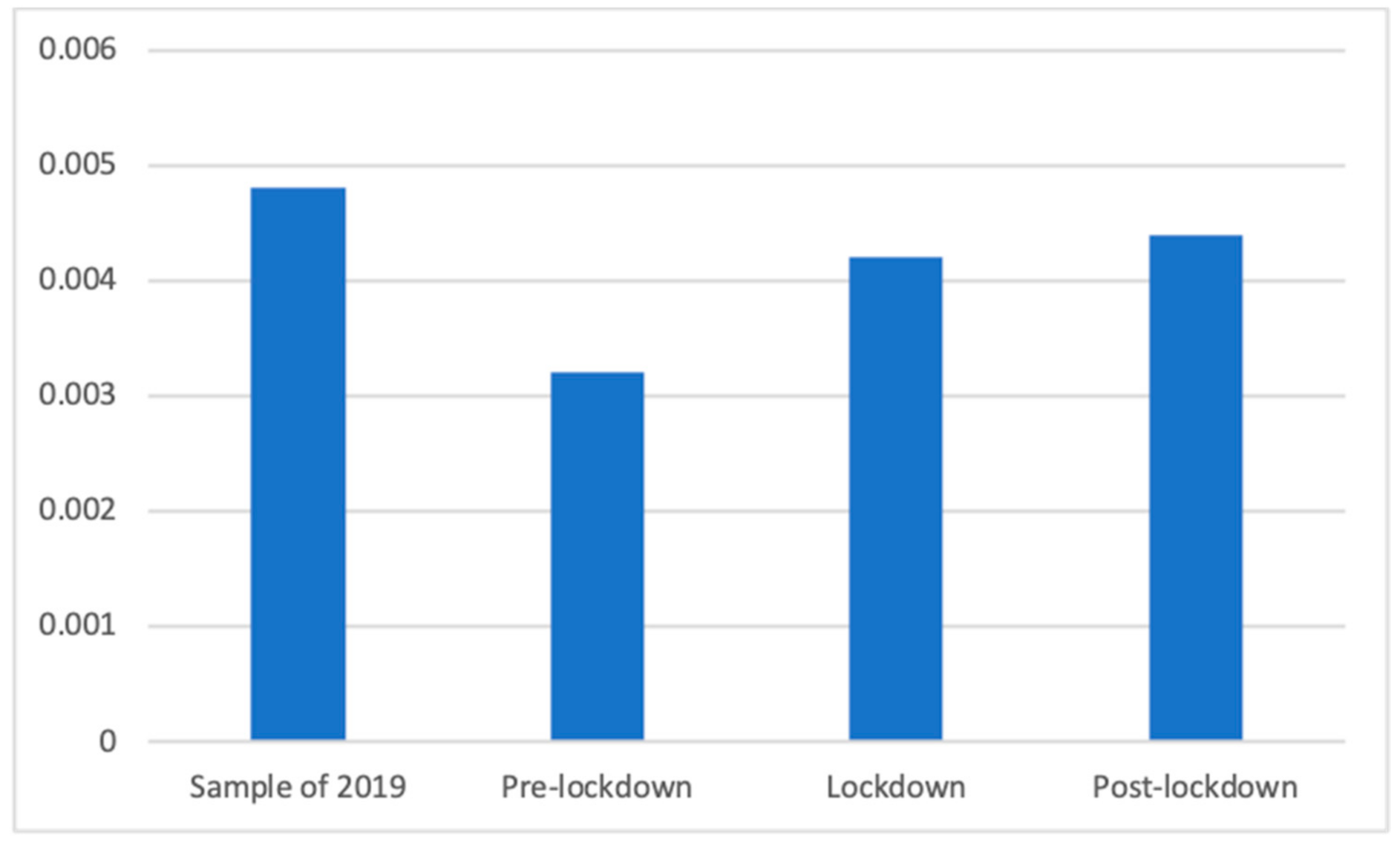
- RQ1: What was the proportion of health advertisements broadcasted daily before, during, and after the lockdown by the main Spanish commercial television broadcasters?
- RQ2: Did the presence of different types of health advertisements on the main Spanish commercial television broadcasters increase during the lockdown compared to the same period in the previous year?
- RQ3: What types of health advertisements were prevalent before, during, and after the lockdown on the main Spanish commercial television broadcasters?
2. Materials and Methods
2.1. Sample
- Lockdown: Since the lockdown was decreed in Spain on 14 March 2020, following the declaration of the state of alarm by the government, until Phase 0 of the de-escalation started on 3 May 2020, and the restrictions started to be progressively eased. This was the most dramatic period, during which the harshest restrictions were applied, and it is central to our analysis because the other periods of the study were designed around this one.
- Pre-lockdown: Fifty days before the beginning of the lockdown, that is, from 24 January 2020 to 13 March 2020. This includes the weeks before the pandemic was declared by the World Health Organization when the virus was gaining media relevance, but, as expected, without having yet influenced the advertising behavior.
- Post-lockdown: Fifty days after the de-escalation started, that is, 4 May 2020 to 22 June 2020. This period includes the ending of the state of alarm on 21 June 2020. It includes the weeks in which the restrictions were being eased, and people could start resuming some of their normal activities, reaching the so-called “new normality”.
- Equivalent dates of 2019: From 14 March 2019 to 3 May 2019, that is, the fifty days included in the central period of analysis. During this period in 2019, however, the SARS-COV-2 had not been detected, thus allowing comparison with a period during which there was no influence of the virus.
2.2. Instrument and Procedure
- Food and non-alcoholic beverages: includes all food products and non-alcoholic beverages that can be purchased for consumption at home;
- Alcoholic beverages: includes all alcoholic beverages that can be purchased for consumption at home, including low or non-alcoholic beverages that are generally alcoholic, such as non-alcoholic beer. The original ECOICOP category also includes tobacco, but given the prohibition on tobacco advertising, it was not included in the study;
- Clothing and footwear: includes clothing materials—including fabrics and accessories such as buttons or sewing threads—garments, accessories, footwear and cleaning, repair and hire of clothing, and footwear;
- Housing, water, electricity, gas and other fuels: includes real estate acquisition or renting, and repair services or materials (painting, minor plumbing, electricians, etc.), other services relating to the dwelling (gardening, security, etc.), and supplies for the dwelling (heating, electricity, water, gas, fuels, heat energy, etc.). In general, this category includes all products and services for the acquisition or maintenance of a dwelling;
- Furnishings, household equipment and routine household maintenance: includes all household or garden furniture and furnishings, carpets and other floor coverings, lighting equipment, household textiles (bed linen, curtains, table linen, etc.), household appliances, glassware, tableware and household utensils, tools and equipment for house and garden (electric drills, lawnmowers, alarms, etc.), non-durable household goods (cleaning products, candles, nails, fire extinguishers, etc.). It also includes all rental, repair or associated services and cleaning or maintenance services;
- Health: This category is further discussed below, but in general terms, it includes health products and medicines, health services and health communication, and PSAs;
- Transport: includes bicycles and motor vehicles (excluding recreational vehicles such as camper vans or boats) and all services and products for their use, reparation, cleaning, or maintenance (including parking expenses, fuel, driving lessons, GPS). It also includes transportation services, such as buses, trains, taxis, flights, or any other private or public transportation method;
- Communication: includes postal and parcel delivery services (it does not include Amazon or food delivery apps, for example), and telephone and Internet providers, services, or equipment (including smartphones or bundled telecommunication services, but excluding computers or video-on-demand services);
- Recreation and culture: includes audiovisual, photographic, and information processing equipment (in general, all technological devices, such as computers or televisions, except for smartphones), and all software, applications and Internet-based services and business that do not specifically apply to any other category (for instance, an Internet-based clothes shop would be included in “clothing and footwear”, but Amazon, with a broader scope, would belong in this category). It also includes major durables for recreation (camper vans, canoes, golf carts, etc.), sports equipment, musical instruments, major durables for indoor recreation (gaming machines, billiard tables, etc.), any other recreational items and equipment (toys, games, celebration articles), and flowers and other garden products. It also includes any repair, maintenance, or complementary service or good applied to the previous goods. It also includes pets and any food, product, or service associated with them. Additionally, it includes all recreational or cultural services and attendance, such as sports events, cinema, theater, concerts, museums, television subscriptions, or any other game of chance, both online and offline. Finally, it includes newspapers, books, and stationery, and package holidays;
- Education: includes all educational services, including language courses, schools, or universities.
- Restaurants and hotels: includes catering services, including restaurants, bars, and take-away local food services. Furthermore, includes accommodation services;
- Miscellaneous goods and services: includes personal care (hairdressing, grooming, hygiene, wellness, etc.), baby or child care (nurseries, babysitters, etc.), personal effects (jewelry, clocks, watches, travel goods, articles for babies, etc.), and counseling, insurance, financial, legal, or funeral services. Similar to the case of tobacco, the original ECOICOP category also includes here services such as prostitution, which, given their illegality, are not advertised and, therefore, were not included in the final codebook.
- Health insurance: although originally included in “other goods and services”, health insurance was moved into this category so that more detailed observations of this type of service could be conducted. When insurance companies were advertised, focusing on other types of insurance or in a general sense, without a focus on the health aspect, they were left outside the health category;
- Care services, such as caretakers or residences for ill or old people, were also moved from the “other goods and services” to this category;
- Institutional communication or PSAs related to health issues, both focused on the coronavirus or on other health aspects, were included in two ad hoc subcategories created for the study: one for the advertising of public institutions and one for the advertising of private institutions;
- Different types of medicines, not differentiated in the original subclassification, were taken into account in the new codebook to enable the study of how medicines that could be used to counter COVID-19 or other specific illnesses were more or less present during the period of analysis. These subcategories were developed following the classification proposed by the World Health Organization in its List of Essential Medicines [43], together with an exploratory observation and the ECOICOP classification.
- With the goal of focusing on products particularly associated with COVID-19 prevention, a specific group was also added, in which facemasks, hydrogel or gloves were included.
- Slimming products, such as drugs and other treatments, excluding food products with a health component, such as anti-cholesterol yogurts;
- Analgesic and anti-inflammatory products, such as ibuprofen or paracetamol;
- Antacids, including all types of stomach protectors;
- Contraceptives, including pills and non-oral forms (such as condoms);
- Antihistamine products;
- Antibiotics, anti-fungal, and other anti-infective products;
- Antipyretic drugs specifically designed to fight fever, excluding products that could have such an effect, but not as the main goal, such as analgesics;
- Antitussive, mucolytic, or anti-flu products: includes drugs and syrups, and nose-sprays or products such as Vicks VapoRub;
- Vitamin supplements, including drugs and chemical products, but not food products with a health plus, such as calcium-rich milk;
- Medical creams and spray, including anti-varicose vein, vaginal, and anti-inflammatory creams and similar;
- Laxatives and antidiarrheal products;
- Homeopathic products;
- Throat lozenges;
- Sleeping pills and other sleeping treatments;
- Other drugs and medical or pharmaceutical products, including only non-durable products that could not be allocated in any of the previous categories;
- Facemasks, gloves, and hydrogels, and similar products specifically recommended to prevent COVID-19;
- Therapeutic equipment, including glasses, hearing aids, wheelchairs, crutches, stairlifts, etc.;
- Other medical products, including bandage strips, adhesive dressing, syringes, merbromin, and pregnancy tests;
- Medical or hospital services, including private doctors, plastic surgery, clinics, etc.;
- Dental services and clinics;
- Paramedical services, including blood tests, thermal treatments, rehab, physiotherapy, opticians, oculists, or otolaryngologists when the services and clinics were advertised rather than glasses or hearing aids;
- Private health insurance;
- Care homes, including retirement homes for elderly persons, residences for disabled persons, or rehabilitation centers;
- Residential care and assistance, including home help or daycare for elderly or disabled persons at home;
- Other medical or aid services, including other health-related services not included in the previous categories, for example, medical credits;
- PSAs by public institutions;
- PSAs campaigns by private institutions.
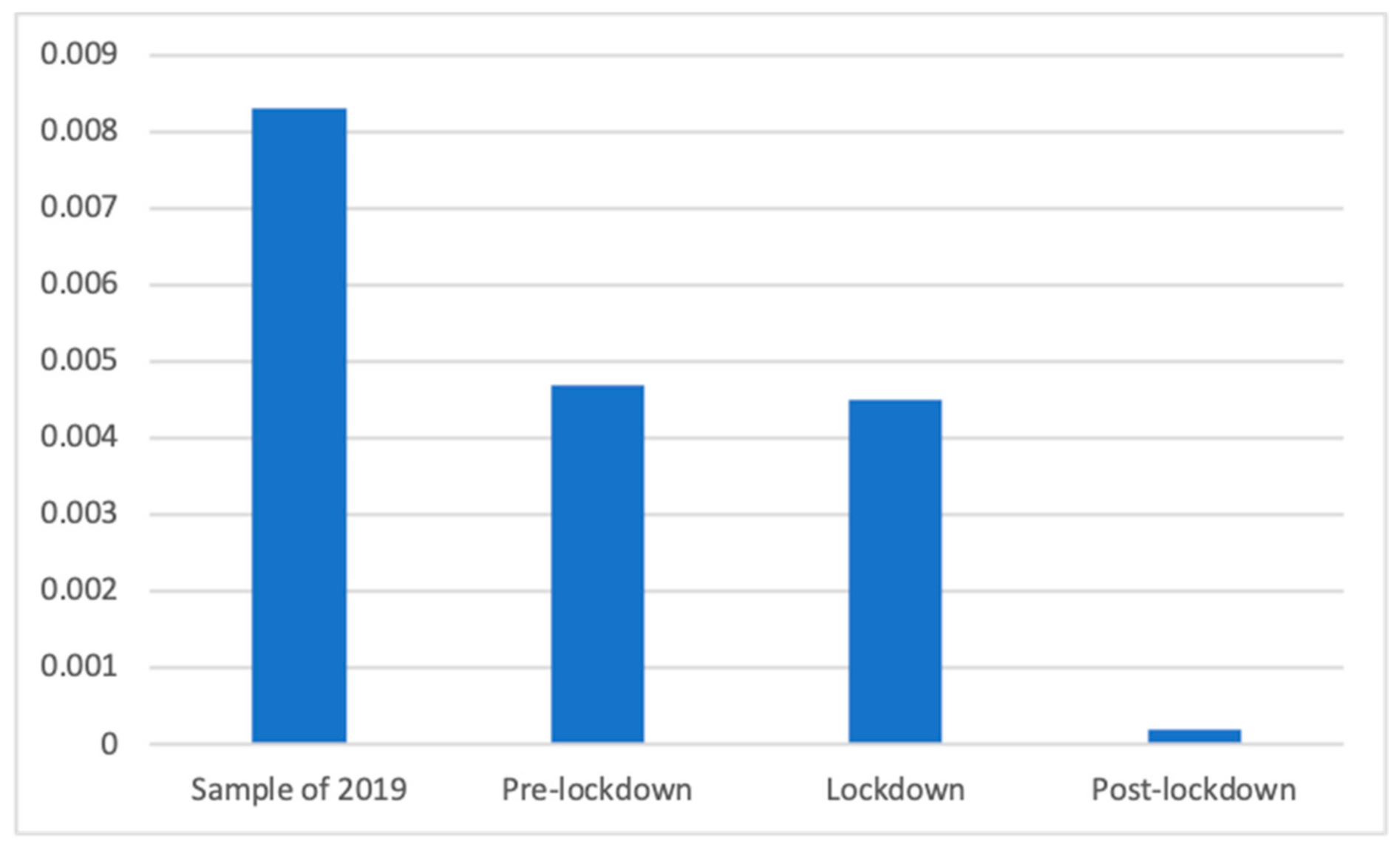
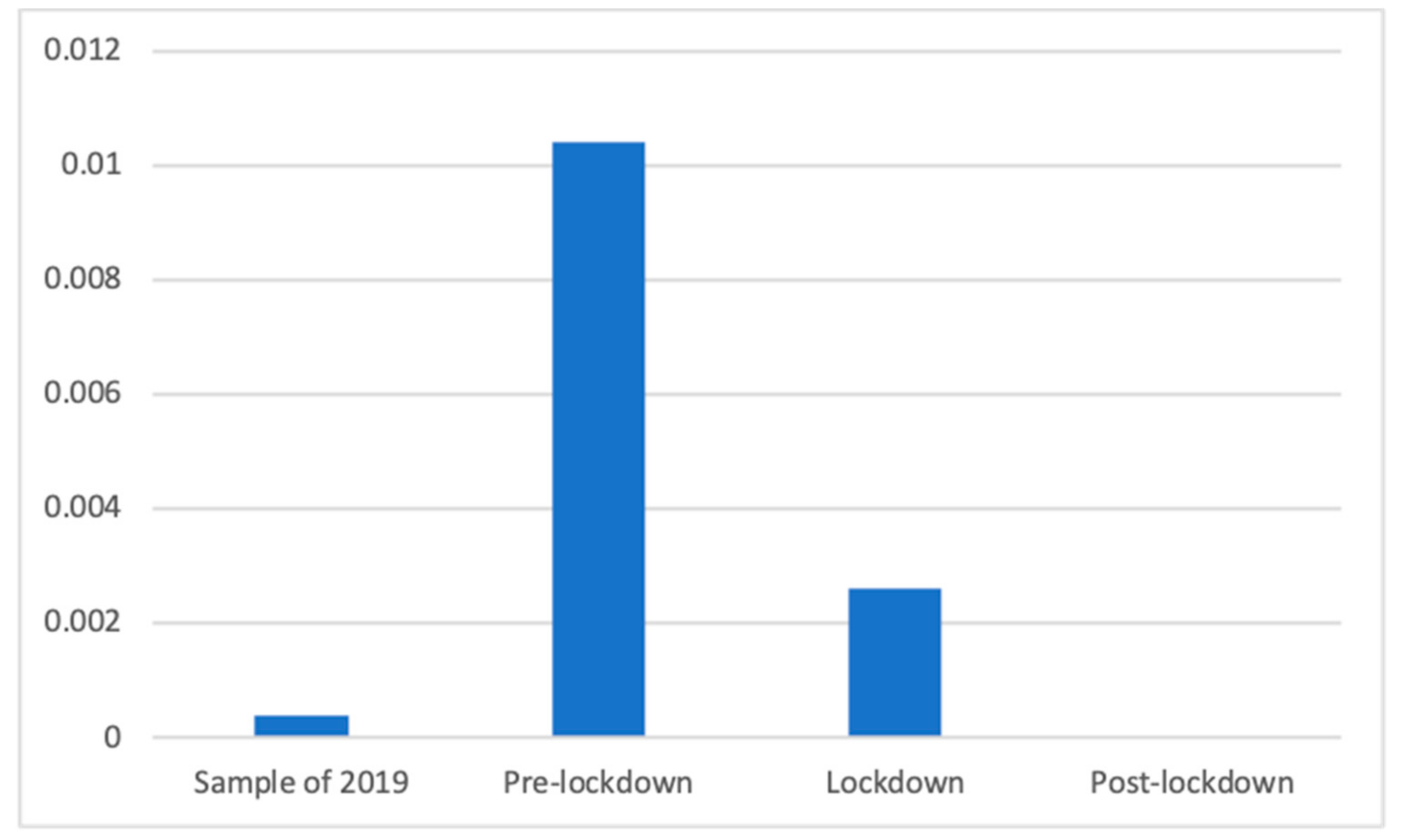
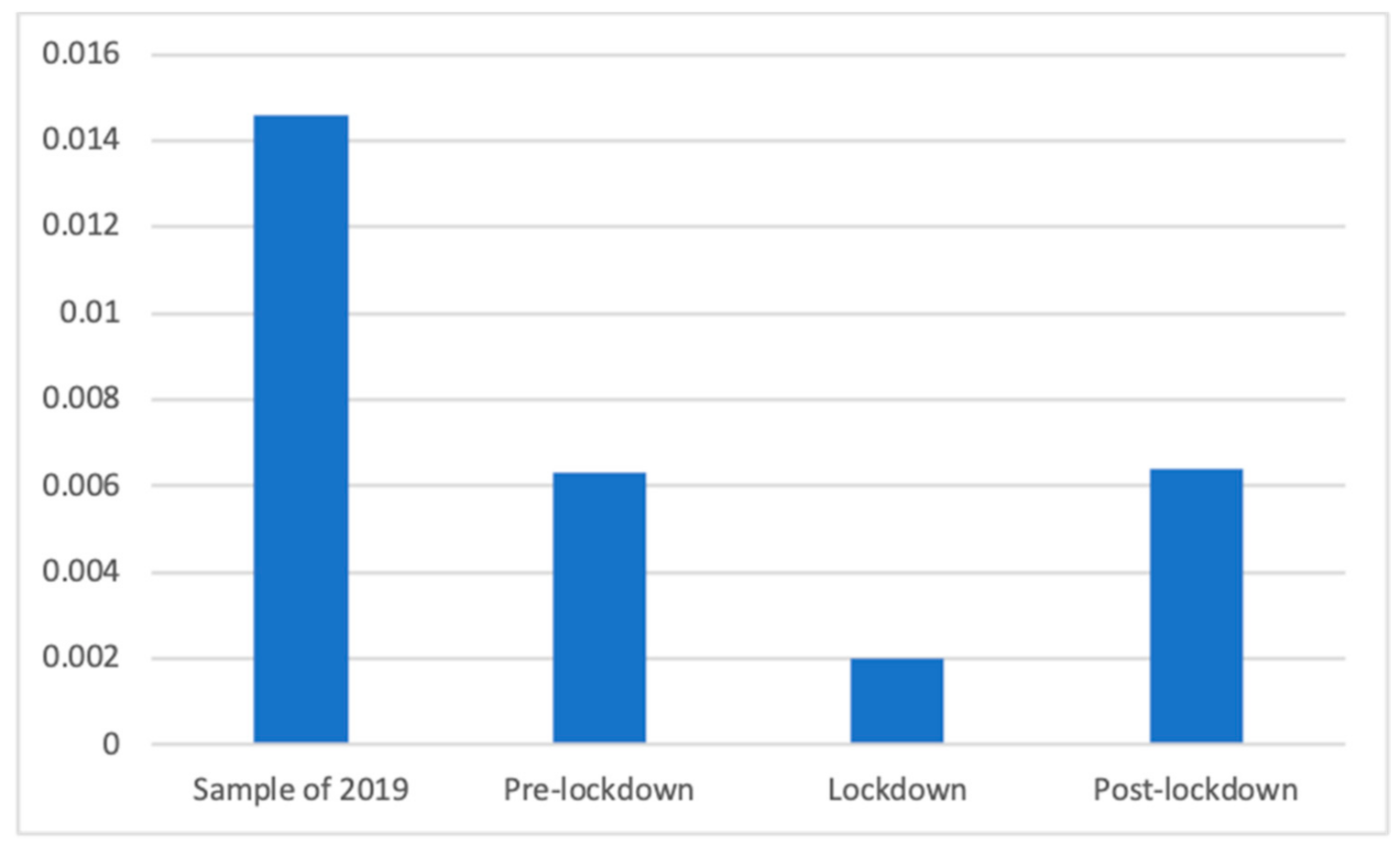
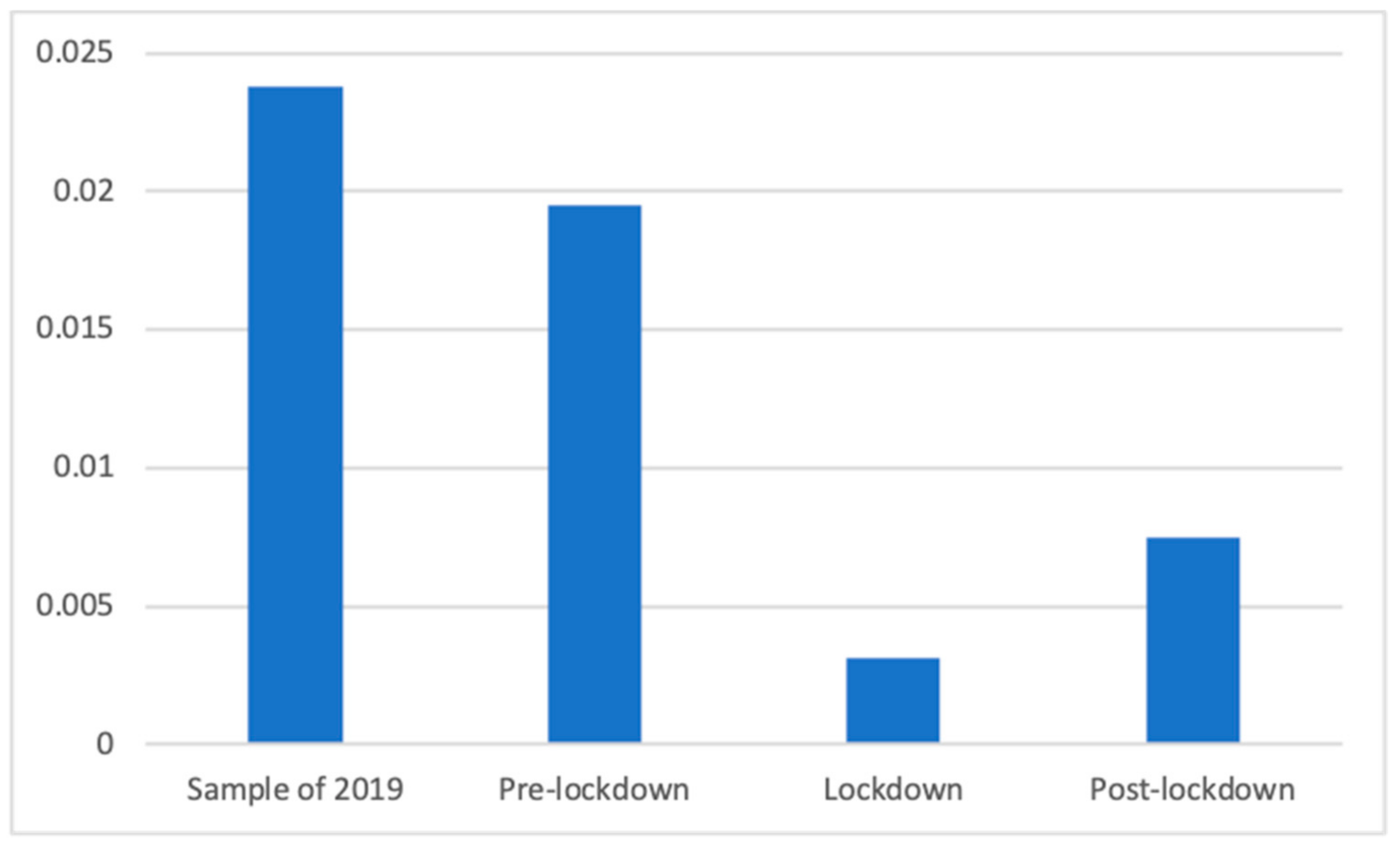
3. Results
Health Advertising during the Lockdown
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Igartua, J.J.; Ortega-Mohedano, F.; Arcila-Calderón, C. Communication use in the times of the coronavirus. A cross-cultural study. El Prof. Inf. 2020, 29, e290318. [Google Scholar] [CrossRef]
- Román-San-Miguel, A.; Valenzuela, N.S.G.; Zambrano, R.E. Las fake news durante el Estado de Alarma por COVID-19. Análisis desde el punto de vista político en la prensa española. Rev. Lat. Comun. Soc. 2020, 78, 359–391. [Google Scholar] [CrossRef]
- Gerbner, G.; Gross, L.; Morgan, M.; Signorielli, N. Living with television: The dynamics of the cultivation process. In Perspectives on Media Effects; Bryant, J., Zillmann, D., Eds.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1986; pp. 17–40. [Google Scholar]
- Katz, E.; Blumler, J.; Gurevitch, M. Uses and Gratifications Research. Public Opin. Q. 1973, 37, 509–523. [Google Scholar] [CrossRef]
- Estudio General de Medios. 1ª Ola 2020. Available online: http://reporting.aimc.es/index.html#/main/television (accessed on 19 November 2020).
- Internet World Stats. Available online: https://www.internetworldstats.com/stats.html (accessed on 19 November 2020).
- Speedtest Global Index. Available online: https://www.speedtest.net/global-index (accessed on 19 November 2020).
- El consumo de Televisión Batió Récords Históricos en Marzo por el Coronavirus. Available online: https://www.20minutos.es/noticia/4211810/0/el-consumo-de-television-batio-records-historicos-en-marzo-por-el-coronavirus/ (accessed on 19 November 2020).
- El Confinamiento Lleva a Récord Histórico el Consumo de Televisión: 5 Horas al Día por Persona. Available online: https://cadenaser.com/ser/2020/05/01/television/1588343709_377699.html (accessed on 19 November 2020).
- Estudio InfoAdex de la Inversión Publicitaria en España 2020. Available online: https://www.infoadex.es/home/wp-content/uploads/2020/02/NP-Estudio-InfoAdex-de-la-Inversión-Publicitaria-en-España-2020.pdf (accessed on 19 November 2020).
- Rogers, E.M. Up-to-date report. J. Health Commun. 1996, 1, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Menashe, C.L. The Power of a Frame: An Analysis of Newspaper coverage of Tobacco Issues–United States. J. Health Commun. 1998, 3, 307–325. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.E.; Wallack, L. A content analysis of sexually transmitted diseases in the print news media. J. Health Commun. 2004, 9, 111–117. [Google Scholar] [CrossRef]
- Collinson, S.; Khan, K.; Heffernan, J.M. The Effects of Media Reports on Disease Spread and Important Public Health Measurements. PLoS ONE 2015, 10, e0141423. [Google Scholar] [CrossRef]
- Noar, S.M. A 10-year retrospective of research in health mass media campaigns: Where do we go from here? J. Health Commun. 2006, 11, 21–42. [Google Scholar] [CrossRef] [Green Version]
- Redman, S.; Spencer, E.A.; Sanson-Fisher, R.W. The role of mass media in changing health-related behaviour: A critical appraisal of two models. Health Promot. Int. 1990, 5, 85–101. [Google Scholar] [CrossRef]
- Shen, F.; Sheer, V.C.; Li, R. Impact of narratives on persuasion in health communication: A meta-analysis. J. Advert. 2015, 44, 105–113. [Google Scholar] [CrossRef]
- Toppenberg-Pejcic, D.; Noyes, J.; Allen, T.; Alexander, N.; Vanderford, M.; Gamhewage, G. Emergency risk communication: Lessons learned from a rapid review of recent gray literature on Ebola, Zika, and Yellow Fever. Health Commun. 2019, 34, 437–455. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, E.; Tinker, T. Effective Health Risk Communication about Pandemic Influenza for Vulnerable Populations. Am. J. Public Health 2019, 99, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Holmes, B.J. Communicating about emerging infectious disease: The importance of research. Health Risk Soc. 2008, 10, 349–360. [Google Scholar] [CrossRef]
- Airhihenbuwa, C.O.; Obregon, R. A critical assessment of theories/models used in health communication for HIV/AIDS. J. Health Commun. 2000, 5, 5–15. [Google Scholar] [CrossRef]
- Blendon, R.; Benson, J.; Desroches, C.; Raleigh, E.; Taylor-Clark, K. The public’s response to severe acute respiratory syndrome in Toronto and the United States. Clin. Infect. Dis. 2004, 38, 925–931. [Google Scholar] [CrossRef] [Green Version]
- Brug, J.; Aro, A.; Oenema, A.; de Zwart, O.; Richardus, J.; Bishop, G. SARS risk perception, knowledge, precautions, and information sources, the Netherlands. Emerg. Infect. Dis. 2004, 10, 1486–1489. [Google Scholar] [CrossRef]
- Costa-Saánchez, C.; Rodríguez-Vázquez, A.I.; López-García, X. Del periodismo transmedia al replicante. Cobertura informativa del contagio de ébola en España por Elpais.com. El Prof. Inf. 2015, 24, 282–290. [Google Scholar] [CrossRef] [Green Version]
- Kostkova, P.; Szomszor, M.; St. Louis, C. #swineflu: The Use of Twitter as an Early Warning and Risk Communication Tool in the 2009 Swine Flu Pandemic. ACM Trans. Manag. Inf. Syst. 2014, 5. [Google Scholar] [CrossRef]
- Wirz, C.D.; Xenos, M.A.; Brossard, D.; Scheufele, D.; Chung, J.H.; Massarani, L. Rethinking social amplification of risk: Social media and Zika in three languages. Risk Anal. 2018, 38, 2599–2624. [Google Scholar] [CrossRef] [Green Version]
- Malecki, K.; Keating, J.A.; Safdar, N. Crisis communication and public perception of COVID-19 risk in the era of social media. Clin. Infect. Dis. 2020, ciaa758. [Google Scholar] [CrossRef]
- Arguin, P.; Navin, A.; Steele, S.; Weld, L.; Kozarsky, P. Health communication during SARS. Emerg. Infect. Dis. 2004, 10, 377–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Túñez-López, M.; Vaz-Álvarez, M.; Fieiras-Ceide, C. Covid-19 and public service media: Impact of the pandemic on public television in Europe. El Prof. Inf. 2020, 29. [Google Scholar] [CrossRef]
- Harris, J.L.; Bargh, J.A.; Brownell, K.D. Priming effects of television food advertising on eating behavior. Health Psychol. 2009, 28, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Mastro, D.E.; Stern, S.R. Representations of race in television commercials: A content analysis of prime-time advertising. J. Broadcast. Electron. Media 2003, 47, 638–647. [Google Scholar] [CrossRef]
- Dixon, H.G.; Scully, M.L.; Wakefield, M.A.; White, V.M.; Crawford, D.A. The effects of television advertisements for junk food versus nutritious food on children’s food attitudes and preferences. Soc. Sci. Med. 2007, 65, 1311–1323. [Google Scholar] [CrossRef]
- Zimmerman, F.J.; Bell, J.F. Associations of television content type and obesity in children. Am. J. Public Health 2010, 100, 334–340. [Google Scholar] [CrossRef]
- Larson, R.J.; Schwartz, L.M.; Woloshin, S.; Welch, H.G. Advertising by academic medical centers. Arch. Intern. Med. 2005, 165, 645–651. [Google Scholar] [CrossRef] [Green Version]
- Brownfield, E.D.; Bernhardt, J.M.; Phan, J.L.; Williams, M.V.; Parker, R.M. Direct-to-consumer drug advertisements on network television: An exploration of quantity, frequency, and placement. J. Health Commun. 2004, 9, 491–497. [Google Scholar] [CrossRef] [Green Version]
- Kaphingst, K.A.; DeJong, W.; Rudd, R.E.; Daltroy, L.H. A content analysis of direct-to-consumer television prescription drug advertisements. J. Health Commun. 2004, 9, 515–528. [Google Scholar] [CrossRef]
- McCombs, M.E.; Shaw, D.L. The agenda-setting function of mass media. Public Opin. Q. 1972, 36, 176–187. [Google Scholar] [CrossRef]
- Lopez-Escobar, E.; Llamas, J.P.; McCombs, M.; Lennon, F.R. Two levels of agenda setting among advertising and news in the 1995 Spanish elections. Political Commun. 1998, 15, 225–238. [Google Scholar] [CrossRef]
- Roberts, M.; McCombs, M. Agenda setting and political advertising: Origins of the news agenda. Political Commun. 1994, 11, 249–262. [Google Scholar] [CrossRef]
- Kim, J.; Ragas, M.W.; Son, H.; Park, K.G.; Chung, Y.; Park, Y.E. Examining influence during a public health crisis: An analysis of the H1N1 outbreak from an agenda-building and agenda-setting perspective. J. Health Mass Commun. 2011, 3, 116–137. [Google Scholar]
- Gever, V.C.; Ezeah, G. The media and health education: Did Nigerian media provide sufficient warning messages on coronavirus disease? Health Educ. Res. 2020, 35, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Ley 7/2010, de 31 de Marzo, General de la Comunicación Audiovisual. BOE núm. 79, de 1 de abril de 2010, ref: BOE-A-2010-5292. Available online: https://www.boe.es/buscar/pdf/2010/BOE-A-2010-5292-consolidado.pdf (accessed on 19 November 2020).
- World Health Organization. The Selection and Use of Essential Medicines: Report of the WHO Expert Committee on Selection and Use of Essential Medicines, 2019 (Including the 21st WHO Model List of Essential Medicines and the 7th WHO Model List of Essential Medicines for Children); WHO Technical Report Series, No. 1021; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Igartua, J.J. Métodos Cuantitativos de Investigación en Comunicación; Bosch: Barcelona, Spain, 2006. [Google Scholar]
- Neuendorf, K.A. The Content Analysis Guidebook; Sage: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Lee, M.; Ohde, S.; Urayama, K.Y.; Takahashi, O.; Fukui, T. Weather and Health Symptoms. Int. J. Environ. Res. Public Health 2018, 15, 1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, F.; Léger, D.; Fressard, L.; Peretti-Watel, P.; Verger, P.; Coconel Group. Covid-19 health crisis and lockdown associated with high level of sleep complaints and hypnotic uptake at the population level. J. Sleep Res. 2020, e13119. [Google Scholar] [CrossRef]
- Jiménez-Sánchez, Á.; Margalina, V.-M.; Vayas-Ruiz, E. Governmental communication and brand advertising during the COVID-19 pandemic. Trípodos 2020, 2, 29–46. [Google Scholar]
- Tysiąc-Miśta, M.; Dziedzic, A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 4703. [Google Scholar] [CrossRef]
- Robinson, E.; Gillespie, S.; Jones, A. Weight-related lifestyle behaviours and the COVID-19 crisis: An online survey study of UK adults during social lockdown. Obes. Sci. Pract. 2020, 6, 735–740. [Google Scholar] [CrossRef]






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Classification | Health Subclassification |
|---|---|
| Food and non-alcoholic beverages | |
| Alcoholic beverages | |
| Clothing and footwear | |
| Housing, water, electricity, gas and other fuels | |
| Furnishings, household equipment and routine household maintenance | |
| Health | Slimming products |
| Analgesic and anti-inflammatory products | |
| Antacids | |
| Contraceptives | |
| Antihistamine products | |
| Antibiotics, anti-fungal and other anti-infective products | |
| Antipyretic | |
| Antitussive, mucolytic or anti-flu products | |
| Vitamin supplements | |
| Medical creams and sprays | |
| Laxatives and antidiarrheal products | |
| Homeopathic products | |
| Throat lozenges | |
| Sleeping pills and other sleeping treatments | |
| Other drugs and medical or pharmaceutical products | |
| Facemasks, gloves and hydrogels | |
| Therapeutic equipment | |
| Other medical products | |
| Medical or hospital services | |
| Dental services and clinics | |
| Paramedical services | |
| Private health insurance | |
| Care homes | |
| Residential care and assistance | |
| Other medical or aid services | |
| PSAs by public institutions | |
| PSAs by private institutions | |
| Transport | |
| Communication | |
| Recreation and culture | |
| Education | |
| Restaurants and hotels | |
| Miscellaneous goods and services |
| Variable | Cohen’s Kappa | Krippendorff’s Alpha |
|---|---|---|
| General classification | 0.781 | 0.781 |
| Health subclassification | 0.813 | 0.813 |
| Average | 0.797 | 0.797 |
| Category | Frequency | Percentage |
|---|---|---|
| Miscellaneous goods and services | 49,880 | 26.0 |
| Food and non-alcoholic beverages | 43,027 | 22.4 |
| Recreation and culture | 29,853 | 15.6 |
| Health | 29,312 | 15.3 |
| Furnishings, household equipment and routine household maintenance | 13,500 | 7.0 |
| Transport | 8093 | 4.2 |
| Communication | 7511 | 3.9 |
| Restaurants and hotels | 3570 | 1.9 |
| Housing, water, electricity, gas and other fuels | 2378 | 1.2 |
| Clothing and footwear | 2283 | 1.2 |
| Alcoholic beverages | 1672 | 0.9 |
| Education | 659 | 0.3 |
| Total | 191,738 | 100.0 |
| Category | Frequency | Percentage |
|---|---|---|
| Non-health advertisements | 162,426 | 84.7 |
| PSAs by public institutions | 8574 | 4.5 |
| Medical creams and sprays | 3170 | 1.7 |
| Dental services and clinics | 3064 | 1.6 |
| Other drugs and medical or pharmaceutical products | 1969 | 1.0 |
| Antitussive, mucolytic or anti-flu products | 1756 | 0.9 |
| Therapeutic equipment | 1597 | 0.8 |
| Analgesic and anti-inflammatory products | 1249 | 0.7 |
| Vitamin supplements | 1208 | 0.6 |
| Sleeping pills and other sleeping treatments | 1170 | 0.6 |
| PSAs by private institutions | 1006 | 0.5 |
| Laxatives and antidiarrheal products | 946 | 0.5 |
| Antacids | 786 | 0.4 |
| Throat lozenges | 752 | 0.4 |
| Slimming products | 703 | 0.4 |
| Private health insurance | 403 | 0.2 |
| Paramedical services | 306 | 0.2 |
| Medical or hospital services | 226 | 0.1 |
| Facemasks, gloves and hydrogels | 202 | 0.1 |
| Antihistamine products | 103 | 0.1 |
| Residential care and assistance | 56 | 0.0 |
| Contraceptives | 40 | 0.0 |
| Other medical or aid services | 26 | 0.0 |
| Antibiotics, anti-fungal and other anti-infective products | 0 | 0.0 |
| Antipyretic | 0 | 0.0 |
| Homeopathic products | 0 | 0.0 |
| Other medical products | 0 | 0.0 |
| Care homes | 0 | 0.0 |
| Total | 191,738 | 100.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanco-Herrero, D.; Gallardo-Camacho, J.; Arcila-Calderón, C. Health Advertising during the Lockdown: A Comparative Analysis of Commercial TV in Spain. Int. J. Environ. Res. Public Health 2021, 18, 1054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031054
Blanco-Herrero D, Gallardo-Camacho J, Arcila-Calderón C. Health Advertising during the Lockdown: A Comparative Analysis of Commercial TV in Spain. International Journal of Environmental Research and Public Health. 2021; 18(3):1054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031054
Chicago/Turabian StyleBlanco-Herrero, David, Jorge Gallardo-Camacho, and Carlos Arcila-Calderón. 2021. "Health Advertising during the Lockdown: A Comparative Analysis of Commercial TV in Spain" International Journal of Environmental Research and Public Health 18, no. 3: 1054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031054