
Systematic Review of Therapeutic Physical Exercise in Patients with Amyotrophic Lateral Sclerosis over Time


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
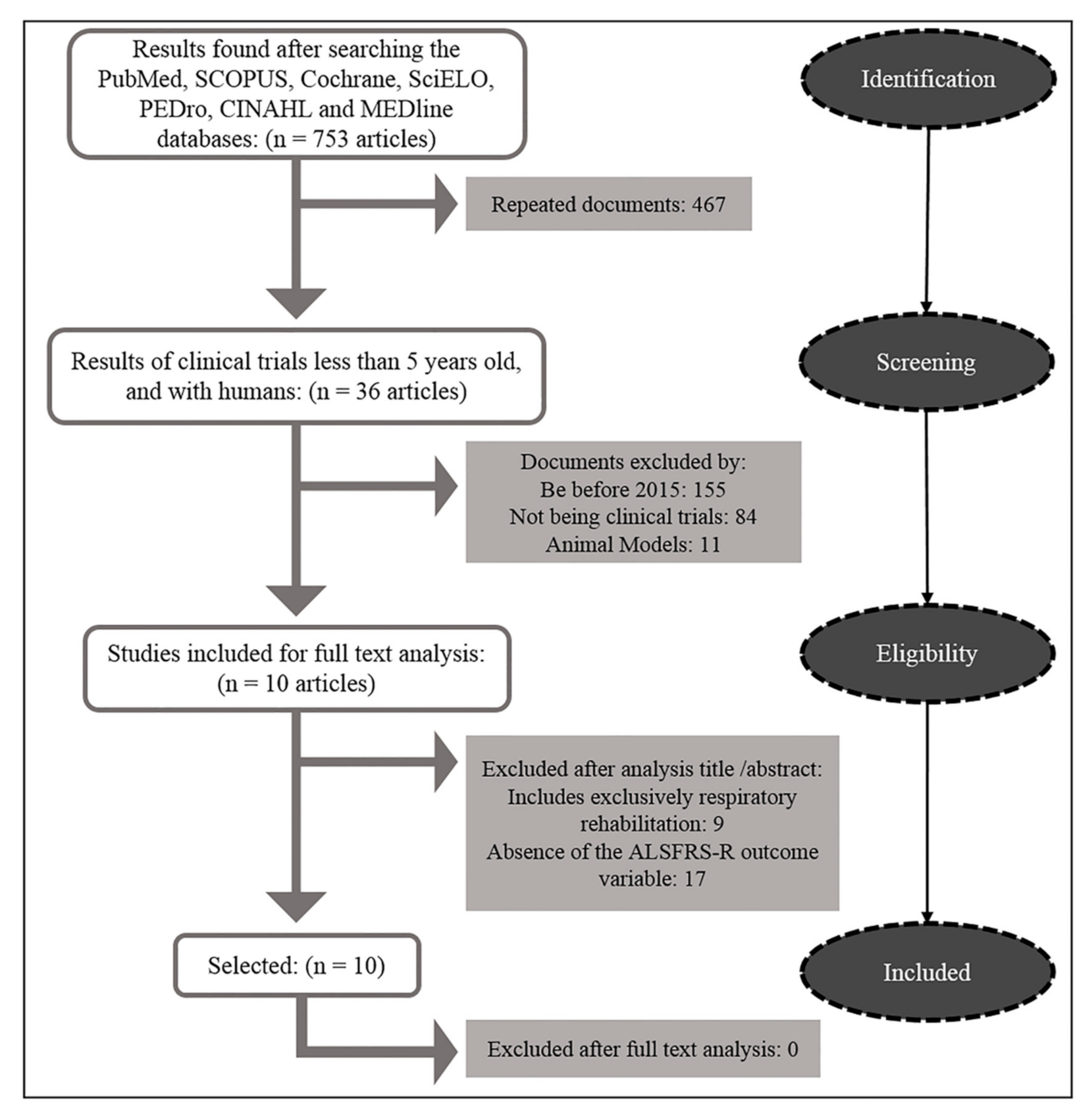
2.1. Search Strategy
2.2. Selection Method
2.3. Selection of Documents
2.4. Evaluation of the Internal Validity of the Selected Documents
3. Results
4. Discussion
4.1. Short-Term Effects
4.2. Medium-Term Effects
4.3. Long-Term Effects
4.4. Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Brown, D.G.; Shorter, J.; Wobst, H.J. Emerging small-molecule therapeutic approaches for amyotrophic lateral sclerosis and frontotemporal dementia. Bioorganic. Med. Chem. Lett. 2020, 30, 126942. [Google Scholar] [CrossRef] [PubMed]
- Orient-López, F.; Terré-Boliart, R.; Guevara-Espinosa, D.; Bernabeu-Guitart, M. Tratamiento neurorrehabilitador de la esclerosis lateral amiotrófica. Rev. Neurol. 2006, 43, 549–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abril Carreres, M.; Ticó Falguera, N.; Garreta Figuera, R. Enfermedades neurodegenerativas. Rehabilitación 2004, 38, 318–324. [Google Scholar] [CrossRef]
- Khan, F.; Turner-Stokes, L.; Ng, L.; Kilpatrick, T. Multidisciplinary rehabilitation for adults with multiple sclerosis (Review). Cochrane Libr. 2007, 18, CD006036. [Google Scholar]
- Arpa Gutiérrez, J.; Enseñat Cantallops, A.; García Martínez, A.; Gastón Zubimendi, I.; Guerrero Sola, A.; Juan García, F.J.; Martínez Martín, M.L.; Montero Orozco, C.; Pascual Calvet, J.; Povedano Panadés, M.; et al. Guía para la Atención de la Esclerosis Lateral Amiotrófica (ELA) en España. Available online: http://www.elaandalucia.es/WP/wp-content/uploads/guia-para-la-atencion-de-la-ela-en-espana.pdf (accessed on 15 June 2020).
- Salas Campos, T.; Rodríguez-Santos, F.; Esteban, J.; Vázquez, P.C.; Pardina, J.S.M.; Carmona, A.C. Spanish adaptation of the revised Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R). Amyotroph. Lateral Scler. 2010, 11, 475–477. [Google Scholar] [CrossRef]
- Kato, N.; Hashida, G.; Konaka, K. Effect of muscle strengthening exercise and time since onset in patients with amyotrophic lateral sclerosis: A 2-patient case series study. Medicine 2018, 97, 1–4. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elikins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques Braga, A.C.; Pinto, A.; Pinto, S.; de Carvalho, M. The role of moderate aerobic exercise as determined by cardiopulmonary exercise testing in ALS. Neurol. Res. Int. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zucchi, E.; Vinceti, M.; Malagoli, C.; Fini, N.; Gessani, A.; Fasano, A.; Rizzi, R.; Sette, E.; Cavazza, S.; Fiocchi, A.; et al. High-frequency motor rehabilitation in amyotrophic lateral sclerosis: A randomized clinical trial. Ann. Clin. Transl. Neurol. 2019, 6, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Merico, A.; Cavinato, M.; Gregorio, C.; Lacatena, A.; Gioia, E.; Piccione, F.; Angelini, C. Effects of combined endurance and resistance training in Amyotrophic Lateral Sclerosis: A pilot, randomized, controlled study. Eur. J. Transl. Myol. 2018, 28, 132–140. [Google Scholar]
- Ferri, A.; Lanfranconi, F.; Corna, G.; Bonazzi, R.; Marchese, S.; Magnoni, A.; Tremolizzo, L. Tailored exercise training counteracts muscle disuse and attenuates reductions in physical function in individuals with amyotrophic lateral sclerosis. Front. Physiol. 2019, 10, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clawson, L.L.; Cudkowicz, M.; Krivickas, L.; Brooks, B.R.; Sanjak, M.; Allred, P.; Atassi, N.; Swartz, A.; Steinhorn, G.; Uchil, A.; et al. A randomized controlled trial of resistance and endurance exercise in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Front. Degener. 2017, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kitano, K.; Asakawa, T.; Kamide, N.; Yorimoto, K.; Yoneda, M.; Kikuchi, Y.; Sawada, M.; Komori, T. Effectiveness of home-based exercises without supervision by physical therapists for patients with early-stage amyotrophic lateral sclerosis: A pilot study. Arch. Phys. Med. Rehabil. 2018, 99, 2114–2117. [Google Scholar] [CrossRef] [PubMed]
- Lunetta, C.; Lizio, A.; Sansone, V.A.; Cellotto, N.M.; Maestri, E.; Bettinelli, M.; Gatti, V.; Melazzini, M.G.; Meola, G. Massimo CorboStrictly monitored exercise programs reduce motor deterioration in ALS: Preliminary results of a randomized controlled trial. J. Neurol. 2016, 263, 52–60. [Google Scholar] [CrossRef]
- Sivaramakrishnan, A.; Madhavan, S. Recumbent stepping aerobic exercise in amyotrophic lateral sclerosis: A pilot study. Neurol. Sci. 2019, 40, 971–978. [Google Scholar] [CrossRef]
- van Groenestijn, A.C.; Schröder, C.D.; van Eijk, R.P.; Veldink, J.H.; Kruitwagen-van Reenen, E.T.; Groothuis, J.T.; Grupstra, H.F.; Tepper, M.; van Vliet, R.O.; Visser-Meily, J.M.A.; et al. Aerobic exercise therapy in ambulatory patients with ALS: A randomized controlled trial. Neurorehabil. Neural Repair 2019, 33, 153–164. [Google Scholar] [CrossRef]
- Kato, N.; Hashida, G.; Kobayashi, M.; Konaka, K. Physical therapy improves lower limb muscle strength but not function in individuals with amyotrophic lateral sclerosis: A case series study. Ann. Phys. Rehabil. Med. 2018, 61, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez de Rivera, F.; Oreja Guevara, C.; Sanz Gallego, I.S.; Valiente, B.S.J.; Recuerda, A.S.; Mendieta, M.A.G.; Arpa, J.; Tejedor, E.D. Evolución de pacientes con esclerosis lateral amiotrófica atendidos en una unidad multidisciplinar. Neurología 2011, 26, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, R.; Martínez-Muriana, A.; Leiva, T.; Gregorio, D.; Ariza, L.; Morell, M.; Esteban-Pérez, J.; García-Redondo, A.; Calvo, A.C.; Atencia-Cibreiro, G.; et al. Neuregulin-1 promotes functional improvement by enhancing collateral sprouting in SOD1G93A ALS mice and after partial muscle denervation. Neurobiol. Dis. 2016, 95, 168–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latimer-Cheung, A.E.; Pilutti, L.A.; Hicks, A.L.; Ginis, K.A.M.; Fenuta, A.M.; MacKibbon, K.A.; Motl, R.W. Effects of exercise training on fitness, mobility, fatigue, and health-related quality of life among adults with multiple sclerosis: A systematic review to inform guideline development. Arch. Phys. Med. Rehabil. 2013, 94, 1800–1828. [Google Scholar] [CrossRef]
- Dal Bello-Haas, V. Physical therapy for individuals with amyotrophic lateral sclerosis: Current insights. Degener. Neurol. Neuromuscul. Dis. 2018, 8, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shefner, J.M. Effects of Strength Training in Amyotrophic Lateral Sclerosis: How Much Do We Know? Muscle Nerve 2019, 59, 6–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuesta-Vargas, A.I.; White, M.; González-Sánchez, M.; Kuisma, R. The optimal frequency of aquatic physiotherapy for individuals with chronic musculoskeletal pain: A randomised controlled trial. Disabil. Rehabil. 2015, 37, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Zaragoza Casterad, J.; Serrano Ostariz, E.; Generelo Lanaspa, E. Dimensiones de la condición física saludable: Evolución según edad y género. Rev. Int. Med. Cienc. Act. Física Del Deport 2005, 5, 50–67. [Google Scholar]
- Alves, W.M.; Alves, T.G.; Ferreira, R.M.; Lima, T.A.; Pimentel, C.P.; Sousa, E.C.; Abrahin, O.; Alves, E.A. Strength training improves the respiratory muscle strength and quality of life of elderly with Parkinson disease. J. Sports Med. Phys Fitness 2019, 59, 1756–1762. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.H.; Chen, H.C.; Liou, T.H.; Li, W.; Chen, S.-S. Exercise Interventions for Individuals with Neurological Disorders: A Systematic Review of Systematic Reviews. Am. J. Phys. Med. Rehabil. 2019, 98, 921–930. [Google Scholar] [CrossRef]
- Lisle, S.; Tennison, M. Amyotrophic lateral sclerosis: The role of exercise. Curr. Sports Med. Rep. 2015, 14, 45–46. [Google Scholar] [CrossRef]
- Lopes de Almeida, J.P.; Silvestre, R.; Pinto, A.C.; de Carvalho, M. Exercise and amyotrophic lateral sclerosis. Neurol. Sci. 2012, 33, 9–15. [Google Scholar] [CrossRef]
- Ferreira, G.D.; Costa, A.C.C.; Plentz, R.D.; Coronel, C.C.; Sbruzzi, G. Respiratory training improved ventilatory function and respiratory muscle strength in patients with multiple sclerosis and lateral amyotrophic sclerosis: Systematic review and meta-analysis. Physiotherapy 2016, 102, 221–228. [Google Scholar] [CrossRef]
- Stroud, N.M.; Minahan, C.L. The impact of regular physical activity on fatigue, depression and quality of life in persons with multiple sclerosis. Health Qual. Life Outcomes 2009, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Orsini, M.; Hasue, R.H.; Leite, M.A.A.; de Menezes, S.L.L.; Silva, J.G.; Oliveira, A.B. Neuromuscular diseases: Revisiting the ‘overtraining’. Fisioter Pesqui 2014, 21, 101–102. [Google Scholar] [CrossRef] [Green Version]
- Kristensen, R.; Bostock, H.; Tan, S.V.; Witt, A.; Fuglsang-Frederiksen, A.; Qerama, E.; Andersen, H.; Tankisi, H. MScanFit motor unit number estimation (MScan)and muscle velocity recovery cycle recordings in amyotrophic lateral sclerosis patients. Clin. Neurophysiol. 2019, 130, 1280–1288. [Google Scholar] [CrossRef] [PubMed]
- Barros, G.; Moreira, I.; Ríos, R. Tratamiento–rehabilitación y manejo global de las enfermedades neuromusculares. Rev. Médica Clínica Las Condes 2018, 29, 560–569. [Google Scholar] [CrossRef]
- Hernández-Vázquez, F.J. El deporte para atender la diversidad: Deporte adaptado y deporte inclusivo. Apunt Educ. Física Deport 2000, 2, 46–53. [Google Scholar]


{kind=link}
| Authors | Type of Study | Randomization | Masked | Variable at Startup | Blinded Subjects | Blinded Therapists | Blinded Evaluators | Measures 85% of the Sample | Intention to Treat Analysis | Main Outcome Variables | Mean or Standard Deviation | PEDro Points |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Marques Braga et al., (2018) [9] | ECA | ● | - | ● | - | - | - | - | ● | ● | ● | 5 |
| Kitano et al., (2018) [14] | EC | - | - | ● | - | - | - | ● | ● | ● | ● | 5 |
| Sivaramakrishnan et al., (2019) [16] | EC | - | - | ● | - | - | - | ● | ● | ● | ● | 5 |
| Clawson et al., (2017) [13] | ECA | ● | - | - | - | - | ● | ● | ● | ● | ● | 6 |
| Kato et al., (2018) [5] | EC | - | - | ● | - | - | - | ● | ● | ● | ● | 5 |
| Van Groenestijn et al., (2019) [17] | ECA | ● | - | ● | - | - | ● | ● | ● | ● | ● | 7 |
| Ferri et al., (2019) [12] | ECA | ● | - | ● | - | - | - | ● | ● | ● | ● | 6 |
| Merico et al., (2018) [11] | ECA | ● | - | ● | - | - | ● | - | ● | ● | ● | 6 |
| Zucchi et al., (2019) [10] | ECA | ● | - | ● | - | - | ● | ● | ● | ● | ● | 7 |
| Lunetta et al., (2015) [15] | ECA | ● | - | ● | - | - | ● | - | ● | ● | ● | 6 |
| Author | Sample Size | Age (Years) | ALS Time | Intervention | Session Frequency | Outcome Variables |
|---|---|---|---|---|---|---|
| Marques Braga et al., (2018) [9] | 50 (48) G1 = SC: 25 (24) G2 = AECI: 25 (24) | G1: 63 (±13.0) G2: 62 (±12.0) | G1 = SC: 9.5 months G2 = AECI: 9 months | G1 AECI: Aerobic exercise of controlled and moderate intensity + SC G2 SC: Standard care (ROM + Gear) | G1: AECI (2 sessions/week) + daily SC—6 months G2: daily SC—6 months | ALSFRS-R CPET FVC, FSS |
| Kitano et al., (2018) [14] | 105 G1 = Home-ex: 21 (15) G2 = Control: 84 | G1: 62.8 (±10.2) G2: 62.7 (±12.1) | G1: 2.2 (±2.4) years G2: 1.5 (±1.7) years | Strength, functional and stretching exercises for upper limbs and trunk muscles | Daily/individualized frequency for 6 months. G1 = unsupervised | ALSFRS-R MMT |
| Sivaramakrishnan et al., (2019) [16] | 9 G1 = Aerobic G: 9 | G1: 59.22 (±12.3) | G1: 2.37 (±1.9) years | Reclining stepped aerobic exercise of moderate intensity. 70 steps/minute. | 40 min. 3 sessions a week. For 4 weeks. | ALSFRS-R 6MWD, TUG FSS, SF-12, BDI |
| Clawson et al., (2017) [13] | 59 G1 = ROM: 21 G2 = RESISTANCE: 18 G3 = ENDURANCE: 20 | G1: 57.68 (±9.72) G2: 63.65 (±10.55) G3: 57.82 (±11.88) | G1: 11.08 (±13.21) G2: 7.25 (±7.21) G3: 7.30 (±6.80) months | G1: Held stretches (30 s) G2: strength exercises (70% RM) G3: moderate/high intensity resistance exercises. | 3 sessions a week. For 6 months. | ALSFRS-R FVC, FSS ASS, VAS VO2 MÁX |
| Kato et al., (2018) [5] | 2 G1 = Strength G: 2 | G1: 56 (±8) | G1: 1.1 (±0.5) years | Moderate/high intensity strength and endurance exercises. | 30 min. 7 sessions a week, For 2 weeks. | ALSFRS-R KEMS, FVC FAC |
| Van Groenestijn et al., (2019) [17] | 57 (32) G1 = AET: 27 (10) G2 = UC: 30 (22) | G1: 60.9 (±10) G2: 59.9 (±10.7) | G1: 15.5 (±10.9) G2: 18 (±14.0) months | G1 AET: Aerobic exercise therapy in cycle ergometer + UC G2 UC: usual care | 50 min. 3 sessions a week. For 16 weeks. | ALSFRS-R ALSAQ-40+FS-36 MCS, PCS, FVC |
| Ferri et al., (2019) [12] | 16 G1= TRAIN: 8 G2= UC: 8 | G1: 50.7 (±3.3) G2: 55.5 (±5.95) | G1: 20.5 (±20.3) G2: 13.4 (±6.6) months | G1 TRAIN: Moderate/high intensity aerobic and strength exercise. G2 UC: usual care | 50 min. 3 sessions a week. For 12 weeks. | ALSFRS-R 6MWD, TUG VO2 MAX, Mc GILL |
| Merico et al., (2018) [11] | 38 G1 = EP: 23 G2 = SNT: 15 | G1: 61.6 (±10.6) G2: 59.8 (±14.7) | G1: 30.2 (±11.8) G2: 30.3 (±6.7) months | G1 EP: Submaximal aerobic exercise 65% HR and 80% strength RM G2 SNT: neuromotor standard exercise | 50 min. 7 sessions a week. For 5 weeks. | ALSFRS-R 6MWT, FIM, CK FSS, VO2 MAX |
| Zucchi et al., (2019) [10] | 65 G1 = IER: 32 G2 = UER: 33 | G1: 65.14 (±9.90) G2: 64.74 (±10.10) | G1: 15.67 (±9.74) G2: 16.64 (±8.98) months | G1: High frequency aerobic and resistance training. G2: Aerobic exercise, low frequency. | 45 min. G1: 5/week and G2: 2/week For 10 weeks. | ALSFRS-R FVC FSS ALSAQ-40 + Mc GILL |
| Lunetta et al., (2015) [15] | 60 (47) G1 = SMEP: 30 (22) G2 = UCP: 30 (25) | G1: 61.1 (±10.1) G2: 60.3 (±9.9) | G1: 15.2 (±7.2) G2: 13.7 (±6.1) months | G1 SMEP: passive, active and cycle ergometer exercises, strictly supervised. G2 UCP: passive habitual care. | G1: and G2: 2/week For 6 months. | ALSFRS-R FVC |
| Variable | Author | Baseline (SD) | Short-Term (1 Month) | Medium-Term (3 Months) | Long-Term (6 Months) | |
|---|---|---|---|---|---|---|
| ALSFRS-R(0–48) | Marques Braga et al. (2018) [9] | Cases | 40.25 (±5.00) | - | - | 34.1 (±7.1) |
| Control | 37.25 (±4.9) | - | - | 29.5 (±7.7) | ||
| Kitano et al. (2018) [14] | Cases | 41.1 (±4.5) | - | - | 38.1 (±5.9) | |
| Control | 40.3 (±4.4) | - | - | 33.1 (±9.2) | ||
| Sivaramakrishnan et al. (2019) [16] | Cases | 32.75 (±7) | 33.25 (±7.55) | 32.62 (±7.4) | - | |
| Control | 32.75 (±7) | - | - | - | ||
| Clawson et al. (2017) [13] | Cases | 39.36 (±4.92) | - | - | 35.41 (±1.26) | |
| Control | 39.67 (±3.71) | - | - | 33.54 (±1.38) | ||
| Kato et al. (2018) [5] | Cases | 43 (±2) | - | - | 37.5 (±1) | |
| Control | 43 (±2) | - | - | - | ||
| Van Groenestijn et al. (2019) [17] | Cases | 42.4 (±4.3) | - | 40.52 (±3.48) | - | |
| Control | 42.2 (±3) | - | 38.28 (±5.52) | - | ||
| Ferri et al. (2019) [12] | Cases | 40.4 (±1.5) | - | 35.7 (±2.6) | - | |
| Control | 35 (±3.4) | - | 23 (±5.6) | - | ||
| Merico et al. (2018) [11] | Cases | 36.1 (±4.71) | 36.1 (±4.71) | - | - | |
| Control | 34.5 (±3.6) | 34.5 (±3.6) | - | - | ||
| Zucchi et al. (2019) [10] | Cases | 39.84 (±5.7) | - | 34.87 (±8.49) | 33.08 (±9.76) | |
| Control | 40.15 (±5.17) | - | 36.39 (±8.01) | 33.0 (±9.42) | ||
| Lunetta et al. (2015) [15] | Cases | 39.1 (±4.7) | 37.0 (±5.1) | 35.1 (±6.2) | 32.8 (±6.5) | |
| Control | 38.3 (±5.1) | 38.1 (±4.3) | 34.3 (±6.4) | 28.7 (±7.5) | ||
| Variable | Study | Baseline | End of Study | |||
|---|---|---|---|---|---|---|
| 1 Month | 3 Months | 6 Months | ||||
| FVC (%) | Clawson LL et al. (2017) [13] | Cases | 88.14 (±11.03) | - | - | 74.34 |
| Control | 91.19 (±77.9) | - | - | 88.59 | ||
| Lunetta et al. (2015) [15] | Cases | 92.5 (±23.3) | - | - | 75.8 (±23.6) | |
| Control | 93.9 (±14.7) | - | - | 66.5 (±26.9) | ||
| Kato et al. (2018) [5] | Cases | 69.05 | - | - | 72.2 | |
| Van Groenestijn et al. (2019) [17] | Cases | 86.9 (±20.2) | - | 79.22 | - | |
| Control | 95.4 (±15.4) | - | 81.88 | - | ||
| Zucchi et al. (2019) [10] | Cases | 91.88 (±18.98) | - | - | 66.24 (±44.96) | |
| Control | 90.70 (±17.68) | - | - | 77.91 (±31.82) | ||
| FSS (1–7) | Sivaramakrishnan et al. (2019) [16] | Cases | 32.87 (±10.45) ÷ 9 | 28.62 (±11.9) ÷9 | - | - |
| Merico et al. (2018) [11] | Cases | 5.4 (±0.27) | 6.69 (±0.21) | - | ||
| Control | 5.4 (±0.2) | 5.19 (±0.16) | - | - | ||
| Zucchi et al. (2019) [10] | Cases | 35.63 (±15.31) ÷ 9 | - | - | 41.42 (±18.49) ÷ 9 | |
| Control | 36.50 (±16.53) ÷ 9 | - | - | 37.38 (±18.73) ÷ 9 | ||
| 6MWD (metros) | Sivaramakrishnan et al. (2019) [16] | Cases | 232.5 (±192.32) | 235.16 (±195.49) | - | - |
| Merico et al. (2018) [11] | Cases | 265.17 (±81.37) | 336.73 (±50.72) | - | - | |
| Control | 236.26 (±76.26) | 239.16 (±5.48) | - | - | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega-Hombrados, L.; Molina-Torres, G.; Galán-Mercant, A.; Sánchez-Guerrero, E.; González-Sánchez, M.; Ruiz-Muñoz, M. Systematic Review of Therapeutic Physical Exercise in Patients with Amyotrophic Lateral Sclerosis over Time. Int. J. Environ. Res. Public Health 2021, 18, 1074. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031074
Ortega-Hombrados L, Molina-Torres G, Galán-Mercant A, Sánchez-Guerrero E, González-Sánchez M, Ruiz-Muñoz M. Systematic Review of Therapeutic Physical Exercise in Patients with Amyotrophic Lateral Sclerosis over Time. International Journal of Environmental Research and Public Health. 2021; 18(3):1074. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031074
Chicago/Turabian StyleOrtega-Hombrados, Laura, Guadalupe Molina-Torres, Alejandro Galán-Mercant, Eduardo Sánchez-Guerrero, Manuel González-Sánchez, and María Ruiz-Muñoz. 2021. "Systematic Review of Therapeutic Physical Exercise in Patients with Amyotrophic Lateral Sclerosis over Time" International Journal of Environmental Research and Public Health 18, no. 3: 1074. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031074