
IL-17F Gene rs763780 and IL-17A rs2275913 Polymorphisms in Patients with Periodontitis

 , and
, and
Abstract
:1. Introduction
2. Material and methods
2.1. Study Subjects
2.2. Periodontal Examination
2.3. Genotyping
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
List of Abbreviations
References
- Kinane, D.F.; Peterson, M.; Stathopoulou, P.G. Environmental and other modifying factors of the periodontal diseases. Periodontology 2000 2006, 40, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Polizzi, A.; Alibrandi, A.; Williams, R.C.; Leonardi, R. Independent impact of periodontitis and cardiovascular disease on elevated soluble urokinase-type plasminogen activator receptor (suPAR) levels. J. Periodontol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Polizzi, A.; Patini, R.; Ferlito, S.; Alibrandi, A.; Palazzo, G. Association among serum and salivary A. actinomycetemcomitans specific immunoglobulin antibodies and periodontitis. BMC Oral Health 2020, 20, 283. [Google Scholar] [CrossRef] [PubMed]
- Sandros, J.; Karlsson, C.; Lappin, D.F.; Madianos, P.N.; Kinane, D.F.; Papapanou, P.N. Cytokine responses of oral epithelial cells to Porphyromonas gingivalis infection. J. Dent. Res. 2000, 79, 1808–1814. [Google Scholar] [CrossRef]
- Di Benedetto, A.; Gigante, I.; Colucci, S.; Grano, M. Periodontal disease: Linking the primary inflammation to bone loss. Clin. Dev. Immunol. 2013, 2013, 503754. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Lo Giudice, A.; Polizzi, A.; Alibrandi, A.; Murabito, P.; Indelicato, F. Identification of the different salivary Interleukin-6 profiles in patients with periodontitis: A cross-sectional study. Arch. Oral Biol. 2020, 122, 104997. [Google Scholar] [CrossRef]
- Mitani, A.; Niedbala, W.; Fujimura, T.; Mogi, M.; Miyamae, S.; Higuchi, N.; Abe, A.; Hishikawa, T.; Mizutani, M.; Ishihara, Y.; et al. Increased expression of interleukin (IL)-35 and IL-17, but not IL-27, in gingival tissues with chronic periodontitis. J. Periodontol. 2015, 86, 301–309. [Google Scholar] [CrossRef]
- Cheng, W.C.; van Asten, S.D.; Burns, L.A.; Evans, H.G.; Walter, G.J.; Hashim, A.; Hughes, F.J.; Taams, L.S. Periodontitis-associated pathogens P. gingivalis and A. actinomycetemcomitans activate human CD14+ monocytes leading to enhanced Th17/IL-17 responses. Eur J. Immunol. 2016, 46, 2211–2221. [Google Scholar] [CrossRef] [Green Version]
- Giannopolou, C.; Cappuyns, I.; Mombelli, A. Effect of smoking on gingival crevicular fluid cytokine profile during experimental gingivitis. J. Clin. Periodontol. 2003, 30, 996–1002. [Google Scholar] [CrossRef]
- Persson, L.; Bergstrom, J.; Gustafsson, A. The effect of tobacco smoking on neutrophil activity following periodontal surgery. J. Periodontol. 2003, 74, 1475–1482. [Google Scholar] [CrossRef]
- Renvert, S.; Dahlén, G.; Wikstrom, M. The clinical and microbiologicaleffects of non-surgical periodontal therapy in smokers and non-smokers. J. Clin. Periodontol. 1998, 25, 153–157. [Google Scholar] [PubMed]
- Persson, L.; Bergstrom, J.; Ito, H.; Gustafsson, A. Tobacco smoking and neutrophil activity in patients with periodontal disease. J. Periodontol. 2001, 72, 90–95. [Google Scholar] [PubMed]
- Giannopoulos, C.; Kamma, J.; Mombelli, A. Effect of inflammation, smoking and stress on gingival crevicular fluid level. J. Clin. Periodontol. 2003, 30, 145–153. [Google Scholar]
- Petropoulos, G.; McKay, I.; Hughes, F. The association between neutrophil numbers and interleukin-1á concentrations in gingival crevicular fluid of smokers and non-smokers with periodontal disease. J. Clin. Periodontol. 2004, 31, 390–395. [Google Scholar] [PubMed]
- Bergström, J. Tobacco smoking and chronic destructive periodontal disease. Odontology 2004, 92, 1–8. [Google Scholar]
- Cheng, W.C.; Hughes, F.J.; Taams, L.S. The presence, function and regulation of IL-17 and Th17 cells in periodontitis. J. Clin. Periodontol. 2014, 41, 541–549. [Google Scholar]
- Gaffen, S.L. Structure and signalling in the IL-17 receptor family. Nat. Rev. Immunol. 2009, 9, 556–567. [Google Scholar]
- Miossec, P.; Kolls, J.K. Targeting IL-17 and TH17 cells in chronic inflammation. Nat. Rev. Drug Discov. 2012, 11, 763–776. [Google Scholar]
- Zenobia, C.; Hajishengallis, G. Basic biology and role of interleukin-17 in immunity and inflammation. Periodontology 2000 2015, 69, 142–159. [Google Scholar]
- Gu, C.; Wu, L.; Li, X. IL-17 family: Cytokines, receptors and signaling. Cytokine 2013, 64, 477–485. [Google Scholar]
- Koenders, M.I.; Marijnissen, R.J.; Devesa, I.; Lubberts, E.; Joosten, L.A.; Roth, J.; van den Berg, W.B. Tumor necrosis factor-interleukin-17 interplay induces S100A8, interleukin- 1 β, and matrix metalloproteinases, and drives irreversible cartilage destruction in murine arthritis: Rationale for combination treatment during arthritis. Arthritis Rheum. 2011, 63, 2329–2339. [Google Scholar] [PubMed]
- Iyoda, M.; Shibata, T.; Kawaguchi, M.; Hizawa, N.; Yamaoka, T.; Kokubu, F.; Akizawa, T. IL-17A and IL-17F stimulate chemokines via MAPK pathways (ERK1/2 and p38 but not JNK) in mouse cultured mesangial cells: Synergy with TNF-alpha and IL-1beta. Am. J. Physiol. Renal. Physiol. 2010, 298, F779–F787. [Google Scholar] [CrossRef] [PubMed]
- Kozak, M.; Dabrowska-Zamojcin, E.; Mazurek-Mochol, M.; Pawlik, A. Cytokines and Their Genetic Polymorphisms Related to Periodontal Disease. J. Clin. Med. 2020, 14, 4045. [Google Scholar]
- Eerligh, P.; Koeleman, B.P.C.; Dudbridge, F.; Bruining, G.J.; Roep, B.O.; Giphart, M.J. Functional genetic polymorphisms in cytokines and metabolic genes as additional genetic markers for susceptibility to develop type 1 diabetes. Genes Immun. 2004, 5, 36–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dziedziejko, V.; Kurzawski, M.; Paczkowska, E.; Machalinski, B.; Pawlik, A. The impact of IL18 gene polymorphisms on mRNA levels and interleukin-18 release by peripheral blood mononuclear cells. Postepy. Hig. Med. Dosw. 2012, 20, 409–414. [Google Scholar] [CrossRef]
- Tang, H.; Pei, H.; Xia, Q.; Tang, Y.; Huang, J.; Huang, J.; Pei, F. Role of gene polymorphisms/haplotypes and serum levels of interleukin-17A in susceptibility to viral myocarditis. Mol. Biol. Rep. 2017, 44, 443–453. [Google Scholar]
- Nordang, G.B.N.; Viken, M.K.; Hollis-Moffatt, J.E.; Merriman, T.R.; Førre, Ø.T.; Helgetveit, K.; Kvien, T.K.; Lie, B.A. Association analysis of the interleukin 17A gene in Caucasian rheumatoid arthritis patients from Norway and New Zealand. Rheumatology 2009, 48, 367–370. [Google Scholar]
- Arisawa, T.; Tahara, T.; Shibata, T.; Nagasaka, M.; Nakamura, M.; Kamiya, Y.; Fujita, H.; Nakamura, M.; Yoshioka, D.; Arima, Y.; et al. The influence of polymorphisms of interleukin-17A and interleukin-17F genes on the susceptibility to ulcerative colitis. J. Clin. Immunol. 2008, 28, 44–49. [Google Scholar]
- Tolba, F.M.; Diab, S.M.; Abdelrahman, A.M.N.; Behairy, O.G.; Almonaem, E.R.A.; Mogahed, M.M.; Mohamed, S.A.-S. Assessment of IL-17F rs763780 gene polymorphism in immune thrombocytopenia. Blood Cells Mol. Dis. 2019, 75, 20–25. [Google Scholar]
- Liang, T.; Xu, Y.T.; Zhang, Y.; Cai, P.C.; Hu, L.H. Interleukin-17A and -17F single nucleotide polymorphisms associate with susceptibility of asthma in Chinese Han population. Hum. Immunol. 2018, 79, 736–742. [Google Scholar]
- Kaur, R.; Rawat, A.K.; Kumar, S.; Aadil, W.; Akhtar, T.; Narang, T.; Chopra, D. Association of genetic polymorphism of interleukin-17A & interleukin-17F with susceptibility of psoriasis. Indian J. Med. Res. 2018, 148, 422–426. [Google Scholar] [PubMed]
- Duarte, P.M.; Miranda, T.S.; Lima, J.A.; Dias Gonçalves, T.E.; Santos, V.R.; Bastos, M.F.; Ribeiro, F.V. Expression of immune-inflammatory markers in sites of chronic periodontitis in patients with type 2 diabetes. J. Periodontol. 2012, 83, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Behfarnia, P.; Birang, R.; Andalib, A.R.; Asadi, S. Comparative Evaluation of IFNγ, IL4 and IL17 Cytokines in Healthy Gingiva and Moderate to Advanced Chronic Periodontitis. Dent. Res. J. 2010, 7, 45–50. [Google Scholar]
- Saraiva, A.M.; Alves e Silva, M.R.M.; Correia Silva, J.d.F.; da Costa, J.E.; Gollob, K.J.; Dutra, W.O.; Moreira, P.R. Evaluation of IL17A expression and of IL17A, IL17F and IL23R gene polymorphisms in Brazilian individuals with periodontitis. Hum. Immunol. 2013, 74, 207–214. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, Y.; Yang, X.O.; Nurieva, R.I.; Chang, S.H.; Ojeda, S.S.; Kang, H.S.; Schluns, K.S.; Gui, J.; Jetten, A.M.; et al. Transcription of IL17 and IL17f is controlled by conserved noncoding sequence 2. Immunity 2012, 36, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S1–S8. [Google Scholar] [CrossRef]
- Johnson, R.B.; Wood, N.; Serio, F.G.; Johnson, R.B. Interleukin-11 and IL-17 and the pathogenesis of periodontal disease. J. Periodontol. 2004, 75, 7–43. [Google Scholar] [CrossRef]
- Stadler, A.F.; Angst, P.D.; Arce, R.M.; Gomes, S.C.; Oppermann, R.V.; Susin, C. Gingival crevicular fluid levels of cytokines/chemokines in chronic periodontitis: A meta-analysis. J. Clin. Periodontol. 2016, 43, 727–745. [Google Scholar] [CrossRef]
- Liukkonen, J.; Gürsoy, U.K.; Pussinen, P.J.; Suominen, A.L.; Könönen, E.; Liukkonen, J. Salivary Concentrations of Interleukin (IL)-1beta, IL-17A, and IL-23 Vary in Relation to Periodontal Status. J. Periodontol. 2016, 87, 1484–1491. [Google Scholar] [CrossRef]
- Honda, T.; Aoki, Y.; Takahashi, N.; Maekawa, T.; Nakajima, T.; Ito, H.; Tabeta, K.; Okui, T.; Kajita, K.; Domon, H. Elevated expression of IL-17 and IL-12 genes in chronic inflammatory periodontal disease. Clin. Chim. Acta 2008, 395, 137–141. [Google Scholar] [CrossRef]
- Chitrapriya, M.N.; Rao, S.R.; Lavu, V.; Chitrapriya, M.N. Interleukin-17 and interleukin-18 levels in different stages of inflammatory periodontal disease. J. Indian Soc. Periodontol. 2015, 19, 14–17. [Google Scholar] [PubMed]
- Cifcibasi, E.; Koyuncuoglu, C.; Ciblak, M.; Badur, S.; Kasali, K.; Firatli, E.; Cintan, S. Evaluation of Local and Systemic Levels of Interleukin-17, Interleukin-23, and Myeloperoxidase in Response to Periodontal Therapy in Patients with Generalized Aggressive Periodontitis. Inflammation 2015, 38, 1959–1968. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, J.D.; Madeira, M.F.M.; Resende, R.G.; Correia-Silva, J.D.F.; Gomez, R.S.; de Souza, D.d.G.; Teixeira, M.M.; Queiroz-Junior, C.M.; da Silva, T.A. Association between polymorphisms in interleukin-17A and -17F genes and chronic periodontal disease. Mediat. Inflamm. 2012, 2012, 846052. [Google Scholar] [CrossRef] [PubMed]
- Zacarias, J.M.; Sippert, E.Â.; Tsuneto, P.Y.; Visentainer, J.E.; de Oliveira e Silva, C.; Sell, A.M. The Influence of Interleukin 17A and IL17F Polymorphisms on Chronic Periodontitis Disease in Brazilian Patients. Mediat. Inflamm. 2015, 2015, 147056. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, H.L.; Warad, S.; Ashok, N.; Baroudi, K.; Tarakji, B. Association of Interleukin-17 polymorphism (-197G/A) in chronic and localized aggressive periodontitis. Braz. Oral Res. 2016, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, N.; Joseph, R.; Balan, S.; Arun, R.; Banerjee, M. Association of interleukin-4 and interleukin-17F polymorphisms in periodontitis in Dravidian ethnicity. Indian J. Hum. Genet. 2013, 19, 58–64. [Google Scholar] [PubMed] [Green Version]
- Borilova Linhartova, P.; Kastovsky, J.; Lucanova, S.; Bartova, J.; Poskerova, H.; Vokurka, J.; Fassmann, A.; Kankova, K.; Holla, L.I. Interleukin-17A Gene Variability in Patients with Type 1 Diabetes Mellitus and Chronic Periodontitis: Its Correlation with IL-17 Levels and the Occurrence of Periodontopathic Bacteria. Mediat. Inflamm. 2016, 2016, 2979846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, F.R.P.; Pessoa, L.D.S.; Vasconcelos, A.C.C.G.; de Aquino Lima, W.; Alves, E.H.P.; Vasconcelos, D.F.P. Polymorphisms in interleukins 17A and 17F genes and periodontitis: Results from a meta-analysis. Mol. Biol. Rep. 2017, 44, 443–453. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Controls | Periodontitis Patients | p-Value (Control vs. Periodontitis) | Controls (Smokers) | Periodontitis Patients (Smokers) | p-Value (Smokers: Control vs. Periodontitis) | Controls (Non-Smokers) | Periodontitis Patients (Non-Smokers) | p-Value (Non-Smokers: Control vs. Periodontitis) |
|---|---|---|---|---|---|---|---|---|---|
| SEX | 55/105 | 84/116 | 0.16 # | 12/22 | 30/40 | 0.53 # | 43/83 | 54/76 | 0.25 # |
| (M/F) | |||||||||
| AGE | 45.28 ± 10.15 | 49.85 ± 8.71 | p < 0.0001 * | 44.18 ± 10.21 | 48.94 ± 8.89 | p = 0.0036 * | 45.58 ± 10.15 | 50.33 ± 8.61 | p < 0.0001 * |
| (mean years ± SD) | |||||||||
| API % | 35.81 ± 20.66 | 72.98 ± 21.03 | p < 0.0001 * | 48.29 ± 25.35 | 83.03 ± 17.45 | p < 0.0001 * | 32.44 ± 17.88 | 68.42 ± 19.50 | p < 0.0001 * |
| (mean ± SD) | |||||||||
| SBI % | 6.53 ± 11.29 | 57.66 ± 25.45 | p < 0.0001 * | 6.56 ± 10.09 | 46.83 ± 25.27 | p < 0.0001 * | 6.52 ± 11.63 | 63.96 ± 22.93 | p < 0.0001 * |
| (mean ± SD) | |||||||||
| PPD mm | 1.63 ± 0.34 | 4.36 ± 1.19 | p < 0.0001 * | 1.74 ± 0.29 | 4.74 ± 1.17 | p < 0.0001 * | 1.60 ± 0.35 | 4.15 ± 1.16 | p < 0.0001 * |
| (mean ± SD) | |||||||||
| CAL mm | 0.41 ± 0.92 | 5.06 ± 1.55 | p < 0.0001 * | 0.54 ± 0.96 | 5.30 ± 1.73 | p < 0.0001 * | 0.37 ± 0.91 | 4.93 ± 1.43 | p < 0.0001 * |
| (mean ± SD) |
| Genotype/Allele | PD Patients | Control Group | pa | Compared Genotypes/Alleles | pb | OR (95%CI) | ||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | |||||
| IL-17F rs763780 | ||||||||
| genotype | ||||||||
| TT | 190 | 95.00% | 148 | 92.50% | 0.38 | |||
| TC | 10 | 5.00% | 12 | 7.50% | TC vs. TT | 0.38 | 0.65 (0.27–1.54) | |
| CC | 0 | 0.00% | 0 | 0.00% | ||||
| IL-17F rs763780 | ||||||||
| Allele | ||||||||
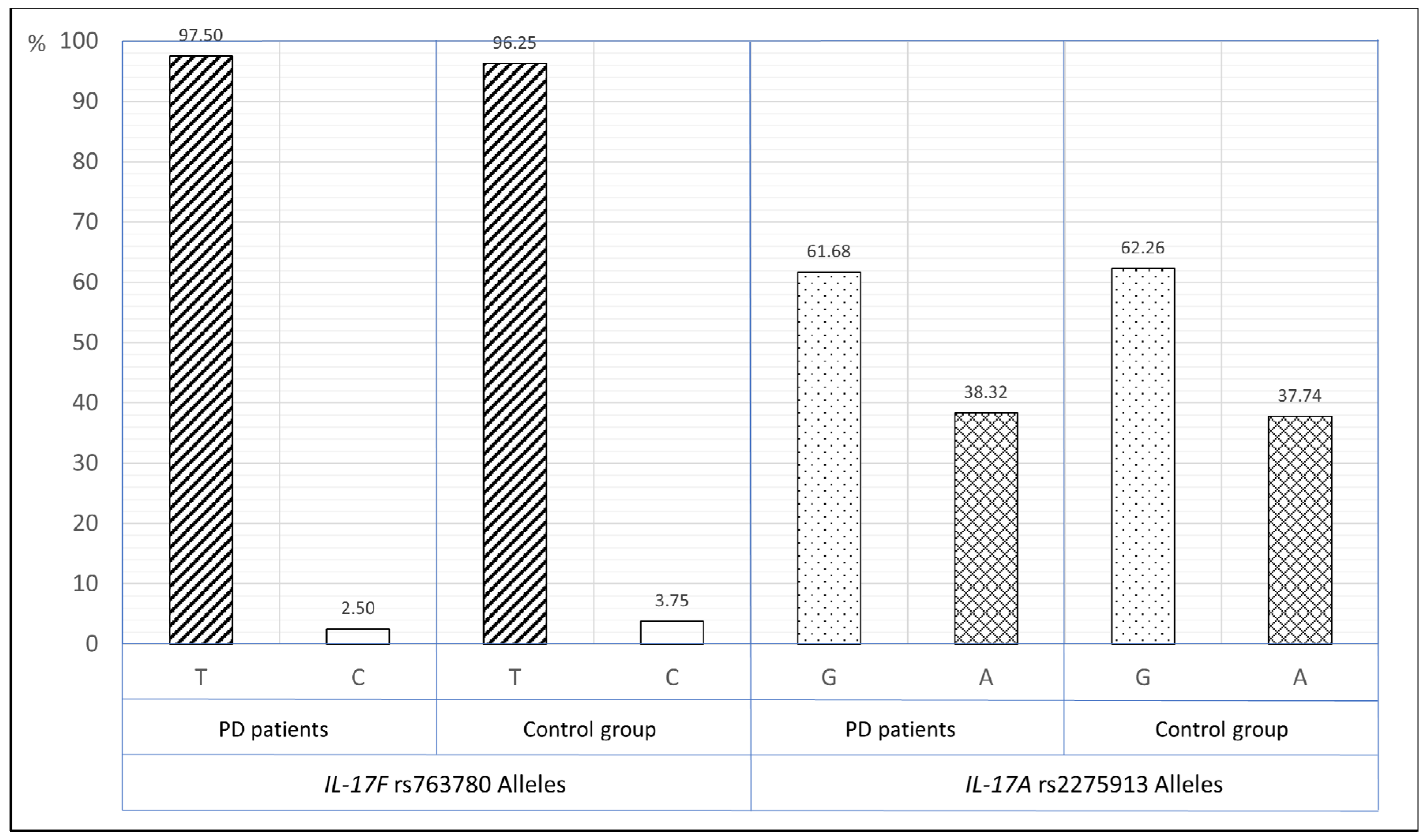
| T | 390 | 97.50% | 308 | 96.25% | ||||
| C | 10 | 2.50% | 12 | 3.75% | C vs. T | 0.39 | 0.66 (0.28–1.54) | |
| IL-17A rs2275913 | ||||||||
| genotype | ||||||||
| GG | 81 | 41.12% | 64 | 40.25% | 0.82 | AA + GA vs. GG | 0.91 | 0.97 (0.63–1.48) |
| GA | 81 | 41.12% | 70 | 44.03% | AA vs. GA + GG | 0.67 | 1.16 (0.66–2.03) | |
| AA | 35 | 17.76% | 25 | 15.72% | AA vs. GG | 0.76 | 1.11 (0.60–2.03) | |
| GA vs. GG | 0.73 | 0.91 (0.58–1.45) | ||||||
| AA vs. GA | 0.65 | 1.21 (0.66–2.22) | ||||||
| IL-17A rs2275913 | ||||||||
| Allele | ||||||||
| G | 243 | 61.68% | 198 | 62.26% | ||||
| A | 151 | 38.32% | 120 | 37.74% | A vs. G | 0.88 | 1.03 (0.76–1.39) | |
| Genotype/Allele | PD Patients | Control Group | pa | Compared Genotypes/Alleles | pb | OR (95%CI) | ||
|---|---|---|---|---|---|---|---|---|
| (Non-Smokers) | (Non-Smokers) | |||||||
| n | % | n | % | |||||
| IL-17F rs763780 | ||||||||
| genotype | ||||||||
| TT | 125 | 96.15% | 116 | 92.06% | 0.19 | |||
| TC | 5 | 3.85% | 10 | 7.94% | TC vs. TT | 0.19 | 0.46 (0.15–1.40) | |
| CC | 0 | 0.00% | 0 | 0.00% | ||||
| IL-17F rs763780 | ||||||||
| Allele | ||||||||
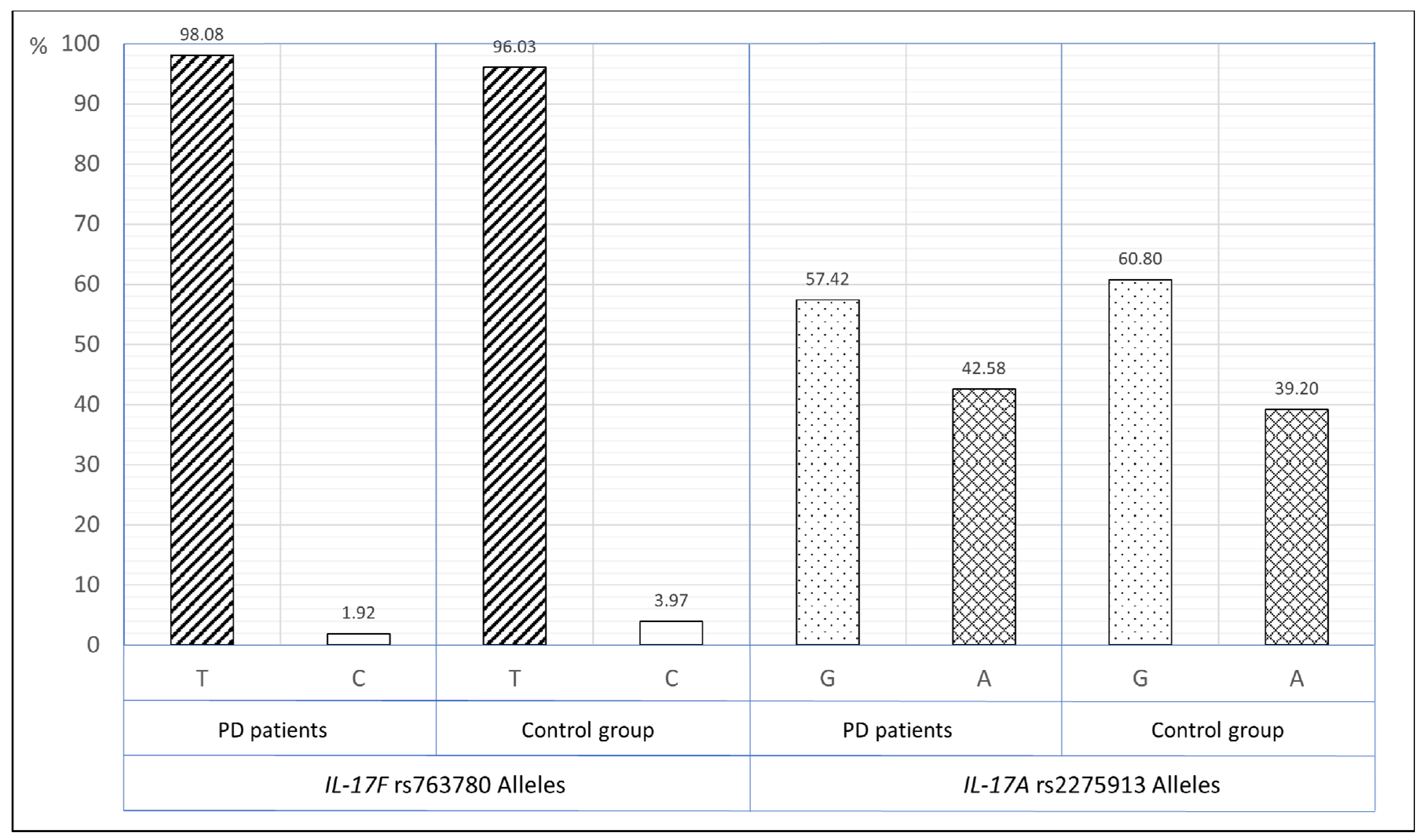
| T | 255 | 98.08% | 242 | 96.03% | ||||
| C | 5 | 1.92% | 10 | 3.97% | C vs. T | 0.20 | 0.48 (0.16–1.41) | |
| IL-17A rs2275913 | ||||||||
| genotype | ||||||||
| GG | 44 | 34.38% | 48 | 38.40% | 0.75 | AA + GA vs. GG | 0.52 | 1.19 (0.71–1.99) |
| GA | 59 | 46.09% | 56 | 44.80% | AA vs. GA + GG | 0.63 | 1.20 (0.63–2.28) | |
| AA | 25 | 19.53% | 21 | 16.80% | AA vs. GG | 0.59 | 1.30 (0.64–2.64) | |
| GA vs. GG | 0.68 | 1.15 (0.66–1.99) | ||||||
| AA vs. GA | 0.86 | 1.13 (0.57–2.24) | ||||||
| IL-17A rs2275913 | ||||||||
| Allele | ||||||||
| G | 147 | 57.42% | 152 | 60.80% | ||||
| A | 109 | 42.58% | 98 | 39.20% | A vs. G | 0.47 | 1.15 (0.81–1.64) | |
| Genotype/Allele | PD Patients | Control Group | pa | Compared Genotypes/Alleles | pb | OR (95%CI) | ||
|---|---|---|---|---|---|---|---|---|
| (Smokers) | (Smokers) | |||||||
| n | % | n | % | |||||
| IL-17F rs763780 | ||||||||
| genotype | ||||||||
| TT | 65 | 92.86% | 32 | 94.12% | 1.00 | |||
| TC | 5 | 7.14% | 2 | 5.88% | TC vs. TT | 1.00 | 1.23 (0.23–6.69) | |
| CC | 0 | 0.00% | 0 | 0.00% | ||||
| IL-17F rs763780 | ||||||||
| Allele | ||||||||
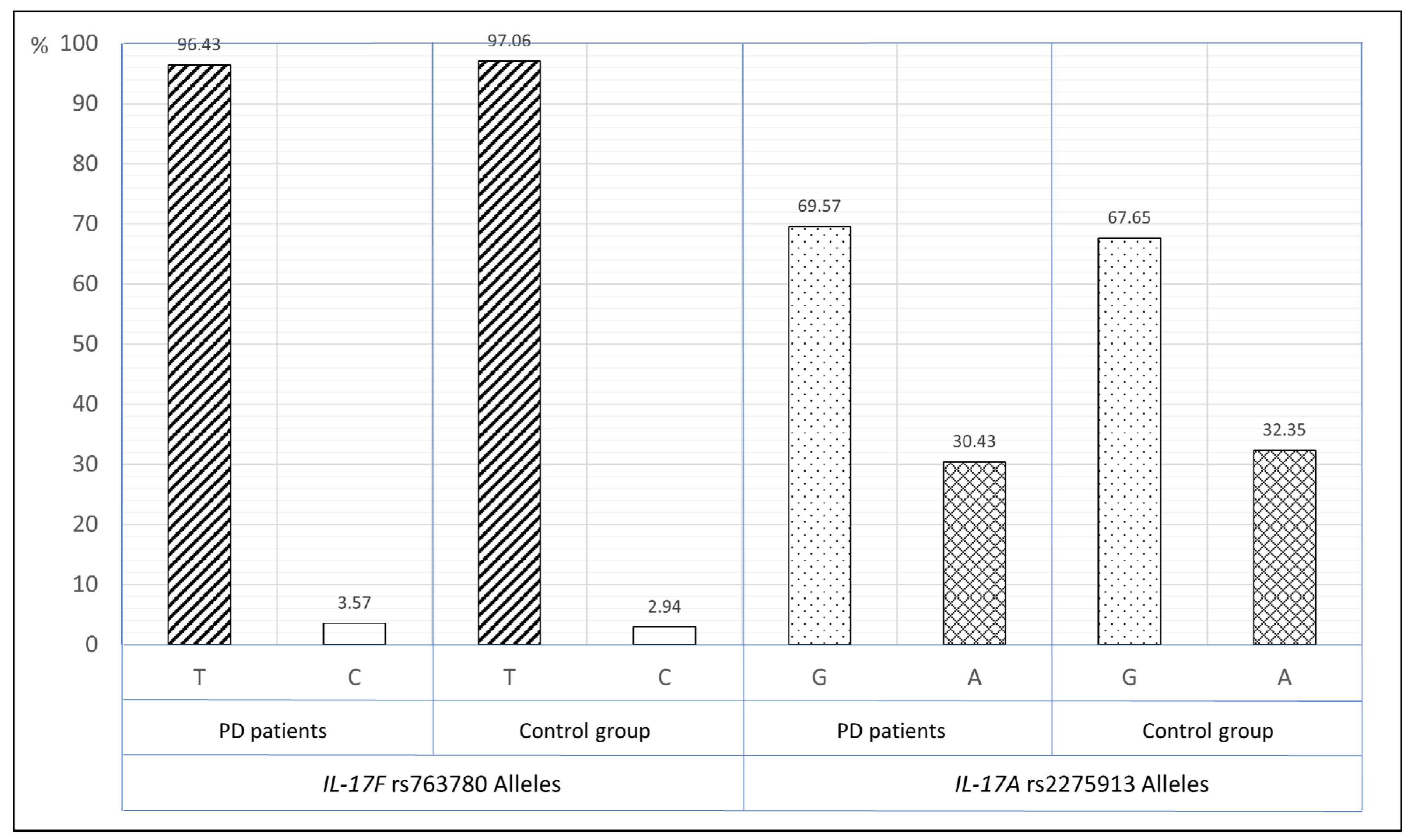
| T | 135 | 96.43% | 66 | 97.06% | ||||
| C | 5 | 3.57% | 2 | 2.94% | C vs. T | 1.00 | 1.22 (0.23–6.47) | |
| IL-17A rs2275913 | ||||||||
| genotype | ||||||||
| GG | 37 | 53.62% | 16 | 47.06% | 0.65 | AA + GA vs. GG | 0.68 | 0.77 (0.34–1.75) |
| GA | 22 | 31.89% | 14 | 41.18% | AA vs. GA + GG | 1.00 | 1.27 (0.37–4.39) | |
| AA | 10 | 14.49% | 4 | 11.76% | AA vs. GG | 1.00 | 1.08 (0.30–3.96) | |
| GA vs. GG | 0.49 | 0.68 (0.28–1.66) | ||||||
| AA vs. GA | 0.74 | 1.59 (0.42–6.07) | ||||||
| IL-17A rs2275913 | ||||||||
| Allele | ||||||||
| G | 96 | 69.57% | 46 | 67.65% | ||||
| A | 42 | 30.43% | 22 | 32.35% | A vs. G | 0.87 | 0.92 (0.49–1.71) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazurek-Mochol, M.; Kozak, M.; Malinowski, D.; Safranow, K.; Pawlik, A. IL-17F Gene rs763780 and IL-17A rs2275913 Polymorphisms in Patients with Periodontitis. Int. J. Environ. Res. Public Health 2021, 18, 1081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031081
Mazurek-Mochol M, Kozak M, Malinowski D, Safranow K, Pawlik A. IL-17F Gene rs763780 and IL-17A rs2275913 Polymorphisms in Patients with Periodontitis. International Journal of Environmental Research and Public Health. 2021; 18(3):1081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031081
Chicago/Turabian StyleMazurek-Mochol, Małgorzata, Małgorzata Kozak, Damian Malinowski, Krzysztof Safranow, and Andrzej Pawlik. 2021. "IL-17F Gene rs763780 and IL-17A rs2275913 Polymorphisms in Patients with Periodontitis" International Journal of Environmental Research and Public Health 18, no. 3: 1081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031081