
LACE Score-Based Risk Management Tool for Long-Term Home Care Patients: A Proof-of-Concept Study in Taiwan


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting, Data Source, and Ethical Concerns
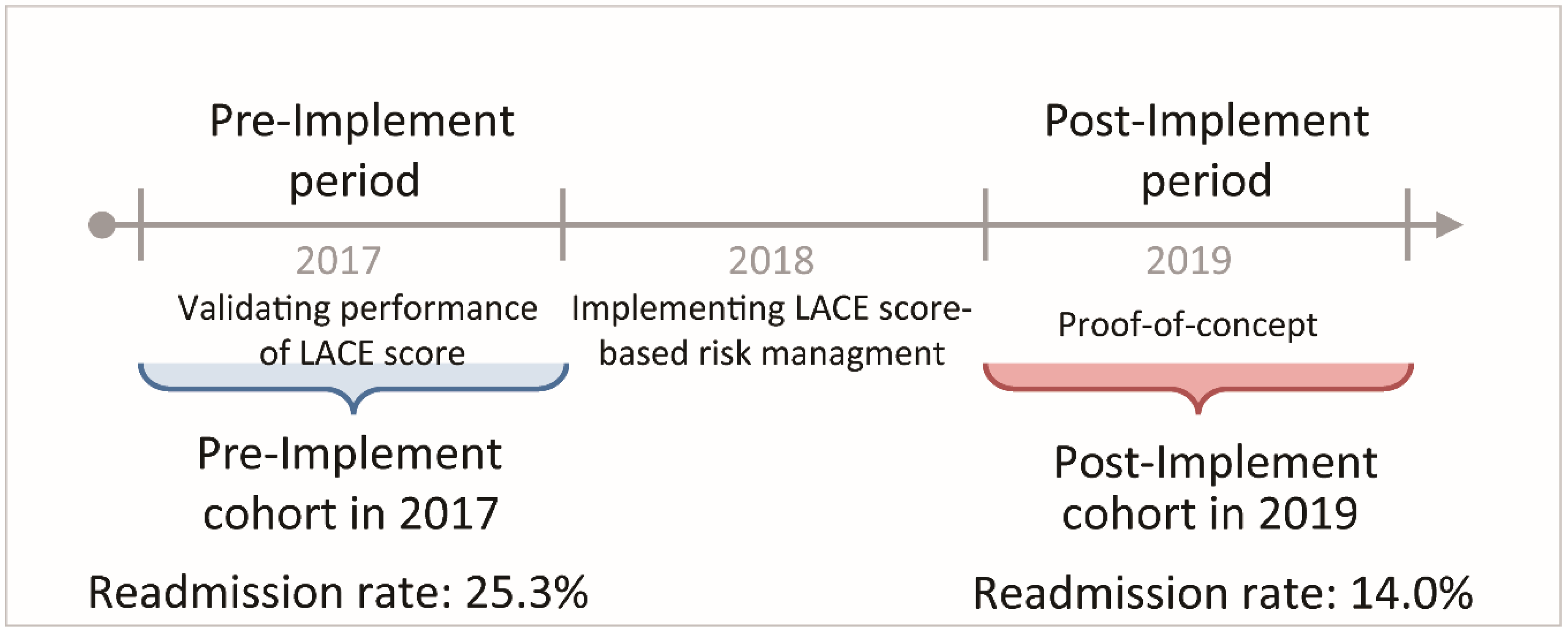
2.2. Pre-Implement Cohort vs. Post-Implement Cohort
2.3. Definition of 30-Day Readmission, Readmission Rate, and Cause-Specific Readmission Rates
2.4. Calculation of LACE Score
2.4.1. L: Length of Stay
2.4.2. A: Acute Admission
2.4.3. C: Comorbidity
2.4.4. E: Emergency Department Visits in the Previous Six Months
2.5. LACE Score-Based Risk Management Tool for Readmission Reduction
2.6. Statistical Analysis
3. Results
3.1. Pre-Implement Cohort and Post-Implement Cohort
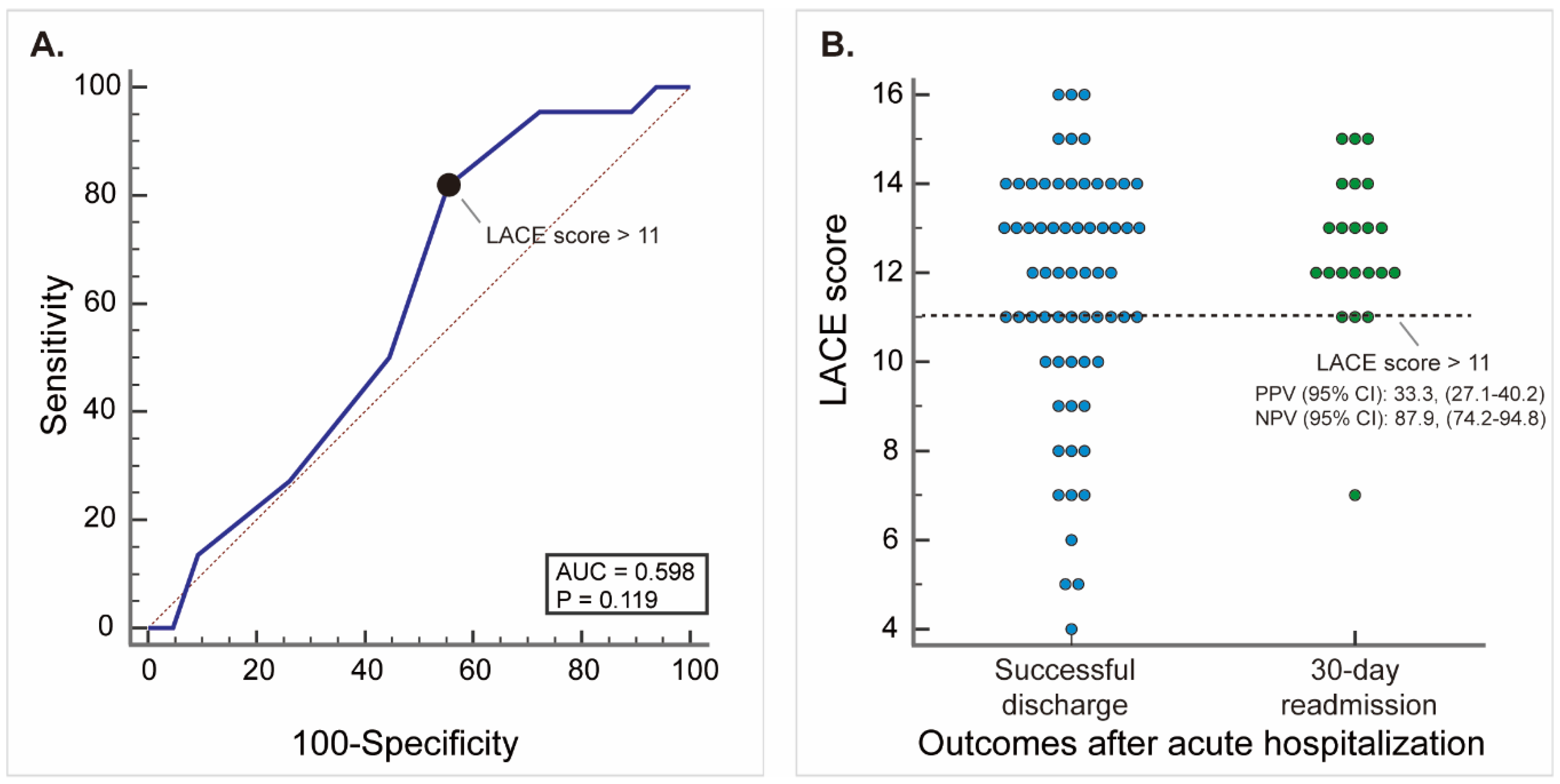
3.2. Validating Performance of LACE Score
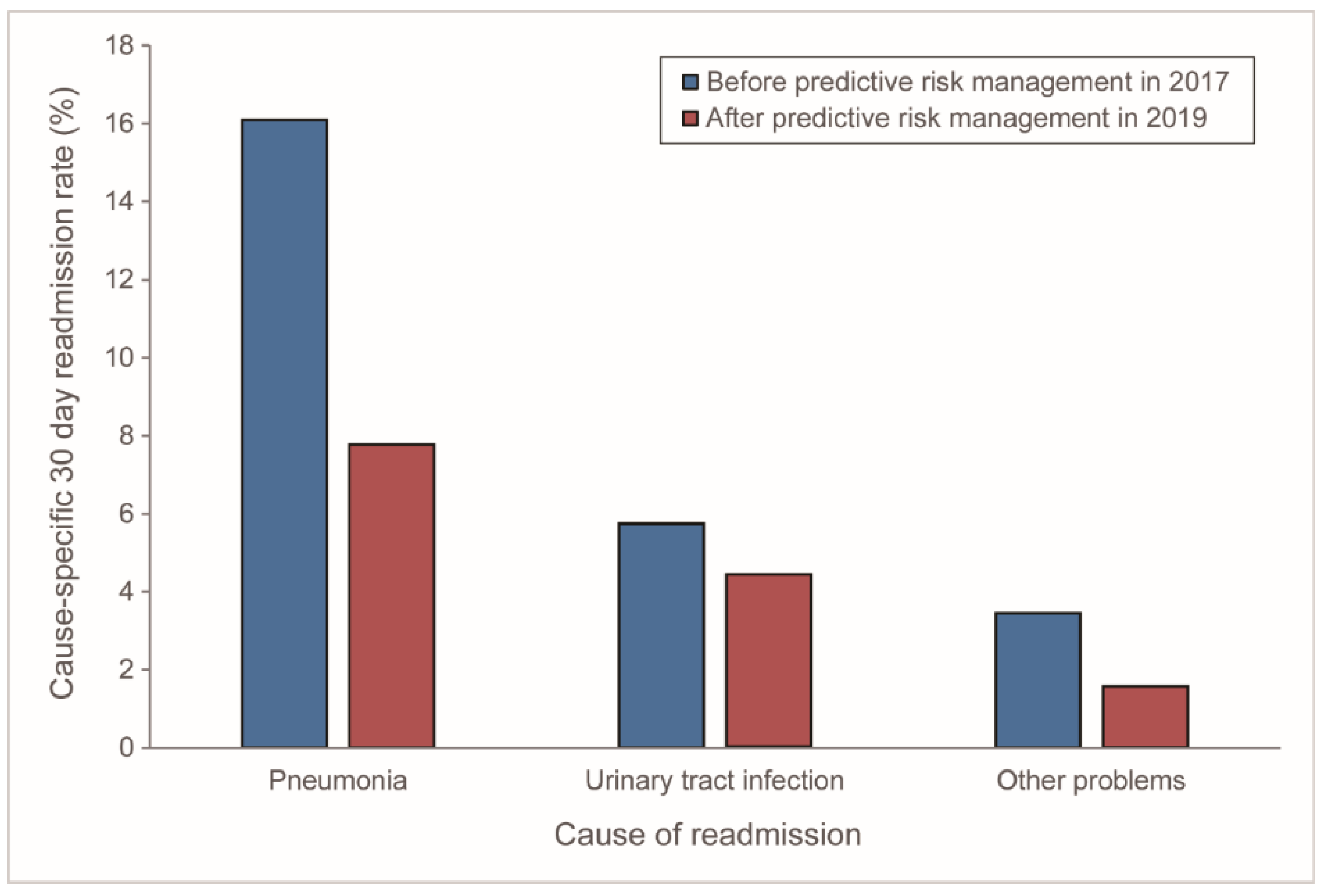
3.3. Readmissions before and after Implementing LACE Score-Based Predictive Risk Management Tool
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Attribute | Value | Points |
|---|---|---|
| Length of stay (days) | <1 | 0 |
| 1 | 1 | |
| 2 | 2 | |
| 3 | 3 | |
| 4–6 | 4 | |
| 7–13 | 5 | |
| ≥14 | 7 | |
| Acute admission | Yes | 3 |
| Comorbidity: Charlson comorbidity index score | 0 | 0 |
| 1 | 1 | |
| 2 | 2 | |
| 3 | 3 | |
| ≥4 | 5 | |
| Emergency department visits in previous 6 months | 0 | 0 |
| 1 | 1 | |
| 2 | 2 | |
| 3 | 3 | |
| ≥4 | 4 |
| Causes of Readmission | No. of Readmissions | Cause-Specific Readmission Rate (%) |
|---|---|---|
| Pneumonia | 14 | 16.1 |
| Urinary tract infection | 5 | 5.7 |
| Herpes zoster infection | 1 | 1.1 |
| Gastrointestinal ulcers | 1 | 1.1 |
| Acute myocardial infarction | 1 | 1.1 |
| Causes of Readmission | No. of Readmissions | Cause-Specific Readmission Rate (%) |
|---|---|---|
| Pneumonia | 14 | 7.4 |
| Urinary tract infection | 8 | 4.2 |
| Fever of unknown origin | 2 | 1.1 |
| Gastrointestinal ulcers | 1 | 0.5 |
References
- Yakusheva, O.; Hoffman, G.J. Does a Reduction in Readmissions Result in Net Savings for Most Hospitals? An Examination of Medicare′s Hospital Readmissions Reduction Program. Med. Care Res. Rev. 2020, 77, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, E.; Kamdar, N.; Kim, N.; Gonzales, G.; Singh, K.; Waljee, A.K. Use of Electronic Medical Records in Development and Validation of Risk Prediction Models of Hospital Readmission: Systematic Review. BMJ 2020, 369, m958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, T.; Heuzenroeder, L.; Feo, R. In-Hospital Interventions for Reducing Readmissions to Acute Care for Adults Aged 65 and Over: An Umbrella Review. Int. J. Qual. Health Care 2020, 32, 414–430. [Google Scholar] [CrossRef] [PubMed]
- Wadhera, R.K.; Joynt Maddox, K.E.; Wasfy, J.H.; Haneuse, S.; Shen, C.; Yeh, R.W. Association of the Hospital Readmissions Reduction Program with Mortality among Medicare Beneficiaries Hospitalized for Heart Failure, Acute Myocardial Infarction, and Pneumonia. JAMA 2018, 320, 2542–2552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, G.J.; Tilson, S.; Yakusheva, O. The Financial Impact of an Avoided Readmission for Teaching and Safety-Net Hospitals Under Medicare’s Hospital Readmission Reduction Program. Med. Care Res. Rev. 2018, 77, 324–333. [Google Scholar] [CrossRef]
- Kripalani, S.; Theobald, C.N.; Anctil, B.; Vasilevskis, E.E. Reducing Hospital Readmission Rates: Current Strategies and Future Directions. Annu. Rev. Med. 2014, 65, 471–485. [Google Scholar] [CrossRef] [Green Version]
- Wasfy, J.H.; Zigler, C.M.; Choirat, C.; Wang, Y.; Dominici, F.; Yeh, R.W. Readmission Rates after Passage of the Hospital Readmissions Reduction Program: A Pre-Post Analysis. Ann. Intern. Med. 2017, 166, 324–331. [Google Scholar] [CrossRef] [Green Version]
- Morkisch, N.; Upegui-Arango, L.D.; Cardona, M.I.; Heuvel, D.V.D.; Rimmele, M.; Sieber, C.C.; Freiberger, E. Components of the transitional care model (TCM) to reduce readmission in geriatric patients: A systematic review. BMC Geriatr. 2020, 20, 1–18. [Google Scholar] [CrossRef]
- Takahashi, P.Y.; Leppin, A.L.; Hanson, G.J. Hospital to Community Transitions for Older Adults: An Update for the Practicing Clinician. Mayo Clin. Proc. 2020, 95, 2253–2262. [Google Scholar] [CrossRef]
- Strassner, C.; Hoffmann, M.; Forstner, J.; Roth, C.; Szecsenyi, J.; Wensing, M. Interventions to Improve Hospital Admission and Discharge Management: An Umbrella Review of Systematic Reviews. Qual. Manag. Health Care 2020, 29, 67–75. [Google Scholar] [CrossRef]
- Grieco, L.; Utley, M.; Crowe, S. Operational research applied to decisions in home health care: A systematic literature review. J. Oper. Res. Soc. 2020, 32. [Google Scholar] [CrossRef]
- Damery, S.; Combes, G. Evaluating the Predictive Strength of the Lace Index in Identifying Patients at High Risk of Hospital Readmission Following an Inpatient Episode: A Retrospective Cohort Study. BMJ Open 2017, 7, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, H.B.; Sieloff, E.; Veeranki, S.P.; Sura, S.D.; Riall, T.S.; Senagore, A.J.; Goodwin, J.S. Risk Prediction Models for Hospital Readmission in Surgery: A Systematic Review. J. Am. Coll. Surg. 2017, 225, E113. [Google Scholar] [CrossRef] [Green Version]
- Hakim, M.A.; Garden, F.L.; Jennings, M.D.; Dobler, C.C. Performance of the Lace Index to Predict 30-Day Hospital Readmissions in Patients with Chronic Obstructive Pulmonary Disease. Clin. Epidemiol. 2018, 10, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Yazdan-Ashoori, P.; Lee, S.F.; Ibrahim, Q.; Van Spall, H.G. Utility of the Lace Index at the Bedside in Predicting 30-Day Readmission or Death in Patients Hospitalized with Heart Failure. Am. Heart J. 2016, 179, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S.M.; Heidenreich, P.; Abbott, B.; Newton, A.; Ward, D. Predictive Models for Identifying Risk of Readmission after Index Hospitalization for Heart Failure: A Systematic Review. Eur. J. Cardiovasc. Nurs. 2018, 17, 675–689. [Google Scholar] [CrossRef] [PubMed]
- Artetxe, A.; Beristain, A.; Graña, M. Predictive models for hospital readmission risk: A systematic review of methods. Comput. Methods Programs Biomed. 2018, 164, 49–64. [Google Scholar] [CrossRef]
- Zhou, H.; Della, P.R.; Roberts, P.; Goh, L.; Dhaliwal, S.S. Utility of models to predict 28-day or 30-day unplanned hospital readmissions: An updated systematic review. BMJ Open 2016, 6, e011060. [Google Scholar] [CrossRef]
- Van Walraven, C.; Dhalla, I.A.; Bell, C.; Etchells, E.; Stiell, I.G.; Zarnke, K.; Austin, P.C.; Forster, A.J. Derivation and Validation of an Index to Predict Early Death or Unplanned Readmission after Discharge from Hospital to the Community. Can. Med. Assoc. J. 2010, 182, 551–557. [Google Scholar] [CrossRef] [Green Version]
- Su, M.C.; Wang, Y.J.; Chen, T.J.; Chiu, S.H.; Chang, H.T.; Huang, M.S.; Hu, L.H.; Li, C.C.; Yang, S.J.; Wu, J.C.; et al. Assess the Performance and Cost-Effectiveness of Lace and Hospital Re-Admission Prediction Models as a Risk Management Tool for Home Care Patients: An Evaluation Study of a Medical Center Affiliated Home Care Unit in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 17. [Google Scholar] [CrossRef] [Green Version]
- Heppleston, E.; Fry, C.H.; Kelly, K.; Shepherd, B.; Wright, R.; Jones, G.; Robin, J.; Murray, P.; Fluck, D.; Han, T.S. Lace Index Predicts Age-Specific Unplanned Readmissions and Mortality after Hospital Discharge. Aging Clin. Exp. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fry, C.H.; Heppleston, E.; Fluck, D.; Han, T.S. Derivation of Age-Adjusted Lace Index Thresholds in the Prediction of Mortality and Frequent Hospital Readmissions in Adults. Intern. Emerg. Med. 2020, 15, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Cotter, P.E.; Bhalla, V.K.; Wallis, S.J.; Biram, R.W.S. Predicting readmissions: Poor performance of the LACE index in an older UK population. Age Ageing 2012, 41, 784–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genet, N.; Boerma, W.G.; Kringos, D.S.; Bouman, A.; Francke, A.L.; Fagerstrom, C.; Melchiorre, M.G.; Greco, C.; Deville, W. Home Care in Europe: A Systematic Literature Review. BMC Health Serv. Res. 2011, 11, 207. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.-T.; Lai, H.-Y.; Hwang, I.-H.; Ho, M.-M.; Hwang, S.-J. Home healthcare services in Taiwan: A nationwide study among the older population. BMC Health Serv. Res. 2010, 10, 274. [Google Scholar] [CrossRef] [Green Version]
- Wong, Z.S.; Hoshino, E.; Ikegami, N. A Cost Projection of Scheduled Physician Home-Visit Services in Japan: 2014 to 2064. J. Aging Soc. Policy 2020. [Google Scholar] [CrossRef]
- Alba, A.C.; Agoritsas, T.; Walsh, M.; Hanna, S.; Iorio, A.; Devereaux, P.J.; McGinn, T.; Guyatt, G. Discrimination and Calibration of Clinical Prediction Models Users’ Guides to the Medical Literature. JAMA 2017, 318, 1377–1384. [Google Scholar] [CrossRef]
- Hansen, L.O.; Greenwald, J.L.; Budnitz, T.; Howell, E.; Halasyamani, L.; Maynard, G.; Vidyarthi, A.; Coleman, E.A.; Williams, M.V. Project Boost: Effectiveness of a Multihospital Effort to Reduce Rehospitalization. J. Hosp. Med. 2013, 8, 421–427. [Google Scholar] [CrossRef]
- Meadow, A.; Sangl, J. Hospital Readmissions in Medicare Home Healthcare: What Are the Leading Risk Indicators? Home Healthc. Now 2019, 37, 213–221. [Google Scholar] [CrossRef]
- Heggestad, A.K.T.; Magelssen, M.; Pedersen, R.; Gjerberg, E. Ethical Challenges in Home-Based Care: A Systematic Literature Review. Nurs Ethics 2020, 0969733020968859. [Google Scholar] [CrossRef]
- Liimatta, H.A.; Lampela, P.; Kautiainen, H.; Laitinen-Parkkonen, P.; Pitkala, K.H. The Effects of Preventive Home Visits on Older People’s Use of Health Care and Social Services and Related Costs. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020, 75, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Chimenti, C.; Sears, G.; McIntyre, J. Sepsis in Home Health Care: Screening, Education, and Rapid Triage. J. Nurs Care Qual. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bowles, K.H.; Cater, J.R. Screening for Risk of Rehospitalization from Home Care: Use of the Outcomes Assessment Information Set and the Probability of Readmission Instrument. Res. Nurs. Health 2003, 26, 118–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shang, J.; Wang, J.; Adams, V.; Ma, C. Risk factors for infection in home health care: Analysis of national Outcome and Assessment Information Set data. Res. Nurs. Health 2020, 43, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.J.; Russell, D.; Dowding, D.; McDonald, M.V.; Murtaugh, C.; Liu, J.F.; Larson, E.L.; Sridharan, S.; Brickner, C. A Predictive Risk Model for Infection-Related Hospitalization among Home Healthcare Patients. J. Healthc. Qual. 2020, 42, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, G.; D’Angelo, D.; Piredda, M.; Petitti, T.; Matarese, M.; Oliveti, A.; De Marinis, M.G. Continuity of Care Interventions for Preventing Hospital Readmission of Older People with Chronic Diseases: A Meta-Analysis. Int. J. Nurs. Stud. 2020, 101, 103396. [Google Scholar] [CrossRef]
- Maatman, T.K.; McGreevy, K.A.; Sood, A.J.; Ceppa, E.P.; House, M.G.; Nakeeb, A.; Schmidt, C.M.; Nguyen, T.K.; Zyromski, N.J. Improved Outpatient Communication Decreases Unplanned Readmission in Necrotizing Pancreatitis. J. Surg. Res. 2020, 253, 139–146. [Google Scholar] [CrossRef]
- Mols, R.E.; Hald, M.; Vistisen, H.S.; Lomborg, K.; Maeng, M. Nurse-Led Motivational Telephone Follow-up after Same-Day Percutaneous Coronary Intervention Reduces Readmission and Contacts to General Practice. J. Cardiovasc. Nurs. 2019, 34, 222–230. [Google Scholar] [CrossRef]
- Parks, C.; Turner, M.; Ward, K.; Murphy, F.; Dame, P.; Hale, K.; Dixon, J.; Lawson, M.; Barber, A.; Monaghan, D. To Call or Not to Call: Assessing the Impact of Nurse Post-Discharge Telephone Calls on 30 Day Hospital Readmission Rates. J. Cardiovasc. Nurs. 2019, 34, 419–420. [Google Scholar]
- Martin, C.; Hinkley, N.; Stockman, K.; Campbell, D. Capitated Telehealth Coaching Hospital Readmission Service in Australia: Pragmatic Controlled Evaluation. J. Med. Internet Res. 2020, 22, e18046. [Google Scholar] [CrossRef]
- Koonin, L.M.; Hoots, B.; Tsang, C.A.; Leroy, Z.; Farris, K.; Jolly, T.; Antall, P.; McCabe, B.; Zelis, C.B.R.; Tong, I.; et al. Trends in the Use of Telehealth During the Emergence of the Covid-19 Pandemic United States, January-March 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1595–1599. [Google Scholar] [CrossRef] [PubMed]
- Goodman-Casanova, J.M.; Dura-Perez, E.; Guzman-Parra, J.; Cuesta-Vargas, A.; Mayoral-Cleries, F. Telehealth Home Support During Covid-19 Confinement for Community-Dwelling Older Adults with Mild Cognitive Impairment or Mild Dementia: Survey Study. J. Med. Internet Res. 2020, 22, e19434. [Google Scholar] [CrossRef] [PubMed]
- Flaks-Manov, N.; Srulovici, E.; Yahalom, R.; Perry-Mezre, H.; Balicer, R.; Shadmi, E. Preventing Hospital Readmissions: Healthcare Providers’ Perspectives on Impactibility Beyond Ehr 30-Day Readmission Risk Prediction. J. Gen. Intern. Med. 2020, 35, 1484–1489. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.D.; Falvey, J.; Hess, E.; Levy, C.R.; Nuccio, E.; Baron, A.E.; Masoudi, F.A.; Stevens-Lapsley, J. Predicting Hospital Readmissions from Home Healthcare in Medicare Beneficiaries. J. Am. Geriatr. Soc. 2019, 67, 2505–2510. [Google Scholar] [CrossRef]
- Leppin, A.L.; Gionfriddo, M.R.; Kessler, M.; Brito, J.P.; Mair, F.S.; Gallacher, K.; Wang, Z.; Erwin, P.J.; Sylvester, T. Preventing 30-Day Hospital Readmissions a Systematic Review and Meta-Analysis of Randomized Trials. Jama Intern. Med. 2014, 174, 1095–1107. [Google Scholar] [CrossRef]
- Kansagara, D.; Englander, H.; Salanitro, A.; Kagen, D.; Theobald, C.; Freeman, M.; Kripalani, S. Risk Prediction Models for Hospital Readmission a Systematic Review. JAMA 2011, 306, 1688–1698. [Google Scholar] [CrossRef] [Green Version]
- Sperrin, M.; Martin, G.P.; Sisk, R.; Peek, N. Missing Data Should Be Handled Differently for Prediction Than for Description or Causal Explanation. J. Clin. Epidemiol. 2020, 125, 183–187. [Google Scholar] [CrossRef]
- Van Smeden, M.; Groenwold, R.H.; Moons, K.G. A cautionary note on the use of the missing indicator method for handling missing data in prediction research. J. Clin. Epidemiol. 2020, 125, 188–190. [Google Scholar] [CrossRef]
- Van Walraven, C.; Wong, J.; Hawken, S.; Forster, A.J. Comparing Methods to Calculate Hospital-Specific Rates of Early Death or Urgent Readmission. CMAJ 2012, 184, E810–E817. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Acute Hospitalizations of the Pre-Implement Cohort in 2017 (n = 87) | Acute Hospitalizations of the Post-Implement Cohort in 2019 (n = 179) | |||||
|---|---|---|---|---|---|---|
| Mean | (SD 1) | Mean | (SD 1) | p-Value | Sig. 2 | |
| Personal Demographics | ||||||
| Gender | 0.711 | |||||
| Female, no. (%) | 40 | (46.0) | 78 | (43.6) | ||
| Male, no. (%) | 47 | (54.0) | 101 | (56.4) | ||
| Age | 87.4 | (12.4) | 84.7 | (12.0) | 0.094 | |
| LACE Score | ||||||
| Length of stay (L) | 5.6 | (0.7) | 5.7 | (0.6) | 0.229 | |
| Acuity of admission (A) | 2.7 | (0.9) | 2.8 | (0.6) | 0.283 | |
| Comorbidities (C) | 1.7 | (0.9) | 1.6 | (0.9) | 0.396 | |
| Emergency department visits (E) | 1.9 | (1.3) | 1.8 | (1.1) | 0.513 | |
| LACE score | 11.8 | (2.6) | 11.6 | (1.8) | 0.465 | |
| Outcome | ||||||
| No. of 30-day readmission | 22 | 25 | 0.023 | * | ||
| Readmission rate %, (95% C.I. 3) | 25.3 | (15.9–38.3) | 14.0 | (9.0–20.3) | 0.039 | * |
| Causes of Readmission | Readmissions before Predictive Risk Management in 2017 1 (Pre-Implement in 2017, n = 87) | Readmissions after Predictive Risk Management in 2019 2 (Post-Implement in 2019, n = 179) | Readmission Rate Difference (%) | ||
|---|---|---|---|---|---|
| No. of Readmissions | Cause-Specific Readmission Rate (%) 3 | No. of Readmissions | Cause-Specific Readmission Rate (%) 3 | ||
| All-cause | 22 | 25.3 | 25 | 14.0 | 11.3 |
| Pneumonia | 14 | 16.1 | 14 | 7.8 | 8.3 |
| Urinary tract infection | 5 | 5.7 | 8 | 4.5 | 1.3 |
| Other problems | 3 | 3.4 | 3 | 1.7 | 1.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, M.-C.; Chen, Y.-C.; Huang, M.-S.; Lin, Y.-H.; Lin, L.-H.; Chang, H.-T.; Chen, T.-J. LACE Score-Based Risk Management Tool for Long-Term Home Care Patients: A Proof-of-Concept Study in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 1135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031135
Su M-C, Chen Y-C, Huang M-S, Lin Y-H, Lin L-H, Chang H-T, Chen T-J. LACE Score-Based Risk Management Tool for Long-Term Home Care Patients: A Proof-of-Concept Study in Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(3):1135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031135
Chicago/Turabian StyleSu, Mei-Chin, Yu-Chun Chen, Mei-Shu Huang, Yen-Hsi Lin, Li-Hwa Lin, Hsiao-Ting Chang, and Tzeng-Ji Chen. 2021. "LACE Score-Based Risk Management Tool for Long-Term Home Care Patients: A Proof-of-Concept Study in Taiwan" International Journal of Environmental Research and Public Health 18, no. 3: 1135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031135