
Can Health-Promoting Schools Contribute to Better Health Behaviors? Physical Activity, Sedentary Behavior, and Dietary Habits among Israeli Adolescents


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedures
2.2. Instruments and Measures
2.2.1. Dependent Variables
2.2.2. Independent Variables
2.3. Data Analysis
2.3.1. School and Study Participants’ Characteristics
2.3.2. Between-Group Differences in Health Behavior
2.3.3. Variables Associated with and Predicting Health Behavior
3. Results
3.1. Schools’ and Study Participants’ Characteristics
3.2. Between-Group Differences in Health Behavior
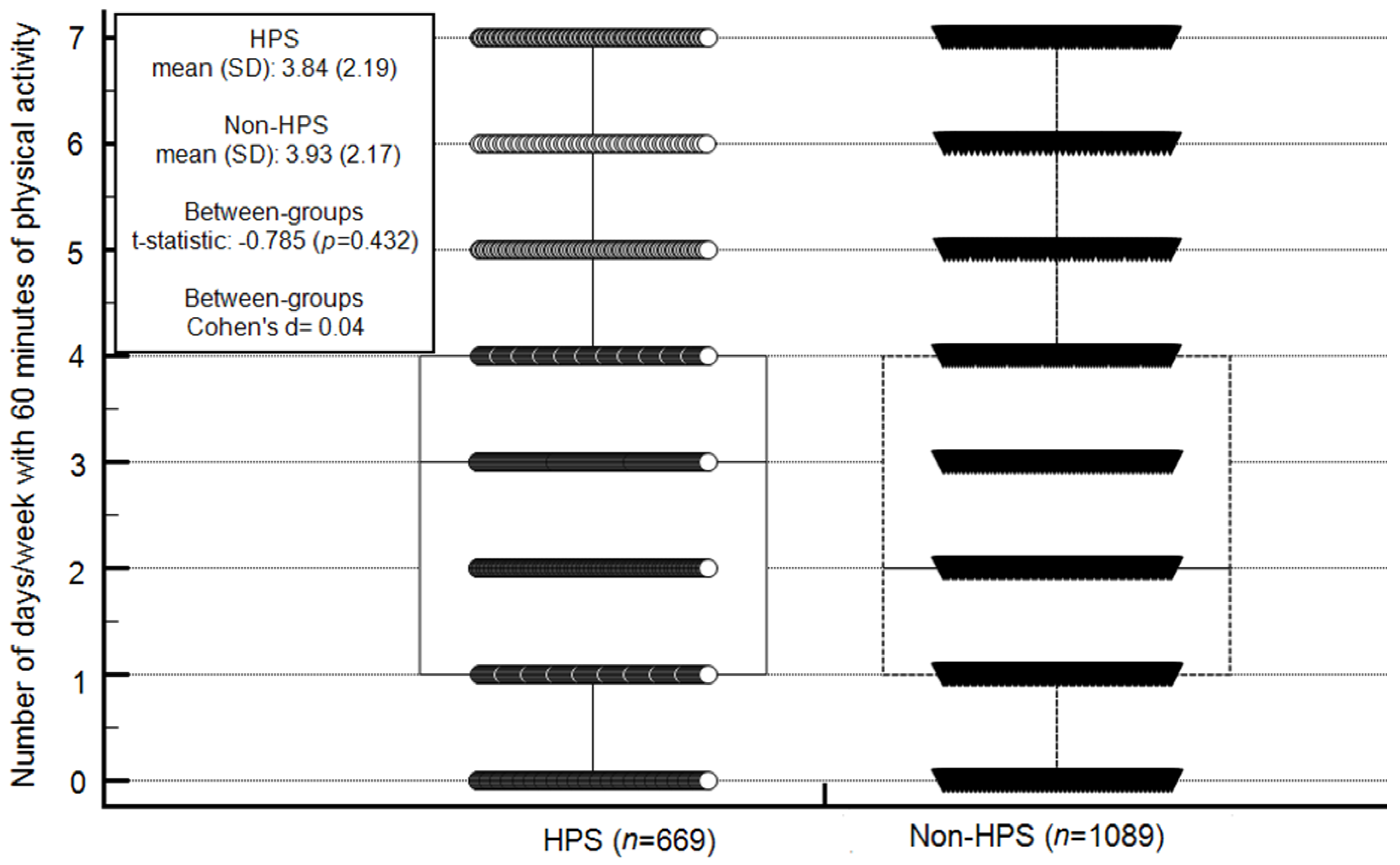
3.2.1. Physical Activity Level
3.2.2. Screen Time
3.2.3. Dieting Behavior
3.2.4. Between-Group Differences in Health Behavior
3.3. Variables Associated with and Predicting Health Behavior
Associations between Study Variables and PA Level and Screen Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whitman, C.V.; Aldinger, C.E. (Eds.) Case Studies in Global School Health Promotion: From Research to Practice; Springer Science & Business Media: Newton, MA, USA, 2009. [Google Scholar]
- World Health Organization. Equity, Social Determinants and Public Health Programmes; Blas, E., Kurup, A.S., Eds.; IRIS: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/handle/10665/44289 (accessed on 15 July 2020).
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020. 2013. Available online: https://apps.who.int/iris/handle/10665/94384 (accessed on 15 July 2020).
- World Health Organization. Ottawa Charter for Health Promotion. 1986. Available online: https://www.euro.who.int/__data/assets/pdf_file/0004/129532/Ottawa_Charter.pdf (accessed on 15 July 2020).
- Schölmerich, V.L.S.; Kawachi, I. Translating the socio-ecological perspective into multilevel interventions gaps between theory and practice. Health Educ. Behav. 2016, 43, 17–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, C.Y.; Gim, N.G.; Kim, Y.; Kim, T. Multi-Year Examination of School-Based Programs in Preventing Childhood Obesity: A Case of a State Policy in the US. Int. J. Public Health 2020, 17, 9425. [Google Scholar] [CrossRef] [PubMed]
- Bastos, P.D.O.; Cavalcante, A.S.P.; Pereira, W.M.G.; De Castro, V.H.S.; Júnior, A.R.F.; Guerra, P.H.; Silva, K.S.; Da Silva, M.R.F.; Filho, V.C.B. Health promoting school interventions in Latin America: A systematic review protocol on the dimensions of the RE-AIM framework. Int. J. Environ. Res. Public Health 2020, 17, 5558. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Demetriou, Y.; Tesler, R.; Gouveia, É.R.; Peralta, M.; Matos, M.G. Healthy lifestyle in children and adolescents and its association with subjective health complaints: Findings from 37 countries and regions from the HBSC Study. Int. J. Environ. Res. Public Health 2019, 16, 3292. [Google Scholar] [CrossRef] [Green Version]
- Marques, A.; Peralta, M.; Santos, T.; Martins, J.; De Matos, M.G. Self-rated health and health-related quality of life are related with adolescents’ healthy lifestyle. Public Health 2019, 170, 89–94. [Google Scholar] [CrossRef]
- World Health Organization. Global Diffusion of eHealth: Making Universal Health Coverage Achievable: Report of the Third Global Survey on eHealth. 2016. Available online: https://apps.who.int/iris/handle/10665/252529 (accessed on 15 July 2020).
- Fenwick-Smith, A.; Dahlberg, E.E.; Thompson, S.C. Systematic review of resilience-enhancing, universal, primary school-based mental health promotion programs. BMC Psychol. 2018, 6, 30. [Google Scholar] [CrossRef]
- Green, S.H.; Mallya, G.; Brensinger, C.; Tierney, A.; Glanz, K. Changes in School Competitive Food Environments after a Health Promotion Campaign. J. Sch. Health 2018, 88, 281–288. [Google Scholar] [CrossRef]
- Griebler, U.; Rojatz, D.; Simovska, V.; Forster, R. Effects of student participation in school health promotion: A systematic review. Health Promot. Int. 2017, 32, 195–206. [Google Scholar] [CrossRef]
- Tesler, R.; Harel-Fisch, Y.; Baron-Epel, O. School health promotion policies and adolescent risk behaviors in Israel: A multilevel analysis. J. Sch. Health 2016, 86, 435–443. [Google Scholar] [CrossRef]
- Procedures and Guidelines for Health-Promoting Schools in Israel. Available online: https://meyda.education.gov.il/files/ChinuchMukar/kol_kore_healthy_2019.pdf (accessed on 17 January 2021).
- Israeli Ministry of Education. Available online: https://www.gov.il/en/departments/ministry_of_education (accessed on 10 December 2020).
- National School Database. Available online: https://cms.education.gov.il/EducationCMS/Applications/Ims (accessed on 7 January 2021).
- Marques, A.; Bordado, J.; Tesler, R.; Demetriou, Y.; Sturm, D.J.; De Matos, M.G. A composite measure of healthy lifestyle: A study from 38 countries and regions from Europe and North America, from the Health Behavior in School-Aged Children survey. Am. J. Hum. Biol. 2020, 11, e23419. [Google Scholar]
- Marques, A.; Loureiro, N.; Avelar-Rosa, B.; Naia, A.; De Matos, M.G. Adolescents’ healthy lifestyle. J. Pediat Braz. 2020, 96, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Bonell, C.; Jones, H.; Campbell, R. Obesity prevention and the Health promoting Schools framework: Essential components and barriers to success. Int. J. Behav. Nutr. Phys. 2015, 12, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucarelli, J.F.; Alaimo, K.; Mang, E.; Martin, C.; Miles, R.; Bailey, D.; Kelleher, D.K.; Drzal, N.B.; Liu, H. Facilitators to promoting health in schools: Is school health climate the key? J. Sch. Health 2014, 84, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.; Singh, S. Viability in delivering oral health promotion activities within the Health Promoting Schools Initiative in KwaZulu-Natal. S. Afr. J. Child Health 2015, 9, 93–97. [Google Scholar] [CrossRef]
- McIsaac, J.L.; Read, K.; Veugelers, P.J.; Kirk, S.F. Culture matters: A case of school health promotion in Canada. Health Promot. Int. 2017, 32, 207–217. [Google Scholar] [CrossRef]
- Behaviour in School-aged Children (HBSC) Study Protocol: Background, Methodology and Mandatory Items for the 2013/14 Survey. Available online: http://www.hbsc.org/methods/ (accessed on 15 July 2020).
- Roberts, C.; Freeman, J.; Samdal, O.; Schnohr, C.W.; De Looze, M.E.; Gabhainn, S.N.; Iannotti, R.; Rasmussen, M.; International HBSC Study Group. The Health Behaviour in School-aged Children (HBSC) study: Methodological developments and current tensions. Int. J. Public Health 2009, 54, 140–150. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Spotlight on Adolescent Health and Well-Being. Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada International Report. Volume 1. Key Findings; Inchley, J., Currie, D., Budisavljevic, S., Torsheim, T., Jåstad, A., Cosma, A., Kelly, C., Arnarsson, A.M., Eds.; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Quick, V.; Byrd-Bredbenner, C.; White, A.A.; Brown, O.; Colby, S.; Shoff, S.; Lohse, B.; Horacek, T.; Kidd, T.; Greene, G. Eat, sleep, work, play: Associations of weight status and health-related behaviors among young adult college students. Am. J. Health Promot. 2014, 29, e64–e72. [Google Scholar] [CrossRef]
- Sigmundová, D.; Sigmund, E.; Tesler, R.; Ng, K.W.; Hamrik, Z.; Mathisen, F.K.; Inchley, J.; Bucksch, J. Vigorous physical activity in relation to family affluence: Time trends in Europe and North America. Int. J. Public Health 2019, 64, 1049–1058. [Google Scholar] [CrossRef] [Green Version]
- Kleszczewska, D.; Szkutnik, A.M.; Siedlecka, J.; Mazur, J. Physical activity, sedentary behaviours and duration of sleep as factors affecting the well-being of young people against the background of environmental moderators. Int. J. Environ. Res. Public Health 2019, 16, 915. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Chaput, J.P.; Adamo, K.B.; Aubert, S.; Barnes, J.D.; Choquette, L.; Duggan, M.; Faulkner, G.; Goldfield, G.S.; Gray, C.E.; et al. Canadian 24-hour movement guidelines for the early years (0–4 years): An integration of physical activity, sedentary behaviour, and sleep. BMC Public Health 2017, 17, 874. [Google Scholar] [CrossRef]
- Hayek, S.; Tessler, R.; Bord, S.; Endevelt, R.; Satran, C.; Livne, I.; Khatib, M.; Harel-Fisch, Y.; Baron-Epel, O. Do Israeli health promoting schools contribute to students’ healthy eating and physical activity habits? Health Promot. Int. 2019, 34, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.H. Factors affecting the utilization of mental health evaluation research findings. Prof. Psychol. 1977, 8, 526. [Google Scholar] [CrossRef]
- Myers, R.H. Classical and Modern Regression with Applications; Duxbury Press: Belmont, CA, USA, 1990. [Google Scholar]
- Beck, H.; Tessler, R.; Moran, D.; Kolobov, T.; Harel-Fisch, Y. A multi-level analysis of healthy behaviors: Physical activity & nutrition among students in Israel. Mov. J. Phys. Educ. Sport Sci. 2018, 11, 510–530. [Google Scholar]
- Riddoch, C.J.; Mattocks, C.; Deere, K.; Saunders, J.; Kirkby, J.; Tilling, K.; Leary, S.D.; Blair, S.N.; Ness, A.R. Objective measurement of levels and patterns of physical activity. Arch. Dis. Child 2007, 92, 963–969. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Strategy on Diet, Physical Activity and Health. Available online: https://www.who.int/dietphysicalactivity/factsheet_young_people/en/ (accessed on 15 July 2020).
- Gorely, T.; Nevill, M.E.; Morris, J.G.; Stensel, D.J.; Nevill, A. Effect of a school-based intervention to promote healthy lifestyles in 7–11 year old children. Int. J. Behav. Nutr. Phys. 2009, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Story, M.; Nanney, M.S.; Schwartz, M.B. Schools and obesity prevention: Creating school environments and policies to promote healthy eating and physical activity. Milbank Q. 2009, 87, 71–100. [Google Scholar] [CrossRef]
- Hallal, P.C.; Martins, R.C.; Ramírez, A. The Lancet Physical Activity Observatory: Promoting physical activity worldwide. Lancet 2014, 9942, 471–472. [Google Scholar] [CrossRef]
- Humbert, M.L.; Chad, K.E.; Spink, K.S.; Muhajarine, N.; Anderson, K.D.; Bruner, M.W.; Girolami, T.M.; Odnokon, P.; Gryba, C.R. Factors that influence physical activity participation among high-and low-SES youth. Qual. Health Res. 2006, 16, 467–483. [Google Scholar] [CrossRef]
- Tesler, R.; Kolobov, T.; Ng, K.W.; Shapiro, E.; Walsh, S.D.; Shuval, K.; Harel-Fisch, Y. Ethnic Disparities in Physical Activity among Adolescents in Israel. Am. J. Health Behav. 2019, 43, 337–348. [Google Scholar] [CrossRef]
- Woodfield, L.; Duncan, M.; Al-Nakeeb, Y.; Nevill, A.; Jenkins, C. Sex, ethnic and socio-economic differences in children’s physical activity. Pediatr. Exerc. Sci. 2002, 14, 277–285. [Google Scholar] [CrossRef]
- Trigueros, R.; Aguilar-Parra, J.M.; Cangas, A.J.; López-Liria, R.; Álvarez, J.F. Influence of physical education teachers on motivation, embarrassment and the intention of being physically active during adolescence. Int. J. Environ. Res. Public Health 2019, 16, 2295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manyanga, T.; Tremblay, M.S.; Chaput, J.P.; Katzmarzyk, P.T.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; et al. Socioeconomic status and dietary patterns in children from around the world: Different associations by levels of country human development? BMC Public Health 2017, 17, 457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trigueros, R.; Mínguez, L.A.; González-Bernal, J.J.; Jahouh, M.; Soto-Camara, R.; Aguilar-Parra, J.M. Influence of teaching style on physical education adolescents’ motivation and health-related lifestyle. Nutrients 2019, 11, 2594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Chen, A. Two pathways underlying the effects of physical education on out-of-school physical activity. Res. Q. Exerc. Sport 2020, 91, 197–208. [Google Scholar] [CrossRef]
- Currie, C.; Morgan, A. A bio-ecological framing of evidence on the determinants of adolescent mental health-a scoping review of the international Health Behaviour in School-Aged Children (HBSC) Study 1983–2020. SSM Popul. Health 2020, 21, 100697. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total (n = 1758): n (%) OR Mean (SD) | Health-Promoting School (n = 669): n (%) OR Mean (SD) | Non-Health-Promoting School (n = 1089): n (%) OR Mean (SD) | Between-Group Differences: Chi Square or t-Statistic (p Value) | Odds Ratio | |
|---|---|---|---|---|---|---|
| Sex | Female, n (%) | 932 (53.00) | 331(49.50) | 488 (44.80) | 3.67 (0.06) | 0.79 |
| Male, n (%) | 826 (47.00) | 338 (50.50) | 601 (55.20) | 3.67 (0.06) | ||
| Grade | 6th, n (%) | 432 (24.60) | 125 (18.70) | 307 (28.20) | 20.16 (<0.001) | 1.70 |
| 8th, n (%) | 541 (30.80) | 161 (24.10) | 380 (34.90) | 22.67 (<0.001) | 1.69 | |
| 10th, n (%) | 412 (23.40) | 257 (38.40) | 155 (14.20) | 135.28 (<0.001) | 0.26 | |
| 11th + 12th, n (%) | 373 (21.20) | 126 (18.80) | 247 (22.70) | 3.76 (0.06) | 1.26 | |
| Weight, kg: mean (SD) | 52.41 (14.11) | 55.14 (14.12) | 50.74 (13.85) | −6.16 (<0.001) | ||
| Height, meters: mean (SD) | 161.08 (12.41) | 162.94 (12.95) | 159.93 (11.94) | −4.83 (<0.001) | ||
| Body mass index: mean (SD) | 20.00 (3.95) | 20.64 (4.04) | 19.61 (3.84) | −5.08 (<0.001) | ||
| Family affluence scale: mean (SD) | 5.67 (1.92) | 8.24 (2.56) | 8.80 (2.42) | 4.57 (<0.001) | ||
| Variables | Health Promotion Schools (n = 669) | Non-Health Promotion Schools (n = 1089) | Between-Group Chi-Squared | |||
|---|---|---|---|---|---|---|
| n (%) | Chi-Squared | n (%) | Chi-Squared | |||
| Achieving physical activity level recommendations | Yes | 68 (10.20) | 424.64 * | 109 (10.00) | 696.64 * | 0.44 |
| No | 601 (89.80) | 989 (90.00) | ||||
| Screen time—computer | <2 h/day | 444 (66.36) | 145.65 * | 733 (67.30) | 266.76 * | 0.18 |
| >2 h/day | 225 (33.63) | 356 (32.69) | ||||
| Screen time—television | <2 h/day | 434 (64.87) | 112.45 * | 714 (65.56) | 209.23 * | 0.18 |
| >2 h/day | 235 (35.12) | 375 (34.43) | ||||
| Screen time—total | <2 h/day | 262 (39.16) | 58.96 * | 393 (36.08) | 158.71 * | 0.15 |
| >2 h/day | 407 (60.83) | 696 (63.91) | ||||
| Dieting in the past year | Yes | 222 (33.18) | 110.77 * | 343 (31.49) | 206.60 * | 0.76 |
| No | 447 (66.81) | 746 (68.50) | ||||
| Variables | Number of Days with 60 min of Physical Activity | Hours of Screen Time | ||||
|---|---|---|---|---|---|---|
| Health-Promoting School (n = 669): n (%) OR Mean (SD) | Non-Health-Promoting School (n = 1089): n (%) OR Mean (SD) | Z Transformation of the Correlation Test: Test Statistic Z | Health-Promoting School (n = 669): n (%) OR Mean (SD) | Non-Health-Promoting School (n = 1089): n (%) OR Mean (SD) | Z Transformation of the Correlation Test: Test Statistic Z | |
| Grade | −0.091 * | −0.237 * | 3.05 * | −0.120 * | −0.102 * | −0.37 |
| Socio-economic status | 0.137 * | 0.153 * | −0.332 | −0.074 | 0.0642 | −0.356 |
| Screen time | −0.072 | −0.004 | −1.38 | ---------------- | ---------------- | ---------------- |
| Number of days with 60 min of physical activity | ---------------- | ---------------- | ---------------- | −0.045 | 0.002 | −0.956 |
| Variables | Unstandardized Standard Error | Standardized Beta Coefficient | t | p Value | |
|---|---|---|---|---|---|
| Constant | 0.37 | 16.22 | <0.001 | ||
| Screen time, hours | 0.05 | −0.07 | −2.90 | 0.004 | |
| Dieting behavior (reference: dieting) | Not dieting | 0.12 | −0.15 | −5.826 | <0.001 |
| School sector (reference: secular) | Religious | 0.06 | −0.03 | −1.22 | 0.22 |
| Arab | 0.02 | −0.02 | −1.10 | 0.22 | |
| Grade | 0.03 | 0.26 | −9.71 | <0.001 | |
| Sex (reference: female) | Male | 0.12 | 0.24 | 9.25 | <0.001 |
| Socio-economic status | 0.02 | 0.13 | 4.93 | <0.001 | |
| Health-promoting school (reference: health-promoting school) | Non-health-promoting school | 0.13 | 0.02 | 0.95 | 0.34 |
| Model summery | F = 32.85; adjusted R2 = 0.15; p < 0.001 | ||||
| Variables | Unstandardized Standard Error | Standardized Betta Coefficient | t | p Value | |
|---|---|---|---|---|---|
| Constant | 0.41 | 13.71 | < 0.001 | ||
| Physical activity level, days active | 0.03 | −0.08 | −2.90 | 0.004 | |
| Dieting behavior (reference: dieting) | Not dieting | 0.14 | 0.03 | 1.24 | 0.215 |
| School sector (reference: secular) | Religious | 0.07 | 0.00 | −0.94 | 0.925 |
| Arab | 0.06 | 0.00 | −0.98 | 0.987 | |
| Grade | 0.06 | −0.12 | −3.97 | < 0.001 | |
| Sex (reference: female) | Male | 0.13 | 0.19 | 6.61 | < 0.001 |
| Socio-economic status | 0.02 | −0.01 | −0.31 | 0.756 | |
| Health-promoting school (reference: health-promoting school) | Non-health-promoting school | 0.13 | −0.01 | −0.63 | 0.528 |
| Model summary | F = 8.38; adjusted R2 = 0.04; p < 0.001 | ||||
| Variables | Odds Ratio | Wald | 95% Confidence Interval | p Value | |
|---|---|---|---|---|---|
| Constant | 54.42 | <0.001 | |||
| Physical activity level, days/week | 1.20 | 32.69 | 1.12–1.28 | <0.001 | |
| Screen time, hours | 1.03 | 1.36 | 0.97–1.10 | 0.24 | |
| School sector (reference, secular) | Religious | 0.92 | 0.27 | 0.67–1.25 | 0.60 |
| Arab | 0.84 | 0.70 | 0.56–1.26 | 0.40 | |
| Grade | 1.23 | 9.38 | 1.07–1.40 | 0.002 | |
| Sex (reference male) | Female | 2.29 | 31.57 | 1.71–3.07 | <0.001 |
| Socio-economic status | 1.00 | 0.08 | 0.95–1.06 | 0.76 | |
| Health-promoting school (reference: health-promoting school) | Non-health-promoting school | 1.03 | 0.05 | 0.77–1.38 | 0.81 |
| Model summary | Chi-squared = 59.52, p < 0.001, Nagelkerke R2 = 0.07. | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beck, H.; Tesler, R.; Barak, S.; Moran, D.S.; Marques, A.; Harel Fisch, Y. Can Health-Promoting Schools Contribute to Better Health Behaviors? Physical Activity, Sedentary Behavior, and Dietary Habits among Israeli Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 1183. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031183
Beck H, Tesler R, Barak S, Moran DS, Marques A, Harel Fisch Y. Can Health-Promoting Schools Contribute to Better Health Behaviors? Physical Activity, Sedentary Behavior, and Dietary Habits among Israeli Adolescents. International Journal of Environmental Research and Public Health. 2021; 18(3):1183. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031183
Chicago/Turabian StyleBeck, Hila, Riki Tesler, Sharon Barak, Daniel Sender Moran, Adilson Marques, and Yossi Harel Fisch. 2021. "Can Health-Promoting Schools Contribute to Better Health Behaviors? Physical Activity, Sedentary Behavior, and Dietary Habits among Israeli Adolescents" International Journal of Environmental Research and Public Health 18, no. 3: 1183. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031183