
Community Socioeconomic Status and Dispatcher-Assisted Cardiopulmonary Resuscitation for Patients with Out-of-Hospital Cardiac Arrest


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
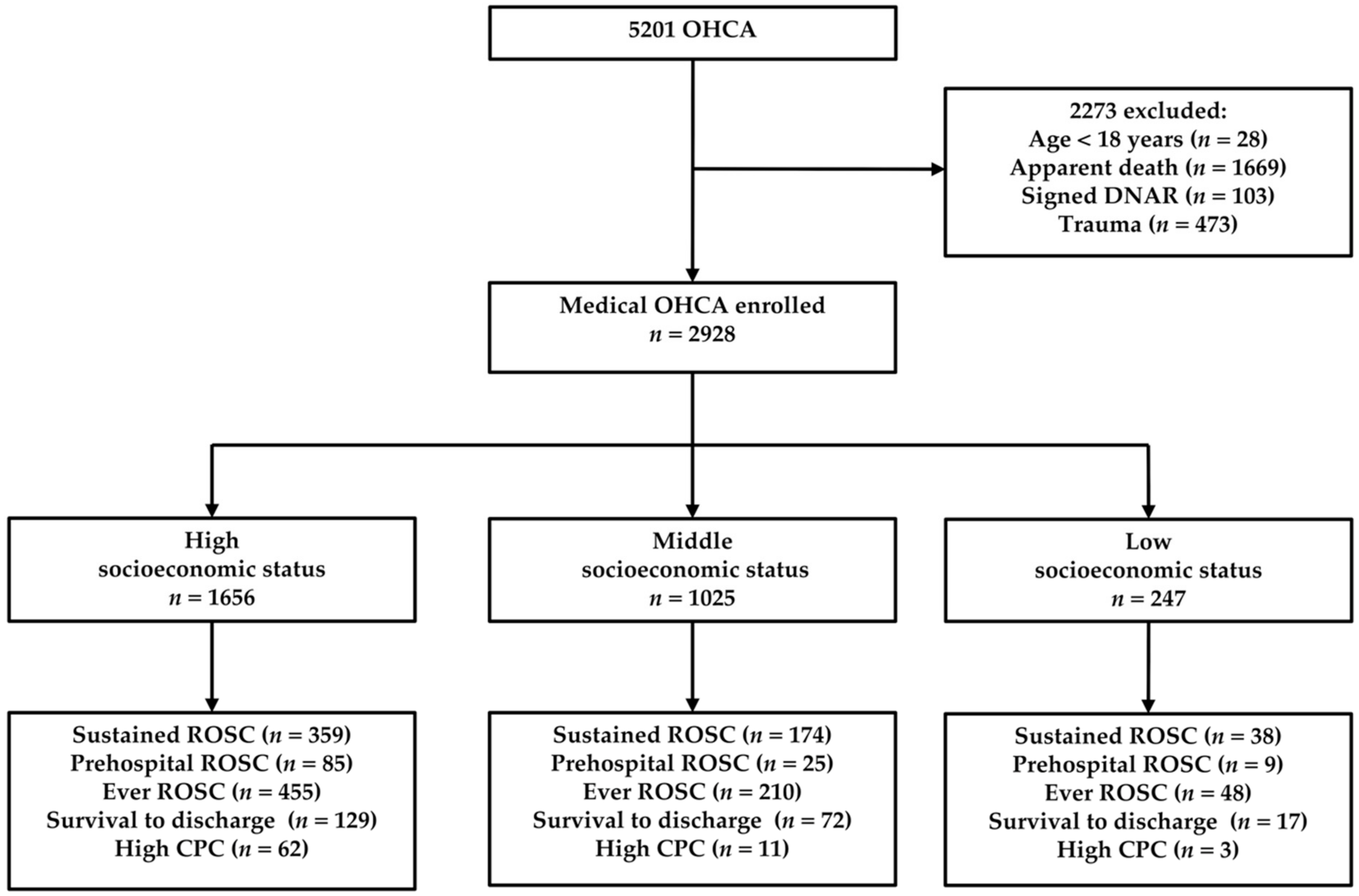
2.2. Selection of Participants
2.3. DA-CPR Program
2.4. Socioeconomic Status
2.5. Data Collection and Processing
2.6. Outcome Measures
2.7. Primary Data Analysis
3. Results
3.1. Socioeconomic Status
3.2. Patient Characteristics
3.3. DA-CPR
3.4. ROSC
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| OHCA | High SES a n = 10 | Middle SES b n = 17 | Low SES c n = 10 | p Value |
|---|---|---|---|---|
| Average price of real state (US dollars/m2) | 2740.9 ± 2251.6 | 285.9 ± 191.2 | 55.9 ± 22.1 | <0.001 |
| Population (103 persons) | 123.1 ± 60.9 | 30.8 ± 12.4 | 13.2 ± 7.1 | <0.001 |
| Area (km2) | 36.1 ± 30.6 | 53.9 ± 22.9 | 91.4 ± 37.6 | 0.001 |
| Population density (103 persons/km2) | 6.2 ± 5.1 | 0.6 ± 0.3 | 0.2 ± 0.1 | <0.001 |
| Mean annual household income (103 US dollars) | 30.5 ± 4.0 | 25.3 ± 2.7 | 22.5 ± 0.9 | <0.001 |
| OHCA | High SES n = 1656 | Middle SES n = 1025 | Low SES n = 247 | p Value |
|---|---|---|---|---|
| Dispatcher can’t recognize need for CPR | 320 (19.3%) | 194 (18.9%) | 48 (19.4%) | 0.964 |
| Difficult access to the victim | 125 (7.5%) | 77 (7.5%) | 14 (5.7%) | 0.561 |
| CPR is already ongoing | 84 (5.1%) | 60 (5.9%) | 5 (2.0%) | 0.049 |
| Overly distraught | 54 (3.3%) | 33 (3.2%) | 8 (3.2%) | 0.998 |
| Third party caller | 23 (1.4%) | 11 (1.1%) | 1 (0.4%) | 0.473 |
| Patient’s status changed | 15 (0.9%) | 7 (0.7%) | 3 (1.2%) | 0.579 |
| Dangerous scene | 6 (0.4%) | 5 (0.5%) | 2 (0.8%) | 0.463 |
| Apparent death | 9 (0.5%) | 2 (0.2%) | 0 | 0.307 |
| Caller unable to move the patient | 5 (0.3%) | 6 (0.6%) | 0 | 0.445 |
| Language barriers | 1 (0.1%) | 2 (0.2%) | 0 | 0.664 |
| Valid DNAR orders | 1 (0.1%) | 1 (0.1%) | 0 | 1 |
References
- Ong, M.E.; Shin, S.D.; De Souza, N.N.; Tanaka, H.; Nishiuchi, T.; Song, K.J.; Ko, P.C.-I.; Leong, B.S.-H.; Khunkhlai, N.; Naroo, G.Y.; et al. Outcomes for out-of-hospital cardiac arrests across 7 countries in Asia: The Pan Asian Resuscitation Outcomes Study (PAROS). Resuscitation 2015, 96, 100–108. [Google Scholar] [CrossRef]
- Chan, P.S.; McNally, B.; Tang, F.; Kellermann, A. Recent trends in survival from out-of-hospital cardiac arrest in the United States. Circulation 2014, 130, 1876–1882. [Google Scholar] [CrossRef] [Green Version]
- Ahn, K.O.; Shin, S.D.; Suh, G.J.; Cha, W.C.; Song, K.J.; Kim, S.J.; Lee, E.J.; Ong, M.E.H. Epidemiology and outcomes from non-traumatic out-of-hospital cardiac arrest in Korea: A nationwide observational study. Resuscitation 2010, 81, 974–981. [Google Scholar] [CrossRef]
- Lim, H.C.; Tham, K.Y. Out of hospital cardiac arrests--the experience of one hospital in Singapore. Resuscitation 2001, 51, 123–127. [Google Scholar] [CrossRef]
- Berg, D.D.; Bobrow, B.J.; Berg, R.A. Key components of a community response to out-of-hospital cardiac arrest. Nat. Rev. Cardiol. 2019, 16, 407–416. [Google Scholar] [CrossRef]
- Luo, S.; Zhang, Y.; Zhang, W.; Zheng, R.; Tao, J.; Xiong, Y. Prognostic significance of spontaneous shockable rhythm conversion in adult out-of-hospital cardiac arrest patients with initial non-shockable heart rhythms: A systematic review and meta-analysis. Resuscitation 2017, 121, 1–8. [Google Scholar] [CrossRef]
- Kiyohara, K.; Nishiyama, C.; Kitamura, T.; Matsuyama, T.; Sado, J.; Shimamoto, T.; Kobayashi, D.; Kiguchi, T.; Okabayashi, S.; Kawamura, T.; et al. The association between public access defibrillation and outcome in witnessed out-of-hospital cardiac arrest with shockable rhythm. Resuscitation 2019, 140, 93–97. [Google Scholar] [CrossRef]
- Ringh, M.; Rosenqvist, M.; Hollenberg, J.; Jonsson, M.; Fredman, D.; Nordberg, P.; Järnbert-Pettersson, H.; Hasselqvist-Ax, I.; Riva, G.; Svensson, L. Mobile-phone dispatch of laypersons for CPR in out-of-hospital cardiac arrest. N. Engl. J. Med. 2015, 372, 2316–2325. [Google Scholar] [CrossRef]
- Jonsson, M.; Härkönen, J.; Ljungman, P.; Rawshani, A.; Nordberg, P.; Svensson, L.; Herlitz, J.; Hollenberg, J. Survival after out-of-hospital cardiac arrest is associated with area-level socioeconomic status. Heart 2019, 105, 632–638. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.Y.; Wang, J.Y.; Teng, N.C.; Chao, T.T.; Tsai, S.L.; Chen, C.L.; Hsu, J.Y.; Wu, C.P.; Lai, C.C.; Chen, L. The secular trends in the incidence rate and outcomes of out-of-hospital cardiac arrest in Taiwan--a nationwide population-based study. PLoS ONE 2015, 10, e0122675. [Google Scholar] [CrossRef] [Green Version]
- Fosbøl, E.L.; Dupre, M.E.; Strauss, B.; Swanson, D.R.; Myers, B.; McNally, B.F.; Anderson, M.L.; Bagai, A.; Monk, L.; Garvey, J.L.; et al. Association of neighborhood characteristics with incidence of out-of-hospital cardiac arrest and rates of bystander-initiated CPR: Implications for community-based education intervention. Resuscitation 2014, 85, 1512–1517. [Google Scholar] [CrossRef]
- Chiang, W.C.; Ko, P.C.; Chang, A.M.; Chen, W.T.; Liu, S.S.; Huang, Y.S.; Chen, S.Y.; Lin, C.H.; Cheng, M.T.; Chong, K.M.; et al. Bystander-initiated CPR in an Asian metropolitan: Does the socioeconomic status matter? Resuscitation 2014, 85, 53–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.Y.; Song, K.J.; Shin, S.D.; Ro, Y.S.; Hong, K.J.; Kim, Y.T.; Hong, S.O.; Park, J.H.; Lee, S.C. A disparity in outcomes of out-of-hospital cardiac arrest by community socioeconomic status: A ten-year observational study. Resuscitation 2018, 126, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Wells, D.M.; White, L.L.; Fahrenbruch, C.E.; Rea, T.D. Socioeconomic status and survival from ventricular fibrillation out-of-hospital cardiac arrest. Ann. Epidemiol. 2016, 26, 418–423.e1. [Google Scholar] [CrossRef] [PubMed]
- Lerner, E.B.; Rea, T.D.; Bobrow, B.J.; Acker, J.E., III; Berg, R.A.; Brooks, S.C.; Cone, D.C.; Gay, M.; Gent, L.M.; Mears, G.; et al. Emergency medical service dispatch cardiopulmonary resuscitation prearrival instructions to improve survival from out-of-hospital cardiac arrest: A scientific statement from the American Heart Association. Circulation 2012, 125, 648–655. [Google Scholar] [CrossRef]
- Teo, M.H.N.; Wong, W.E.J.; Daniel, P.C.-Y.N.; Kweh, R.H.C.; Ho, R.Y.J.; Koh, J.H.; Leong, S.-H.B.; Pang, J.; Hwang, Y.-F.J. The use of dispatcher assistance in improving the quality of cardiopulmonary resuscitation: A randomised controlled trial. Resuscitation 2019, 138, 153–159. [Google Scholar] [CrossRef] [Green Version]
- Harjanto, S.; Na, M.X.; Hao, Y.; Ng, Y.Y.; Doctor, N.; Goh, E.S.; Leong, B.S.-H.; Gan, H.N.; Chia, M.Y.C.; Tham, L.P.; et al. A before-after interventional trial of dispatcher-assisted cardio-pulmonary resuscitation for out-of-hospital cardiac arrests in Singapore. Resuscitation 2016, 102, 85–93. [Google Scholar] [CrossRef]
- Hagihara, A.; Onozuka, D.; Shibuta, H.; Hasegawa, M.; Nagata, T. Dispatcher-assisted bystander cardiopulmonary resuscitation and survival in out-of-hospital cardiac arrest. Int. J. Cardiol. 2018, 265, 240–245. [Google Scholar] [CrossRef]
- Park, J.H.; Ro, Y.S.; Shin, S.D.; Song, K.J.; Hong, K.J.; Kong, S.Y. Dispatcher-assisted bystander cardiopulmonary resuscitation in rural and urban areas and survival outcomes after out-of-hospital cardiac arrest. Resuscitation 2018, 125, 1–7. [Google Scholar] [CrossRef]
- Lee, S.Y.; Ro, Y.S.; Shin, S.D.; Song, K.J.; Ahn, K.O.; Kim, M.J.; Hong, S.O.; Kim, Y.T. Interaction effects between highly-educated neighborhoods and dispatcher-provided instructions on provision of bystander cardiopulmonary resuscitation. Resuscitation 2016, 99, 84–91. [Google Scholar] [CrossRef]
- Lu, C.H.; Fang, P.H.; Lin, C.H. Dispatcher-assisted cardiopulmonary resuscitation for traumatic patients with out-of-hospital cardiac arrest. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 97. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.F.W.; Sim, Z.J.; Shahidah, N.; Hao, Y.; Ng, Y.Y.; Leong, B.S.; Zarinah, S.; Teo, W.K.L.; Goh, G.S.Y.; Jaafar, H.; et al. Barriers to dispatcher-assisted cardiopulmonary resuscitation in Singapore. Resuscitation 2016, 105, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.C.; Duncan, G.J.; McDonough, P.; Williams, D.R. Optimal indicators of socioeconomic status for health research. Am. J. Public Health 2002, 92, 1151–1157. [Google Scholar] [PubMed]
- Becker, L.B.; Han, B.H.; Meyer, P.M.; Wright, F.A.; Rhodes, K.V.; Smith, D.W.; Barrett, J. Racial differences in the incidence of cardiac arrest and subsequent survival. The CPR Chicago Project. N. Engl. J. Med. 1993, 329, 600–606. [Google Scholar] [CrossRef]
- Iwashyna, T.J.; Christakis, N.A.; Becker, L.B. Neighborhoods matter: A population-based study of provision of cardiopulmonary resuscitation. Ann. Emerg. Med. 1999, 34, 459–468. [Google Scholar] [PubMed] [Green Version]
- Mitchell, M.J.; Stubbs, B.A.; Eisenberg, M.S. Socioeconomic status is associated with provision of bystander cardiopulmonary resuscitation. Prehospital Emerg. Care 2009, 13, 478–486. [Google Scholar] [CrossRef]
- Vaillancourt, C.; Lui, A.; De Maio, V.J.; Wells, G.A.; Stiell, I.G. Socioeconomic status influences bystander CPR and survival rates for out-of-hospital cardiac arrest victims. Resuscitation 2008, 79, 417–423. [Google Scholar] [CrossRef]
- Government Tainan City, Taiwan, Bureau of Land Administration. Available online: https://land.tainan.gov.tw/index.aspx (accessed on 1 July 2018).
- Lin, C.H.; Chiang, W.C.; Ma, M.H.; Wu, S.Y.; Tsai, M.C.; Chi, C.H. Use of automated external defibrillators in patients with traumatic out-of-hospital cardiac arrest. Resuscitation 2013, 84, 586–591. [Google Scholar] [CrossRef]
- Nuño, T.; Bobrow, B.J.; Rogge-Miller, K.A.; Panczyk, M.; Mullins, T.; Tormala, W. Disparities in telephone CPR access and timing during out-of-hospital cardiac arrest. Resuscitation 2017, 115, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Meischke, H.; Ike, B.; Painter, I.; Chavez, D.; Yip, M.P.; Bradley, S.M.; Tu, S.-P. Delivering 9-1-1 CPR Instructions to Limited English Proficient Callers: A Simulation Experiment. J. Immigr. Minor Health 2015, 17, 1049–1054. [Google Scholar] [CrossRef]
- Rostanski, S.K.; Kummer, B.R.; Miller, E.C.; Marshall, R.S.; Williams, O.; Willey, J.Z. Impact of Patient Language on Emergency Medical Service Use and Prenotification for Acute Ischemic Stroke. Neurohospitalist 2019, 9, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N.R.; Weiss, S.J.; Tate, R.; Oglesbee, S.; Ernst, A.A. Language disparities in patients transported by emergency medical services. Am. J. Emerg. Med. 2015, 33, 1737–1741. [Google Scholar] [CrossRef] [PubMed]
- Hollenberg, J.; Claesson, A.; Ringh, M.; Nordberg, P.; Hasselqvist-Ax, I.; Nord, A. Effects of native language on CPR skills and willingness to intervene in out-of-hospital cardiac arrest after film-based basic life support training: A subgroup analysis of a randomised trial. BMJ Open 2019, 9, e025531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandel, T.L.; Chao, W.Y.; Liang, C.H. Language Shift and Language Accommodation across Family Generations in Taiwan. J. Multiling. Multicult. Dev. 2006, 27, 126–147. [Google Scholar] [CrossRef]
- Lee, S.Y.; Ro, Y.S.; Shin, S.D.; Song, K.J.; Hong, K.J.; Park, J.H.; Kong, S.Y. Recognition of out-of-hospital cardiac arrest during emergency calls and public awareness of cardiopulmonary resuscitation in communities: A multilevel analysis. Resuscitation 2018, 128, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Swor, R.; Khan, I.; Domeier, R.; Honeycutt, L.; Chu, K.; Compton, S. CPR training and CPR performance: Do CPR-trained bystanders perform CPR? Acad. Emerg. Med. 2006, 13, 596–601. [Google Scholar] [CrossRef] [Green Version]
- Beard, M.; Swain, A.; Dunning, A.; Baine, J.; Burrowes, C. How effectively can young people perform dispatcher-instructed cardiopulmonary resuscitation without training? Resuscitation 2015, 90, 138–142. [Google Scholar] [CrossRef]
- Takei, Y.; Kamikura, T.; Nishi, T.; Maeda, T.; Sakagami, S.; Kubo, M.; Inaba, H. Recruitments of trained citizen volunteering for conventional cardiopulmonary resuscitation are necessary to improve the outcome after out-of-hospital cardiac arrests in remote time-distance area: A nationwide population-based study. Resuscitation 2016, 105, 100–108. [Google Scholar] [CrossRef]
- Li, H.; Shen, X.; Xu, X.; Wang, Y.; Chu, L.; Zhao, J.; Inaba, H. Bystander cardiopulmonary resuscitation training in primary and secondary school children in China and the impact of neighborhood socioeconomic status: A prospective controlled trial. Medicine 2018, 97, e12673. [Google Scholar] [CrossRef]
- Fang, P.H.; Lin, Y.Y.; Lu, C.H.; Lee, C.C.; Lin, C.H. Impacts of Emergency Medical Technician Configurations on Outcomes of Patients with Out-of-Hospital Cardiac Arrest. Int. J. Environ. Res. Public Health 2020, 17, 1930. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.H.; Ng, Y.Y.; Chiang, W.C.; Karim, S.A.; Shin, S.D.; Tanaka, H.; Nishiuchi, T.; Kajino, K.; Khunkhlai, N.; Ma, H.-M.; et al. Variation of current protocols for managing out-of-hospital cardiac arrest in prehospital settings among Asian countries. J. Formos. Med. Assoc. 2016, 115, 628–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| OHCA | High SES (n = 1656) | Middle SES (n = 1025) | Low SES (n = 247) | p Value |
|---|---|---|---|---|
| Age (years) (mean ± SD) | 68.5 ± 16.7 | 70.6 ± 16.0 | 69.5 ± 14.5 | 0.010 * |
| Age (>65 years) (n, %) | 984 (59.4%) | 664 (64.8%) | 156 (63.2%) | 0.017 * |
| Male (n, %) | 1056 (63.8%) | 650 (63.4%) | 161 (65.2%) | 0.874 |
| Public areas (n, %) | 152 (9.2%) | 88 (8.6%) | 17 (6.9%) | 0.475 |
| Witnessed (n, %) | 781 (47.2%) | 567 (55.3%) | 129 (52.2%) | <0.001 * |
| EMS Response time (min) (mean ± SD) | 6.5 ± 2.6 | 8.3 ± 4.0 | 9.8 ± 5.8 | <0.001 * |
| EMS Scene time (min) (mean ± SD) | 10.6 ± 5.2 | 10.3 ± 9.0 | 10.6 ± 7.4 | <0.001 * |
| EMS Transportation time (min) (mean ± SD) | 6.0 ± 4.9 | 9.0 ± 5.4 | 14.4 ± 7.5 | <0.001 * |
| High quality of DA-CPR (n, %) | 306 (18.5%) | 166 (16.2%) | 38 (15.4%) | 0.215 |
| Shockable rhythm (n, %) | 251 (15.2%) | 141 (13.8%) | 25 (10.1%) | 0.092 |
| Bystander CPR (n, %) | 450 (27.2%) | 316 (30.8%) | 51 (20.6%) | 0.004 * |
| Prehospital ROSC (n, %) | 85 (5.1%) | 25 (2.4%) | 9 (3.6%) | 0.003 * |
| Ever ROSC (n, %) | 455 (27.5%) | 210 (20.5%) | 48 (19.4%) | <0.001 * |
| Sustained ROSC (n, %) | 359 (21.7%) | 174 (17.0%) | 38 (15.4%) | 0.003 * |
| Survival to discharge (n, %) | 129 (7.8%) | 72 (7.0%) | 17 (6.9%) | 0.718 |
| Good neurologic outcome at discharge (n, %) | 62 (3.7%) | 11 (1.1%) | 3 (1.2%) | <0.001 * |
| OHCA | High SES (n = 1656) | Middle SES (n = 1025) | Low SES (n = 247) | p Value |
|---|---|---|---|---|
| Dispatcher recognition of cardiac arrest (n, %) | 633 (38.2%) | 387 (37.8%) | 77 (31.2%) | 0.099 |
| Time of dispatcher recognition of cardiac arrest (sec) (mean ± SD) | 43.9 ± 35.3 | 41.7 ± 37.1 | 64.1 ± 76.4 | 0.004 * |
| Early dispatcher recognition of cardiac arrest (≤60 s) (n, %) | 499 (30.1%) | 319 (31.1%) | 54 (21.9%) | 0.029 |
| Dispatcher initiation of CPR (n, %) | 563 (34.0%) | 332 (32.4%) | 69 (27.9%) | 0.151 |
| High quality of DA-CPR (n, %) | 306 (18.5%) | 166 (16.2%) | 38 (15.4%) | 0.215 |
| OHCA | Sustained ROSC (n = 571) | Non-sustained ROSC (n = 2357) | p Value |
|---|---|---|---|
| Age (years) (mean ± SD) | 66.5 ± 16.0 | 70.0 ± 16.3 | <0.001 |
| Age (> 65 years) (n, %) | 311 (54.5%) | 1493 (63.4%) | <0.001 |
| Male (n, %) | 353 (61.8%) | 1514 (64.2%) | 0.282 |
| High SES group (n, %) | 359 (62.9%) | 1297 (55.0%) | 0.001 |
| Middle SES group (n, %) | 174 (30.5%) | 851 (36.1%) | 0.011 |
| Low SES group (n, %) | 38 (6.7%) | 209 (8.9%) | 0.088 |
| Response time (min) (mean ± SD) | 6.8 ± 3.1 | 7.5 ± 3.8 | <0.001 |
| Scene time (min) (mean ± SD) | 9.7 ± 4.8 | 10.7 ± 7.4 | 0.001 |
| Transportation time (min) (mean ± SD) | 7.2 ± 5.9 | 7.9 ± 5.9 | 0.021 |
| Dispatcher recognition of cardiac arrest (n, %) | 162 (28.4%) | 935 (39.7%) | <0.001 |
| Time of dispatcher recognition of cardiac arrest (sec) (mean ± SD) | 50.8 ± 49.9 | 43.4 ± 38.5 | 0.032 |
| Dispatcher initiation of CPR (n, %) | 144 (25.2%) | 820 (34.8%) | <0.001 |
| High quality of DA-CPR (n, %) | 84 (14.7%) | 426 (18.1%) | 0.057 |
| Witnessed (n, %) | 390 (68.3%) | 1087 (46.1%) | <0.001 |
| Public location (n, %) | 82 (14.4%) | 175 (7.4%) | <0.001 |
| Epinephrine use (n, %) | 41 (7.2%) | 99 (4.2%) | 0.003 |
| LMA use (n, %) | 452 (79.2%) | 1917 (81.3%) | 0.236 |
| Shockable (n, %) | 128 (22.4%) | 289 (12.3%) | <0.001 |
| Bystander CPR (n, %) | 176 (30.8%) | 641 (27.2%) | 0.083 |
| Prehospital ROSC (n, %) | 80 (14.0%) | 39 (1.7%) | <0.001 |
| Ever ROSC (n, %) | 545 (95.4%) | 168 (17.1%) | <0.001 |
| Survival to discharge (n, %) | 201 (35.2%) | 17 (0.7%) | <0.001 |
| Good neurologic outcome at discharge (n, %) | 74 (13.0%) | 2 (0.1%) | <0.001 |
| OHCA | Unadjusted Odds Ratio (95% CIs) | p Value | Adjusted Odds Ratio (95% CIs) | p Value |
|---|---|---|---|---|
| Age (>65 y/o) | 0.69 (0.58–0.83) | <0.001 * | ||
| Male | 0.90 (0.75–1.09) | 0.282 | ||
| High SES group | 1.38 (1.15–1.67) | <0.001 * | 1.54 (1.06–2.23) | 0.024 * |
| Middle SES group | 0.78 (0.64–0.95) | 0.011 * | ||
| Low SES group | 0.73 (0.51–1.05) | 0.088 | ||
| Response time (≤5 min) | 1.47 (1.21–1.78) | <0.001 * | 1.50 (1.04–2.16) | 0.031 * |
| Scene time (≤8 min) | 1.53 (1.26–1.84) | <0.001 * | ||
| Transportation time (≤5 min) | 1.25 (1.03–1.50) | 0.021 * | ||
| Dispatcher recognition of cardiac arrest | 0.60 (0.49–0.74) | <0.001 * | ||
| Early dispatcher recognition of cardiac arrest (≤60 s) | 0.63 (0.44–0.92) | 0.015 * | ||
| Dispatcher initiation of CPR | 0.63 (0.51–0.78) | <0.001 * | ||
| High quality of DA-CPR | 0.78 (0.61–1.01) | 0.057 | ||
| Witnessed | 2.52 (2.07–3.06) | <0.001 * | 1.63 (1.15–2.32) | 0.007 * |
| Public location | 2.09 (1.58–2.77) | <0.001 * | ||
| Epinephrine use | 1.76 (1.21–2.57) | 0.003 * | ||
| LMA use | 0.87 (0.70–1.09) | 0.236 | ||
| Shockable rhythm | 2.07 (1.64–2.61) | <0.001 * | 3.49 (2.30–5.30) | <0.001 * |
| Bystander CPR | 1.19 (0.98–1.46) | 0.083 | 1.45 (1.03–2.06) | 0.036 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzeng, C.-F.; Lu, C.-H.; Lin, C.-H. Community Socioeconomic Status and Dispatcher-Assisted Cardiopulmonary Resuscitation for Patients with Out-of-Hospital Cardiac Arrest. Int. J. Environ. Res. Public Health 2021, 18, 1207. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031207
Tzeng C-F, Lu C-H, Lin C-H. Community Socioeconomic Status and Dispatcher-Assisted Cardiopulmonary Resuscitation for Patients with Out-of-Hospital Cardiac Arrest. International Journal of Environmental Research and Public Health. 2021; 18(3):1207. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031207
Chicago/Turabian StyleTzeng, Ching-Fang, Chien-Hsin Lu, and Chih-Hao Lin. 2021. "Community Socioeconomic Status and Dispatcher-Assisted Cardiopulmonary Resuscitation for Patients with Out-of-Hospital Cardiac Arrest" International Journal of Environmental Research and Public Health 18, no. 3: 1207. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031207