Influences of Recreational Tennis-Playing Exercise Time on Cardiometabolic Health Parameters in Healthy Elderly: The ExAMIN AGE Study


Abstract
:1. Introduction
2. Materials and Methods
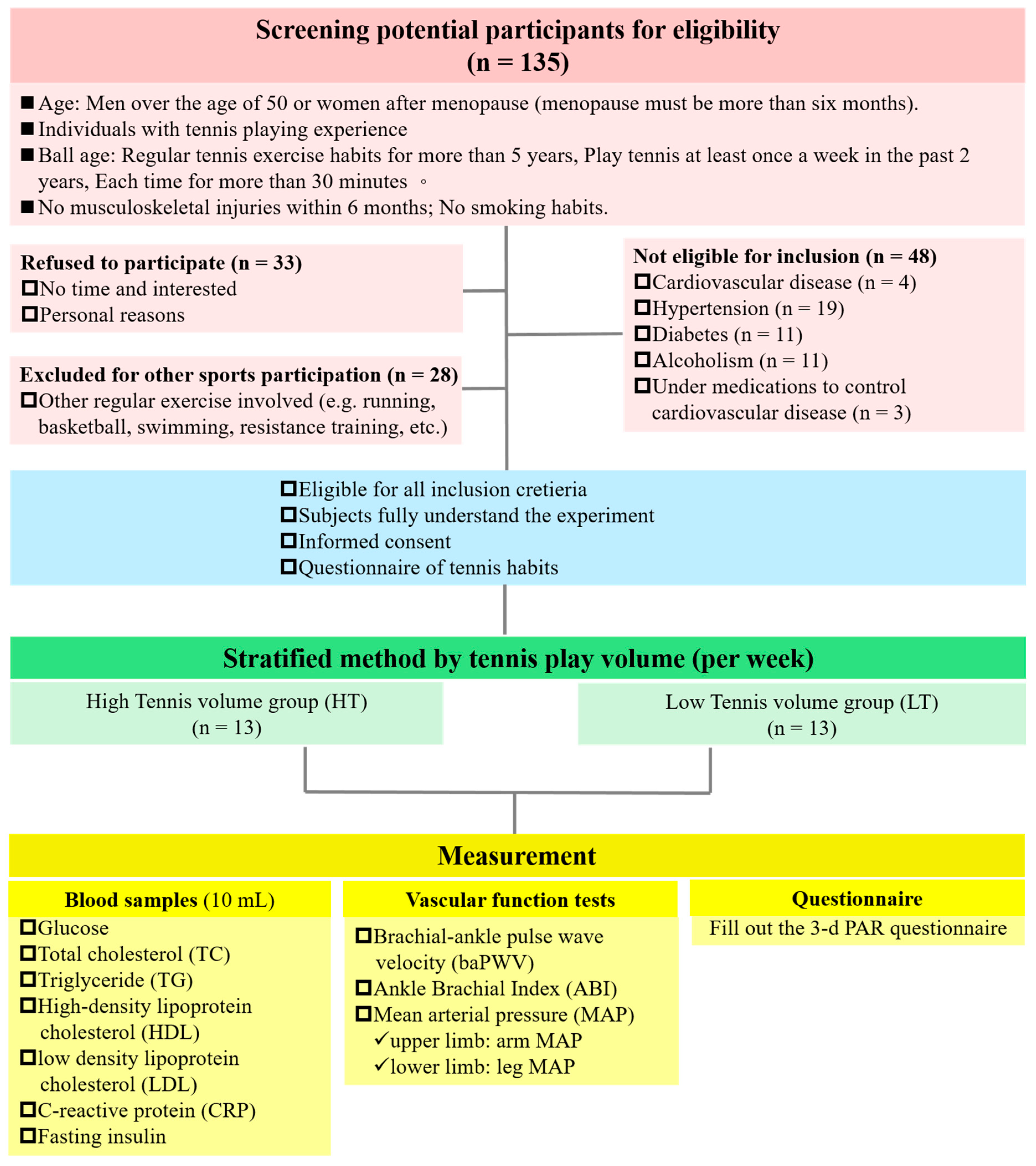
2.1. Participants and Ethical Statement
2.2. Study Design
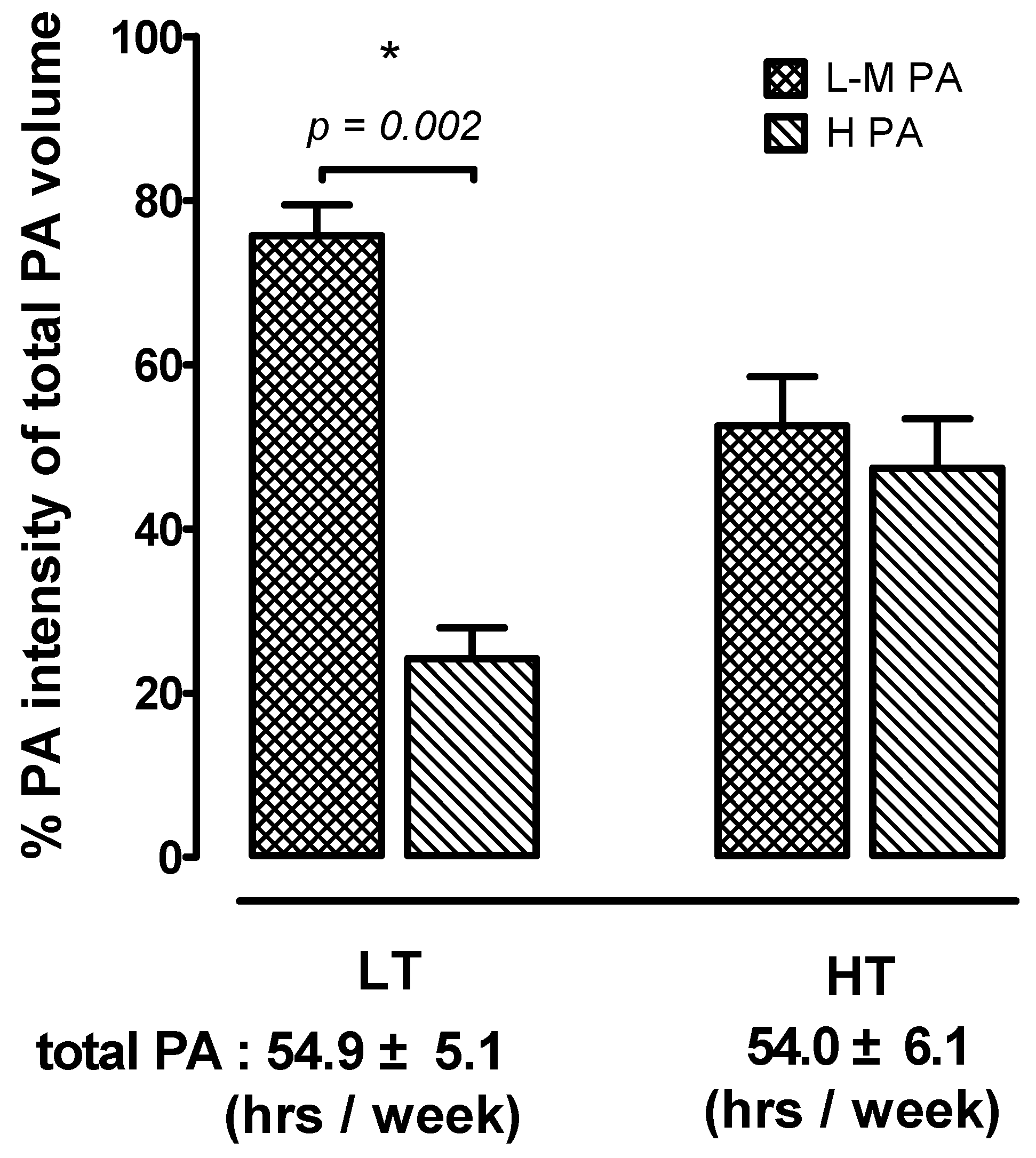
2.3. Physical Activity and Exercise Intensity/Duration Analyses
2.4. The Calculation Method for Tennis Playing Time
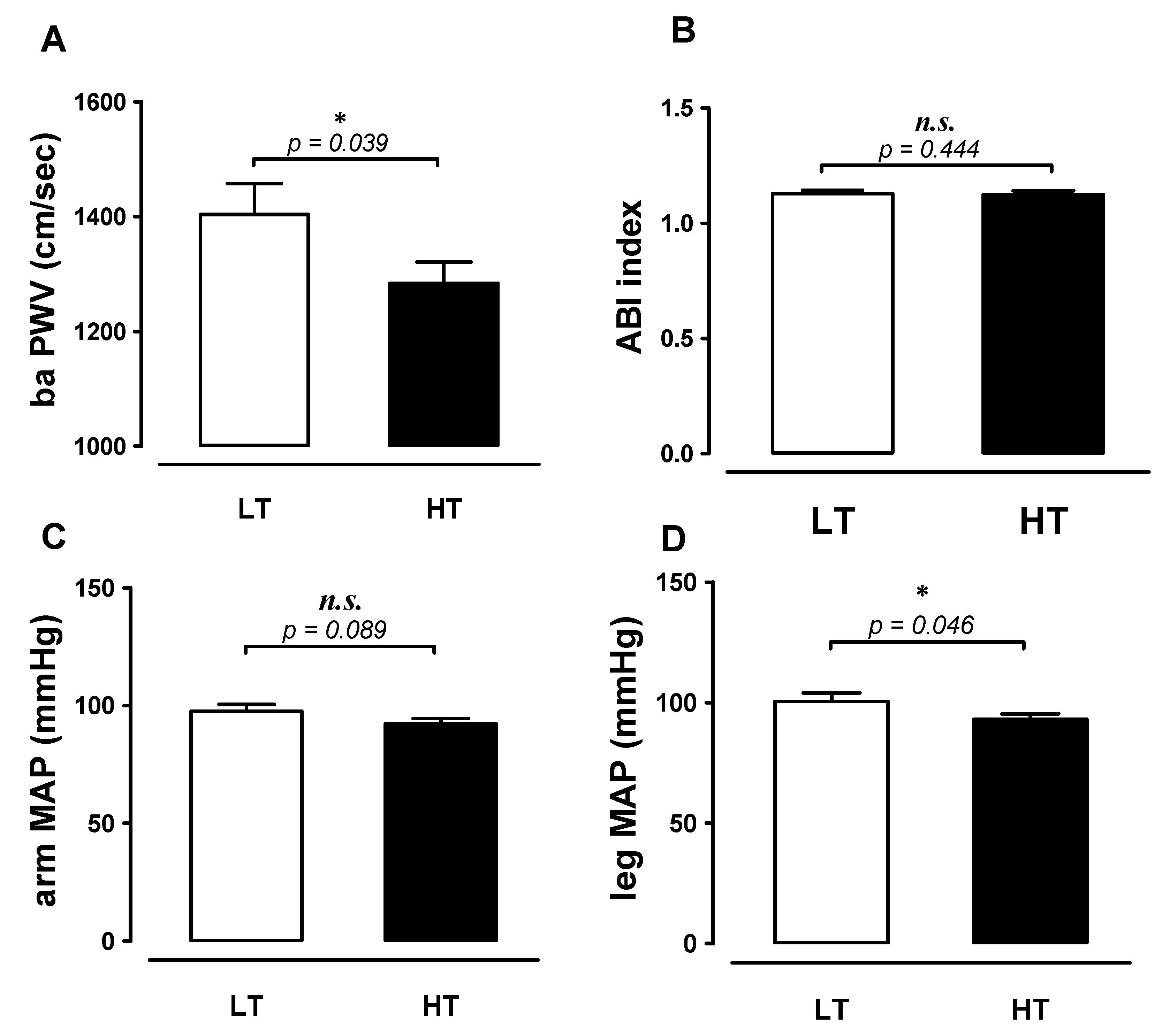
2.5. Brachial-Ankle Pulse Wave Velocity (baPWV) and Other Hemodynamics Measurements
2.6. Blood Metabolic Health Biomarkers Analyses
2.7. Homeostasis Model Assessment of Insulin Resistance (HOMA-IR Index)
2.8. Statistical Analyses
3. Results
3.1. Participant’s Anthropometry
3.2. Amount of Tennis Playing and Physical Activity
3.3. Differences in Blood Metabolic Health-Related Biomarkers
3.4. Differences in baPWV to Varied Tennis Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sui, X.; LaMonte, M.J.; Laditka, J.N.; Hardin, J.W.; Chase, N.; Hooker, S.P.; Blair, S.N. Cardiorespiratory fitness and adiposity as mortality predictors in older adults. J. Am. Med. Assoc. 2007, 298, 2507–2516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, K.E.; Thompson, P.D.; Caspersen, C.J.; Kendrick, J.S. Physical activity and the incidence of coronary heart disease. Annu. Rev. Public Health 1987, 8, 253–287. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N.; Kohl, H.W.; Paffenbarger, R.S.; Clark, D.G.; Cooper, K.H.; Gibbons, L.W. Physical fitness and all-cause mortality: A prospective study of healthy men and women. J. Am. Med. Assoc. 1989, 262, 2395–2401. [Google Scholar] [CrossRef]
- Shephard, R.J.; Balady, G.J. Exercise as cardiovascular therapy. Circulation 1999, 99, 963–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, A.S. Insulin resistance with aging: Effects of diet and exercise. Sports Med. 2000, 30, 327–346. [Google Scholar] [CrossRef]
- Deiseroth, A.; Streese, L.; Köchli, S.; Wüst, R.S.; Infanger, D.; Schmidt-Trucksäss, A.; Hanssen, H. Exercise and arterial stiffness in the elderly: A combined cross-sectional and randomized controlled trial (examin age). Front. Physiol. 2019, 10, 1119. [Google Scholar] [CrossRef] [Green Version]
- Hussain, S.R.; Macaluso, A.; Pearson, S.J. High-intensity interval training versus moderate-intensity continuous training in the prevention/management of cardiovascular disease. Cardiol. Rev. 2016, 24, 273–281. [Google Scholar] [CrossRef]
- Groppel, J.; DiNubile, N. Tennis: For the health of it! Phys. Sportsmed. 2009, 37, 40–50. [Google Scholar] [CrossRef]
- Kovacs, M.S. Tennis physiology: Training the competitive athlete. Sports Med. 2007, 37, 189–198. [Google Scholar] [CrossRef]
- Marks, B. Health benefits for veteran (senior) tennis players. Br. J. Sports Med. 2006, 40, 469–476. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Fernandez, J.; Sanz-Rivas, D.; Sanchez-Muñoz, C.; Pluim, B.M.; Tiemessen, I.; Mendez-Villanueva, A. A comparison of the activity profile and physiological demands between advanced and recreational veteran tennis players. J. Strength Cond. Res. 2009, 23, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Bekraoui, N.; Fargeas-Gluck, M.A.; Léger, L. Oxygen uptake and heart rate response of 6 standardized tennis drills. Appl. Physiol. Nutr. Metab. 2012, 37, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Oja, P.; Kelly, P.; Pedisic, Z.; Titze, S.; Bauman, A.; Foster, C.; Hamer, M.; Hillsdon, M.; Stamatakis, E. Associations of specific types of sports and exercise with all-cause and cardiovascular-disease mortality: A cohort study of 80306 British adults. Br. J. Sports Med. 2016, 51, 812–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chomistek, A.K.; Cook, N.R.; Flint, A.J.; Rimm, E.B. Vigorous-intensity leisure-time physical activity and risk of major chronic disease in men. Med. Sci. Sports Exerc. 2012, 44, 1898–1905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, N.; Fujie, S.; Horii, N.; Miyamoto-Mikami, E.; Tsuji, K.; Uchida, M.; Hamaoka, T.; Tabata, I.; Iemitsu, M. Effects of different exercise modes on arterial stiffness and nitric oxide synthesis. Med. Sci. Sports Exerc. 2018, 50, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Fu, J.; Sun, S.; Zhao, G.; Cheng, W.; Dou, C.; Quan, M. Effects of HIIT and MICT on cardiovascular risk factors in adults with overweight and/or obesity: A meta-analysis. PLoS ONE 2019, 14, e0210644. [Google Scholar] [CrossRef] [PubMed]
- Jelleyman, C.; Yates, T.; O’Donovan, G.; Gray, L.J.; King, J.A.; Khunti, K.; Davies, M.J. The effects of high-intensity interval training on glucose regulation and insulin resistance: A meta-analysis. Obes. Rev. 2015, 16, 942–961. [Google Scholar] [CrossRef] [Green Version]
- Hemmatinafar, M.; Kordi, M.; Choopani, S.; Choobineh, S.; Gharari Arefi, R. The effect of high intensity interval training (HIIT) on plasma adiponectin levels, insulin sensitivity and resistance in sedentary young men. J. Adv. Med. Biomed. Res. 2013, 21, 1–12. [Google Scholar]
- Hwang, C.L.; Yoo, J.K.; Kim, H.K.; Hwang, M.H.; Handberg, E.M.; Petersen, J.W.; Christou, D.D. Novel all-extremity high-intensity interval training improves aerobic fitness, cardiac function and insulin resistance in healthy older adults. Exp. Gerontol. 2016, 82, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Lakatta, E.G. Arterial and cardiac aging: Major shareholders in cardiovascular disease enterprises part III: Cellular and molecular clues to heart and arterial aging. Circulation 2003, 107, 490–497. [Google Scholar] [CrossRef] [Green Version]
- Mattace-Raso, F.U.S.; van der Cammen, T.J.M.; Hofman, A.; van Popele, N.M.; Bos, M.L.; Schalekamp, M.A.D.H.; Asmar, R.; Reneman, R.S.; Hoeks, A.P.G.; Breteler, M.M.B.; et al. Arterial stiffness and risk of coronary heart disease and stroke. Circulation 2006, 113, 657–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334. [Google Scholar] [CrossRef] [PubMed]
- Muniyappa, R.; Sowers, J.R. Role of insulin resistance in endothelial dysfunction. Rev. Endocr. Metab. Disord. 2013, 14, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Jia, G.; Sowers, J.R. Endothelial dysfunction potentially interacts with impaired glucose metabolism to increase cardiovascular risk. Hypertension 2014, 64, 1192–1193. [Google Scholar] [CrossRef] [Green Version]
- Bouchard, C.; Tremblay, A.; Leblanc, C.; Lortie, G.; Savard, R.; Thériault, G. A method to assess energy expenditure in children and adults. Am. J. Clin. Nutr. 1983, 37, 461–467. [Google Scholar] [CrossRef]
- Yamashina, A.; Tomiyama, H.; Takeda, K.; Tsuda, H.; Arai, T.; Hirose, K.; Koji, Y.; Hori, S.; Yamamoto, Y. Validity, reproducibility, and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement. Hypertens. Res. 2002, 25, 359–364. [Google Scholar] [CrossRef] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Gando, Y.; Yamamoto, K.; Murakami, H.; Ohmori, Y.; Kawakami, R.; Sanada, K.; Higuchi, M.; Tabata, I.; Miyachi, M. Longer time spent in light physical activity is associated with reduced arterial stiffness in older adults. Hypertension 2010, 56, 540–546. [Google Scholar] [CrossRef] [Green Version]
- Davis, M.G.; Fox, K.R. Physical activity patterns assessed by accelerometry in older people. Eur. J. Appl. Physiol. 2007, 100, 581–589. [Google Scholar] [CrossRef]
- Ferrauti, A.; Bergeron, M.F.; Pluim, B.M.; Weber, K. Physiological responses in tennis and running with similar oxygen uptake. Eur. J. Appl. Physiol. 2001, 85, 27–33. [Google Scholar] [CrossRef]
- Pluim, B.M.; Groppel, J.L.; Miley, D.; Crespo, M.; Turner, M.S. Health benefits of tennis. Br. J. Sports Med. 2018, 52, 201–202. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, M.; Pluim, B.; Groppel, J.; Crespo, M.; Roetert, E.P.; Hainline, B.; Miller, S.; Reid, M.; Pestre, B.; De Vylder, M.; et al. Health, Wellness and Cognitive Performance Benefits of Tennis. J. Med. Sci. Tennis 2016, 21, 14–21. [Google Scholar]
- Mitranun, W.; Deerochanawong, C.; Tanaka, H.; Suksom, D. Continuous vs interval training on glycemic control and macro- and microvascular reactivity in type 2 diabetic patients. Scand. J. Med. Sci. Sports 2014, 24, e69–e76. [Google Scholar] [CrossRef] [PubMed]
- Marcinko, K.; Sikkema, S.R.; Samaan, M.C.; Kemp, B.E.; Fullerton, M.D.; Steinberg, G.R. High intensity interval training improves liver and adipose tissue insulin sensitivity. Mol. Metab. 2015, 4, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Krentz, A.J.; Viljoen, A.; Sinclair, A. Insulin resistance: A risk marker for disease and disability in the older person. Diabet. Med. 2013, 30, 535–548. [Google Scholar] [CrossRef]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef]
- Joyner, M.J.; Casey, D.P. Regulation of increased blood flow (hyperemia) to muscles during exercise: A hierarchy of competing physiological needs. Physiol. Rev. 2015, 95, 549–601. [Google Scholar] [CrossRef] [Green Version]
- Tinken, T.M.; Thijssen, D.H.; Hopkins, N.; Dawson, E.A.; Cable, N.T.; Green, D.J. Shear stress mediates endothelial adaptations to exercise training in humans. Hypertension 2010, 55, 312–318. [Google Scholar] [CrossRef] [Green Version]
- Green, D.J.; Fowler, D.T.; O’Driscoll, J.G.; Blanksby, B.A.; Taylor, R.R. Endothelium-derived nitric oxide activity in forearm vessels of tennis players. J. Appl. Physiol. 1996, 81, 943–948. [Google Scholar] [CrossRef]
- Kagaya, A.; Ohmori, F.; Okuyama, S.; Muraoka, Y.; Sato, K. Blood flow and arterial vessel diameter change during graded handgrip exercise in dominant and non-dominant forearms of tennis players. Adv. Exp. Med. Biol. 2010, 662, 365–370. [Google Scholar]
- Green, D.J.; Smith, K.J. Effects of exercise on vascular function, structure, and health in humans. Cold Spring Harb. Perspect. Med. 2018, 8, a029819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos, J.S.; Dalleck, L.C.; Tjonna, A.E.; Beetham, K.S.; Coombes, J.S. The impact of high-intensity interval training versus moderate-intensity continuous training on vascular function: A systematic review and meta-analysis. Sports Med. 2015, 45, 679–692. [Google Scholar] [CrossRef] [PubMed]
- Ashor, A.W.; Lara, J.; Siervo, M.; Celis-Morales, C.; Mathers, J.C. Effects of Exercise Modalities on Arterial Stiffness and Wave Reflection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2014, 9, e110034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tordi, N.; Mourot, L.; Colin, E.; Regnard, J. Intermittent versus constant aerobic exercise: Effects on arterial stiffness. Eur. J. Appl. Physiol. 2010, 108, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, F.G.R.; Hiatt, W.R.; Jönsson, B.; Lacroix, P.; et al. Measurement and interpretation of the ankle-brachial index: A scientific statement from the American Heart Association. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heikkilä, A.; Venermo, M.; Kautiainen, H.; Aarnio, P.; Korhonen, P. Physical Activity Improves Borderline Ankle–Brachial Index Values in a Cardiovascular Risk Population. Ann. Vasc. Surg. 2016, 32, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, B.B.; Dobrosielski, D.A.; Althouse, A.D.; Stewart, K.J. The effect of exercise training on ankle-brachial index in type 2 diabetes. Atherosclerosis 2013, 230, 125–130. [Google Scholar] [CrossRef]
- Endes, S.; Schaffner, E.; Caviezel, S.; Dratva, J.; Autenrieth, C.S.; Wanner, M.; Martin, B.; Stolz, D.; Pons, M.; Turk, A.; et al. Long-term physical activity is associated with reduced arterial stiffness in older adults: Longitudinal results of the SAPALDIA cohort study. Age Ageing 2016, 45, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Sugawara, J.; Otsuki, T.; Tanabe, T.; Hayashi, K.; Maeda, S.; Matsuda, M. Physical activity duration, intensity, and arterial stiffening in postmenopausal women. Am. J. Hypertens. 2006, 19, 1032–1036. [Google Scholar] [CrossRef] [Green Version]
- Van de Laar, R.J.; Ferreira, I.; van Mechelen, W.; Prins, M.H.; Twisk, J.W.; Stehouwer, C.D. Lifetime vigorous but not light-to-moderate habitual physical activity impacts favorably on carotid stiffness in young adults: The Amsterdam growth and health longitudinal study. Hypertension 2010, 55, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Way, K.L.; Hackett, D.A.; Baker, M.K.; Johnson, N.A. The effect of regular exercise on insulin sensitivity in type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Metab. 2016, 40, 253–271. [Google Scholar] [CrossRef] [PubMed]
- Sandoo, A.; van Zanten, J.J.V.; Metsios, G.S.; Carroll, D.; Kitas, G.D. The endothelium and its role in regulating vascular tone. Open Cardiovasc. Med. J. 2010, 4, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Maeda, S.; Tanabe, T.; Otsuki, T.; Sugawara, J.; Iemitsu, M.; Miyauchi, T.; Kuno, S.; Ajisaka, R.; Matsuda, M. Moderate regular exercise increases basal production of nitric oxide in elderly women. Hypertens. Res. 2004, 27, 947–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rugbeer, N.; Ramklass, S.; Mckune, A.; Van Heerden, J. The effect of group exercise frequency on health related quality of life in institutionalized elderly. Pan Afr. Med. J. 2017, 26, 35. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081–1093. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables\Group | HT (n = 13, 8 M/5 F) | LT (n = 13, 7 M/6 F) | t |
|---|---|---|---|
| Height (cm) | 166.04 ± 1.83 | 162.21 ± 2.00 | −1.41 |
| Wight (kg) | 63.30 ± 2.59 | 62.90 ± 2.90 | −0.10 |
| BMI (kg/m2) | 22.92 ± 0.78 | 23.42 ± 0.61 | 0.51 |
| Age (year) | 61.54 ± 1.32 | 60.89 ± 1.07 | −0.38 |
| Tennis participated years (year) | 28.62 ± 0.84 | 22.77 ± 3.52 | −1.62 |
| Tennis play frequency (days/week) | 5.46 ± 0.24 | 3.27 ± 0.41 | −4.66 ** |
| Tennis play hours (h/day) | 2.60 ± 0.22 | 1.33 ± 0.14 | −4.92 ** |
| Total tennis play time (h/week) | 14.02 ± 1.32 | 4.47 ± 0.67 | −6.45 ** |
| Variables\Group | HT n = 13 | LT n = 13 | t | ES |
|---|---|---|---|---|
| Glucose (mg/dL) | 92.46 ± 1.29 | 95.38 ± 1.98 | 1.24 | 0.48 |
| CHOL (mg/dL) | 215.69 ± 8.37 | 208.92 ± 7.40 | −0.61 | 0.24 |
| TG (mg/dL) | 86.77 ± 12.16 | 65.46 ± 7.03 | −1.52 | 0.60 |
| HDL (mg/dL) | 66.56 ± 4.67 | 62.94 ± 4.01 | −0.59 | 0.23 |
| LDL (mg/dL) | 126.08 ± 8.56 | 124.46 ± 5.14 | −0.16 | 0.06 |
| CRP (mg/dL) | 0.40 ± 0.23 | 0.09 ± 0.03 | −1.32 | 0.05 |
| Insulin (μU/mL) | 6.17 ± 0.49 | 9.55 ± 1.92 | 1.70 * | 0.67 |
| HOMA-IR | 1.41 ± 0.11 | 2.27 ± 0.48 | 1.76 * | 0.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chao, H.-H.; Liao, Y.-H.; Chou, C.-C. Influences of Recreational Tennis-Playing Exercise Time on Cardiometabolic Health Parameters in Healthy Elderly: The ExAMIN AGE Study. Int. J. Environ. Res. Public Health 2021, 18, 1255. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031255
Chao H-H, Liao Y-H, Chou C-C. Influences of Recreational Tennis-Playing Exercise Time on Cardiometabolic Health Parameters in Healthy Elderly: The ExAMIN AGE Study. International Journal of Environmental Research and Public Health. 2021; 18(3):1255. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031255
Chicago/Turabian StyleChao, Hsiao-Han, Yi-Hung Liao, and Chun-Chung Chou. 2021. "Influences of Recreational Tennis-Playing Exercise Time on Cardiometabolic Health Parameters in Healthy Elderly: The ExAMIN AGE Study" International Journal of Environmental Research and Public Health 18, no. 3: 1255. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031255