
Effects of a HIIT Protocol on Cardiovascular Risk Factors in a Type 1 Diabetes Mellitus Population




Abstract
:1. Introduction
2. Materials and Methods
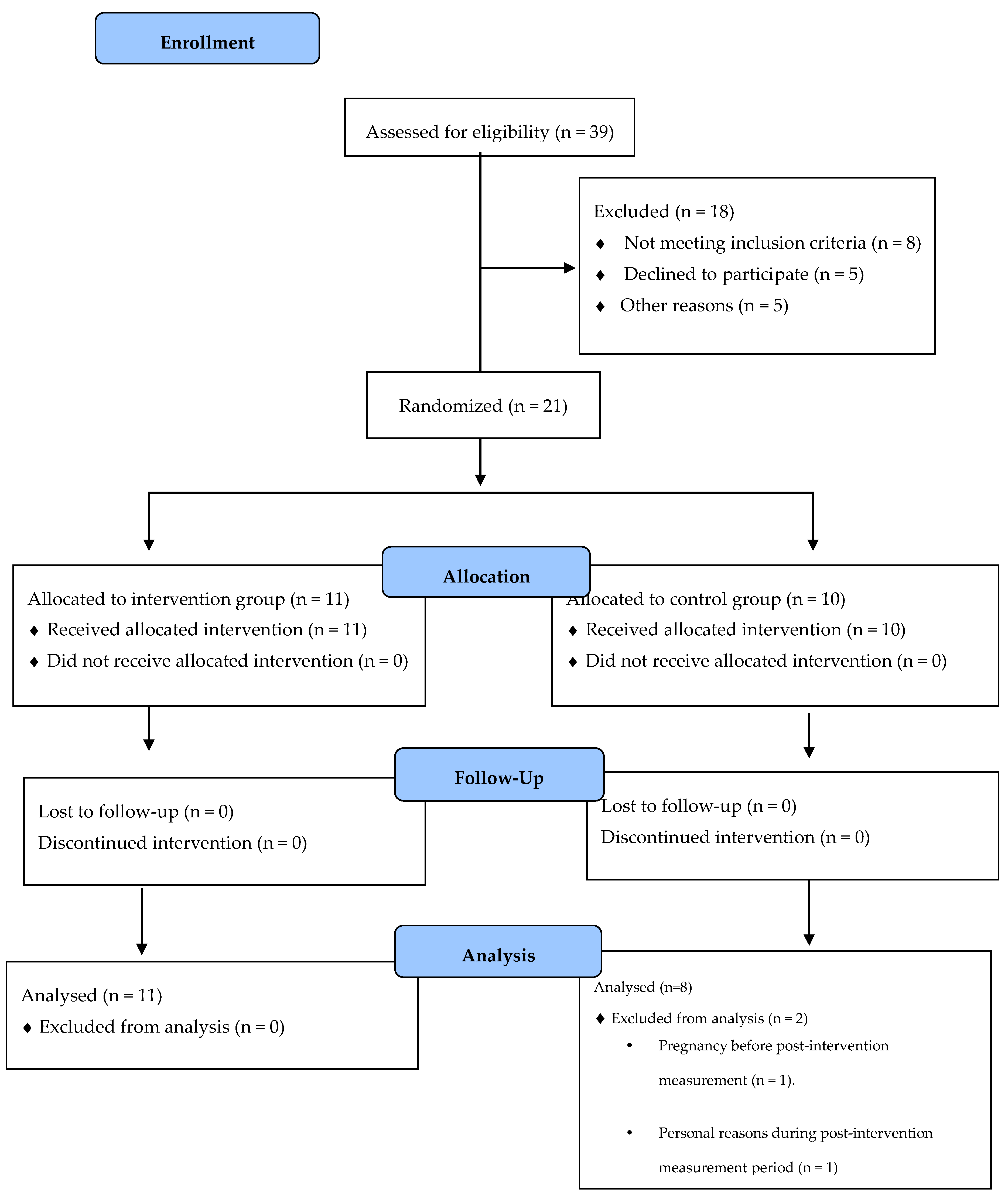
2.1. Participants
2.2. Experimental Design
2.3. Procedures
2.3.1. Body Composition
2.3.2. Heart Rate Variability
2.3.3. VO2max and Peak Power Output
2.3.4. Fasting Glucose
2.4. Training Protocol
2.5. Statistical Analysis
3. Results
3.1. Adverse Events
3.2. Cardiovascular Risk Factor Outcomes
3.2.1. VO2max
3.2.2. Body Composition
3.2.3. Heart Rate Variability
3.2.4. Fasting Glucose
4. Discussion
4.1. VO2max
4.2. Body Composition
4.3. Heart Rate Variability
4.4. Fasting Glucose
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Riddell, M.C.; Gallen, I.W.; Smart, C.E.; Taplin, C.E.; Adolfsson, P.; Lumb, A.N.; Kowalski, A.; Rabasa-Lhoret, R.; McCrimmon, R.J.; Hume, C.; et al. Exercise management in type 1 diabetes: A consensus statement. Lancet Diabetes Endocrinol. 2017, 5, 377–390. [Google Scholar] [CrossRef] [Green Version]
- International Diabetes Federation. Atlas de la Diabetes de la FID, 9th ed.; International Diabetes Federation: Brussels, Belguim, 2019; Available online: www.diabetesatlas.org (accessed on 15 November 2020).
- WHO. OMS|Informe Mundial Sobre la Diabetes; WHO (World Health Organization): Geneva, Switzerland, 2016. [Google Scholar]
- Farinha, J.B.; Krause, M.; Rodrigues-Krause, J.; Reischak-Oliveira, A. Exercise for type 1 diabetes mellitus management: General considerations and new directions. Med Hypotheses 2017, 104, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Katsarou, A.; Gudbjörnsdottir, S.; Rawshani, A.; Dabelea, D.; Bonifacio, E.; Anderson, B.; Jacobsen, L.M.; Schatz, D.A. Lernmark, Åke Type 1 diabetes mellitus. Nat. Rev. Dis. Prim. 2017, 3, nrdp201716. [Google Scholar] [CrossRef]
- DiMeglio, L.A.; Evans-Molina, C.; A Oram, R. Type 1 diabetes. Lancet 2018, 391, 2449–2462. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [Green Version]
- Leroux, C.; Brazeau, A.-S.; Gingras, V.; Desjardins, K.; Strychar, I.; Rabasa-Lhoret, R. Lifestyle and Cardiometabolic Risk in Adults with Type 1 Diabetes: A Review. Can. J. Diabetes 2014, 38, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Yardley, J.E.; Hay, J.L.; Abou-Setta, A.M.; Marks, S.D.; McGavock, J. A systematic review and meta-analysis of exercise interventions in adults with type 1 diabetes. Diabetes Res. Clin. Pract. 2014, 106, 393–400. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; ACSM: Baltimore, MD, USA, 2020. [Google Scholar]
- Lascar, N.; Kennedy, A.; Hancock, B.; Jenkins, D.; Andrews, R.C.; Greenfield, S.; Narendran, P. Attitudes and Barriers to Exercise in Adults with Type 1 Diabetes (T1DM) and How Best to Address Them: A Qualitative Study. PLoS ONE 2014, 9, e108019. [Google Scholar] [CrossRef] [Green Version]
- Codella, R.; Terruzzi, I.; Luzi, L. Why should people with type 1 diabetes exercise regularly? Acta Diabetol. 2017, 54, 615–630. [Google Scholar] [CrossRef]
- Röhling, M.; Strom, A.; Bönhof, G.J.; Roden, M.; Ziegler, D. Cardiorespiratory Fitness and Cardiac Autonomic Function in Diabetes. Curr. Diabetes Rep. 2017, 17, 1–10. [Google Scholar] [CrossRef]
- Colberg, S.R.; Laan, R.; Dassau, E.; Kerr, D. Physical Activity and Type 1 Diabetes: Time for a rewire? J. Diabetes Sci. Technol. 2015, 9, 609–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle: Part II: Anaerobic energy, neuromuscular load and practical applications. Sports Med. 2013, 43, 927–954. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.R.; Macaluso, A.; Pearson, S.J. High-Intensity Interval Training Versus Moderate-Intensity Continuous Training in the Prevention/Management of Cardiovascular Disease. Cardiol. Rev. 2016, 24, 273–281. [Google Scholar] [CrossRef] [PubMed]
- De Nardi, A.T.; Tolves, T.; Lenzi, T.L.; Signori, L.U.; Da Silva, A.M.V. High-intensity interval training versus continuous training on physiological and metabolic variables in prediabetes and type 2 diabetes: A meta-analysis. Diabetes Res. Clin. Pract. 2018, 137, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Benichou, T.; Pereira, B.; Mermillod, M.; Tauveron, I.; Pfabigan, D.; Maqdasy, S.; Dutheil, F. Heart rate variability in type 2 diabetes mellitus: A systematic review and meta–analysis. PLoS ONE 2018, 13, e0195166. [Google Scholar] [CrossRef] [Green Version]
- Cygankiewicz, I.; Zareba, W. Heart Rate Variability. In Interventional Neuroradiology; Elsevier BV: Amsterdam, The Netherlands, 2013; Volume 117, pp. 379–393. [Google Scholar] [CrossRef]
- Taralov, Z.Z.; Terziyski, K.V.; Kostianev, S.S. Heart Rate Variability as a Method for Assessment of the Autonomic Nervous System and the Adaptations to Different Physiological and Pathological Conditions. Folia Med. 2016, 57, 173–180. [Google Scholar] [CrossRef] [Green Version]
- McCraty, R.; Shaffer, F. Heart Rate Variability: New Perspectives on Physiological Mechanisms, Assessment of Self-regulatory Capacity, and Health Risk. Glob. Adv. Health Med. 2015, 4, 46–61. [Google Scholar] [CrossRef] [Green Version]
- McGinn, R.; Kenny, G.P. Autonomic dysfunction associated with Type 1 diabetes: A role for fitness? Clin. Auton. Res. 2014, 24, 249–251. [Google Scholar] [CrossRef] [Green Version]
- Voulgari, C.; Pagoni, S.; Vinik, A.; Poirier, P. Exercise improves cardiac autonomic function in obesity and diabetes. Metabolism 2013, 62, 609–621. [Google Scholar] [CrossRef]
- De Abreu, R.M.; Rehder-Santos, P.; Simões, R.P.; Catai, A.M. Can high-intensity interval training change cardiac autonomic control? A systematic review. Braz. J. Phys. Ther. 2019, 23, 279–289. [Google Scholar] [CrossRef]
- Mottalib, A.; Kasetty, M.; Mar, J.Y.; Elseaidy, T.; Ashrafzadeh, S.; Hamdy, O. Weight Management in Patients with Type 1 Diabetes and Obesity. Curr. Diabetes Rep. 2017, 17, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riaz, H.; Khan, M.S.; Siddiqi, T.J.; Usman, M.S.; Shah, N.; Goyal, A.; Khan, S.S.; Mookadam, F.; Krasuski, R.A.; Ahmed, H. Association Between Obesity and Cardiovascular Outcomes: A Systematic Review and Meta-analysis of Mendelian Randomization Studies. JAMA Netw. Open 2018, 1, e183788. [Google Scholar] [CrossRef] [PubMed]
- Keating, S.E.; Johnson, N.A.; Mielke, G.I.; Coom, J.S. A systematic review and meta-analysis of interval training versus moderate-intensity continuous training on body adiposity. Obes. Rev. 2017, 18, 943–964. [Google Scholar] [CrossRef]
- Lee, A.S.; Johnson, N.A.; McGill, M.J.; Overland, J.; Luo, C.; Baker, C.J.; Martinez-Huenchullan, S.; Wong, J.; Flack, J.R.; Twigg, S.M. Effect of High-Intensity Interval Training on Glycemic Control in Adults with Type 1 Diabetes and Overweight or Obesity: A Randomized Controlled Trial with Partial Crossover. Diabetes Care 2020, 43, 2281–2288. [Google Scholar] [CrossRef] [PubMed]
- Minnebeck, K.; Vorona, E.; Zinn, S.; Gellner, R.; Hinder, J.; Brand, S.-M.; Kabar, I.; Alten, F.; Schmitz, B. Four weeks of high-intensity interval training (HIIT) improve the cardiometabolic risk profile of overweight patients with type 1 diabetes mellitus (T1DM). Eur. J. Sport Sci. 2020, 24, 1–11. [Google Scholar] [CrossRef]
- Scott, S.N.; Cocks, M.; Andrews, R.C.; Narendran, P.; Purewal, T.S.; Cuthbertson, D.J.; Wagenmakers, A.J.M.; Shepherd, S.O. High-Intensity Interval Training Improves Aerobic Capacity without a Detrimental Decline in Blood Glucose in People with Type 1 Diabetes. J. Clin. Endocrinol. Metab. 2018, 104, 604–612. [Google Scholar] [CrossRef]
- Farinha, J.B.; Ramis, T.R.; Vieira, A.F.; Macedo, R.C.; Rodrigues-Krause, J.; Boeno, F.P.; Schroeder, H.T.; Müller, C.H.; Boff, W.; Krause, M.; et al. Glycemic, inflammatory and oxidative stress responses to different high-intensity training protocols in type 1 diabetes: A randomized clinical trial. J. Diabetes Complicat. 2018, 32, 1124–1132. [Google Scholar] [CrossRef]
- Boff, W.; Da Silva, A.M.; Farinha, J.B.; Rodrigues-Krause, J.; Reischak-Oliveira, A.; Tschiedel, B.; Puñales, M.; Bertoluci, M.C. Superior Effects of High-Intensity Interval vs. Moderate-Intensity Continuous Training on Endothelial Function and Cardiorespiratory Fitness in Patients with Type 1 Diabetes: A Randomized Controlled Trial. Front. Physiol. 2019, 10, 450. [Google Scholar] [CrossRef]
- Petersmann, A.; Nauck, M.; Müller-Wieland, D.; Kerner, W.; Müller, U.A.; Landgraf, R.; Freckmann, G.; Heinemann, L. Definition, Classification and Diagnosis of Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2018, 126, 406–410. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.A.; Jiang, B.; McElwee-Malloy, M.; Wakeman, C.; Breton, M.D. Fluctuations of Hyperglycemia and Insulin Sensitivity Are Linked to Menstrual Cycle Phases in Women with T1D. J. Diabetes Sci. Technol. 2015, 9, 1192–1199. [Google Scholar] [CrossRef] [Green Version]
- Perrotta, A.S.; Jeklin, A.T.; Hives, B.A.; Meanwell, L.E.; Warburton, D.E. Validity of the Elite HRV Smartphone Application for Examining Heart Rate Variability in a Field-Based Setting. J. Strength Cond. Res. 2017, 31, 2296–2302. [Google Scholar] [CrossRef] [PubMed]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart Rate Variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Sassi, R.; Cerutti, S.; Lombardi, F.; Malik, M.; Huikuri, H.V.; Peng, C.-K.; Schmidt, G.; Yamamoto, Y.; Gorenek, B.; Lip, G.Y.; et al. Advances in heart rate variability signal analysis: Joint position statement by the e-Cardiology ESC Working Group and the European Heart Rhythm Association co-endorsed by the Asia Pacific Heart Rhythm Society. Europace 2015, 17, 1341–1353. [Google Scholar] [CrossRef]
- Alansare, A.B.; Alford, K.; Lee, S.; Church, T.; Jung, H.C. The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults. Int. J. Environ. Res. Public Health 2018, 15, 1508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piras, A.; Persiani, M.; Damiani, N.; Perazzolo, M.; Raffi, M. Peripheral heart action (PHA) training as a valid substitute to high intensity interval training to improve resting cardiovascular changes and autonomic adaptation. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 115, 763–773. [Google Scholar] [CrossRef]
- Tsekouras, Y.E.; Tambalis, K.D.; Sarras, S.E.; Antoniou, A.K.; Kokkinos, P.; Sidossis, L.S. Validity and Reliability of the New Portable Metabolic Analyzer PNOE. Front. Sports Act. Living 2019, 1, 24. [Google Scholar] [CrossRef]
- Klonoff, D.C.; Parkes, J.L.; Kovatchev, B.P.; Kerr, D.; Bevier, W.C.; Brazg, R.L.; Christiansen, M.; Bailey, T.S.; Nichols, J.H.; Kohn, M.A. Investigation of the Accuracy of 18 Marketed Blood Glucose Monitors. Diabetes Care 2018, 41, 1681–1688. [Google Scholar] [CrossRef] [Green Version]
- Scott, S.; Shepherd, S.O.; Andrews, R.C.; Narendran, P.; Purewal, T.S.; Kinnafick, F.; Cuthbertson, D.J.; Atkinson-Goulding, S.; Noon, T.; Wagenmakers, A.J.; et al. A Multidisciplinary Evaluation of a Virtually Supervised Home-Based High-Intensity Interval Training Intervention in People with Type 1 Diabetes. Diabetes Care 2019, 42, 2330–2333. [Google Scholar] [CrossRef] [Green Version]
- Ito, S. High-intensity interval training for health benefits and care of cardiac diseases—The key to an efficient exercise protocol. World J. Cardiol. 2019, 11, 171–188. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Pariser, G. Cardiorespiratory Fitness Levels and its Correlates Among Adults with Diabetes. Cardiopulm. Phys. Ther. J. 2013, 24, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Rissanen, A.-P.E.; Tikkanen, H.; Koponen, A.S.; Aho, J.M.; Peltonen, J.E. Central and Peripheral Cardiovascular Impairments Limit V·O2peak in Type 1 Diabetes. Med. Sci. Sports Exerc. 2015, 47, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Chimen, M.; Kennedy, A.; Nirantharakumar, K.; Pang, T.T.; Andrews, R.; Narendran, P. What are the health benefits of physical activity in type 1 diabetes mellitus? A literature review. Diabetologia 2012, 55, 542–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, S.; Shepherd, S.O.; Strauss, J.A.; Wagenmakers, A.J.M.; Cocks, M. Home-based high-intensity interval training reduces barriers to exercise in people with type 1 diabetes. Exp. Physiol. 2020, 105, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Madden, A.; Smith, S. Body composition and morphological assessment of nutritional status in adults: A review of anthropometric variables. J. Hum. Nutr. Diet. 2016, 29, 7–25. [Google Scholar] [CrossRef]
- Corbin, K.D.; A Driscoll, K.; E Pratley, R.; Smith, S.R.; Maahs, D.M.; Mayer-Davis, E.J. Obesity in Type 1 Diabetes: Pathophysiology, Clinical Impact, and Mechanisms. Endocr. Rev. 2018, 39, 629–663. [Google Scholar] [CrossRef] [Green Version]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef]
- Jelleyman, C.; Yates, T.L.; O’Donovan, G.; Gray, L.J.; King, J.A.; Khunti, K.; Davies, M.J. The effects of high-intensity interval training on glucose regulation and insulin resistance: A meta-analysis. Obes. Rev. 2015, 16, 942–961. [Google Scholar] [CrossRef] [Green Version]
- Moradi-Lakeh, M.; Forouzanfar, M.H.; El Bcheraoui, C.; Daoud, F.; Afshin, A.; Hanson, S.W.; Vos, T.; Naghavi, M.; Murray, C.J.; Mokdad, A.H. High Fasting Plasma Glucose, Diabetes, and Its Risk Factors in the Eastern Mediterranean Region, 1990–2013: Findings from the Global Burden of Disease Study 2013. Diabetes Care 2016, 40, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Schauer, I.E.; Snell-Bergeon, J.K.; Bergman, B.C.; Maahs, D.M.; Kretowski, A.; Eckel, R.H.; Rewers, M. Insulin Resistance, Defective Insulin-Mediated Fatty Acid Suppression, and Coronary Artery Calcification in Subjects with and without Type 1 Diabetes: The CACTI study. Diabetes 2010, 60, 306–314. [Google Scholar] [CrossRef] [Green Version]
- Monaco, C.M.F.; Hughes, M.C.; Ramos, S.V.; Varah, N.E.; Lamberz, C.; Rahman, F.A.; McGlory, C.; Tarnopolsky, M.A.; Krause, M.P.; Laham, R.; et al. Altered mitochondrial bioenergetics and ultrastructure in the skeletal muscle of young adults with type 1 diabetes. Diabetology 2018, 61, 1411–1423. [Google Scholar] [CrossRef] [Green Version]
- Calella, P.; Gallè, F.; Fornelli, G.; Liguori, G.; Valerio, G. Type 1 diabetes and body composition in youth: A systematic review. Diabetes/Metab. Res. Rev. 2020, 36, e3211. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| HIIT Group | Control Group | ||||
|---|---|---|---|---|---|
| Pre | Post | Pre | Post | ES | |
| VO2max (mL/min/kg). | 37.1 ± 4.1 | 40.4 ± 3.8 * | 37.0 ± 5.5 | 37.2 ± 5.1 | 0.71 |
| Fat Mass (Kg)/% Fat mass | 17.1 ± 4.4/24.2% ± 7.6 | 16.0 ± 4.2/22.4% ± 7.4 * | 15.4 ± 4.5/21.4% ± 9.6 | 15.3 ± 4.6/21.1% ± 9.8 | 0.16 |
| Lean Mass (Kg)/%Lean Mass | 53.5 ± 8.7/75.9% ± 7.7 | 55.3 ± 8.8/77.6% ± 7.4 * | 57.6 ± 9.8/79.9% ± 7.8 | 57.9 ± 10.0/80.2% ± 7.4 | 0.28 |
| rMSSD (ms). | 37.8 ± 27.9 | 44.3 ± 27.7 * | 40.0 ± 15.9 | 39.3 ± 16.5 | 0.22 |
| LF/HF ratio (ms2). | 2.6 ± 1.6 | 1.5 ± 0.9 * | 2.1 ± 2.0 | 1.9 ± 2.2 | 0.23 |
| Fasting Glucose (mg/dL). | 135 ± 24.9 | 124.5 ± 15.6 * | 131.8 ± 21.1 | 135.9 ± 25.0 | 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alarcón-Gómez, J.; Calatayud, J.; Chulvi-Medrano, I.; Martín-Rivera, F. Effects of a HIIT Protocol on Cardiovascular Risk Factors in a Type 1 Diabetes Mellitus Population. Int. J. Environ. Res. Public Health 2021, 18, 1262. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031262
Alarcón-Gómez J, Calatayud J, Chulvi-Medrano I, Martín-Rivera F. Effects of a HIIT Protocol on Cardiovascular Risk Factors in a Type 1 Diabetes Mellitus Population. International Journal of Environmental Research and Public Health. 2021; 18(3):1262. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031262
Chicago/Turabian StyleAlarcón-Gómez, Jesús, Joaquín Calatayud, Iván Chulvi-Medrano, and Fernando Martín-Rivera. 2021. "Effects of a HIIT Protocol on Cardiovascular Risk Factors in a Type 1 Diabetes Mellitus Population" International Journal of Environmental Research and Public Health 18, no. 3: 1262. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031262