1. Child Mortality Is (Still) a Worldwide Concern
Nearly 4% of the world’s children each year do not survive to their fifth birthday [
1]. Moreover, a large, growing, and worrisome disparity in Child Mortality (CM) exists between Low- and Middle-Income Countries (LMIC) and high-income countries. In high-income countries, advances in healthcare, access to clean water and sanitation, and improvements in overall quality of life have reduced the under-5 mortality rate to 5 per 1000 live births [
2]. These life enhancing conditions stand in contrast to conditions present in LMIC, where CM in 2018 was as high as 6.81% [
2]. Even in LMIC that enjoy improved conditions, vast disparities in risk and protective factors and mortality rates remain depending on household circumstances and locality. Reducing CM is an explicit goal of the United Nations Development Program [
3], which advocates for improvements in deleterious conditions that increase the likelihood of CM and for increased research to advance knowledge about which specific conditions are implicated in CM in different contexts. The global community recognizes the crucial need to end preventable child deaths, making it an essential part of the Global Strategy for Women’s, Children’s, and Adolescents’ Health (2016–2030) [
4] and UN Sustainable Development Goal 3 [
5]. In consequence, having evidence-based indications of specific factors (or combinations of factors) that carry the most weight in determining under-5 CM would contribute directly to designing tailored and more effective interventions.
Under-5 CM has both proximal and distal causes. Proximal causes are usually medical or biological conditions that result in human demise (i.e., preterm birth complications, pneumonia, congenital anomalies, sepsis, diarrhea and malaria [
6]). By the time a proximal cause of death is identified, it may be too late to save a child’s life. Much attention has rightly focused on proximal causes of CM over the years. However, proximal causes arise from known and unknown distal causes. On this account, the global heath community should be equally concerned with identifying distal causes that likely give rise to proximal causes of CM. Often, distal causes are treatable or even preventable obviating proximal causes. For example, diarrhea is a common proximal cause of CM, but poor sanitation or contaminated water are major distal causes of the proximal diarrhea cause of mortality in young children [
7].
Multiple potential distal causes have been identified, but research so far has focused on only a small number of distal causes at time. These restricted approaches help in understanding how and why a distal cause is associated with CM, but have inhibited identifying the relative importance of different causes. Organizations and institutions need to know which causes are more relevant and should be targeted first.
The primary aim of this study was to identify and order by predictive power distal causes that contribute to under-5 CM. To reach this aim, we applied Machine Learning (ML) to a large multivariate UNICEF dataset from a large number of LMIC.
2. Materials and Methods
In this study we used data from the Multiple Indicator Cluster Survey (MICS), an international household survey developed and supported by UNICEF. We selected and processed the dataset to obtain information about mothers and the environment in which they lived (see Participants). In particular, we selected MICS items that inform about distal causes potentially associated with CM.
We then applied a ML approach to automatically identify mothers who had at least one child who died before the age of 5 years, based on selected MICS items (see Predictive Performance of MICS Indicators for Under-5 Child Mortality).
From the trained model, we obtained the importance of the MICS items in terms of predictive potency, and analysed the top 10 items in terms of relevance to proximal causes of CM. Finally (see Predictive Confirmation of MICS Indicators in Reducing Under-5 Child Mortality), we retrospectively validate the results, by analysing how country-level variations of CM are associated with the variation of the percentage of households with improved conditions, across two administrations of the MICS.
2.1. Participants
The sample consisted in 275,160 mothers between the ages of 15 and 49 years (M = 32.85, SD = 8.44) from 247,247 households that were randomly selected from 27 LMIC (for the selection of the households see Section 1: MICS in
Supplementary Material). Mothers were classified as (a) mothers with no deceased child before the age of 5 years (noU5D) and (b) mothers with at least one child who died before the age of 5 years (U5D). The noU5D class could include mothers with a child who died after the age of 5 years. Data were extracted from the 2009–2013 and 2013–2017 (round 4 and 5) administrations of the MICS. All MICS indicators were screened, and 37 (see
Table 1) were selected as pertinent for this study (for the selection procedure see
Section 2: Data processing in
Supplementary Material). Ethics approvals were handled in each site in which data were collected.
2.2. Predictive Performance of MICS Indicators for under-5 Child Mortality
In this study we leverage on a ML model to extract information from the MICS dataset, similar to other data mining approaches [
8,
9]. A Random Forest model [
10], which is based on an ensemble of decision trees, was trained on the 37 MICS indicators to predict mother class (U5D v. noU5D) and identify indicators associated with CM. Having assessed the reliability of the model, we considered the importance of MICS indicators resulting from the training process (for the model optimization and stability see
Section 3: Analytical Plan of
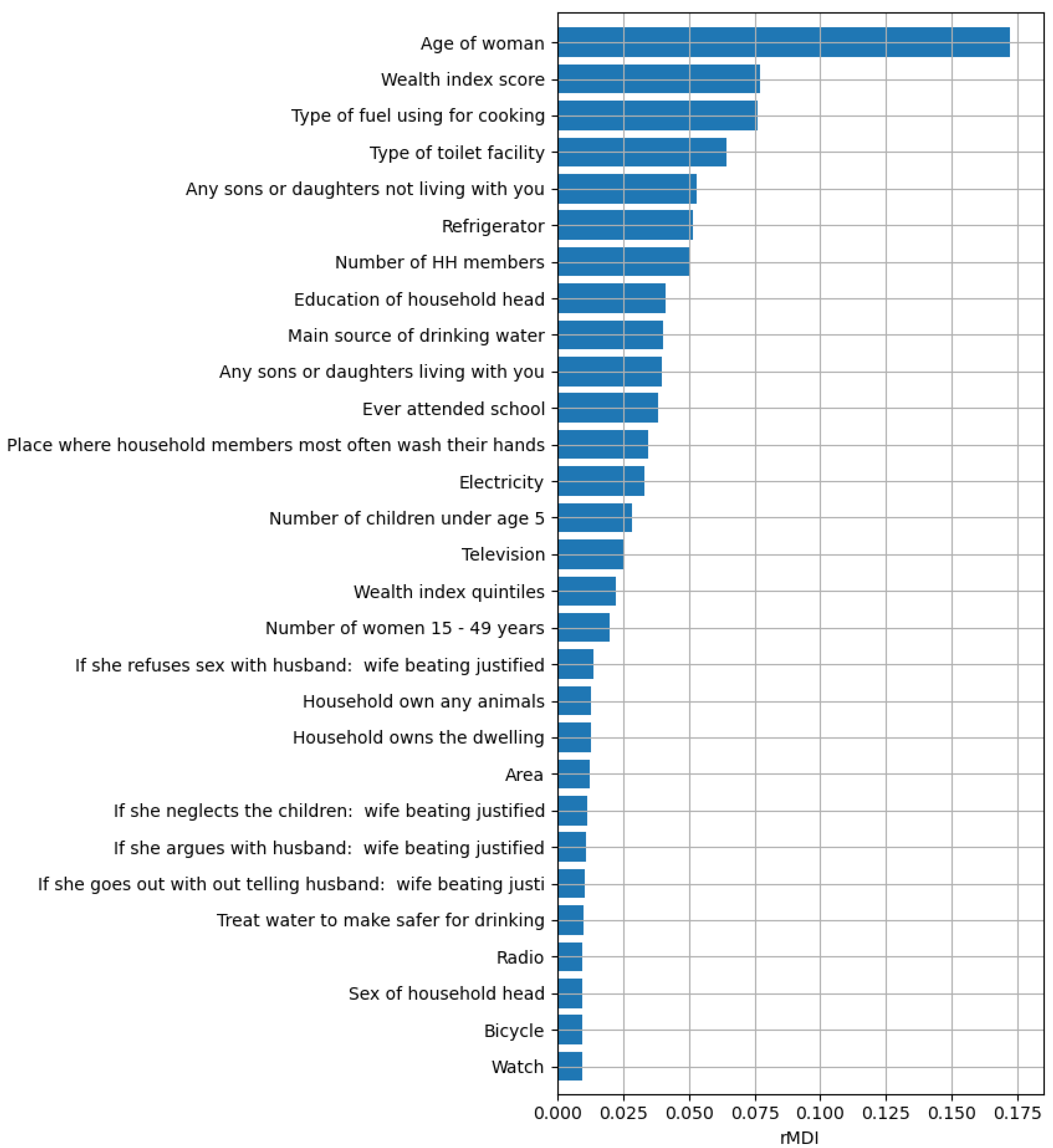
Supplementary Material). The ranked list of 29 residual indicators is shown in
Figure 1.
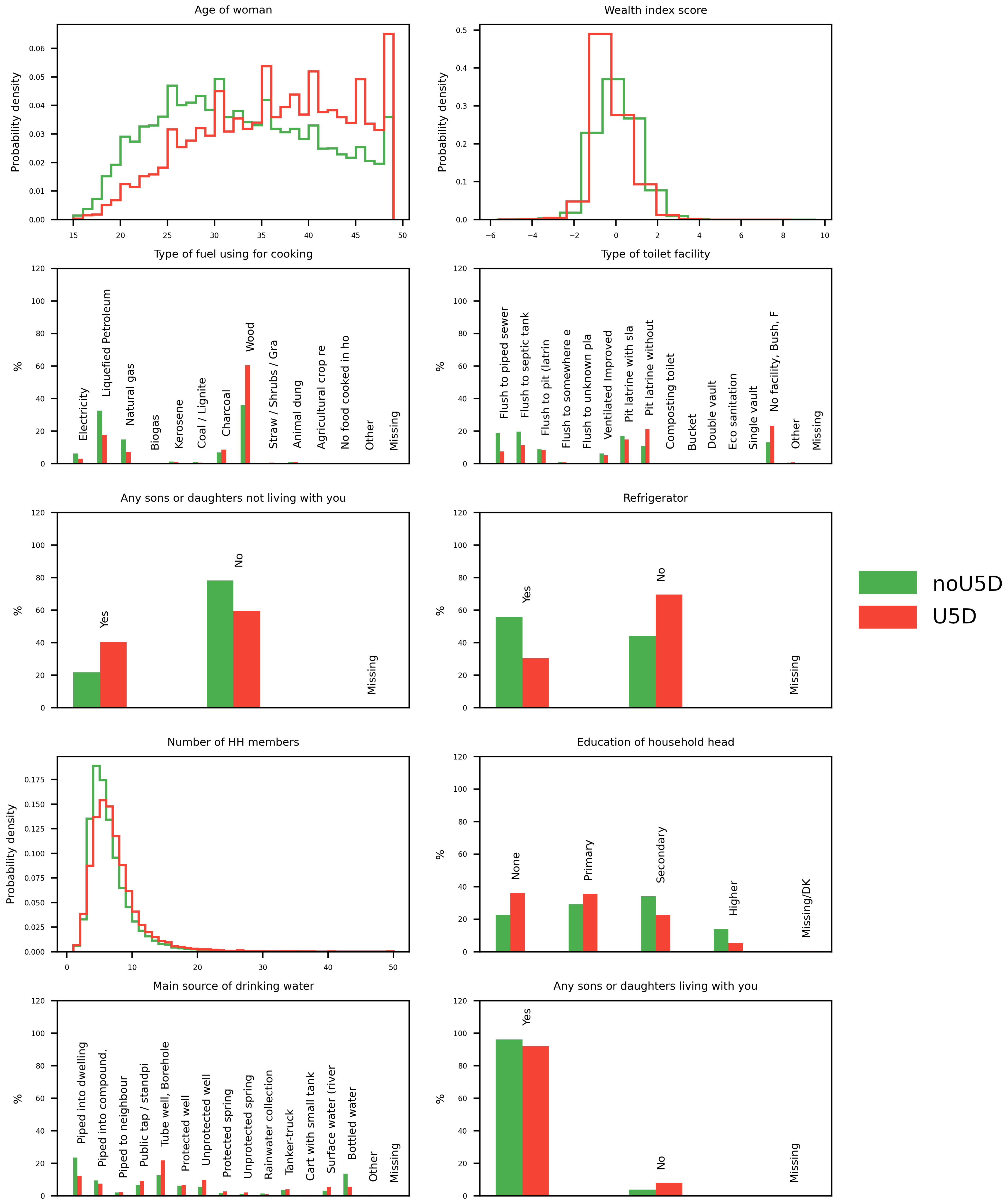
This ML analysis of 37 potential distal causes of under-5 CM in more than a quarter of a million households in 27 LMIC identified and prioritized the top 10 likely distal causes, whose distributions are shown in
Figure 2 (for the analysis of ML results see
Section 4: Machine Learning Results of
Supplementary Material).
The top 10 indicators naturally fall into 3 groups: 2 (#1 and #8) refer to characteristics of the mother or head of household, with older maternal age (rMDI = 0.172) and education of the head of the household (rMDI = 0.041) associated with greater likelihood of having had a child who died before the age of 5. Five of the top 10 predictors of CM refer to characteristics of the home environment, including #2 family wealth index score (rMDI = 0.077), #3 fuel used for cooking (rMDI = 0.076), #4 toilet facilities (rMDI = 0.064), #6 availability of refrigeration (rMDI = 0.052), and # 9 drinking water (rMDI = 0.04). Three personal characteristics of the household complete the top ten: #5 other (living) children not living in the household (rMDI = 0.053), #7 the number of household members (rMDI = 0.051), and #10 the number of children living in the household (rMDI = 0.04).
2.3. Predictive Confirmation of MICS Indicators in Reducing under-5 Child Mortality
The data set used to identify the top 10 distal causes of CM came from the 2009–2013 and 2013–2017 administrations of the MICS. To confirm the efficacy of these 10 distal causes in reducing CM, we used data from the 2005–2007 administration (round 3) of the MICS for 7 countries which took part in both the 2005–2007 and 2013–2017 MICS administrations and computed both the improvement in each distal cause and the change in CM between the two administrations (see
Section 3: Analytical Plan in
Supplementary Material).
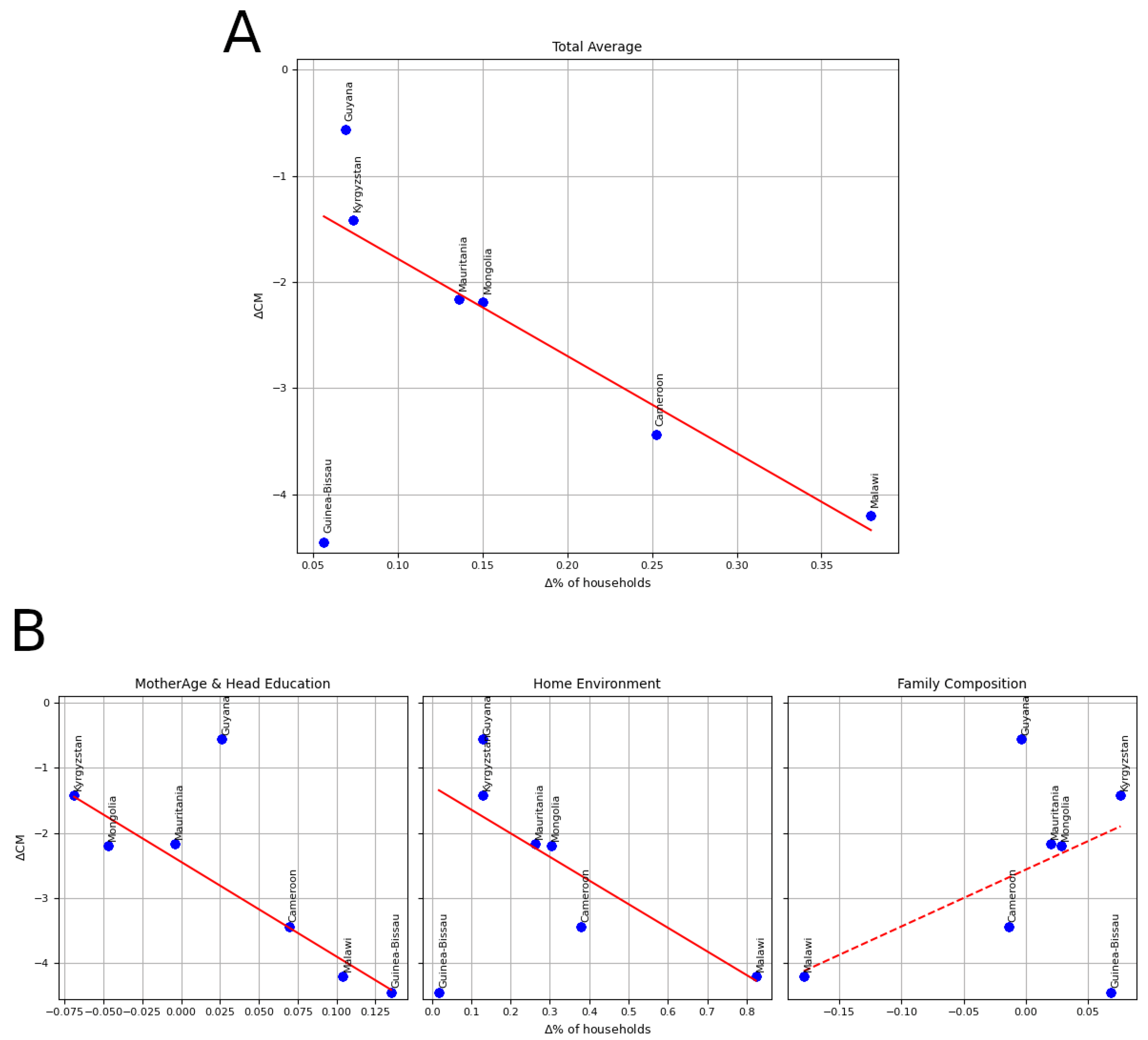
Next, we estimated the relevance of each group of distal causes in reducing CM [
11] by fitting a linear regression to predict the variation in CM (
CM) based on the variation of the percentage of households with improved characteristics of the identified distal causes (
%). Confirming the ML analysis, significant linear associations emerged for the first two groups of predictors and for the total improvement (
Figure 3 and
Table 2).
3. Distal Causes of Child Mortality
Notably, all 10 likely distal causes of CM are preventable and treatable using social, educational, or physical interventions. The overall improvement in the top 10 distal causes is significantly associated with the reduction of CM (). Here we discuss the top 10 distal causes, considering the three groups: characteristics of the mother and household head, the home environment, and household composition.
3.1. Characteristics of the Mother and Household Head
The improvement in the characteristics of the mother and household dead was significantly associated with the reduction in CM ().
3.1.1. Older Maternal Age
It has long been known that children born to very young (teenage) mothers are at increased risk of poor health outcomes and even death [
12], and that pregnancy timing associated with the healthiest outcomes for children occurs in mothers’ 20 s [
13]. We found that older maternal age was the strongest predictor of having had a child younger than 5 die. One interpretation is that older mothers have a greater probability of having more children and, as a consequence, greater probability of having a child who died before the age of 5. Alternately, there is greater risk for both maternal and CM at very old (as there is at very young) ages of mothers [
14]. Some MICS data support the first interpretation; two Pearson correlations (N = 644,009) showed associations between mothers’ age and their number of children,
, and number of children and number of deceased children,
. However, on the second interpretation it is also the case that mothers over 35 years are more likely to have preterm births, and intrauterine growth retardation and being born low birth weight are also more likely for children born to mothers over the age of 35 [
15]. Rates of chromosomal disorders and prematurity in offspring to older mothers are much greater than those to younger mothers [
15] as are congenital malformations [
16] and multiple births [
17]. For women over 50, these problems multiply [
18]. Whichever or both, our results (based on data going up to age 5 years) draw attention to the lesser recognized fact that, after infancy and in the aggregate, older maternal age is a strong predictor of having a child under-5 die.
3.1.2. Education of the Household Head
Children of mothers who lack any education are 2.6 times more likely to die before reaching age 5 compared to children of mothers with a secondary or higher education [
19]. Mothers’ education correlates significantly with nutritional and developmental gains of their children [
20]. Parent educational level predicts knowledge of child care and child development [
21].
3.2. The Home Environment
The improvement in the Home Environment was significantly associated with the reduction in the CM (p = 0.03919).
Scientists, policy makers, and humanitarians have long pointed to housing quality and its effects on human well-being [
22], including direct links to CM [
23]. Five of the top 10 predictors of CM involve characteristics of the home environment, including the family wealth index score, fuel used for cooking, toilet facilities, refrigeration, and quality of drinking water.
3.2.1. Family Wealth
Along with education and occupation, family wealth is a central component of socio-economic status [
24]. Socio-economic status is associated with differences in parenting behaviours that are connected with nutrition and health promotion, such as prenatal care and breastfeeding, beginning very early in a child’s life [
25]. Children with low socio-economic status are more likely to suffer injuries and to die, even in high-income countries [
26], as their homes often have safety hazards (e.g., water heaters set too high in temperature) and lack safety protections (e.g., smoke alarms; [
27]). Likewise, poor families are likely to live in places that increase children’s exposure to pollutants and neurotoxins, with negative implications for health and survival [
28]. Under-5 mortality rates are, on average, twice as high for the poorest households in LMIC compared to the richest [
29].
3.2.2. Cooking Fuel
Not having electricity imposes problems on health as families are forced to resort to solid biofuels to cook or to provide heat. Such devices often produce smoke that is not properly ventilated, and resultant high levels of indoor pollutants contribute to premature child death. Having an open stove with no chimney in the household increases indoor pollutants that pose health risks, just as open fires in a house increase susceptibility to respiratory illness [
30]. In LMIC, acute respiratory illness is a leading proximal cause of death among young children, but acute respiratory illness is associated with exposure to indoor air pollution [
27]. Exposure to wood smoke has other adverse health consequences for children as well. Inadequate ventilation increases the likelihood of childhood asthma, respiratory infections, and inflammations. The World Health Organization estimated that 2.3 billion people in LMIC use biomass fuels or coal for cooking, particularly those living in rural areas with limited access to electricity [
31].
3.2.3. Toilet Facilities
Not having proper facilities to deal with waste contributes to childhood illness and mortality [
32]. To reduce CM, it is critical to eliminate children’s exposure to excreta. In rural areas around the world, less than half the population has access to improved sanitation facilities [
33]. In some informal urban settlements in poor Asian, African, and South American cities, mortality rates among young children are estimated at 150–200 per 1000 [
34] where the largest number of cases involve diarrhea, which is caused by bacterial, viral, and parasitic pathogens connected to poor hygiene and sanitation [
35].
3.2.4. Refrigeration
Food-borne illnesses are common when homes lack adequate facilities for food preparation and storage, which often means food is left out for later consumption, thus increasing the likelihood of contamination [
36]. Many pathogens multiply more quickly at room temperature than when refrigerated or frozen, which creates a risk for food contamination and gastro-intestinal illness [
37]. Cooking foods often kills bacteria in the short term, but microbes quickly multiply when cooked foods are not properly stored. Contamination of foods used to wean the child from the breast is a leading cause of diarrheal disease and malnutrition in children under 5 [
38]. Thus, having facilities for properly storing and refrigerating food is critical to reducing disease exposure.
3.2.5. Drinking Water
Children without access to clean water are at much higher risk of diarrheal diseases and for waterborne diseases, such as cholera and enteric fevers. Lack of access to clean water is also a major contributor to poor nutritional status [
39], and diarrhea and intestinal parasites contribute to malnutrition [
40]. Data from 74 countries revealed that under-5s were most likely to live in houses that had no access to clean water [
41]. Even when communities or countries make provisions for improving access to drinking water, the source of water and the manner in which water is transported undermine children’s health. Children’s vulnerability to pathogens from contaminated water relates to their exposure: Children actively explore their environments and are unaware of sanitation conditions that can lead to morbidities through disruptions in the immune system. When water does not come into the house, storage becomes a contamination issue. Young children may dip their hands into water or drop water scoops on the floor, which then becomes a source of disease [
42].
3.3. Household Composition
Three characteristics of household composition complete the top 10 determinants of CM we identified. They are other (living) children not living in the household, the number of household members, and the number of children living in the household. Perhaps the second two relate commonly to pernicious generic effects of crowding in the household and, in combination with the first, to the division of finite parenting resources.
The association between improvement of Household Composition and reduction in CM was not significant (
p = 0.10907): this might be due to the fact that these distal causes require more time to show their effects on the reduction in CM or because distal factors can work and combine in a variety of ways to promote a particular outcome, sometimes including trade-offs with other distal factors. The untoward consequences of crowding have long been of concern to scholars interested in the health and adaptive functioning of children [
43]. Crowded conditions are systematically associated with respiratory illnesses, meningitis, and gastrointestinal problems in children [
44]. Crowding encourages the spread of infection and increases the likelihood of injury and death as a consequence of lifestyle choices, like co-sleeping which may be a factor in sudden infant death syndrome [
45]. Living in crowded quarters increases the likelihood of poor overall health among children, partly as a consequence of having more direct exposure to viral and bacterial pathogens [
44].
Overcrowding often coincides with poor overall housing quality (e.g., poor ventilation, lack of household facilities, poor external construction) [
46]. Living in confined space increases stress and poor treatment by others in the household: For example, parents living in crowded conditions are less responsive to and involved with their children and engage in less effective monitoring and lower levels of individual supervision [
47]. Age spacing in the household composition could also have an impact in terms of (a) what types of pathogens a young child is likely to be exposed to, and (b) what type of care a young child is likely to receive [
48]. In effect, the overall impact of crowding could reduce the likelihood that parents engage in behaviors that reduce the probabilities of children being injured or becoming ill.
4. Implications for Intervention
The pressing question is often asked: “What effective and sustainable interventions promote and support behavior changes required to accelerate reductions in under-5 mortality?” The high-ranking distal predictors of CM identified in this study point to optimal targets to pursue to reduce CM. Thus, the findings may help governments and NGOs in their humanitarian campaigns. Our findings suggest that many under-5 child deaths are likely preventable by attending to distal their causes. Young children who die each year could be saved by discouraging “geriatric primiparity,” improving education of household heads, augmenting family wealth, improving housing (focusing on cooking fuels, toilet facilities, refrigeration, and drinking water), and reducing family size and crowding in the home. For example, an important caregiver behavior of that contributes to child survival is knowledge of the correct infant sleeping position. In Argentina and Brazil, educational interventions that encouraged caregivers to put their infants to sleep on their backs resulted in significant improvements in sleeping position and reduced sudden infant death syndrome [
49]. Of course, such interventions constitute only one part of a comprehensive strategy for enhancing child survival. They need to be complemented with interventions targeting communities and health care systems. For example, a prominent barrier to remediating CM is the belief that only high technology, clinic-based interventions can reduce mortality [
50]. Health care workers may believe that only intravenously delivered solutions combat diarrhea and that this treatment is expensive, requires skilled care, and is not readily available to poor mothers in LMIC. Although effective oral rehydration salts may be available at minimal cost, the causal factors we have identified upstream from downstream treatments may obviate diarrhea in the first place. In short, our findings have two noteworthy policy implications. First, initiatives to increase public awareness about the roles of age and education as well as specifics of the household environment and composition offer promise to reduce CM. Second, the current study might promote interest in a “big data” approach to other topics in the social and behavioral sciences as well as public health.
5. Conclusions
In this study we used a machine learning framework derived from bio-informatics to delineate and rank distal causes of under-5 CM in LMIC. To our knowledge, this is the first time that a ML framework has been applied to the MICS dataset or to identifying and prioritizing causes of under-5 CM.
By 2017, 118 of 195 countries had an under-5 mortality rate below the UN Sustainable Development Goal target of fewer than 25 deaths per 1000 live births. Progress will need to accelerate in the remaining 77 countries (many in sub-Saharan Africa and Southern Asia) to achieve the target by 2030 [
51]. In addition, in countries that have already achieved the target, efforts should be intensified to reduce within-country inequity in mortality. When the knowledge and technology for life-saving interventions are available, it is unacceptable that 15,000 children die every day from preventable causes. Our study identifies and priorities up-stream distal causes—and presumptive targets of intervention—likely to reduce down-stream proximal causes of under-5 CM.
Mortality rates among children are key indicators of child well-being and more broadly of future sustainable social and economic development. CM is part of the larger canon of health disparities that pervade communities and nations with poor resources and that are at the forefront of efforts by international organizations, such as the United Nations and the World Health Organization, to improve human life [
3]. Identifying factors that influence CM is requisite to evidence-based policymaking to improve the survival chances of the world’s children.
Although knowledge about proximal causes of CM has advanced considerably over the last half-century, less research has been done to understand the distal causes of those proximal causes, especially in LMIC. Our understanding of child survival, derived from research conducted in high-income countries, may not readily apply to LMIC. The poverty and limited resources that characterize environments in LMIC present difficult circumstances for research, policies, and programs that promote child well-being. Many families living in LMIC experience physical and social conditions that increase the likelihood children will not live to see their 5th birthday. The present study identifies and orders distal causes of under-5 CM in a large number of LMIC. The results point to concrete protective factors that can be addressed so that more children will survive. Innovative analytic methods, such as those used in this study, will help to move that process forward.
Author Contributions
Conceptualization, A.B., G.G., M.H.B. and G.E.; Data curation, G.G., M.H.B. and J.E.L.; Investigation, M.H.B., K.D.-D., J.E.L., R.H.B., M.C. and G.E.; Methodology, A.B. and G.G.; Resources, G.G.; Software, A.B.; Supervision, M.H.B. and G.E.; Writing—original draft, A.B. and G.E.; Writing—review & editing, A.B., G.G., M.H.B., K.D.-D., J.E.L., R.H.B., M.C. and G.E. All authors have read and agreed to the published version of the manuscript.
Funding
A.B. was supported by a Post-doctoral Fellowship within MIUR programme framework “Dipartimenti di Eccellenza” (DiPSCO, University of Trento). G.E. was supported by NAP SUG 2015, Singapore Ministry of Education ACR Tier 1 (RG149/16 and RT10/19). M.H.B. was supported by the Intramural Research Program of the NIH/NICHD, USA, and an International Research Fellowship at the Institute for Fiscal Studies (IFS), London, UK, funded by the European Research Council (ERC) under the Horizon 2020 research and innovation programme (grant agreement No 695300-HKADeC-ERC-2015-AdG). Computational resources were provided by the National Super Computing Center of Singapore (Project ID: 12001609; Computational study of Child Development in Low Resource Contexts.
Institutional Review Board Statement
The study was approved by the Internal Review Board of the Nanyang Technological University: IRB-2020-04-040.
Informed Consent Statement
Ethics approvals and informed consents were handled in each site in which data were collected.
Data Availability Statement
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- United Nations Inter-Agency Group for Child Mortality Estimation. Levels & Trends in Child Mortality. 2019. Available online: https://www.unicef.org/reports/levels-and-trends-child-mortality-report-2019 (accessed on 25 March 2020).
- World Bank Group. Mortality Rate, under-5 (per 1000 Live Births). 2020. Available online: https://databank.worldbank.org/reports.aspx?source=2&series=SH.DYN.MORT&country= (accessed on 25 March 2020).
- United Nations Development Programme. Human Development Report 2019. 2019. Available online: http://hdr.undp.org/sites/default/files/hdr2019.pdf (accessed on 25 March 2020).
- World Health Organization. The Global Strategy for Women’s, Children’s and Adolescents’ Health, 2016–2030. 2016. Available online: https://www.who.int/life-course/partners/global-strategy/global-strategy-2016-2030/en/ (accessed on 25 March 2020).
- United Nations. Sustainable Development Goal 3. 2016. Available online: https://sustainabledevelopment.un.org/sdg3 (accessed on 25 March 2020).
- World Health Organization. Children: Reducing Mortality. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality (accessed on 25 March 2020).
- Cabral, J.P. Water microbiology. Bacterial pathogens and water. Int. J. Environ. Res. Public Health 2010, 7, 3657–3703. [Google Scholar] [CrossRef] [PubMed]
- Hüllermeier, E. Fuzzy methods in machine learning and data mining: Status and prospects. Fuzzy Sets Syst. 2005, 156, 387–406. [Google Scholar] [CrossRef]
- Ishibuchi, H.; Nojima, Y. Analysis of interpretability-accuracy tradeoff of fuzzy systems by multiobjective fuzzy genetics-based machine learning. Int. J. Approx. Reason. 2007, 44, 4–31. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Huber, P.J. Robust Statistics; John Wiley & Sons: Hoboken, NJ, USA, 2004; Volume 523. [Google Scholar]
- Bornstein, M.H.; Putnick, D.L.; Suwalsky, J.T.; Gini, M. Maternal chronological age, prenatal and perinatal history, social support, and parenting of infants. Child Dev. 2006, 77, 875–892. [Google Scholar] [CrossRef] [Green Version]
- Waldron, I.; Weiss, C.C.; Hughes, M.E. Interacting effects of multiple roles on women’s health. J. Health Soc. Behav. 1998, 39, 216–236. [Google Scholar] [CrossRef]
- Restrepo-Méndez, M.C.; Victora, C.G. Maternal mortality by age: Who is most at risk? Lancet Glob. Health 2014, 2, e120–e121. [Google Scholar] [CrossRef] [Green Version]
- Berkowitz, G.S.; Skovron, M.L.; Lapinski, R.H.; Berkowitz, R.L. Delayed childbearing and the outcome of pregnancy. N. Engl. J. Med. 1990, 322, 659–664. [Google Scholar] [CrossRef]
- Stein, Z.; Susser, M. The risks of having children in later life. West. J. Med. 2000, 173, 295. [Google Scholar] [CrossRef] [Green Version]
- Russell, R.B.; Petrini, J.R.; Damus, K.; Mattison, D.R.; Schwarz, R.H. The changing epidemiology of multiple births in the United States. Obstet. Gynecol. 2003, 101, 129–135. [Google Scholar]
- Salihu, H.M.; Shumpert, M.N.; Slay, M.; Kirby, R.S.; Alexander, G.R. Childbearing beyond maternal age 50 and fetal outcomes in the United States. Obstet. Gynecol. 2003, 102, 1006–1014. [Google Scholar] [PubMed]
- United Nations Inter-Agency Group for Child Mortality Estimation. Levels & Trends in Child Mortality. 2017. Available online: https://childmortality.org/wp-content/uploads/2018/10/UN-IGME-Child-Mortality-Report-2018.pdf (accessed on 25 March 2020).
- Affleck, W.; Pelto, G. Caregivers’ responses to an intervention to improve young child feeding behaviors in rural Bangladesh: A mixed method study of the facilitators and barriers to change. Soc. Sci. Med. 2012, 75, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.H.; Cote, L.R.; Haynes, O.M.; Hahn, C.S.; Park, Y. Parenting knowledge: Experiential and sociodemographic factors in European American mothers of young children. Dev. Psychol. 2010, 46, 1677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaise, N.Y.H.; Dovie, D.B. Diarrheal diseases in the history of public health. Arch. Med Res. 2007, 38, 159–163. [Google Scholar] [CrossRef]
- Yongsi, H.N.; Ntetu, A.L. Household standard of living and children’s health in Cameroon. J. Dev. Areas 2008, 42, 251–259. [Google Scholar] [CrossRef]
- Bornstein, M.H.; Bradley, R.H. Socioeconomic Status, Parenting, and Child Development; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2003. [Google Scholar]
- Hajizadeh, S.; Ramezani Tehrani, F.; Simbar, M.; Farzadfar, F. Factors influencing the use of prenatal care: A systematic review. J. Midwifery Reprod. Health 2016, 4, 544–557. [Google Scholar]
- Overpeck, M.D.; Brenner, R.A.; Trumble, A.C.; Trifiletti, L.B.; Berendes, H.W. Risk factors for infant homicide in the United States. N. Engl. J. Med. 1998, 339, 1211–1216. [Google Scholar] [CrossRef]
- Gauderman, W.J.; Avol, E.; Gilliland, F.; Vora, H.; Thomas, D.; Berhane, K.; McConnell, R.; Kuenzli, N.; Lurmann, F.; Rappaport, E.; et al. The effect of air pollution on lung development from 10 to 18 years of age. N. Engl. J. Med. 2004, 351, 1057–1067. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Effects of Air Pollution on Children’s Health and Development: A Review of the Evidence. 2005. Available online: https://apps.who.int/iris/handle/10665/107652 (accessed on 25 March 2020).
- Chao, F.; You, D.; Pedersen, J.; Hug, L.; Alkema, L. National and regional under-5 mortality rate by economic status for low-income and middle-income countries: A systematic assessment. Lancet Glob. Health 2018, 6, e535–e547. [Google Scholar] [CrossRef]
- Yang, C.Y.; Chiu, J.F.; Chiu, H.F.; Kao, W.Y. Damp housing conditions and respiratory symptoms in primary school children. Pediatr. Pulmonol. 1997, 24, 73–77. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines for Indoor Air Quality: Household Fuel Combustion. 2014. Available online: https://www.who.int/airpollution/guidelines/household-fuel-combustion/IAQ_HHFC_guidelines.pdf (accessed on 25 March 2020).
- Baltazar, J.C.; Solon, F.S. Disposal of faeces of children under two years old and diarrhoea incidence: A case-control study. Int. J. Epidemiol. 1989, 18, S16–S19. [Google Scholar] [CrossRef] [PubMed]
- WHO/UNICEF Joint Monitoring Programme for Water Supply and Sanitation. Progress on Drinking Water and Sanitation: Special Focus on Sanitation; World Health Organization: Geneve, Switzerland, 2008. [Google Scholar]
- Bartlett, S. Water, sanitation and urban children: The need to go beyond “improved” provision. Environ. Urban. 2003, 15, 57–70. [Google Scholar]
- Podewils, L.J.; Mintz, E.D.; Nataro, J.P.; Parashar, U.D. Acute, infectious diarrhea among children in developing countries. Semin. Pediatr. Infect. Dis. 2004, 15, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, S. Children’s experience of the physical environment in poor urban settlements and the implications for policy, planning and practice. Environ. Urban. 1999, 11, 63–74. [Google Scholar] [CrossRef]
- Ehiri, J.E.; Azubuike, M.C.; Ubbaonu, C.N.; Anyanwu, E.C.; Ibe, K.M.; Ogbonna, M.O. Critical control points of complementary food preparation and handling in eastern Nigeria. Bull. World Health Organ. 2001, 79, 423–433. [Google Scholar]
- Motarjemi, Y.; Käferstein, F.; Moy, G.; Quevedo, F. Contaminated weaning food: A major risk factor for diarrhoea and associated malnutrition. Bull. World Health Organ. 1993, 71, 79. [Google Scholar] [PubMed]
- Lechtig, A.; Doyle, B. The impact of water and sanitation on malnutrition and underfive mortality rates. WATERfront 1996, 8, 5–19. [Google Scholar]
- Rice, A.L.; Sacco, L.; Hyder, A.; Black, R.E. Malnutrition as an underlying cause of childhood deaths associated with infectious diseases in developing countries. Bull. World Health Organ. 2000, 78, 1207–1221. [Google Scholar]
- Nandy, S.; Gordon, D. Children living in squalor: Shelter, water and sanitation deprivations in developing countries. Child. Youth Environ. 2009, 19, 202–228. [Google Scholar]
- Lindskog, P.; Lundqvist, J. Why Poor Children Stay Sick: The Human Ecology of Child Health and Welfare in Rural Malawi; Nordiska Afrikainstitutet: Uppsala, Sweden, 1989. [Google Scholar]
- Evans, G.W. Child development and the physical environment. Annu. Rev. Psychol. 2006, 57, 423–451. [Google Scholar] [CrossRef] [Green Version]
- Galpin, O.; Whitaker, C.; Dubiel, A. Helicobacter pylori infection and overcrowding in childhood. Lancet 1992, 339, 619. [Google Scholar] [CrossRef]
- Jaine, R.; Baker, M.; Venugopal, K. Acute rheumatic fever associated with household crowding in a developed country. Pediatr. Infect. Dis. J. 2011, 30, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Vandivere, S.; Hair, E.C.; Theokas, C.; Cleveland, K.; McNamara, M.; Atienza, A.; Vandivere, S. How Housing Affects Child Well-Being; Funders’ Network for Smart Growth and Livable Communities: Coral Gables, FL, USA, 2006. [Google Scholar]
- Bradley, R.H.; Caldwell, B.M. The relation of infants’ home environments to achievement test performance in first grade: A follow-up study. Child Dev. 1984, 55, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Conde-Agudelo, A.; Rosas-Bermudez, A.; Castaño, F.; Norton, M.H. Effects of birth spacing on maternal, perinatal, infant, and child health: A systematic review of causal mechanisms. Stud. Fam. Plan. 2012, 43, 93–114. [Google Scholar] [CrossRef] [PubMed]
- Issler, R.M.S.; Marostica, P.J.C.; Giugliani, E.R.J. Infant sleep position: A randomized clinical trial of an educational intervention in the maternity ward in Porto Alegre, Brazil. Birth 2009, 36, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [Green Version]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed on 25 March 2020).
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).


 ,
, 



{kind=link}
{kind=link}
{kind=link}