
Test–Retest Reliability of a Conventional Gait Model for Registering Joint Angles during Initial Contact and Toe-Off in Healthy Subjects

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Analysis of Data
2.4. Sample Size Calculation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CGM | conventional gait model |
| LAMBECOM | Laboratory of Analysis of Movement, Biomechanics, Ergonomics, and Motor Control |
| IC | initial contact |
| TO | toe-off |
| ICC | intraclass correlation coefficient |
| CI | confidence interval |
| SD | standard deviation |
| SEM | standard error of measurement |
| MDC | minimal detectable change |
| LOA | limits of agreement |
References
- Castelli, A.; Paolini, G.; Cereatti, A.; Della Croce, U. A 2D Markerless Gait Analysis Methodology: Validation on Healthy Subjects. Comput. Math. Methods Med. 2015, 2015, 186780. [Google Scholar] [CrossRef] [Green Version]
- Andreopoulou, G.; Mahad, D.J.; Mercer, T.H.; Van Der Linden, M.L. Test-retest reliability and minimal detectable change of ankle kinematics and spatiotemporal parameters in MS population. Gait Posture 2019, 74, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Whittle, M.W. Clinical gait analysis: A review. Hum. Mov. Sci. 1996, 15, 369–387. [Google Scholar] [CrossRef]
- Mentiplay, B.F.; Clark, R.A. Modified conventional gait model versus cluster tracking: Test-retest reliability, agreement and impact of inverse kinematics with joint constraints on kinematic and kinetic data. Gait Posture 2018, 64, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Ancillao, A. Stereophotogrammetry in Functional Evaluation: History and Modern Protocols. In Modern Functional Evaluation Methods for Muscle Strength and Gait Analysis; Springer Briefs in Applied Sciences and Technology; Springer: Cham, Switzerland; Berlin/Heidelberg, Germany, 2018; pp. 1–19. [Google Scholar]
- Baker, R. Gait analysis methods in rehabilitation. J. Neuroeng. Rehabil. 2006, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.B.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef]
- Baker, R.; Leboeuf, F.; Reay, J.; Sangeux, M. The Conventional Gait Model-Success and Limitations. In Handbook of Human Motion; Müller, B., Wolf, S., Eds.; Springer: Cham, Switzerland; Berlin/Heidelberg, Germany, 2018; pp. 489–508. [Google Scholar]
- Wedege, P.; Steffen, K.; Strøm, V.; Opheim, A.I. Reliability of three-dimensional kinematic gait data in adults with spinal cord injury. J. Rehabil. Assist. Technol. Eng. 2017, 4, 2055668317729992. [Google Scholar] [CrossRef] [Green Version]
- Collins, T.D.; Ghoussayni, S.N.; Ewins, D.J.; Kent, J.A. A six degrees-of-freedom marker set for gait analysis: Repeatability and comparison with a modified Helen Hayes set. Gait Posture 2009, 30, 173–180. [Google Scholar] [CrossRef]
- Manca, M.; Leardini, A.; Cavazza, S.; Ferraresi, G.; Marchi, P.; Zanaga, E.; Benedetti, M.G. Repeatability of a new protocol for gait analysis in adult subjects. Gait Posture 2010, 32, 282–284. [Google Scholar] [CrossRef]
- Wolf, A.; Senesh, M. Estimating joint kinematics from skin motion observation: Modelling and validation. Comput. Methods Biomech. Biomed. Eng. 2011, 14, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, R.; Armada-da-Silva, P.; Pool-Goudzwaard, A.L.; Moniz-Pereira, V.; Veloso, A.P. Three dimensional multi-segmental trunk kinematics and kinetics during gait: Test-retest reliability and minimal detectable change. Gait Posture 2016, 46, 18–25. [Google Scholar] [CrossRef] [PubMed]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Fortes, C.E.; Carmo, A.A.D.; Rosa, K.Y.A.; Lara, J.P.R.; Mendes, F.A.D.S. Immediate changes in post-stroke gait using a shoe lift on the nonaffected lower limb: A preliminary study. Physiother. Theory Pract. 2020, 1, 1–6. [Google Scholar] [CrossRef]
- Kim, S.J.; Yoo, G.E.; Shin, Y.; Cho, S.R. Gait training for adults with cerebral palsy following harmonic modification in rhythmic auditory stimulation. Ann. N. Y. Acad. Sci. 2020, 1473, 11–19. [Google Scholar] [CrossRef]
- Swank, C.; Almutairi, S.; Wang-Price, S.; Gao, F. Immediate kinematic and muscle activity changes after a single robotic exoskeleton walking session post-stroke. Top. Stroke Rehabil. 2020, 27, 503–515. [Google Scholar] [CrossRef]
- Gor-García-Fogeda, M.D.; De La Cuerda, R.C.; Tejada, M.C.; Alguacil-Diego, I.M.; Molina-Rueda, F. Observational Gait Assessments in People With Neurological Disorders: A Systematic Review. Arch. Phys. Med. Rehabil. 2016, 97, 131–140. [Google Scholar] [CrossRef]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Monaghan, K.; Delahunt, E.; Caulfield, B. Increasing the number of gait trial recordings maximises intra-rater reliability of the CODA motion analysis system. Gait Posture 2007, 25, 303–315. [Google Scholar] [CrossRef]
- Schwartz, M.H.; Trost, J.P.; Wervey, R.A. Measurement and management of errors in quantitative gait data. Gait Posture 2004, 20, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Laroche, D.; Duval, A.; Morisset, C.; Beis, J.-N.; D’Athis, P.; Maillefert, J.F.; Ornetti, P. Test–retest reliability of 3D kinematic gait variables in hip osteoarthritis patients. Osteoarthr. Cartil. 2011, 19, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Fernández-González, P.; Koutsou, A.; Cuesta-Gómez, A.; Carratalá-Tejada, M.; Miangolarra-Page, J.C.; Molina-Rueda, F. Reliability of Kinovea® Software and Agreement with a Three-Dimensional Motion System for Gait Analysis in Healthy Subjects. Sensors 2020, 20, 3154. [Google Scholar] [CrossRef] [PubMed]
- Vicon Documentation. Available online: https://docs.vicon.com/display/Nexus25/Plug-in+Gait+kinematic+variables (accessed on 20 March 2020).
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Bartlett, J.W.; Frost, C. Reliability, repeatability and reproducibility: Analysis of measurement errors in continuous variables. Ultrasound Obstet. Gynecol. 2008, 31, 466–475. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Yeo, S.S.; Park, G.Y. Accuracy Verification of Spatio-Temporal and Kinematic Parameters for Gait Using Inertial Measurement Unit System. Sensors 2020, 20, 1343. [Google Scholar] [CrossRef] [Green Version]
- Meldrum, D.; Shouldice, C.; Conroy, R.M.; Jones, K.; Forward, M. Test-retest reliability of three-dimensional gait analysis: Including a novel approach to visualising agreement of gait cycle waveforms with Bland and Altman plots. Gait Posture 2014, 39, 265–271. [Google Scholar] [CrossRef]
- Wilken, J.M.; Rodriguez, K.M.; Brawner, M.; Darter, B.J. Reliability and Minimal Detectible Change values for gait kinematics and kinetics in healthy adults. Gait Posture 2012, 35, 301–307. [Google Scholar] [CrossRef]
- de Vet, H.C.; Terwee, C.B.; Ostelo, R.W.; Beckerman, H.; Knol, D.L.; Bouter, L.M. Minimal changes in health status questionnaires: Distinction between minimally detectable change and minimally important change. Health Qual. Life Outcomes 2006, 4, 54. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Baker, R.; Esquenazi, A.; Benedetti, M.G.; Desloovere, K. Gait analysis: Clinical facts. Eur. J. Phys. Rehabil. Med. 2016, 52, 560–574. [Google Scholar] [PubMed]
- Horsak, B.; Schwab, C.; Leboeuf, F.; Kranzl, A. Reliability of walking and stair climbing kinematics in a young obese population using a standard kinematic and the CGM2 model. Gait Posture 2021, 83, 96–99. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
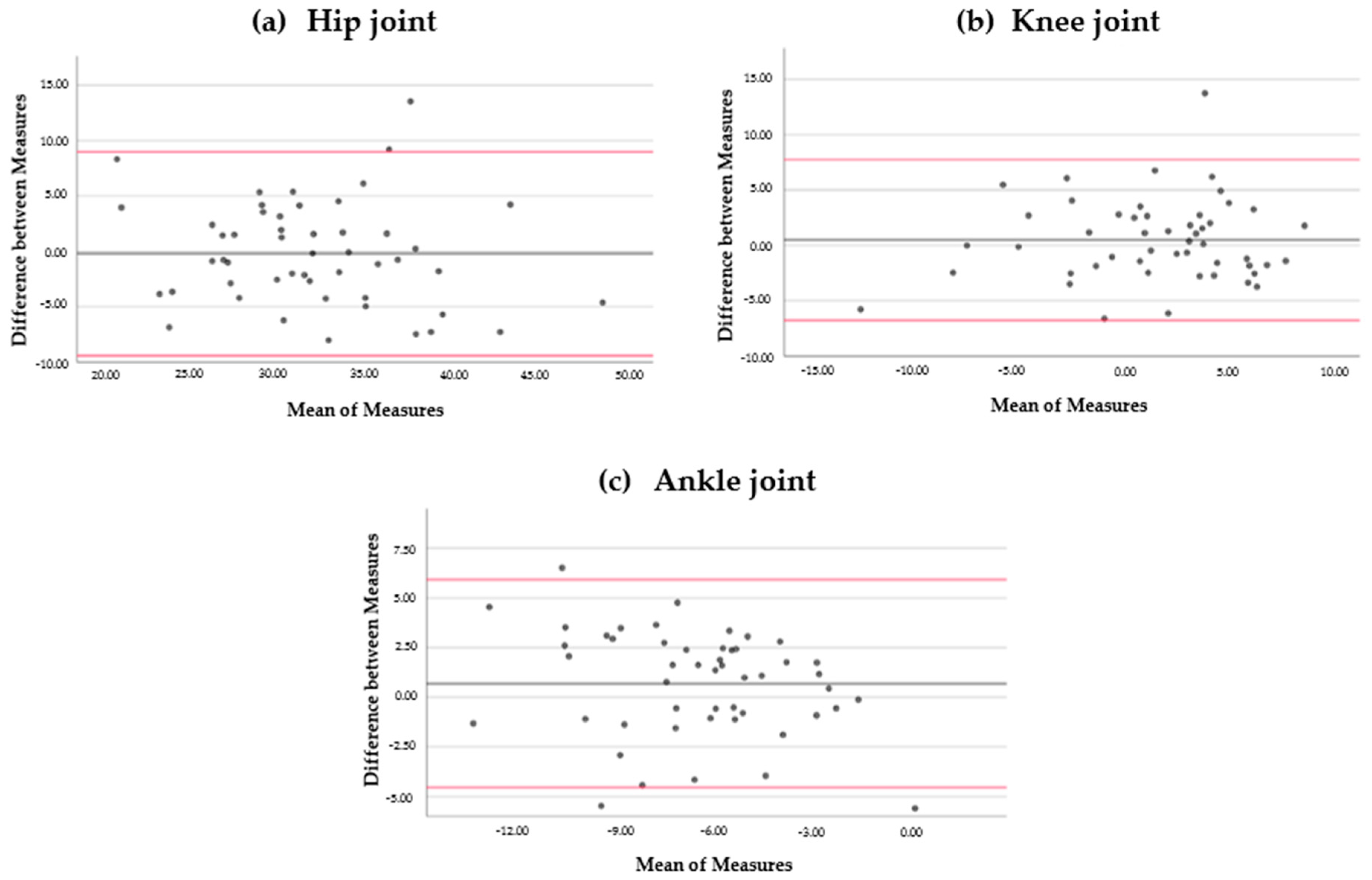
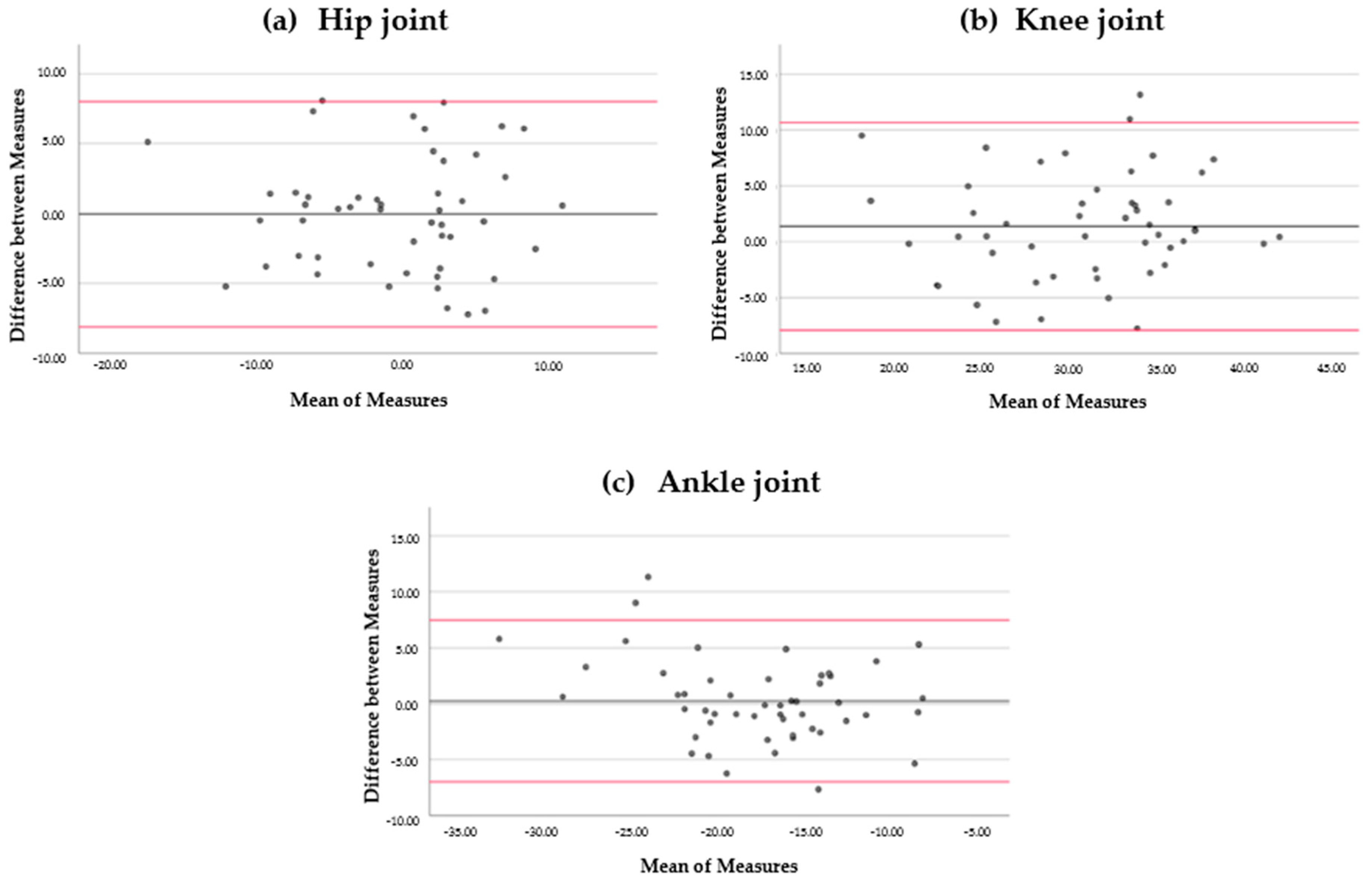
| Parameter | ICC | (95% CI) | Mean | D | SD (DIFF) | 95% LOA | SEM | MDC |
|---|---|---|---|---|---|---|---|---|
| Hip angle at IC (°) | 0.837 | 0.712–0.907 | 32.03 | 0.2 | 4.69 | −9.39 → 8.99 | 1.98 | 5.24 |
| Knee angle at IC (°) | 0.825 | 0.693–0.901 | 1.49 | 0.47 | 3.70 | −6.78 → 7.74 | 1.55 | 4.29 |
| Ankle angle at IC (°) | 0.774 | 0.602–0.871 | −6.58 | 0.69 | 2.67 | −4.54 → 5.93 | 1.27 | 3.52 |
| Hip angle at TO (°) | 0.880 | 0.788–0.932 | −0.66 | 0.05 | 4.10 | −8.11 → 7.99 | 1.03 | 2.85 |
| Knee angle at TO (°) | 0.814 | 0.671–0.895 | 30.75 | 1.37 | 4.75 | −7.94 → 10.68 | 0.96 | 3.30 |
| Ankle angle at TO (°) | 0.880 | 0.788–0.9321 | −17.80 | 0.24 | 3.68 | −6.98 → 7.46 | 1.077 | 2.56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molina-Rueda, F.; Fernández-González, P.; Cuesta-Gómez, A.; Koutsou, A.; Carratalá-Tejada, M.; Miangolarra-Page, J.C. Test–Retest Reliability of a Conventional Gait Model for Registering Joint Angles during Initial Contact and Toe-Off in Healthy Subjects. Int. J. Environ. Res. Public Health 2021, 18, 1343. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031343
Molina-Rueda F, Fernández-González P, Cuesta-Gómez A, Koutsou A, Carratalá-Tejada M, Miangolarra-Page JC. Test–Retest Reliability of a Conventional Gait Model for Registering Joint Angles during Initial Contact and Toe-Off in Healthy Subjects. International Journal of Environmental Research and Public Health. 2021; 18(3):1343. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031343
Chicago/Turabian StyleMolina-Rueda, Francisco, Pilar Fernández-González, Alicia Cuesta-Gómez, Aikaterini Koutsou, María Carratalá-Tejada, and Juan Carlos Miangolarra-Page. 2021. "Test–Retest Reliability of a Conventional Gait Model for Registering Joint Angles during Initial Contact and Toe-Off in Healthy Subjects" International Journal of Environmental Research and Public Health 18, no. 3: 1343. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031343