
The Relationship of Race, Psychosocial Stress and Resiliency Indicators to Neurocognitive Impairment among Older Americans Enrolled in the Health and Retirement Survey: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Primary Determinants: Race/Ethnicity, Toxic Stress, and Resilience Promoting Factors
2.1.2. Other Measures
2.1.3. Outcome
2.2. Data Analysis
3. Results
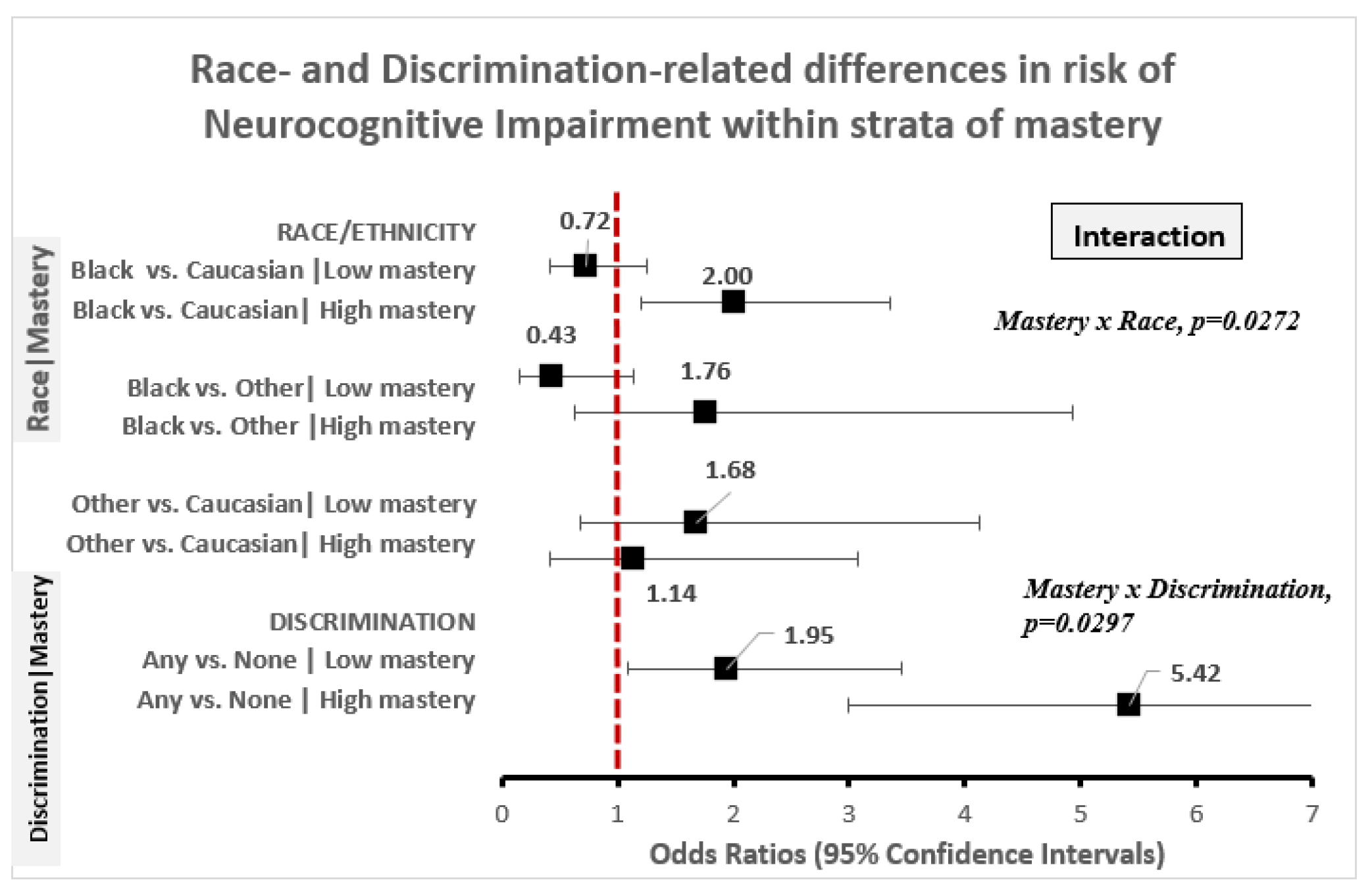
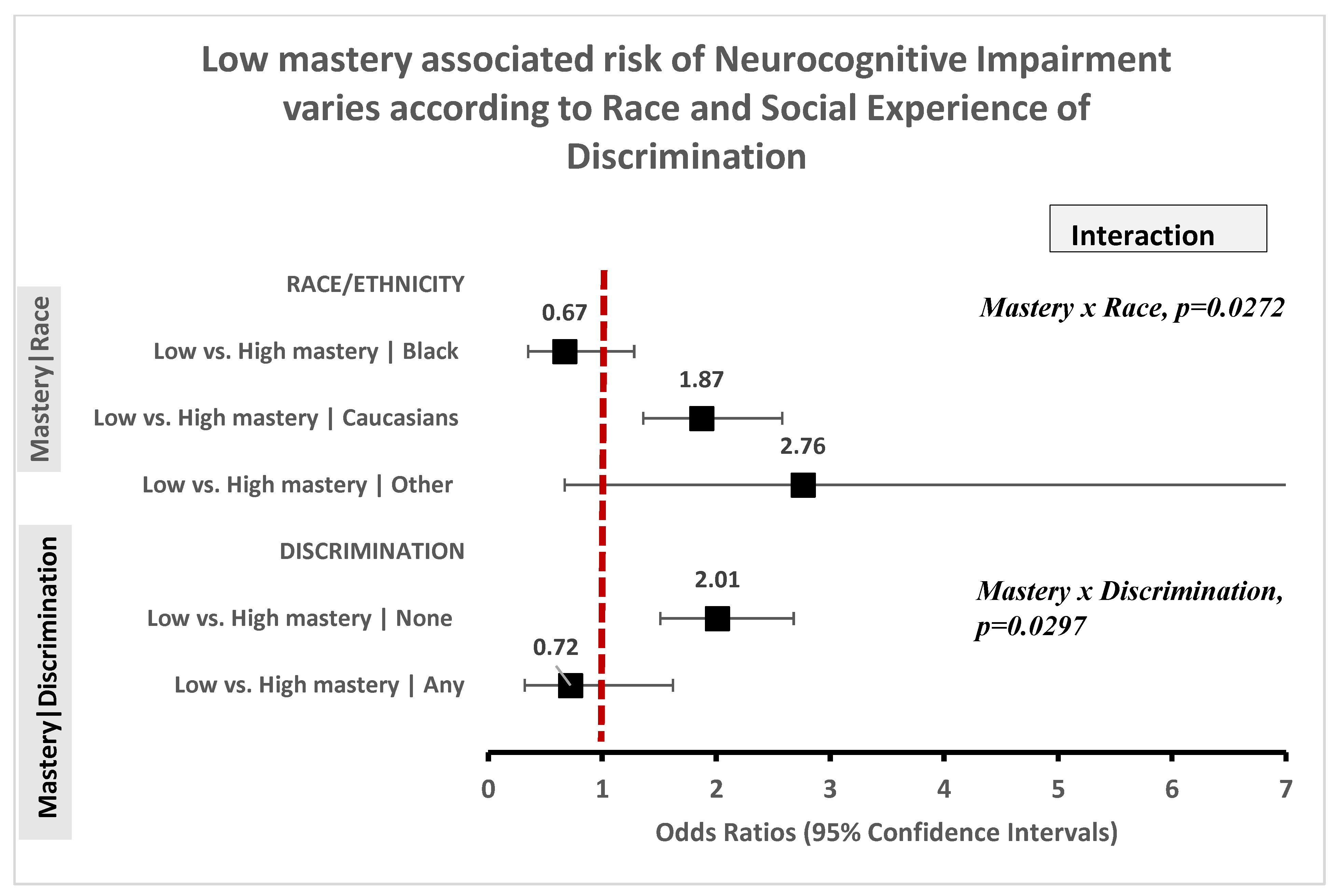
3.1. Race Is Not Associated with Cognitive Impairment, But Disparities Persist According to Level of Mastery
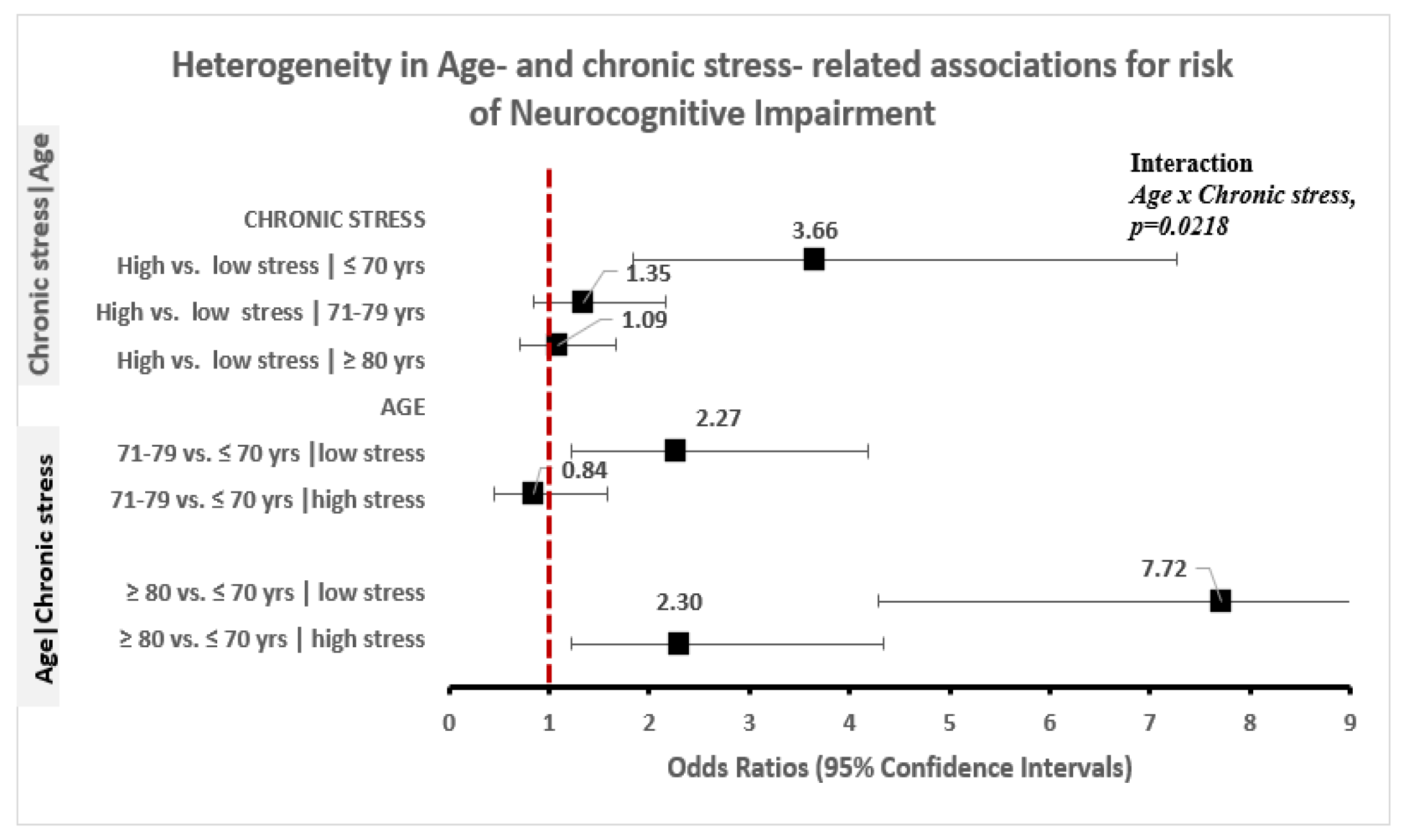
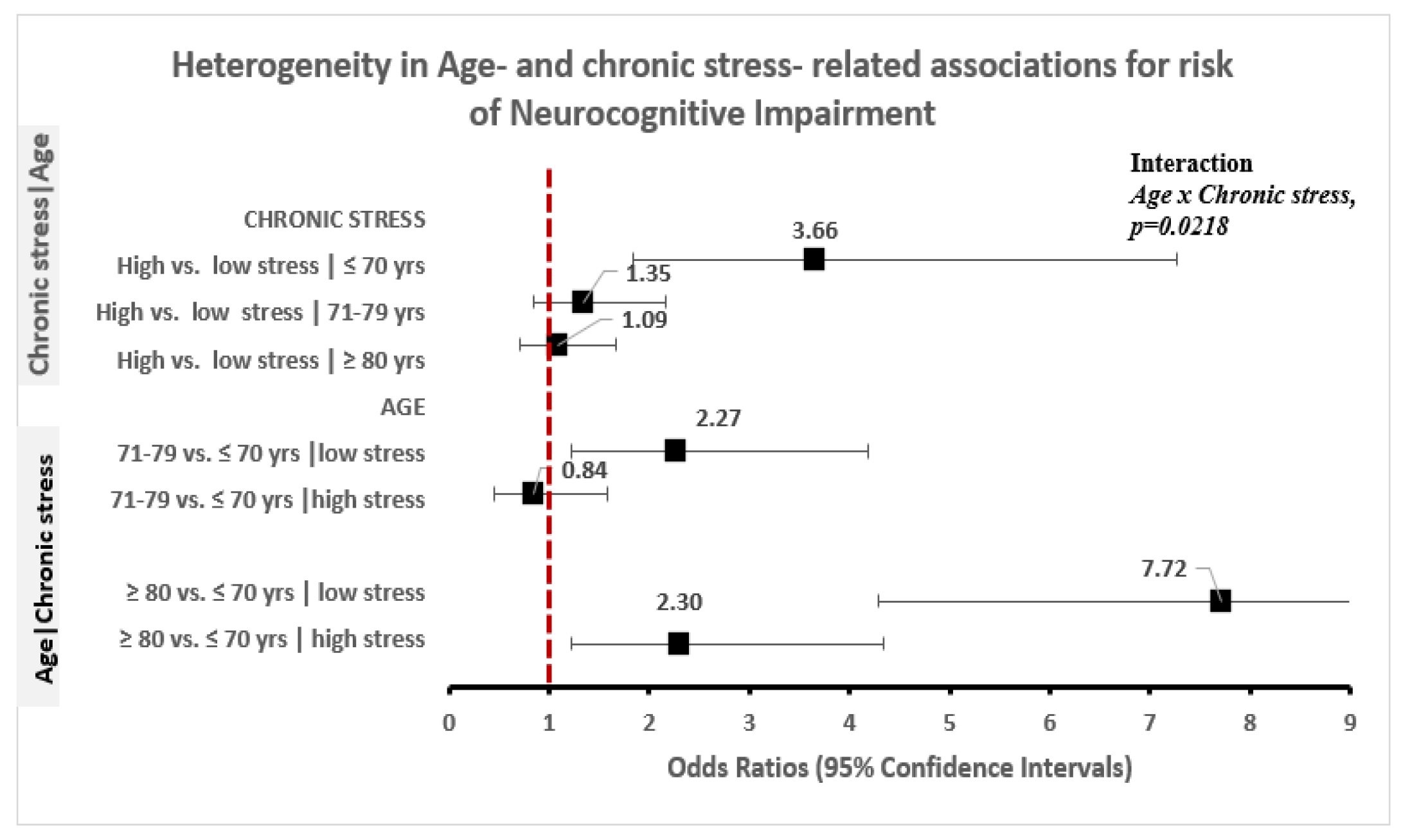
3.2. High Toxic Stress Is Associated with Higher NI; Relationship Varies by Mastery Level and Age
3.3. Low RPF Is Associated with NI, But Relationship Varies by Race and the Experience of Discrimination
3.4. Increasing Age Is Associated with Higher Risk of NI; Relationship Varies by Level of Stress
3.5. Other Factors Associated with Increased Risk of NI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- U.S. Census Bureau PD. Annual Estimates of the Resident Population by Sex, Race and Hispanic Origin for the United States, States and Counties: 1 April 2010 to 1 July 2014; U.S. Census Bureau, Population Division: Washington, DC, USA, 2015.
- The Henry J. Kaiser Family Foundation. Key Facts Race, Ethnicity & Medical Care, 2007. Available online: www.kff.org (accessed on 19 May 2020).
- Jones, C.P. Levels of racism: A theoretic framework and a gardener’s tale. Am. J. Public Health 2000, 90, 1212–1215. [Google Scholar]
- Gee, G.; Walsemann, K. Does health predict the reporting of racial discrimination or do reports of discrimination predict health? Findings from the National Longitudinal Study of Youth. Soc. Sci. Med. 2009, 68, 1676–1684. [Google Scholar] [CrossRef]
- Williams, D.R.; Yan, Y.; Jackson, J.S.; Anderson, N.B. Racial Differences in Physical and Mental Health: Socio-economic Status, Stress and Discrimination. J. Health Psychol. 1997, 2, 335–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, D.H.; Nuru-Jeter, A.M.; Lincoln, K.D.; Francis, D.D. Conceptualizing Racial Disparities in Health: Advancement of a Socio-Psychobiological Approach. Du Bois Rev. Soc. Sci. Res. Race 2011, 8, 63–77. [Google Scholar] [CrossRef]
- Edwards, F.; Lee, H.; Esposito, M. Risk of being killed by police use of force in the United States by age, race–ethnicity, and sex. Proc. Natl. Acad. Sci. USA 2019, 116, 16793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, F.; Esposito, M.H.; Lee, H. Risk of Police-Involved Death by Race/Ethnicity and Place, United States, 2012–2018. Am. J. Public Health 2018, 108, 1241–1248. [Google Scholar] [CrossRef]
- DeGue, S.; Fowler, K.A.; Calkins, C. Deaths Due to Use of Lethal Force by Law Enforcement: Findings from the National Violent Death Reporting System, 17 U.S. States, 2009–2012. Am. J. Prev. Med. 2016, 51 (Suppl. 3), S173–S187. [Google Scholar] [CrossRef] [Green Version]
- Jones, C.P. Toward the Science and Practice of Anti-Racism: Launching a National Campaign Against Racism. Ethn. Dis. 2018, 28 (Suppl. 1), 231–234. [Google Scholar] [CrossRef]
- Wordes, M.; Bynum, T.S.; Corley, C.J. Locking Up Youth: The Impact of Race on Detention Decisions. J. Res. Crime Delinq. 1994, 31, 149–165. [Google Scholar] [CrossRef]
- Leiber, M.J.; Fox, K.C. Race and the Impact of Detention on Juvenile Justice Decision Making. Crime Delinq. 2005, 51, 470–497. [Google Scholar] [CrossRef]
- Leiber, M.J.; Johnson, J.D. Being Young and Black: What Are Their Effects on Juvenile Justice Decision Making? Crime Delinq. 2007, 54, 560–581. [Google Scholar] [CrossRef]
- Chae, D.H.; Walters, K.L. Racial discrimination and racial identity attitudes in relation to self-rated health and physical pain and impairment among two-spirit American Indians/Alaska Natives. Am. J. Public Health 2009, 99 (Suppl. 1), S144–S151. [Google Scholar] [CrossRef] [PubMed]
- Koball, H.L.; Besculides, M.; Goesling, B.; Lincoln, K.D.; Chae, D.H. Stress, Marital Satisfaction, and Psychological Distress Among African Americans. J. Fam. Issues 2010, 31, 1081–1105. [Google Scholar]
- Sue, D.W.; Bucceri, J.; Lin, A.I.; Nadal, K.L.; Torino, G.C. Racial microaggressions and the Asian American experience. Cult. Divers. Ethn. Minority Psychol. 2007, 13, 72–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, D.H.; Yoshikawa, H. Perceived group devaluation, depression, and HIV-risk behavior among Asian gay men. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2008, 27, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Noh, S.; Kaspar, V. Perceived discrimination and depression: Moderating effects of coping, acculturation, and ethnic support. Am. J. Public Health 2003, 93, 232–238. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Westphal, M.; Mancini, A.D. Resilience to loss and potential trauma. Annu. Rev. Clin. Psychol. 2011, 7, 511–535. [Google Scholar] [CrossRef] [Green Version]
- Ungar, M. The social ecology of resilience: Addressing contextual and cultural ambiguity of a nascent construct. Am. J. Orthopsychiatry 2011, 81, 1–17. [Google Scholar] [CrossRef]
- Fontes, A.P.; Neri, A.L. Resilience in aging: Literature review. Ciência Saúde Coletiva 2015, 20, 1475–1495. [Google Scholar]
- McIntyre, R.S.; Xiao, H.X.; Syeda, K.; Vinberg, M.; Carvalho, A.F.; Mansur, R.B.; Maruschak, N.; Cha, D.S. The Prevalence, Measurement, and Treatment of the Cognitive Dimension/Domain in Major Depressive Disorder. CNS Drugs 2015, 29, 577–589. [Google Scholar] [CrossRef]
- Zhang, Z.; Mark, D.H.; Yu, Y.-L. Life Course Pathways to Racial Disparities in Cognitive Impairment among Older Americans. J. Health Soc. Behav. 2016, 57, 184–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, A.L.; Mungas, D.M.; Crane, P.K.; Gibbons, L.E.; MacKay-Brandt, A.; Manly, J.J.; Mukherjee, S.; Romero, H.; Sachs, B.; Thomas, M.; et al. Effects of education and race on cognitive decline: An integrative study of generalizability versus study-specific results. Psychol. Aging 2015, 30, 863–880. [Google Scholar] [CrossRef] [PubMed]
- Miles, T.P.; Froehlich, T.E.; Bogardus, S.T.; Inouye, S.K. Dementia and race: Are there differences between African Americans and Caucasians? J. Am. Geriatr. Soc. 2001, 49, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Maercker, A.; Hilpert, P.; Burri, A. Childhood trauma and resilience in old age: Applying a context model of resilience to a sample of former indentured child laborers. Aging Ment. Health 2016, 20, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Amir, M.; Lev-Wiesel, R. Time does not heal all wounds: Quality of life and psychological distress of people who survived the holocaust as children 55 years later. J. Trauma. Stress 2003, 16, 295–299. [Google Scholar] [CrossRef]
- Landau, R.; Litwin, H. The effects of extreme early stress in very old age. J. Trauma. Stress 2000, 13, 473–487. [Google Scholar] [CrossRef]
- Beutel, M.E.; Glaesmer, H.; Wiltink, J.; Marian, H.; Brähler, E. Life satisfaction, anxiety, depression and resilience across the life span of men. Aging Male Off. J. Int. Soc. Study Aging Male 2010, 13, 32–39. [Google Scholar] [CrossRef]
- Pietrzak, R.H.; Cook, J.M. Psychological resilience in older U.S. veterans: Results from the national health and resilience in veterans study. Depress. Anxiety 2013, 30, 432–443. [Google Scholar] [CrossRef]
- Willis, K.J.; Hakim, A.M. Stroke prevention and cognitive reserve: Emerging approaches to modifying risk and delaying onset of dementia. Front. Neurol. 2013, 4, 13. [Google Scholar] [CrossRef] [Green Version]
- Heron, M. Deaths: Leading Causes for 2017. Natl. Vital Stat. Rep. 2019, 68, 1–76. [Google Scholar]
- Hurd, M.D.; Martorell, P.; Delavande, A.; Mullen, K.J.; Langa, K.M. Monetary costs of dementia in the United States. N. Engl. J. Med. 2013, 368, 1326–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hale, J.M. Cognitive Disparities: The Impact of the Great Depression and Cumulative Inequality on Later-Life Cognitive Function. Demography 2017, 54, 2125–2158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keith, V. Stress, discrimination, and coping in late life. In Handbook of Minority Aging; Whitfield, K.E., Baker, T.A., Eds.; Springer Publishing Company: New York, NY, USA, 2014; pp. 65–84. [Google Scholar]
- Juster, F.T.; Richard, M.S. An Overview of the Health and Retirement Study. J. Hum. Resour. 1995, 30, S7–S56. [Google Scholar] [CrossRef]
- Jacqui, S.; Lindsay, H.R.; Gwenith, G.F.; Amanda, S.; David, W. HRS Psychosocial and Lifestyle Questionnaire 2006–2016; Survey Research Center, Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 2017. [Google Scholar]
- Robert, B.W.; Herzog, A.R. Overview of the Health Measures in the Health and Retirement Survey. J. Human Resour. 1995, 30, S84–S107. [Google Scholar]
- Daviglus, M.L.; Plassman, B.L.; Pirzada, A.; Bell, C.C.; Bowen, P.E.; Burke, J.R.; Connolly, E.S.; Dunbar-Jacob, J.M.; Granieri, E.C.; McGarry, K.; et al. Risk factors and preventive interventions for Alzheimer disease: State of the science. Arch. Neurol. 2011, 68, 1185–1190. [Google Scholar] [CrossRef]
- Barnes, D.E.; Yaffe, K. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol. 2011, 10, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Brandt, J.; Spencer, M.; Folstein, M. The telephone interview for cognitive status. Neuropsychiatry Neuropsychol. Behav. Neurol. 1988, 1, 111–117. [Google Scholar]
- Welsh, K.A.; Breitner, J.C.; Magruder-Habib, K.M. Detection of dementia in the elderly using telephone screening of cognitive status. Neuropsychiatry Neuropsychol. Behav. Neurol. 1993, 6, 103–110. [Google Scholar]
- Mary Beth, O.; Gwenith, G.F.; Herzog, A.R. Documentation of Cognitive Functioning Measures in the Health and Retirement Study; Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 2005. [Google Scholar]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage: Newbury Park, CA, USA, 1991. [Google Scholar]
- Greenland, S.J.E. Commentary: Interactions in Epidemiology: Relevance, Identification, and Estimation. Epidemiology 2009, 20, 14–17. [Google Scholar] [CrossRef]
- Steven, G.H.; Connor, J. Technical Description of the Health and Retirement Study Sample Design; Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 1995. [Google Scholar]
- Qureshi, S.U.; Long, M.E.; Bradshaw, M.R.; Pyne, J.M.; Magruder, K.M.; Kimbrell, T.; Hudson, T.J.; Jawaid, A.; Schulz, P.E.; Kunik, M.E. Does PTSD impair cognition beyond the effect of trauma? J. Neuropsychiatry Clin. Neurosci. 2011, 23, 16–28. [Google Scholar] [CrossRef]
- Aggarwal, N.T.; Wilson, R.S.; Beck, T.L.; Rajan, K.B.; De Leon, C.F.; Evans, D.A.; Everson-Rose, S.A. Perceived stress and change in cognitive function among adults 65 years and older. Psychosom. Med. 2014, 76, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heim, C.; Nemeroff, C.B. The role of childhood trauma in the neurobiology of mood and anxiety disorders: Preclinical and clinical studies. Biol. Psychiatry 2001, 49, 1023–1039. [Google Scholar] [CrossRef] [Green Version]
- Hedges, D.W.; Woon, F.L. Early-life stress and cognitive outcome. Psychopharmacology 2011, 214, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, L.; Joëls, M.; Roozendaal, B.; Wolf, O.T.; Oitzl, M.S. Stress effects on memory: An update and integration. Neurosci. Biobehav. Rev. 2012, 36, 1740–1749. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, L.; Wolf, O.T. The context counts: Congruent learning and testing environments prevent memory retrieval impairment following stress. Cogn. Affect. Behav. Neurosci. 2009, 9, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Schwabe, L.; Wolf, O.T. Stress impairs the reconsolidation of autobiographical memories. Neurobiol. Learn Mem. 2010, 94, 153–157. [Google Scholar] [CrossRef]
- Weerda, R.; Muehlhan, M.; Wolf, O.T.; Thiel, C.M. Effects of acute psychosocial stress on working memory related brain activity in men. Hum. Brain Mapp. 2010, 31, 1418–1429. [Google Scholar] [CrossRef]
- Magariños, A.M.; McEwen, B.S.; Flügge, G.; Fuchs, E. Chronic psychosocial stress causes apical dendritic atrophy of hippocampal CA3 pyramidal neurons in subordinate tree shrews. J. Neurosci. Off. J. Soc. Neurosci. 1996, 16, 3534–3540. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, E.; Czéh, B.; Kole, M.H.; Michaelis, T.; Lucassen, P.J. Alterations of neuroplasticity in depression: The hippocampus and beyond. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2004, 14 (Suppl. 5), S481–S490. [Google Scholar] [CrossRef]
- Brunson, K.L.; Kramár, E.; Lin, B.; Chen, Y.; Colgin, L.L. Mechanisms of late-onset cognitive decline after early-life stress. J. Neurosci. Off. J. Soc. Neurosci. 2005, 25, 9328–9338. [Google Scholar] [CrossRef]
- Salthouse, T.A. When does age-related cognitive decline begin? Neurobiol. Aging 2009, 30, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccinin, A.M.; Muniz-Terrera, G.; Clouston, S.; Reynolds, C.A.; Thorvaldsson, V.; Deary, I.J.; Deeg, D.J.; Johansson, B. Coordinated analysis of age, sex, and education effects on change in MMSE scores. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2013, 68, 374–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deary, I.J.; Corley, J.; Gow, A.J.; Harris, S.E.; Houlihan, L.M.; Marioni, R.E.; Penke, L.; Rafnsson, S.B.; Starr, J.M. Age-associated cognitive decline. Br. Med. Bull. 2009, 92, 135–152. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Venegas, C.; Schneider, D.C.; Myrskyla, M.; Mehta, N.K. Life expectancy with and without cognitive impairment by diabetes status among older Americans. PLoS ONE 2017, 12, e0190488. [Google Scholar] [CrossRef] [Green Version]
- Gottesman, R.F.; Schneider, A.L.; Albert, M.; Alonso, A.; Bandeen-Roche, K.; Coker, L.; Coresh, J.; Knopman, D.; Power, M.C.; Rawlings, A.; et al. Midlife hypertension and 20-year cognitive change: The atherosclerosis risk in communities neurocognitive study. JAMA Neurol. 2014, 71, 1218–1227. [Google Scholar] [CrossRef]
- Howard, J.T.; Sparks, P.J. The Role of Education in Explaining Racial/Ethnic Allostatic Load Differentials in the United States. Biodemography Soc. Biol. 2015, 61, 18–39. [Google Scholar] [CrossRef]
- Brondolo, E.; Brady, N.; Pencille, M.; Beatty, D.; Contrada, R.J. Coping with Racism: A Selective Review of the Literature and a Theoretical and Methodological Critique. J. Behav. Med. 2009, 32, 64–88. [Google Scholar] [CrossRef]
- Nkwata, A.K.; Song, X.; Zhang, M.; Ezeamama, A.E. Change in quality of life over eight years in a nationally representative sample of US adults with heart disease and type 2 diabetes:minority race and toxic stress as keysocial determinants. BMC Public Health 2020, 20, 684. [Google Scholar] [CrossRef]
- Hudson, D.L.; Puterman, E.; Bibbins-Domingo, K.; Matthews, K.A.; Adler, N.E. Race, life course socioeconomic position, racial discrimination, depressive symptoms and self-rated health. Soc. Sci. Med. 2013, 97, 7–14. [Google Scholar] [CrossRef]
- Meyer, J.D. Race-based job discrimination, disparities in job control, and their joint effects on health. Am. J. Ind. Med. 2014, 57, 587–595. [Google Scholar] [CrossRef] [Green Version]
- Malat, J.; Mayorga-Gallo, S.; Williams, D.R. The effects of whiteness on the health of whites in the USA. Soc. Sci. Med. 2018, 199, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T.T.; Aiello, A.E.; Leurgans, S.; Kelly, J.; Barnes, L.L. Self-reported experiences of everyday discrimination are associated with elevated C-reactive protein levels in older African-American adults. Brain Behav. Immun. 2010, 24, 438–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, T.T.; Barnes, L.L.; Bienias, J.L.; Lackland, D.T.; Evans, D.A.; Mendes de Leon, C.F. Perceived discrimination and blood pressure in older African American and white adults. J. Gerontol. Ser. ABiol. Sci. Med. Sci. 2009, 64, 1002–1008. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R.; Mohammed, S.A. Discrimination and racial disparities in health: Evidence and needed research. J. Behav. Med. 2009, 32, 20–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieger, N.; Sidney, S. Racial discrimination and blood pressure: The CARDIA Study of young black and white adults. Am. J. Public Health 1996, 86, 1370–1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, D.R.; Neighbors, H. Racism, discrimination and hypertension: Evidence and needed research. Ethn. Dis. 2001, 11, 800–816. [Google Scholar]
- Farmer, H.R.; Wray, L.A.; Thomas, J.R. Do Race and Everyday Discrimination Predict Mortality Risk? Evidence FROM the Health and Retirement Study. Gerontol. Geriatr. Med. 2019, 5, 2333721419855665. [Google Scholar]
- Jones, C. The impact of racism on health. Ethn. Dis. 2002, 12, S2-10-3. [Google Scholar]
- Dominguez, T.P.; Dunkel-Schetter, C.; Glynn, L.M.; Hobel, C.; Sandman, C.A. Racial differences in birth outcomes: The role of general, pregnancy, and racism stress. Health Psychol. 2008, 27, 194. [Google Scholar] [CrossRef] [Green Version]
- Rankin, K.M.; David, R.J.; Collins, J.W., Jr. African American women’s exposure to interpersonal racial discrimination in public settings and preterm birth: The effect of coping behaviors. Ethn. Dis. 2011, 21, 370–376. [Google Scholar]
- Mustillo, S.; Krieger, N.; Gunderson, E.P.; Sidney, S.; McCreath, H.; Kiefe, C.I. Self-reported experiences of racial discrimination and Black-White differences in preterm and low-birthweight deliveries: The CARDIA Study. Am. J. Public Health 2004, 94, 2125–2131. [Google Scholar] [CrossRef] [PubMed]
- Montross, L.P.; Depp, C.; Daly, J.; Reichstadt, J.; Golshan, S.; Moore, D.; Sitzer, D.; Jeste, D.V. Correlates of self-rated successful aging among community-dwelling older adults. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2006, 14, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Nygren, B.; Aléx, L.; Jonsén, E.; Gustafson, Y.; Norberg, A.; Lundman, B. Resilience, sense of coherence, purpose in life and self-transcendence in relation to perceived physical and mental health among the oldest old. Aging Ment. Health 2005, 9, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.; Iliffe, S. Psychological approach to successful ageing predicts future quality of life in older adults. Health Qual. Life Outcomes 2011, 9, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (N = 6317) | Normal (N = 6019) | Impaired (N = 298) | p-Value |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||
| Age: mean (SD) | 73.9 (6.7) | 73.7 (6.5) | 78.7 (8.1) | |
| Age categories (years) | <0.0001 | |||
| ≤70 | 2076 (32.9) | 2025 (33.6) | 51 (17.1) | |
| 71–79 | 3055 (48.4) | 2942 (48.9) | 113 (37.9) | |
| >80 | 1186 (18.7) | 1052 (17.5) | 132 (45.0) | |
| Sex: Female | 3764 (59.6) | 3601 (59.8) | 163 (54.7) | 0.0782 |
| Marital Status | 0.0002 | |||
| Never married | 177 (02.8) | 167 (02.8) | 10 (03.3) | |
| Married/partnered | 3910 (61.9) | 3761 (62.5) | 149 (50.0) | |
| Separated/Divorced | 672 (10.6) | 633 (10.5) | 39 (13.1) | |
| Widowed | 1558 (24.7) | 1458 (24.2) | 100 (33.6) | |
| Education | <0.0001 | |||
| Less than High School/GED | 1326 (21.0) | 1203 (20.0) | 123 (41.3) | |
| High-school graduate | 2062 (32.6) | 1979 (32.9) | 83 (27.8) | |
| Some college and above | 2927 (46.4) | 2835 (47.1) | 92 (30.9) | |
| Race | 0.0414 | |||
| White/Caucasian | 5217 (82.6) | 4987 (82.8) | 230 (77.2) | |
| Black/AA | 815 (12.9) | 765 (12.7) | 50 (16.8) | |
| Other | 285 (04.5) | 267 (04.4) | 18 (06.0) | |
| Have Health Insurance | 6081 (98.1) | 5810 (98.1) | 271 (97.1) | 0.2474 |
| Ever smoked | 3459 (55.2) | 3299 (55.2) | 160 (54.2) | 0.7745 |
| Current alcohol use | 3209 (50.8) | 3120 (51.8) | 89 (29.9) | <0.0001 |
| No. of comorbidities ever had | <0.0001 | |||
| None | 424 (06.7) | 410 (06.8) | 14 (04.7) | |
| One | 1096 (17.3) | 1061 (17.6) | 35 (11.7) | |
| Two | 1719 (27.2) | 1665 (27.7) | 54 (18.1) | |
| Three or more | 3077 (48.7) | 2882 (47.9) | 195 (65.4) | |
| Diagnosis of HD, T2DM or Stroke | 3177 (50.2) | 2973 (49.4) | 204 (68.5) | <0.0001 |
| Measures of Toxic Stress | ||||
| Chronic stressors | 0.005 | |||
| Low | 4542 (71.9) | 4349 (72.2) | 193 (64.8) | |
| High | 1775 (28.1) | 1670 (27.8) | 105 (35.2) | |
| Everyday discrimination | <0.0001 | |||
| Zero | 5888 (94.3) | 5638 (94.8) | 250 (84.5) | |
| One or more | 357 (05.7) | 311 (05.2) | 46 (15.5) | |
| Perceived constraints | <0.0001 | |||
| Low | 4262 (67.8) | 4122 (68.9) | 140 (47.0) | |
| High | 2021 (32.2) | 1863 (31.1) | 158 (53.0) | |
| Measures of resilience | ||||
| Personal mastery | <0.0001 | |||
| Low | 2206 (34.9) | 2049 (34.0) | 157 (52.7) | |
| High | 4111 (65.1) | 3970 (66.0) | 141 (47.3) | |
| Control over Health | <0.0001 | |||
| Low | 2794 (45.6) | 2624 (44.9) | 170 (60.1) | |
| High | 3329 (54.4) | 3216 (55.1) | 113 (39.9) | |
| Control over finances | <0.0001 | |||
| Low | 2375 (38.1) | 2224 (37.4) | 151 (51.7) | |
| High | 3867 (61.9) | 3726 (62.6) | 141 (48.3) | |
| Control over social life | <0.0001 | |||
| Low | 1892 (30.3) | 1748 (29.4) | 144 (49.7) | |
| High | 4345 (69.7) | 4199 (70.6) | 146 (50.3) | |
| Positive Social Support domains | ||||
| Immediate Family (Spouse & children) | 0.0247 | |||
| Low social support | 2314 (38.6) | 2188 (38.3) | 126 (45.0) | |
| High social support | 3678 (61.4) | 3524 (61.7) | 154 (55.2) | |
| Extended Family (Others & friends) | 0.0095 | |||
| Low social support | 1473 (23.6) | 1388 (23.3) | 85 (30.0) | |
| High social support | 4759 (76.4) | 4561 (76.7) | 198 (70.0) | |
| All Relationship groups combined | <0.0001 | |||
| Low social support | 841 (13.3) | 772 (12.9) | 69 (23.1) | |
| High social support | 5462 (86.7) | 5233 (87.1) | 229 (76.9) |
| Characteristic | All (N = 6317) | White/Caucasian (N = 5217) | Black/African American (N = 815) | Other (N = 285) | p-Value |
|---|---|---|---|---|---|
| Dimensions of Toxic Stress | N (%) | N (%) | N (%) | ||
| Chronic stressors | 0.0084 | ||||
| Low | 4542 (71.9) | 3792 (72.7) | 560 (68.7) | 190 (66.7) | |
| High | 1775 (28.1) | 1425 (27.3) | 255 (31.3) | 95 (33.3) | |
| Everyday discrimination | <0.0001 | ||||
| Zero | 5888 (94.3) | 4925 (95.3) | 716 (90.2) | 247 (87.2) | |
| One or more | 357 (5.8) | 244 (4.7) | 78 (9.8) | 35 (12.8) | |
| Perceived constraints | 0.0009 | ||||
| Low | 4262 (67.8) | 3538 (68.2) | 561 (69.3) | 163 (57.8) | |
| High | 2021 (32.2) | 1653 (31.8) | 249 (30.7) | 119 (42.2) | |
| Measures of resilience | |||||
| Personal mastery | 0.9508 | ||||
| Low | 2206 (34.9) | 1820 (34.9) | 288 (35.3) | 98 (34.4) | |
| High | 4111 (65.1) | 3397 (65.1) | 527 (64.7) | 187 (65.6) | |
| Control over Health | 0.2371 | ||||
| Low | 2794 (45.6) | 2330 (46.0) | 351 (45.2) | 113 (40.8) | |
| High | 3329 (54.4) | 2740 (54.0) | 425 (54.8) | 164 (50.2) | |
| Control over finances | 0.1666 | ||||
| Low | 2375 (38.1) | 1989 (38.5) | 280 (35.0) | 106 (37.7) | |
| High | 3867 (61.9) | 3173 (61.5) | 519 (65.0) | 175 (62.3) | |
| Control over social life | 0.0155 | ||||
| Low | 1892 (30.3) | 1594 (30.9) | 207 (26.0) | 91 (32.3) | |
| High | 4345 (69.7) | 3565 (69.1) | 589 (74.0) | 191 (67.7) | |
| Positive Social Support (All Relationship groups combined) | 0.3237 | ||||
| Low social support | 841 (13.3) | 681 (13.1) | 115 (14.2) | 45 (15.8) | |
| High social support | 5462 (86.7) | 4525 (86.9) | 697 (85.8) | 240 (84.2) | |
| Neurocognitive impairment | 0.0414 | ||||
| Normal | 6019 (95.3) | 4987 (95.6) | 765 (93.9) | 267 (93.7) | |
| Impaired | 298 (4.7) | 230 (4.4) | 50 (6.1) | 18 (6.3) |
| Variable | n/N | Model 1 (Crude) * | Model 2 ɤ | Model 3 α | Model 4 † |
|---|---|---|---|---|---|
| Race | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Black (AA) vs. Caucasian | 50/815 | 1.76 (1.21, 2.56) | 1.33 (0.89, 1.99) | 1.26 (0.82, 1.94) | 1.32 (0.87, 2.00) |
| Other vs. Caucasian | 18/285 | 2.09 (1.18, 3.72) | 1.63 (0.95, 2.82) | 1.45 (0.87, 2.43) | 1.59 (0.93, 2.72) |
| Toxic stress indicators | |||||
| Everyday discrimination | |||||
| One or more experiences vs. None | 46/357 | 4.05 (2.61, 6.30) | 3.31(2.12, 5.19) | ||
| Chronic stressors | |||||
| High vs. low chronic stress | 105/1775 | 1.88 (1.43, 2.49) | 1.88 (1.42, 2.48) | ||
| Perceived constraints | |||||
| High vs. Low | 158/2021 | 2.91 (2.03, 4.17) | 2.16 (1.52, 3.07) | ||
| Resilience indicators | |||||
| Perceived Mastery | |||||
| Low vs. High global mastery | 157/2206 | 2.38 (1.78, 3.20) | 1.85 (1.38, 2.48) | ||
| Positive social support from all groups | |||||
| Low vs. High | 69/841 | 1.89 (1.36, 2.62) | 1.45 (0.95, 2.21) | ||
| Domain-specific mastery | |||||
| Low vs. High control over health | 170/2794 | 2.04 (1.54, 2.70) | 1.70 (1.31, 2.21) | ||
| Low vs. High control over finances | 151/2375 | 1.93 (1.46, 2.57) | 1.96 (1.44, 2.67) | ||
| Low vs. High Social life | 144/1892 | 2.40 (1.70, 3.38) | 2.02 (1.43, 2.85) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nkwata, A.K.; Zhang, M.; Song, X.; Giordani, B.; Ezeamama, A.E. The Relationship of Race, Psychosocial Stress and Resiliency Indicators to Neurocognitive Impairment among Older Americans Enrolled in the Health and Retirement Survey: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 1358. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031358
Nkwata AK, Zhang M, Song X, Giordani B, Ezeamama AE. The Relationship of Race, Psychosocial Stress and Resiliency Indicators to Neurocognitive Impairment among Older Americans Enrolled in the Health and Retirement Survey: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(3):1358. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031358
Chicago/Turabian StyleNkwata, Allan K., Ming Zhang, Xiao Song, Bruno Giordani, and Amara E. Ezeamama. 2021. "The Relationship of Race, Psychosocial Stress and Resiliency Indicators to Neurocognitive Impairment among Older Americans Enrolled in the Health and Retirement Survey: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 3: 1358. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031358