Gender Differences in the Relationships among Metabolic Syndrome and Various Obesity-Related Indices with Nonalcoholic Fatty Liver Disease in a Taiwanese Population


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Recruitment
2.2. Collection of Demographic, Medical and Laboratory Data
2.3. Definition of MetS
2.4. Calculations of Obesity-Related Indices
2.5. Assessment of NAFLD
2.6. Ethics Statement
2.7. Statistical Analysis
3. Results
3.1. Determinants of NAFLD
3.2. Interactions between Gender and MetS and Obesity-Related Indices on NAFLD
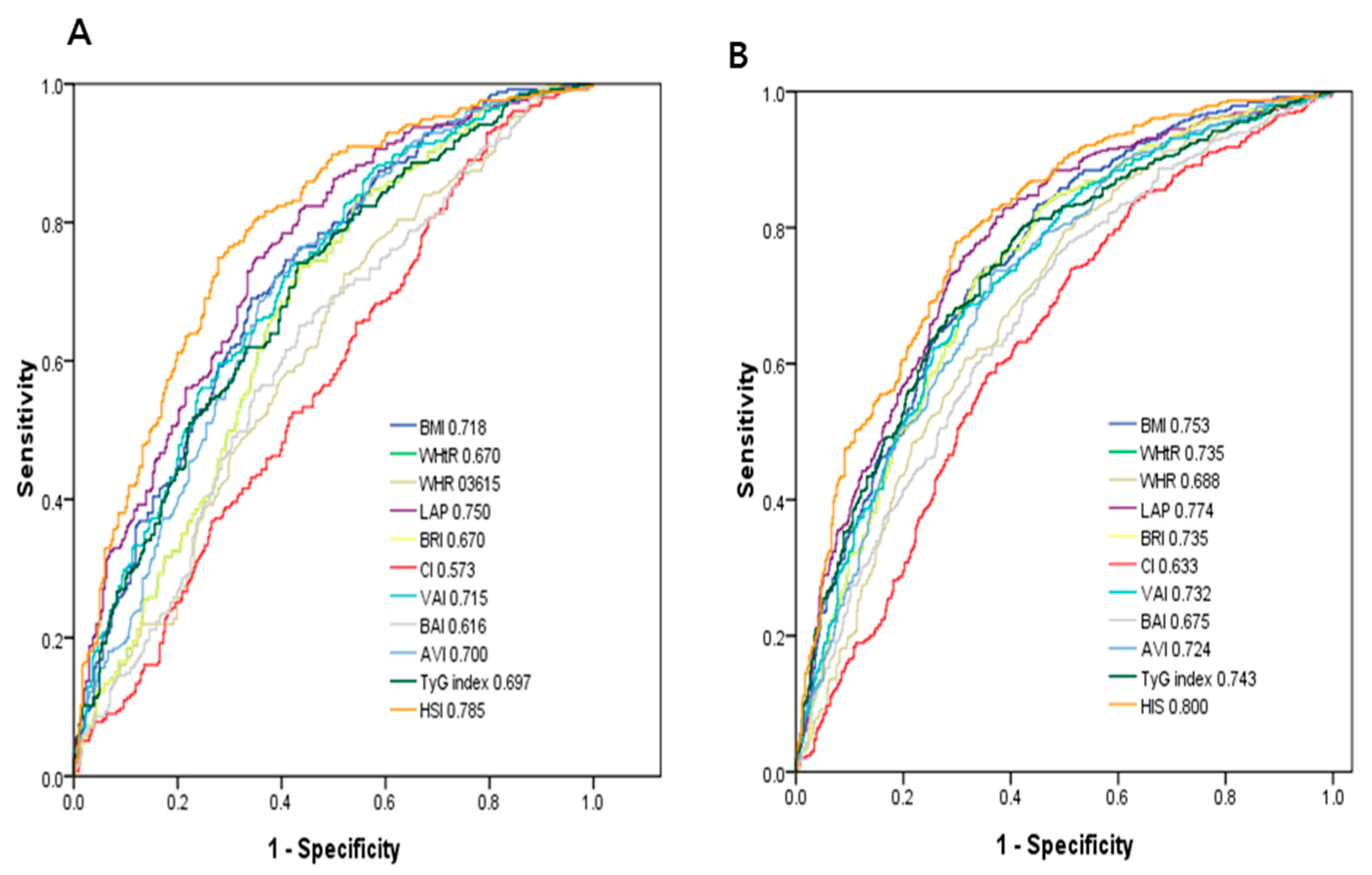
3.3. ROC Curve Analysis for the Obesity-Related Indices in Identifying NAFLD
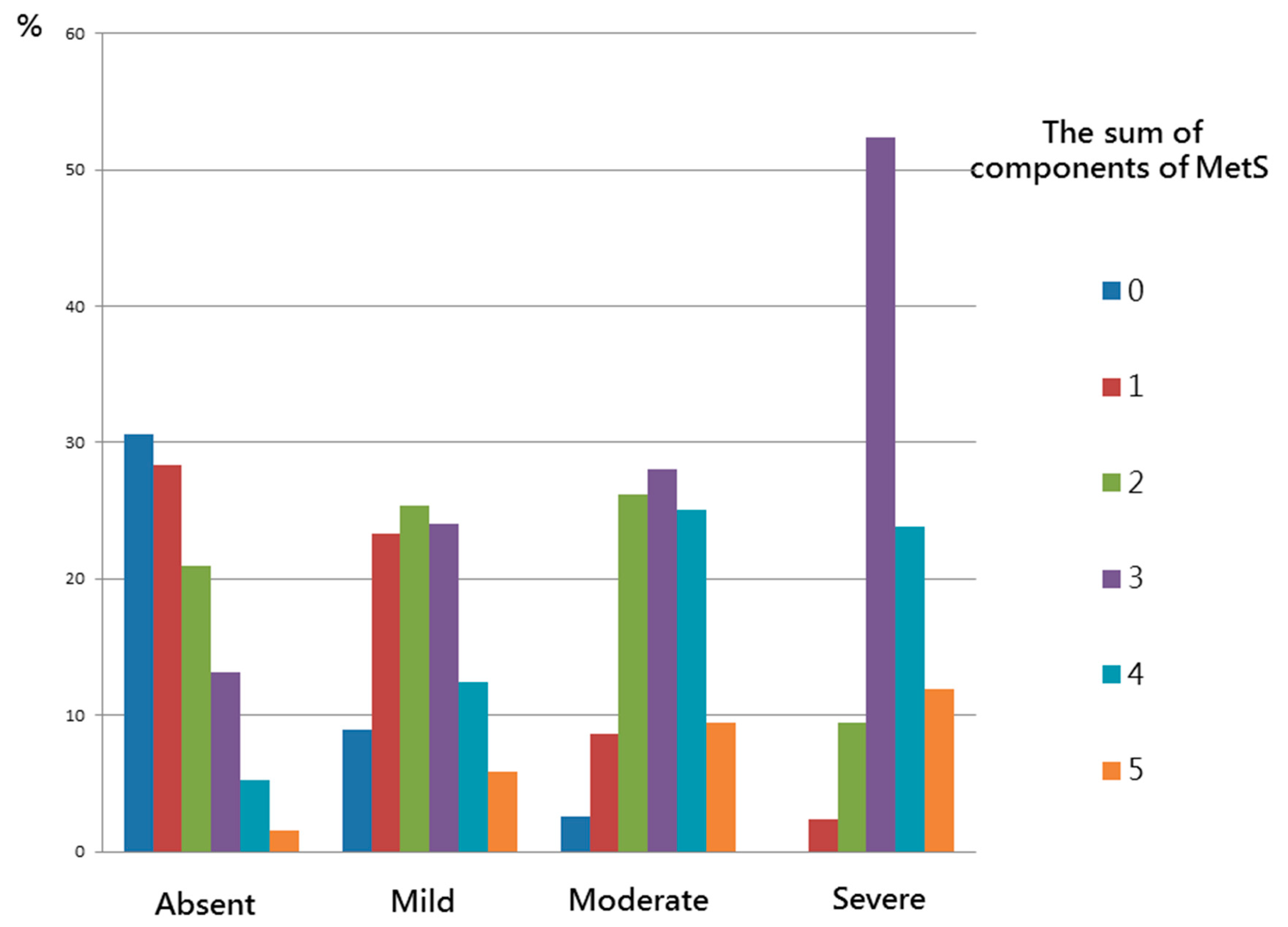
3.4. Association between MetS and the Obesity-Related Indices with the Severity of NAFLD
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclosure
References
- Bellentani, S. The epidemiology of non-alcoholic fatty liver disease. Liver Int. 2017, 37, 81–84. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident diabetes mellitus: An updated meta-analysis of 501 022 adult individuals. Gut 2020. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Hwang, L.-C.; Bai, C.-H.; Chen, C.-J. Prevalence of Obesity and Metabolic Syndrome in Taiwan. J. Formos. Med. Assoc. 2006, 105, 626–635. [Google Scholar] [CrossRef] [Green Version]
- Adejumo, E.N.; Adejumo, A.O.; Azenabor, A.; Ekun, A.O.; Enitan, S.S.; Adebola, O.K.; Ogundahunsi, O.A. Anthropometric parameter that best predict metabolic syndrome in South west Nigeria. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 48–54. [Google Scholar] [CrossRef]
- Cheng, C.-H.; Ho, C.-C.; Yang, C.-F.; Huang, Y.-C.; Lai, C.-H.; Liaw, Y.-P. Waist-to-hip ratio is a better anthropometric index than body mass index for predicting the risk of type 2 diabetes in Taiwanese population. Nutr. Res. 2010, 30, 585–593. [Google Scholar] [CrossRef]
- Huang, K.-C.; Lin, W.-Y.; Lee, L.-T.; Chen, C.-Y.; Lo, H.; Hsia, H.-H.; Liu, I.-L.; Shau, W.-Y.; Lin, R.-S. Four anthropometric indices and cardiovascular risk factors in Taiwan. Int. J. Obes. 2002, 26, 1060–1068. [Google Scholar] [CrossRef] [Green Version]
- Mansourghanaei, R.; Mansour-Ghanaei, F.; Naghipour, M.; Joukar, F.; Atrkar-Roushan, Z.; Tabatabaii, M.; Ghorani, N. The role of anthropometric indices in the prediction of non-alcoholic fatty liver disease in the PERSIAN Guilan Cohort study (PGCS). J. Med. Life 2018, 11, 194–202. [Google Scholar] [CrossRef]
- Motamed, N.; Rabiee, B.; Hemasi, G.R.; Ajdarkosh, H.; Khonsari, M.R.; Maadi, M.; Keyvani, H.; Zamani, F. Body Roundness Index and Waist-to-Height Ratio are Strongly Associated With Non-Alcoholic Fatty Liver Disease: A Population-Based Study. Zahedan J. Res. Med. Sci. 2016, 16, e39575. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Kim, D.; Kim, H.J.; Lee, C.-H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.-H.; Cho, S.-H.; Sung, M.-W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Isomaa, B.; Henricsson, M.; Almgren, P.; Tuomi, T.; Taskinen, M.-R.; Groop, L. The metabolic syndrome influences the risk of chronic complications in patients with Type II diabetes. Diabetologia 2001, 44, 1148–1154. [Google Scholar] [CrossRef] [Green Version]
- Tan, C.E.; Ma, S.; Wai, D.; Chew, S.-K.; Tai, E.-S. Can We Apply the National Cholesterol Education Program Adult Treatment Panel Definition of the Metabolic Syndrome to Asians? Diabetes Care 2004, 27, 1182–1186. [Google Scholar] [CrossRef] [Green Version]
- Kahn, H.S. The “lipid accumulation product” performs better than the body mass index for recognizing cardiovascular risk: A population-based comparison. BMC Cardiovasc. Disord. 2005, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.M.; Bredlau, C.; Bosy-Westphal, A.; Mueller, M.; Shen, W.; Gallagher, D.; Maeda, Y.; McDougall, A.; Peterson, C.M.; Ravussin, E.; et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity 2013, 21, 2264–2271. [Google Scholar] [CrossRef] [Green Version]
- Valdez, R. A simple model-based index of abdominal adiposity. J. Clin. Epidemiol. 1991, 44, 955–956. [Google Scholar] [CrossRef]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A. Visceral Adiposity Index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 33, 920–922. [Google Scholar] [CrossRef] [Green Version]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A Better Index of Body Adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rodríguez-Morán, M. Abdominal volume index. An anthropometry-based index for estimation of obesity is strongly related to impaired glucose tolerance and type 2 diabetes mellitus. Arch. Med. Res. 2003, 34, 428–432. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Simental-Mendía, L.E.; González-Ortiz, M.; Martínez-Abundis, E.; Ramos-Zavala, M.G.; Hernández-González, S.O.; Jacques-Camarena, O.; Rodríguez-Morán, M. The Product of Triglycerides and Glucose, a Simple Measure of Insulin Sensitivity. Comparison with the Euglycemic-Hyperinsulinemic Clamp. J. Clin. Endocrinol. Metab. 2010, 95, 3347–3351. [Google Scholar] [CrossRef] [Green Version]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American association for the study of liver diseases, American college of gastroenterology, and the American gastroenterological association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Jia, J.; Li, Y.M.; Wang, B.Y.; Lu, L.G.; Shi, J.P.; Chan, L.Y. Chinese association for the study of liver disease Guidelines for the diagnosis and management of nonalcoholic fatty liver disease: Update. J. Dig. Dis. 2010, 12, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Farrell, G.C.; Chitturi, S.; Lau, G.K.K.; Sollano, J.D. Guidelines for the assessment and management of non-alcoholic fatty liver disease in the Asia?Pacific region: Executive summary. J. Gastroenterol. Hepatol. 2007, 22, 775–777. [Google Scholar] [CrossRef] [PubMed]
- Sirota, J.C.; McFann, K.; Targher, G.; Johnson, R.J.; Chonchol, M.; Jalal, D.I. Elevated serum uric acid levels are associated with non-alcoholic fatty liver disease independently of metabolic syndrome features in the United States: Liver ultrasound data from the National Health and Nutrition Examination Survey. Metabolism 2013, 62, 392–399. [Google Scholar] [CrossRef] [Green Version]
- Marchesini, G.; Bugianesi, E.; Forlani, G.; Cerrelli, F.; Lenzi, M.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; Melchionda, N.; et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003, 37, 917–923. [Google Scholar] [CrossRef]
- Manco, M. Metabolic syndrome in childhood from impaired carbohydrate metabolism to nonalcoholic fatty liver disease. J. Am. Coll. Nutr. 2011, 30, 295–303. [Google Scholar] [CrossRef]
- Williams, C.D.; Stengel, J.; Asike, M.I.; Torres, D.M.; Shaw, J.; Contreras, M.; Landt, C.L.; Harrison, S.A. Prevalence of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis Among a Largely Middle-Aged Population Utilizing Ultrasound and Liver Biopsy: A Prospective Study. Gastroenterology 2011, 140, 124–131. [Google Scholar] [CrossRef]
- Gaggini, M.; Morelli, M.; Buzzigoli, E.; DeFronzo, R.A.; Bugianesi, E.; Gastaldelli, A. Non-Alcoholic Fatty Liver Disease (NAFLD) and Its Connection with Insulin Resistance, Dyslipidemia, Atherosclerosis and Coronary Heart Disease. Nutrients 2013, 5, 1544–1560. [Google Scholar] [CrossRef]
- Kojta, I.; Chacińska, M.; Błachnio-Zabielska, A.U. Obesity, Bioactive Lipids, and Adipose Tissue Inflammation in Insulin Resistance. Nutrients 2020, 12, 1305. [Google Scholar] [CrossRef]
- Boutari, C.; Perakakis, N.; Mantzoros, C.S. Association of Adipokines with Development and Progression of Nonalcoholic Fatty Liver Disease. Endocrinol. Metab. 2018, 33, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Motamed, N.; Sohrabi, M.; Poustchi, H.; Maadi, M.; Malek, M.; Keyvani, H.; Amoli, M.S.; Zamani, F. The six obesity indices, which one is more compatible with metabolic syndrome? A population based study. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-S.; Lin, T.-H.; Guo, S.-E.; Tsai, M.-H.; Chiang, M.-S.; Huang, T.-J.; Chen, M.-Y. Waist-to-height ratio is a useful index for nonalcoholic fatty liver disease in children and adolescents: A secondary data analysis. BMC Public Health 2017, 17, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Targher, G.; Lonardo, A. Ultrasonographic fatty liver indicator detects mild steatosis and correlates with metabolic/histological parameters in various liver diseases. Metabolism 2017, 72, 57–65. [Google Scholar] [CrossRef]
- Nelson, S.M.; Hoskins, J.D.; Lisanti, C.; Chaudhuri, J. Ultrasound Fatty Liver Indicator: A Simple Tool for Differentiating Steatosis From Nonalcoholic Steatohepatitis: Validity in the Average Obese Population. J. Ultrasound Med. 2020, 39, 749–759. [Google Scholar] [CrossRef]
- Praveenraj, P.; Gomes, R.M.; Kumar, S.; Karthikeyan, P.; Shankar, A.; Parthasarathi, R.; Senthilnathan, P.; Rajapandian, S.; Palanivelu, C. Prevalence and Predictors of Non-Alcoholic Fatty Liver Disease in Morbidly Obese South Indian Patients Undergoing Bariatric Surgery. Obes. Surg. 2015, 25, 2078–2087. [Google Scholar] [CrossRef]
- Frith, J.; Day, C.P.; Robinson, L.; Elliott, C.S.; Jones, D.E.; Newton, J.L. Potential strategies to improve uptake of exercise interventions in non-alcoholic fatty liver disease. J. Hepatol. 2010, 52, 112–116. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Dos-Santos-Silva, I.; A Leon, D.; Douglas, I.J.; Smeeth, L. Association of BMI with overall and cause-specific mortality: A population-based cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol. 2018, 6, 944–953. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, G.; Miglioli, L.; Masutti, F.; Tiribelli, C.; Marchesini, G.; Bellentani, S. Prevalence of and risk factors for nonalcoholic fatty liver disease: The Dionysos nutrition and liver study. Hepatology 2005, 42, 44–52. [Google Scholar] [CrossRef]
- Milic, S.; Lulić, D.; Štimac, D. Non-alcoholic fatty liver disease and obesity: Biochemical, metabolic and clinical presentations. World J. Gastroenterol. 2014, 20, 9330–9337. [Google Scholar]
- Hsiao, T.; Chen, J.; Wang, J.-D. Insulin resistance and ferritin as major determinants of nonalcoholic fatty liver disease in apparently healthy obese patients. Int. J. Obes. 2004, 28, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thamer, C.; Machann, J.; Haap, M.; Stefan, N.; Heller, E.; Schnödt, B.; Stumvoll, M.; Claussen, C.; Fritsche, A.; Schick, F.; et al. Intrahepatic lipids are predicted by visceral adipose tissue mass in healthy subjects. Diabetes Care 2004, 27, 2726–2729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marin, P.; Andersson, B.; Ottosson, M.; Olbe, L.; Chowdhury, B.; Kvist, H.; Holm, G.; Sjöström, L.; Björntorp, P. The morphology and metabolism of intraabdominal adipose tissue in men. Metabolism 1992, 41, 1242–1248. [Google Scholar] [CrossRef]
- Dai, H.; Wang, W.; Chen, R.; Chen, Z.; Lu, Y.; Yuan, H. Lipid accumulation product is a powerful tool to predict non-alcoholic fatty liver disease in Chinese adults. Nutr. Metab. 2017, 14, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Hu, J.; Li, Z.; Li, T.; Chen, M.; Wu, L.; Liu, W.; Han, H.; Yao, R.; Fu, L. A Novel Indicator Of Lipid Accumulation Product Associated With Metabolic Syndrome In Chinese Children And Adolescents. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2075–2083. [Google Scholar] [CrossRef] [Green Version]
- Ozcabi, B.; Demirhan, S.; Akyol, M.; Akay, H.O.; Güven, A. Lipid accumulation product is a predictor of nonalcoholic fatty liver disease in childhood obesity. Korean J. Pediatr. 2019, 62, 450–455. [Google Scholar] [CrossRef] [Green Version]
- Yoo, H.J.; Hong, S.-H.; Kim, J.A.; Lee, Y.-B.; Roh, E.; Mook, C.K.; Baik, S.H. The Waist-to-Hip Ratio is a Better Obesity Index than Body Mass Index and Waist Circumference for Screening for Nonalcoholic Fatty Liver Disease in Postmenopausal Women. In Proceedings of the 21st European Congress of Endocrinology; BioScientifica: Bristol, UK, 2019. [Google Scholar]
- Hu, X.; Huang, Y.; Bao, Z.; Wang, Y.; Shi, D.; Liu, F.; Gao, Z.; Yu, X. Prevalence and factors associated with nonalcoholic fatty liver disease in shanghai work-units. BMC Gastroenterol. 2012, 12, 123. [Google Scholar] [CrossRef] [Green Version]
- Benites-Zapata, V.A.; Toro-Huamanchumo, C.J.; Urrunaga-Pastor, D.; Guarnizo-Poma, M.; Lazaro-Alcantara, H.; Paico-Palacios, S.; Pantoja-Torres, B.; del Carmen Ranilla-Seguin, V.; Insulin Resistance and Metabolic Syndrome Research Group. High waist-to-hip ratio levels are associated with insulin resistance markers in normal-weight women. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 636–642. [Google Scholar] [CrossRef]
- Ilhan, G.A.; Yildizhan, B. Visceral adiposity indicators as predictors of metabolic syndrome in postmenopausal women. J. Turk. Soc. Obstet. Gynecol. 2019, 16, 164–168. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Ballestri, S.; Fairweather, D.; Win, S.; Than, T.A.; Abdelmalek, M.F.; Suzuki, A. Sex Differences in Nonalcoholic Fatty Liver Disease: State of the Art and Identification of Research Gaps. Hepatology 2019, 70, 1457–1469. [Google Scholar] [CrossRef]
- Lonardo, A.; Suzuki, A. Sexual Dimorphism of NAFLD in Adults. Focus on Clinical Aspects and Implications for Practice and Translational Research. J. Clin. Med. 2020, 9, 1278. [Google Scholar] [CrossRef] [PubMed]
- Barton, M. Cholesterol and atherosclerosis: Modulation by oestrogen. Curr. Opin. Lipidol. 2013, 24, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.M.; Brancati, F.L.; Diehl, A.M. Nonalcoholic fatty liver disease. Gastroenterology 2002, 122, 1649–1657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovejoy, J.C.; Champagne, C.M.; De Jonge, L.; Xie, H.; Smith, S.R. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int. J. Obes. 2008, 32, 949–958. [Google Scholar] [CrossRef] [Green Version]
- Cooke, P.S.; Naaz, A. Role of Estrogens in Adipocyte Development and Function. Exp. Biol. Med. 2004, 229, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Abdelmalek, M.F.; Pang, H.; Guy, C.D.; Smith, A.D.; Diehl, A.M.; Suzuki, A. Gender and menopause impact severity of fibrosis among patients with nonalcoholic steatohepatitis. Hepatology 2014, 59, 1406–1414. [Google Scholar] [CrossRef]
- Khan, R.S.; Bril, F.; Cusi, K.; Newsome, P.N. Modulation of Insulin Resistance in Nonalcoholic Fatty Liver Disease. Hepatology 2019, 70, 711–724. [Google Scholar] [CrossRef]
- Fujii, H.; Kawada, N.; Japan Study Group of NAFLD (JSG-NAFLD). Japan Study Group of NAFLD (JSG-NAFLD) The Role of Insulin Resistance and Diabetes in Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2020, 21, 3863. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Meale (n = 764) | Female (n = 1205) | ||||
|---|---|---|---|---|---|---|
| NAFLD (−) (n = 410) | NAFLD (+) (n = 354) | p | NAFLD (−) (n = 733) | NAFLD (+) (n = 472) | p | |
| The severity of NAFLD | <0.001 | <0.001 | ||||
| Absent | 100 | 0 | 100 | 0 | ||
| Mild | 0 | 50.3 | 0 | 54.9 | ||
| Moderate | 0 | 40.6 | 0 | 40.5 | ||
| Sever | 0 | 5.6 | 0 | 4.7 | ||
| Age (year) | 56.36 ± 14.47 | 53.86 ± 13.41 | 0.014 | 53.20 ± 13.85 | 57.03 ± 11.77 | <0.001 |
| Systolic BP (mmHg) | 129.83 ± 17.56 | 133.49 ± 17.13 | 0.004 | 128.22 ± 21.25 | 137.28 ± 19.67 | <0.001 |
| Diastolic BP (mmHg) | 76.81 ± 10.82 | 80.73 ± 11.31 | <0.001 | 75.05 ± 12.28 | 77.74 ± 10.45 | <0.001 |
| Current smoking (%) | 24.14 | 28.77 | 0.148 | 3.16 | 1.92 | 0.194 |
| Diabetes mellitus history (%) | 10.00 | 13.84 | 0.100 | 5.32 | 16.31 | <0.001 |
| Hypertension history (%) | 26.59 | 30.23 | 0.265 | 17.05 | 31.78 | <0.001 |
| Hyperlipidemia history (%) | 2.20 | 4.80 | 0.047 | 0.82 | 2.75 | 0.008 |
| MetS (%) | 22.98 | 50.56 | <0.001 | 18.33 | 55.08 | <0.001 |
| Laboratory parameters | ||||||
| AST (U/L) | 26.28 ± 7.93 | 31.79 ± 14.82 | <0.001 | 24.58 ± 8.05 | 28.21 ± 13.60 | <0.001 |
| ALT (U/L) | 23.77 ± 14.56 | 39.88 ± 28.01 | <0.001 | 18.50 ± 11.50 | 27.77 ± 17.69 | <0.001 |
| Fasting glucose (mg/dL) | 98.52 ± 24.16 | 104.76 ± 30.37 | 0.002 | 93.17 ± 18.80 | 108.39 ± 33.77 | <0.001 |
| Triglyceride (mg/dL) | 99.5 (74–138.25) | 146.5 (100.75–217) | <0.001 | 82 (61–116.5) | 128 (96.25–175) | <0.001 |
| Total cholesterol (mg/dL) | 193.04 ± 37.06 | 196.74 ± 37.49 | 0.171 | 203.02 ± 36.94 | 207.12 ± 37.34 | 0.062 |
| HDL cholesterol (mg/dL) | 49.00 ± 11.08 | 42.94 ± 8.42 | <0.001 | 60.43 ± 13.71 | 52.19 ± 11.47 | <0.001 |
| LDL cholesterol (mg/dL) | 118.56 ± 33.83 | 121.22 ± 33.06 | 0.274 | 117.14 ± 32.26 | 125.40 ± 36.86 | <0.001 |
| eGFR (mL/min/1.73 m2) | 88.31 ± 13.07 | 89.86 ± 12.87 | 0.099 | 90.51 ± 19.12 | 87.98 ± 16.88 | 0.019 |
| Uric acid (mg/dL) | 6.40 ± 1.41 | 6.74 ± 1.57 | 0.002 | 4.92 ± 1.25 | 5.46 ± 1.26 | <0.001 |
| Obesity-related indices | ||||||
| BMI (kg/m2) | 24.42 ± 3.25 | 26.97 ± 3.38 | <0.001 | 23.11 ± 3.45 | 26.64 ± 3.91 | <0.001 |
| WHtR | 0.51 ± 0.06 | 0.55 ± 0.05 | <0.001 | 0.49 ± 0.06 | 0.55 ± 0.06 | <0.001 |
| WHR | 0.90 ± 0.08 | 0.92 ± 0.06 | 0.001 | 0.82 ± 0.08 | 0.87± 0.07 | <0.001 |
| LAP | 29.56 ± 27.01 | 55.65 ± 44.30 | <0.001 | 21.85 ± 19.51 | 47.26 ± 43.12 | <0.001 |
| BRI | 3.67 ± 1.11 | 4.35 ± 1.11 | <0.001 | 3.31 ± 1.24 | 4.41 ± 1.27 | <0.001 |
| CI | 1.23 ± 0.08 | 1.26 ± 0.07 | <0.001 | 1.18 ± 0.09 | 1.22 ± 0.09 | <0.001 |
| VAI | 3.41 ± 2.66 | 5.84 ± 5.11 | <0.001 | 3.17 ± 2.43 | 6.16 ± 8.21 | <0.001 |
| BAI | 26.48 ± 3.53 | 27.89 ± 3.78 | <0.001 | 30.36 ± 4.37 | 33.03 ± 4.88 | <0.001 |
| AVI | 15.08 ± 2.86 | 17.18 ± 3.15 | <0.001 | 12.38 ± 2.88 | 14.78 ± 3.19 | <0.001 |
| TyG index | 8.51 ± 0.56 | 8.94 ± 0.62 | <0.001 | 8.27 ± 0.53 | 8.83 ± 0.62 | <0.001 |
| HSI | 31.7 ± 4.8 | 36.9 ± 5.2 | <0.001 | 31.1 ± 4.4 | 36.7 ± 5.2 | <0.001 |
| Characteristics | Male (n = 764) | Female (n = 1205) | Interaction p | ||||
|---|---|---|---|---|---|---|---|
| Multivariable | Multivariable | ||||||
| OR | 95% Confidence Interval | p | OR | 95% Confidence Interval | p | ||
| MetS | 2.716 | 1.914–3.854 | <0.001 | 4.034 | 2.997–5.428 | <0.001 | 0.019 |
| Obesity-related indices | |||||||
| BMI (per 1 kg/m2) | 1.211 | 1.143–1.282 | <0.001 | 1.257 | 1.205–1.311 | <0.001 | 0.156 |
| WHtR (per 0.01) | 1.120 | 1.080–1.162 | <0.001 | 1.126 | 1.099–1.154 | <0.001 | 0.107 |
| WHR (per 0.01) | 1.034 | 1.004–1.065 | 0.024 | 1.068 | 1.044–1.093 | <0.001 | 0.025 |
| LAP (per 1) | 1.023 | 1.016–1.030 | <0.001 | 1.038 | 1.030–1.045 | <0.001 | 0.001 |
| BRI (per 1) | 1.693 | 1.416–2.024 | <0.001 | 1.766 | 1.565–1.992 | <0.001 | 0.080 |
| CI (per 0.1) | 1.552 | 1.211–1.990 | <0.001 | 1.401 | 1.204–1.631 | <0.001 | 0.512 |
| VAI (per 1) | 1.212 | 1.139–1.290 | <0.001 | 1.257 | 1.191–1.326 | <0.001 | 0.244 |
| BAI (per 1) | 1.098 | 1.034–1.167 | 0.002 | 1.114 | 1.075–1.156 | <0.001 | 0.968 |
| AVI (per 1) | 1.220 | 1.135–1.313 | <0.001 | 1.241 | 1.176–1.310 | <0.001 | 0.452 |
| TyG index (per 1) | 2.888 | 2.132–3.913 | <0.001 | 4.493 | 3.387–5.959 | <0.001 | 0.012 |
| HSI (per 1) | 1.215 | 1.153–1.280 | <0.001 | 1.264 | 1.214–1.315 | <0.001 | 0.707 |
| MetS | Male | Female | Interaction p | ||||
|---|---|---|---|---|---|---|---|
| Multivariable | Multivariable | ||||||
| OR | 95% Confidence Interval | p | OR | 95% Confidence Interval | p | ||
| Age <45 years old (n = 469) | 4.637 | 1.875–11.469 | 0.001 | 8.452 | 3.692–19.352 | <0.001 | 0.340 |
| Age 45–55 years old (n = 501) | 2.484 | 1.181–5.224 | 0.016 | 5.967 | 3.086–11.540 | <0.001 | 0.047 |
| Age 55–65 years old (n = 496) | 3.124 | 1.431–6.820 | 0.004 | 3.763 | 2.152–6.580 | <0.001 | 0.739 |
| Age ≥65 years old (n = 503) | 2.645 | 1.435–4.874 | 0.002 | 2.753 | 1.586–4.778 | <0.001 | 0.707 |
| Absent (n = 1143) | Mild (n = 437) | Moderate (n = 347) | Severe (n = 42) | p | |
|---|---|---|---|---|---|
| Diabetes mellitus history (%) | 7.0 | 13.0 * | 18.4 * | 11.9 | <0.001 |
| Hypertension history (%) | 20.5 | 29.7 * | 33.7 * | 23.8 | <0.001 |
| Hyperlipidemia history (%) | 1.3 | 3.2 | 4.0 * | 4.8 | 0.006 |
| Obesity-related indices | |||||
| BMI (kg/m2) | 23.58 ± 3.44 | 25.66 ± 3.03 * | 27.68 ± 3.77 *,† | 31.06 ± 4.23 *,†,# | <0.001 |
| WHtR | 0.50 ± 0.06 | 0.53 ± 0.05 * | 0.56 ± 0.06 *,† | 0.61 ± 0.05 *,†,# | <0.001 |
| WHR | 0.85 ± 0.09 | 0.88 ± 0.07 * | 0.90 ± 0.07 *,† | 0.93 ± 0.07 *,† | <0.001 |
| LAP | 24.62 ± 22.78 | 42.36 ± 35.44 * | 58.58 ± 50.38 *,† | 75.52 ± 43.83 *,†,# | <0.001 |
| BRI | 3.44 ± 1.21 | 4.05 ± 1.03 * | 4.66 ± 1.25 *,† | 5.60 ± 1.18 *,†,# | <0.001 |
| CI | 1.20 ± 0.09 | 1.22 ± 0.08 * | 1.24 ± 0.08 *,† | 1.28 ± 0.08 *,† | <0.001 |
| VAI | 3.26 ± 2.51 | 5.21 ± 4.79 * | 6.96 ± 9.27 *,† | 6.67 ± 3.95 * | <0.001 |
| BAI | 28.95 ± 4.49 | 30.26 ± 4.57 * | 31.63 ± 5.76 *,† | 33.73 ± 4.03 *,† | <0.001 |
| AVI | 13.36 ± 3.15 | 14.88 ± 3.02 * | 16.54± 3.37 *,† | 19.37 ± 3.74 *,†,# | <0.001 |
| TyG index | 8.35 ± 0.55 | 8.74 ± 0.61 * | 9.03 ± 0.62 *,† | 9.08 ± 0.54 *,† | <0.001 |
| HSI | 31.3 ± 4.6 | 34.9 ± 4.2 * | 38.4 ± 5.1 *,† | 42.9 ± 5.5 *,†,# | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, I.-T.; Lee, M.-Y.; Wang, C.-W.; Wu, D.-W.; Chen, S.-C. Gender Differences in the Relationships among Metabolic Syndrome and Various Obesity-Related Indices with Nonalcoholic Fatty Liver Disease in a Taiwanese Population. Int. J. Environ. Res. Public Health 2021, 18, 857. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18030857
Lin I-T, Lee M-Y, Wang C-W, Wu D-W, Chen S-C. Gender Differences in the Relationships among Metabolic Syndrome and Various Obesity-Related Indices with Nonalcoholic Fatty Liver Disease in a Taiwanese Population. International Journal of Environmental Research and Public Health. 2021; 18(3):857. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18030857
Chicago/Turabian StyleLin, I-Ting, Mei-Yueh Lee, Chih-Wen Wang, Da-Wei Wu, and Szu-Chia Chen. 2021. "Gender Differences in the Relationships among Metabolic Syndrome and Various Obesity-Related Indices with Nonalcoholic Fatty Liver Disease in a Taiwanese Population" International Journal of Environmental Research and Public Health 18, no. 3: 857. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18030857