
Relationships between Physical and Mental Health in Adolescents from Low-Income, Rural Communities: Univariate and Multivariate Analyses



Abstract
:1. Introduction
Current Study
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Parent Demographic Survey
2.2.2. Student Demographic Survey
2.2.3. PROMIS Pediatric Item Bank v1.0-Physical Activity-Short Form 8a
2.2.4. PROMIS Pediatric Item Bank v2.0-Anxiety-Short Form 8a
2.2.5. PROMIS Pediatric Item Bank v2.0-Depressive Symptoms-Short Form 8a
2.2.6. PROMIS Pediatric Item Bank v1.0-Psychological Stress Experiences-Short Form 8a
2.2.7. Body Shape Satisfaction Scale (BSS)
2.2.8. Rosenberg Self-Esteem Scale (RSES)
2.2.9. Functional Fitness and Health Testing
2.3. Procedure
2.4. Statistical Analyses
2.5. Missing Data
3. Results
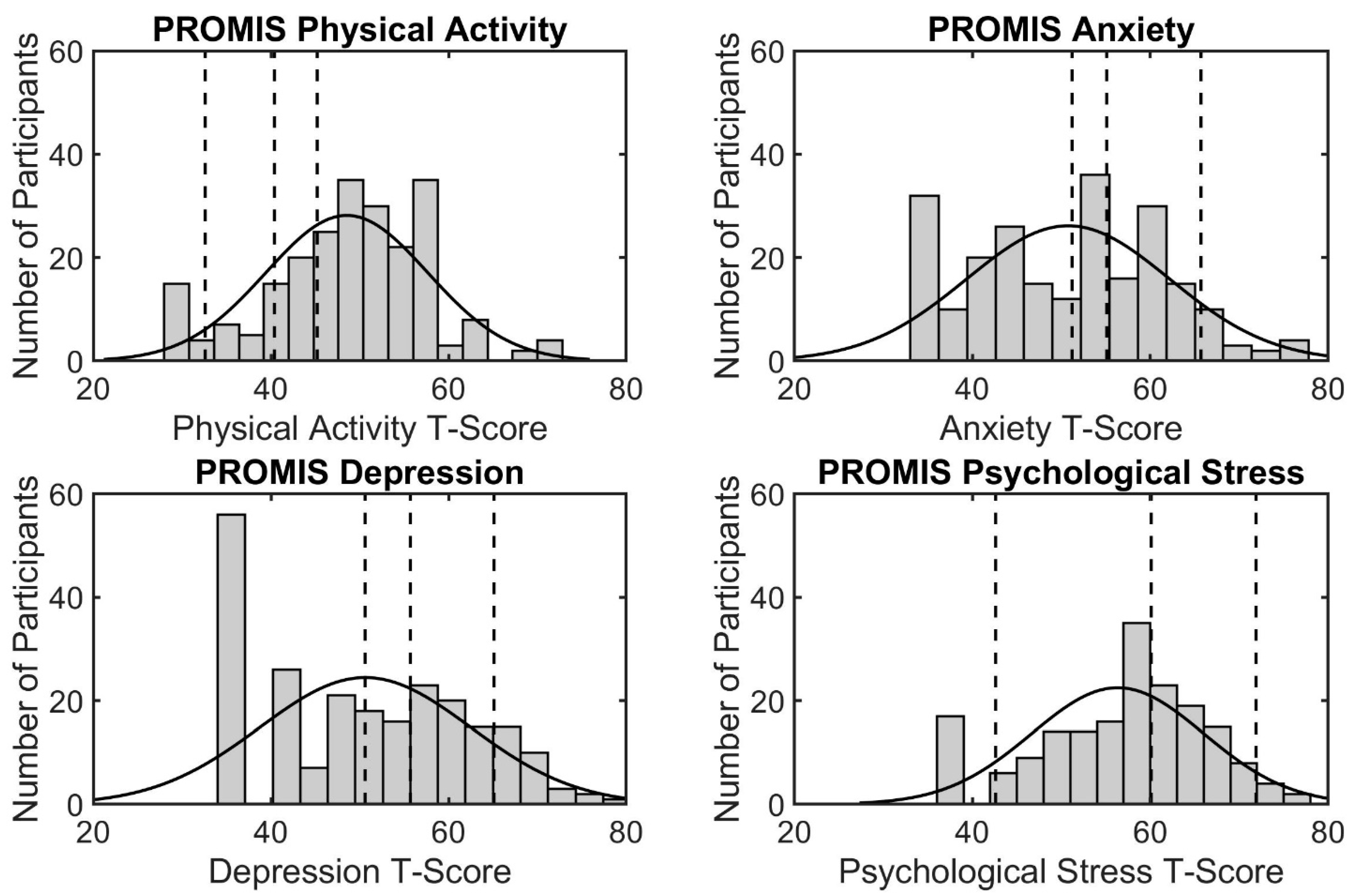
3.1. Mental and Physical Health Characteristics
3.2. Relationships between Mental and Physical Health
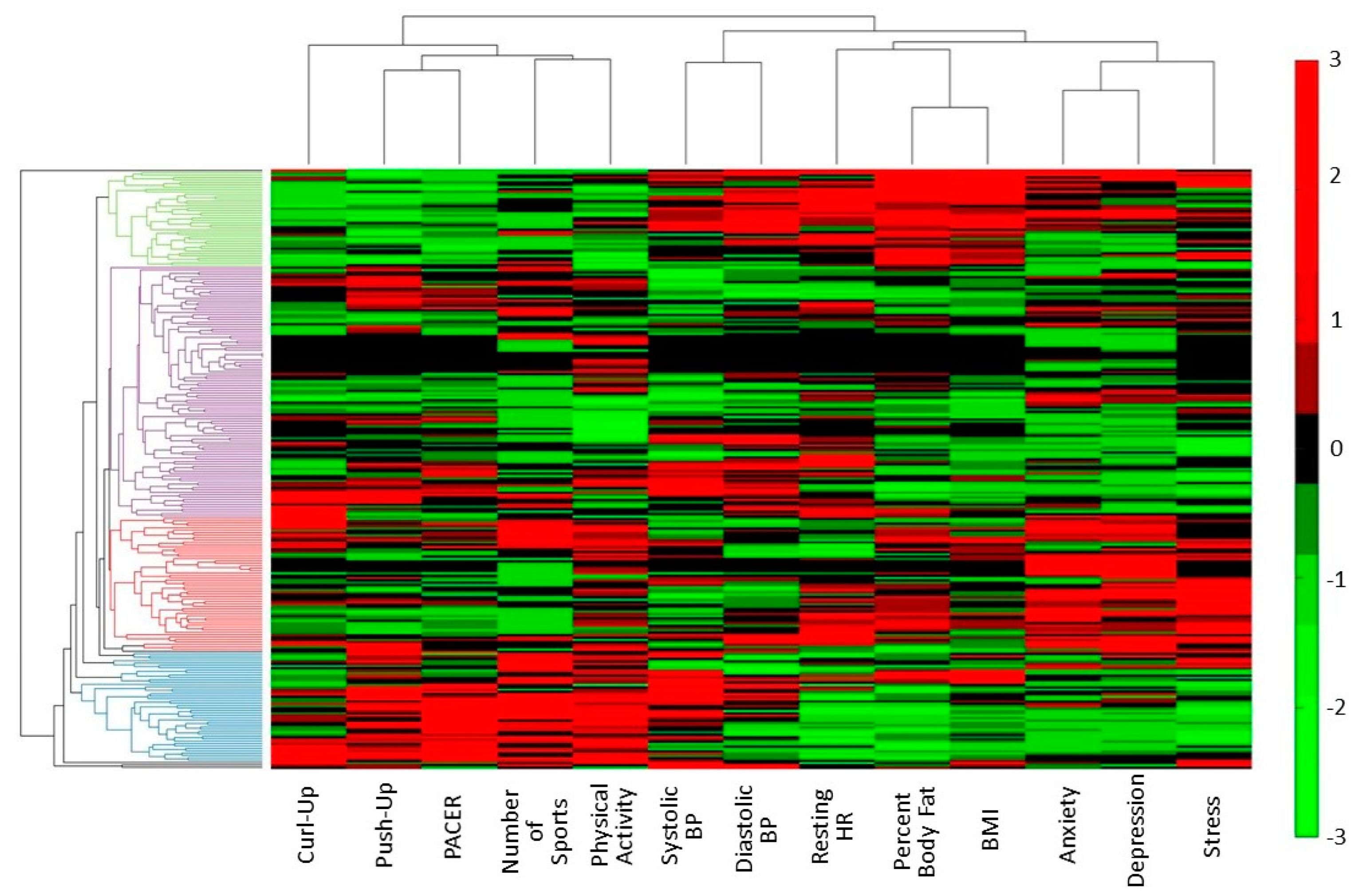
3.3. Data Driven Classification of Variable Clusters
3.4. Data Driven Classification of Participant Clusters
4. Discussion
4.1. Prevalence of Physical and Mental Health Issues
4.2. Relationships between Mental and Physical Health
4.3. Limitations and Future Research
4.4. Implications for Policy, Theory, and Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Das, J.K.; Salam, R.A.; Lassi, Z.S.; Naveed Khan, M.; Mahmood, W.; Patel, V.; Bhutta, A.Z. Interventions for Adolescent Mental Health: An Overview of Systematic Reviews. J. Adolesc. Health 2016, 59, S49–S60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J.; et al. Youth risk behavior surveillance: United States, 2017. Morb. Mortal. Wkly. Rep. 2018, 67, 1–114. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Denstel, K.D.; Beals, K.; Bolling, C.; Wright, C.; Crouter, S.E.; McKenzie, T.L.; Pate, R.R.; Saelens, B.E.; Staiano, A.E.; et al. Results from the United States 2016 Report Card on Physical Activity for Children and Youth. J. Phys. Act. Health 2016, 13, S307–S313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Health Statistics. National Health and Nutrition Examination Survey; National Center for Health Statistics: Hyattsville, MD, USA, 2006.
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity among Adults and Youth: United States, 2015–2016; National Center for Health Statistics: Hyattsville, MD, USA, 2017.
- Federal Interagency Forum on Child and Family Statistics. America’s Children: Key National Indicators of Well-Being; Federal Interagency Forum on Child and Family Statistics: Washington, DC, USA, 2017.
- Merikangas, K.; He, J.-P.; Burstein, M.; Swanson, S.; Avenevoli, S.; Lihong, C.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime Prevalence of Mental Disorders in US Adolescents: Results from the National Comorbidity Study-Adolescent Supplement. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services; Substance Abuse and Mental Health Services Administration; Center for Behavioral Health Statistics and Quality. Results from the 2017 National Survey on Drug Use and Health: Detailed Tables; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2018.
- Mojtabai, R.; Olfson, M.; Han, B. National Trends in the Prevalence and Treatment of Depression in Adolescents and Young Adults. Pediatrics 2016, 138, e20161878. [Google Scholar] [CrossRef] [Green Version]
- Biddle, S.J.H.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [Green Version]
- Lubans, D.; Richards, J.; Hillman, C.; Faulkner, G.; Beauchamp, M.; Nilsson, M.; Kelly, P.; Smith, J.; Raine, L.; Biddle, S. Physical Activity for Cognitive and Mental Health in Youth: A Systematic Review of Mechanisms. Pediatrics 2016, 138, e20161642. [Google Scholar] [CrossRef] [Green Version]
- Biddle, S.J.H.; Ciaccioni, S.; Thomas, G.; Vergeer, I. Physical activity and mental health in children and adolescents: An updated review of reviews and an analysis of causality. Psychol. Sport Exerc. 2019, 42, 146–155. [Google Scholar] [CrossRef]
- Mcdowell, C.P.; Macdonncha, C.; Herring, M.P. Brief report: Associations of physical activity with anxiety and depression symptoms and status among adolescents. J. Adolesc. 2017, 55, 1–4. [Google Scholar] [CrossRef]
- McMahon, E.M.; Corcoran, P.; O’Regan, G.; Keeley, H.; Cannon, M.; Carli, V.; Wasserman, C.; Hadlaczky, G.; Sarchiapone, M.; Apter, A.; et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur. Child Adolesc. Psychiatry 2017, 26, 111–122. [Google Scholar] [CrossRef]
- Fløtnes, I.S.; Nilsen, T.I.L.; Augestad, L.B. Norwegian adolescents, physical activity and mental health: The Young-HUNT study. Nor. Epidemiol. 2011, 20, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Boone, E.M.; Leadbeater, B.J. Game on: Diminishing risks for depressive symptoms in early adolescence through positive involvement in team sports. J. Res. Adolesc. 2006, 16, 79–90. [Google Scholar] [CrossRef]
- Weiss, M.R.; Kipp, L.E.; Bolter, N.D. Training for life: Optimizing positive youth development through sport and physical activity. In The Oxford Handbook of Sport and Performance Psychology; Murphy, S., Ed.; Oxford University Press: Oxford, UK, 2012; pp. 448–475. [Google Scholar]
- Johnson, J.A.; Johnson, A.M. Urban-rural differences in childhood and adolescent obesity in the United States: A systematic review and meta-analysis. Child. Obes. 2015, 11, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Hanson, M.D.; Chen, E. Socioeconomic status and health behaviors in adolescence: A review of the literature. J. Behav. Med. 2007, 30, 263–285. [Google Scholar] [CrossRef] [PubMed]
- Collins, P. Black Feminist Thought: Knowledge Consciousness, and the Politics of Empowerment, 2nd ed.; Routledge: New York, NY, USA, 1990. [Google Scholar]
- Crenshaw, K. Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine, Feminist Theory and Antiracist Politics. Univ. Chicago Leg. Forum 1989, 1989, 8. [Google Scholar]
- Trygg, N.F.; Gustafsson, P.E.; Månsdotter, A. Languishing in the crossroad? A scoping review of intersectional inequalities in mental health. Int. J. Equity Health 2019, 18, 115. [Google Scholar] [CrossRef] [Green Version]
- Reiss, F. Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Soc. Sci. Med. 2013, 90, 24–31. [Google Scholar] [CrossRef]
- Priester, M.A.; Browne, T.; Iachini, A.; Clone, S.; DeHart, D.; Seay, K.D. Treatment Access Barriers and Disparities Among Individuals with Co-Occurring Mental Health and Substance Use Disorders: An Integrative Literature Review. J. Subst. Abuse Treat. 2016, 61, 47–59. [Google Scholar] [CrossRef] [Green Version]
- Douthit, N.; Kiv, S.; Dwolatzky, T.; Biswas, S. Exposing some important barriers to health care access in the rural USA. Public Health 2015, 129, 611–620. [Google Scholar] [CrossRef]
- Waldorf, B.; Kim, A. The Index of Relative Rurality (IRR): US County Data for 2000 and 2010. Purdue Univ. Res. Repos. 2018. [Google Scholar] [CrossRef]
- U.S. Census Bureau. 2019: ACS 5-Year Estimates Data Profiles; U.S. Census Bureau: Suitland, MD, USA, 2019.
- Cella, D.; Yount, S.; Rothrock, N.; Gershon, R.; Cook, K.; Reeve, B.; Ader, D.; Fries, J.F.; Bruce, B.; Rose, M.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS): Progress of an NIH Roadmap Cooperative Group during its First Two Years. Med. Care 2010, 45, S3–S11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, C.A.; Bevans, K.B.; Teneralli, R.E.; Smith, A.W.; Bowles, H.R.; Forrest, C.B. Self-Reported Pediatric Measures of Physical Activity, Sedentary Behavior and Strength Impact for PROMIS®: Conceptual Framework. Pediatr. Phys. Ther. 2014, 26, 376–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, C.A.; Bevans, K.B.; Teneralli, R.E.; Smith, A.W.; Bowles, H.R.; Forrest, C.B. Self-Reported Pediatric Measures of Physical Activity, Sedentary Behavior and Strength Impact for PROMIS®: Item Development. Pediatr. Phys. Ther. 2014, 26, 385–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forrest, C.B.; Bevans, K.B.; Tucker, C.; Riley, A.W.; Ravens-Sieberer, U.; Gardner, W.; Pajer, K. Commentary: The Patient-Reported Outcome Measurement Information System (PROMIS®) for Children and Youth: Application to Pediatric Psychology. J. Pediatr. Psychol. 2012, 37, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Irwin, D.E.; Stucky, B.; Langer, M.M.; Thissen, D.; DeWitt, E.M.; Lai, J.; Varni, J.W.; Yeatts, K.; Dewalt, D.A. An item response analysis of the pediatric PROMIS anxiety and depressive symptoms scales. Qual. Life Res. 2010, 19, 595–607. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Mental Health (NIMH). Child and Adolescent Mental Health. Available online: https://www.nimh.nih.gov/health/topics/child-and-adolescent-mental-health/index.shtml (accessed on 12 February 2019).
- Bevans, K.B.; Gardner, W.; Pajer, K.A.; Becker, B.; Carle, A.; Tucker, C.A.; Forrest, C.B. Psychometric Evaluation of the PROMIS® Pediatric Psychological and Physical Stress Experiences Measures. J. Pediatr. Psychol. 2018, 43, 678–692. [Google Scholar] [CrossRef] [Green Version]
- Bevans, K.B.; Gardner, W.; Pajer, K.; Riley, A.W.; Forrest, C.B. Qualitative development of the PROMIS® pediatric stress response item banks. J. Pediatr. Psychol. 2013, 38, 173–191. [Google Scholar] [CrossRef] [Green Version]
- Pingitore, R.; Spring, B.; Garfield, D. Gender differences in body satisfaction. Obes. Res. 1997, 5, 402–409. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Wall, M.M.; Larson, N.; Story, M.; Fulkerson, J.A.; Eisenberg, M.E.; Hannan, P.J. Secular trends in weight status and weight-related attitudes and behaviors in adolescents from 1999 to 2010. Prev. Med. (Baltim.) 2012, 54, 77–81. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, M. Society and the Adolescent Self Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Van Den Berg, P.A.; Mond, J.; Eisenberg, M.; Ackard, D.; Neumark-Sztainer, D. The link between body dissatisfaction and self-esteem in adolescents: Similarities across gender, age, weight status, race/ethnicity, and socioeconomic status. J. Adolesc. Health 2010, 47, 290–296. [Google Scholar] [CrossRef] [Green Version]
- Cella, D.; Riley, W.; Stone, A.; Rothrock, N.; Reeve, B.; Yount, S.; Amtmann, D.; Bode, R.; Buysse, D.; Choi, S.; et al. Initial Adult Health Item Banks and First Wave Testing of the Patient Reported Outcomes Measurement Information System (PROMIS) Network: 2005–2008. J. Clin. Epidemiol. 2010, 63, 1179–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothrock, N.; Hays, R.; Spritzer, K.; Yount, S.; Riley, W.; Cella, D. Relative to the general US population, chronic diseases are associated with poorer health-related quality of life as measured by the Patient-Reported Outcomes Measurement Information System (PROMIS). J. Clin. Epidemiol. 2010, 63, 1195–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Child and Adolescent Health Measurement Initiative; Data Resource Center for Child and Adolescent Health. 2016 National Survey of Children’s Health (NSCH) Data Query; Child and Adolescent Health Measurement Initiative: Baltimore, MD, USA, 2017. [Google Scholar]
- Center for Disease Control. Youth Risk Behavior Survey Data Summary & Trends Report 2007–2017; CDC: Atlanta, GA, USA, 2017.
- Duncan, S.C.; Duncan, T.E.; Strycker, L.A.; Chaumeton, N.R. Relations between youth antisocial and prosocial activities. J. Behav. Med. 2002, 25, 425–438. [Google Scholar] [CrossRef] [PubMed]
- Melnyk, B.M.; Jacobson, D.; Kelly, S.; Belyea, M.; Shaibi, G.; Small, L.; O’Haver, J.; Marsiglia, F.F. Promoting Healthy Lifestyles in High School Adolescents: A Randomized Controlled Trial. Am. J. Prev. Med. 2013, 45, 407–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annesi, J.J.; Trinity, J.; Mareno, N.; Walsh, S.M. Association of a behaviorally based high school health education curriculum with increased exercise. J. Sch. Nurs. 2015, 31, 196–204. [Google Scholar] [CrossRef]
- Feiss, R.; Beth, S.; Monaye, D.; Elaine, M.; Karley, R.; Julio, M.; Thomas, C.M.; Pangelinan, M. A Systematic Review and Meta-Analysis of School-Based Stress, Anxiety, and Depression Prevention Programs for Adolescents. J. Youth Adolesc. 2019, 48, 1668–1685. [Google Scholar] [CrossRef]
- Griner, D.; Smith, T.B. Culturally adapted mental health interventions: A meta-analytic review. Psychother. Theory Res. Pract. Train. 2006, 43, 531–548. [Google Scholar] [CrossRef] [Green Version]
- Planey, A.M.; Smith, S.M.N.; Moore, S.; Walker, T.D. Barriers and facilitators to mental health help-seeking among African American youth and their families: A systematic review study. Child. Youth Serv. Rev. 2019, 101, 190–200. [Google Scholar] [CrossRef]
- Mellor, C. School-based interventions targeting stigma of mental illness: Systematic review. Psychiatr. Bull. 2014, 38, 164–171. [Google Scholar] [CrossRef]
- Mukolo, A.; Heflinger, C.A. Rurality and African American Perspectives on Children’s Mental Health Services. J. Emot. Behav. Disord. 2011, 19, 83–97. [Google Scholar] [CrossRef]
- Thomas, J.; Thirlaway, K.; Bowes, N.; Meyers, R. Effects of combining physical activity with psychotherapy on mental health and well-being: A systematic review. J. Affect. Disord. 2020, 265, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Ray, R. An Intersectional Analysis to Explaining a Lack of Physical Activity Among Middle Class Black Women. Sociol. Compass 2014, 6, 780–791. [Google Scholar] [CrossRef]
- López, N.; Vargas, E.; Juarez, M.; Cacari-stone, L.; Bettez, S. What’s Your “Street Race”? Leveraging Multidimensional Measures of Race and Intersectionality for Examining Physical and Mental Health Status among Latinxs. Sociol. Race Ethn. 2018, 4, 49–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, C.R. Adding interactions to models of intersectional health inequalities: Comparing multilevel and conventional methods. Soc. Sci. Med. 2019, 221, 95–105. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Variables | Number of Participants (%), N = 253 |
|---|---|
| Sex | |
| Male | 114 (45.1%) |
| Female | 139 (54.9%) |
| Age | |
| 15 | 151 (59.7%) |
| 16 | 80 (31.6%) |
| 17 | 15 (5.9%) |
| 186 | 1 (0.4%) |
| Not Reported | 6 (2.4%) |
| Ethnicity | |
| Caucasian/White | 105 (41.5%) |
| African American/Black | 114 (45.1%) |
| Hispanic/Latino | 4 (1.6%) |
| Asian/Pacific Islander | 2 (0.8%) |
| Native American | 1 (0.4%) |
| Mixed Race | 11 (4.3%) |
| Not Reported | 16 (6.3%) |
| Household Income | |
| USD <30,000 | 109 (43.1%) |
| USD 30,000–49,999 | 40 (15.8%) |
| USD 50,000–99,999 | 53 (20.9%) |
| USD 100,000+ | 20 (7.9%) |
| Not Reported | 31 (12.3%) |
| Parental Education | |
| Did Not Finish HS | 39 (15.4%) |
| HS Diploma/GED 1 | 74 (29.2%) |
| Some College | 44 (17.4%) |
| Trade, Technical, or Vocational Training | 11 (4.3%) |
| Associate degree | 26 (10.3%) |
| Bachelor’s Degree | 26 (10.3%) |
| Master’s Degree | 10 (4.0%) |
| Professional Degree | 4 (1.6%) |
| Doctoral Degree | 0 (0.0%) |
| Multiple Degrees Selected | 4 (1.6%) |
| Not Reported | 15 (5.9%) |
| Questionnaire | Normal | Mild | Moderate | Severe |
|---|---|---|---|---|
| PROMIS Physical Activity | 164 (64.8%) | 32 (12.6%) | 19 (7.5%) | 15 (5.9%) |
| PROMIS Anxiety | 110 (43.5%) | 32 (12.6%) | 70 (27.7%) | 22 (8.7%) |
| PROMIS Depression | 110 (43.5%) | 34 (13.4%) | 58 (22.9%) | 33 (13.0%) |
| Low | Average | High | Very High | |
| PROMIS Psychological Stress | 17 (6.7%) | 94 (37.2%) | 60 (23.7%) | 11 (4.3%) |
| Test | Underweight | Normal | Overweight | Obese |
|---|---|---|---|---|
| Obesity (by BMI) | 4 (1.6%) | 120 (47.4%) | 40 (15.8%) | 59 (23.3%) |
| Very Lean | HFZ | NI | NI–HR 1 | |
| FITNESSGRAM—Body Fat | 6 (2.4%) | 121 (47.8%) | 51 (20.2%) | 44 (17.4%) |
| HFZ | NI | NI–HR 1 | ||
| FITNESSGRAM—PACER 2 | 20 (7.9%) | 39 (15.4%) | 160 (63.2%) | |
| HFZ | NI | |||
| FITNESSGRAM—Push-Up | 125 (49.4%) | 98 (38.7%) | ||
| FITNESSGRAM—Curl-Up | 126 (49.8%) | 98 (38.7%) |
| Body Fat % | BMI | Physical Activity | Anxiety | Depressive Symptoms | Psychological Stress | Body Satisfaction | Self-Esteem | |
|---|---|---|---|---|---|---|---|---|
| Body Fat % | 1 | |||||||
| BMI | 0.899 *** | 1 | ||||||
| Physical Activity | −0.031 | 0.103 | 1 | |||||
| Anxiety | 0.217 * | 0.257 * | 0.013 | 1 | ||||
| Depressive Symptoms | 0.149 | 0.217 * | 0.103 | 0.640 *** | 1 | |||
| Psychological Stress | 0.232 * | 0.223 * | −0.013 | 0.441 *** | 0.555 *** | 1 | ||
| Body Satisfaction | −0.258 | −0.305 * | −0.100 | −0.122 | −0.307 * | −0.065 | 1 | |
| Self-Esteem | −0.206 | −0.236 | 0.110 | −0.441 ** | −0.490 ** | −0.392 ** | 0.360 * | 1 |
| Body Fat % | BMI | Physical Activity | Anxiety | Depressive Symptoms | Psychological Stress | Body Satisfaction | Self-Esteem | |
|---|---|---|---|---|---|---|---|---|
| Body Fat % | 1 | |||||||
| BMI | 0.928 *** | 1 | ||||||
| Physical Activity | −0.140 | −0.121 | 1 | |||||
| Anxiety | 0.188 * | 0.209 * | 0.178 * | 1 | ||||
| Depressive Symptoms | 0.148 | 0.181 * | 0.243 ** | 0711 *** | 1 | |||
| Psychological Stress | 0.163 | 0.154 | 0.178 | 0.526 *** | 0.566 *** | 1 | ||
| Body Satisfaction | −0.445 * | −0.456 * | 0.166 | −0.440 * | −0.407 * | 0.018 | 1 | |
| Self-Esteem | −0.182 | −0.320* | −0.112 | −0.436 ** | −0.709 *** | −0.635 ** | 0.491 * | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feiss, R.; Pangelinan, M.M. Relationships between Physical and Mental Health in Adolescents from Low-Income, Rural Communities: Univariate and Multivariate Analyses. Int. J. Environ. Res. Public Health 2021, 18, 1372. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041372
Feiss R, Pangelinan MM. Relationships between Physical and Mental Health in Adolescents from Low-Income, Rural Communities: Univariate and Multivariate Analyses. International Journal of Environmental Research and Public Health. 2021; 18(4):1372. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041372
Chicago/Turabian StyleFeiss, Robyn, and Melissa M. Pangelinan. 2021. "Relationships between Physical and Mental Health in Adolescents from Low-Income, Rural Communities: Univariate and Multivariate Analyses" International Journal of Environmental Research and Public Health 18, no. 4: 1372. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041372