
The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question (PICO)
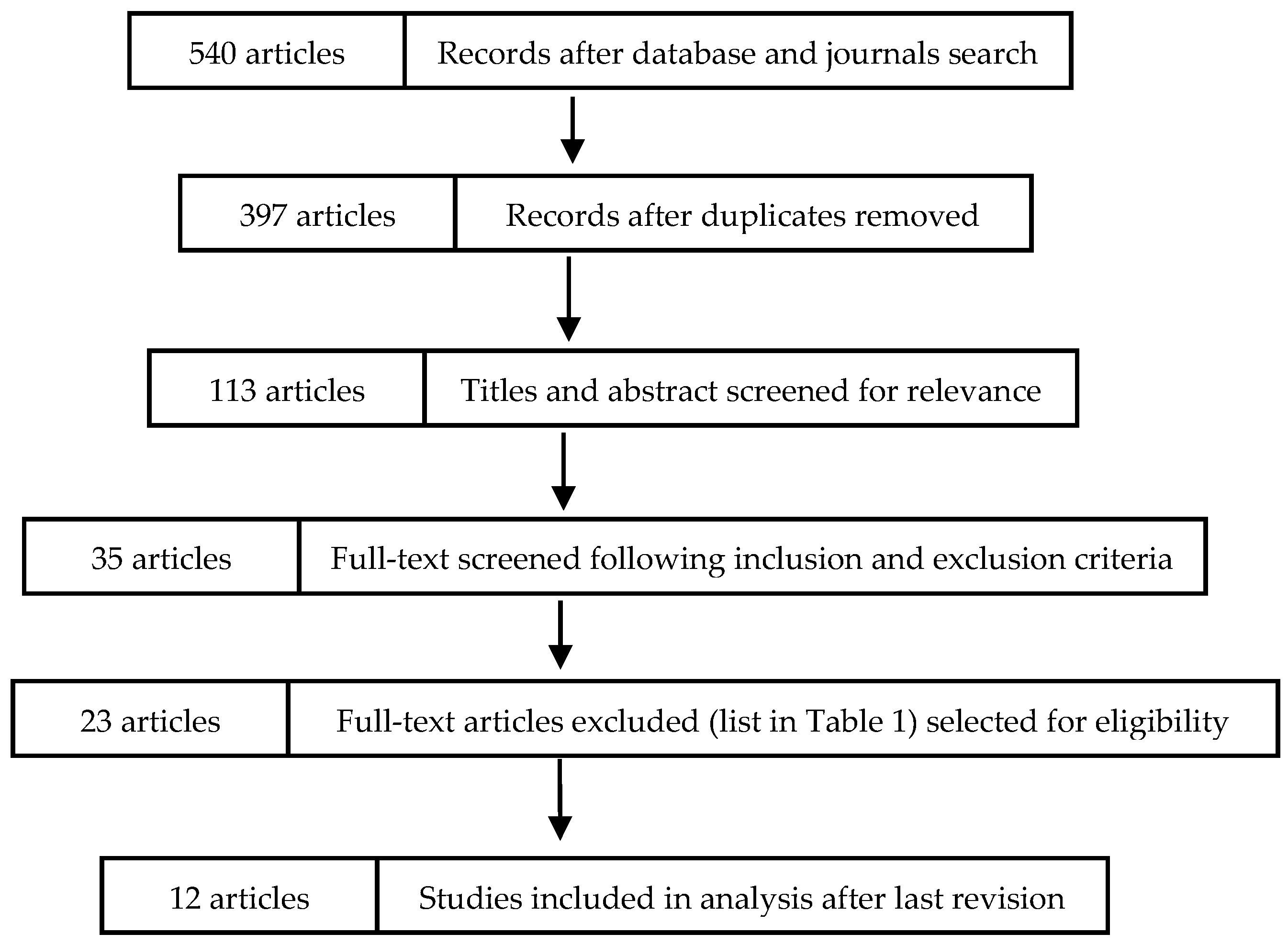
2.2. Study Selection and Eligibility Criteria
2.3. Search Strategy
2.4. Screening and Selection of Papers
2.5. Risk of Bias in Individual Studies
2.6. Data Analysis and Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ORHs | Rotating-Oscillating Heads |
| SAHs | Sonic Action Heads |
| WMD | Weighted Mean Differences |
| CI | Confidence Intervals |
| RCTs | Randomised Clinical Trials |
| GI | Gingival Index |
| PI | Plaque Index |
| BoP | Bleeding on Probing |
References
- Axelsson, P.; Nyström, B.; Lindhe, J. The long-term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults. J. Clin. Periodontol. 2004, 31, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Haffajee, A.D.; Thompson, M.; Torresyap, G.; Guerrero, D.; Socransky, S.S. Efficacy of manual and powered toothbrushes (I). Effect on clinical parameters. J. Clin. Periodontol. 2001, 28, 937–946. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Van der Weijden, F.; Doerfer, C.; Herrera, D.; Shapira, L.; Polak, D.; Madianos, P.; Louropoulou, A.; Machtei, E.; Donos, N.; et al. Primary prevention of periodontitis, Managing gingivitis. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S71–S76. [Google Scholar] [CrossRef]
- Marsh, P.D. Contemporary perspective on plaque control. Br. Dent. J. 2012, 212, 601–606. [Google Scholar] [CrossRef]
- Sambunjak, D.; Nickerson, J.W.; Poklepovic, T.; Johnson, T.M.; Imai, P.; Tugwell, P.; Worthington, H.V. Flossing for the management of periodontal diseases and dental caries in adults. Cochrane Database Syst. Rev. 2011, 12. [Google Scholar] [CrossRef] [PubMed]
- Delaurenti, M.; Ward, M.; Souza, S.; Jenkins, W.; Putt, M.S.; Milleman, K.R.; Milleman, J.L. The Effect of Use of a Sonic Power Toothbrush and a Manual Toothbrush Control on Plaque and Gingivitis. J. Clin. Dent. 2017, 28, A1–A6. [Google Scholar] [PubMed]
- Ayad, F.; Petrone, D.M.; Wachs, G.N.; Mateo, L.R.; Chaknis, P.; Panagakos, F. Comparative efficacy of a specially engineered sonic powered toothbrush with unique sensing and control technologies to two commercially available power toothbrushes on established plaque and gingivitis. J. Clin. Dent. 2012, 23, A5–A10. [Google Scholar]
- Robinson, P.G.; Deacon, S.A.; Deery, C.; Heanue, M.; Walmsley, A.D.; Worthington, H.V.; Glenny, A.M.; Shaw, W.C. Manual versus powered toothbrushing for oral health. Cochrane Database Syst. Rev. 2005, 18, 2. [Google Scholar]
- Heanue, M.; Deacon, S.A.; Deery, C.; Robinson, P.G.; Walmsley, A.D. Worthington HV, Shaw WC. Manual versus powered toothbrushing for oral health. Cochrane Database Syst. Rev. 2003, 1, CD002281, Update in, Cochrane Database Syst Rev. 2005, 2, CD002281. [Google Scholar] [CrossRef]
- Deery, C.; Heanue, M.; Deacon, S.; Robinson, P.G.; Walmsley, A.D.; Worthington, H.; Shaw, W.; Glenny, A.M. The effectiveness of manual versus powered toothbrushes for dental health. A systematic review. J. Dent. 2004, 32, 197–211. [Google Scholar] [CrossRef]
- Cosola, S.; Marconcini, S.; Boccuzzi, M.; Menchini Fabris, G.B.; Covani, U.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. Radiological Outcomes of Bone-Level and Tissue-Level Dental Implants, Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6920. [Google Scholar] [CrossRef]
- Sicilia, A.; Arregui, I.; Gallego, M.; Cabezas, B.; Cuesta, S. A systematic review of powered vs manual toothbrushes in periodontal cause-related therapy. J. Clin. Periodontol. 2002, 29 (Suppl. 33), 9–54. [Google Scholar] [CrossRef]
- Grender, J.; Williams, K.; Walters, P.; Klukowska, M.; Reick, H. Plaque removal efficacy of oscillating-rotating power toothbrushes, Review of six comparative clinical trials. Am. J. Dent. 2013, 26, 68–74. [Google Scholar]
- Yaacob, M.; Worthington, H.V.; Deacon, S.A.; Deery, C.; Walmsley, A.D.; Robinson, P.G.; Glenny, A.M. Powered versus manual toothbrushing for oral health (Review). Cochrane Database Syst. Rev. 2014, 6. [Google Scholar] [CrossRef]
- De Jager, M.; Rmaile, A.; Darch, O.; Bikker, J.W. The Effectiveness of Manual versus High-Frequency, High-Amplitude Sonic Powered Toothbrushes for Oral Health, A Meta-Analysis. J. Clin. Dent. 2017, 28, A13–A28. [Google Scholar]
- Brothwell, D.J.; Jutai, D.K.; Hawkins, R.J. An update of mechanical oral hygiene practices, Evidence-based recommendations for disease prevention. J. Can. Dent. Assoc. 1998, 64, 295–306. [Google Scholar] [PubMed]
- Deacon, S.A.; Glenny, A.M.; Deery, C.; Robinson, P.G.; Heanue, M.; Walmsley, A.D.; Shaw, W.C. Different powered toothbrushes for plaque control and gingival health. Cochrane Database Syst. Rev. 2010, 8, 12. [Google Scholar]
- Bader, H.I.; Boyd, R.L. Comparative efficacy of a rotary and a sonic powered toothbrush on improving gingival health in treated adult periodontitis patients. Am. J. Dent. 1999, 12, 143–147. [Google Scholar]
- Biesbrock, A.R.; Bartizek, R.D.; Gerlach, R.W.; Terézhalmy, G.T. Oral hygiene regimens, plaque control, and gingival health, A two-month clinical trial with antimicrobial agents. J. Clin. Dent. 2007, 18, 101–105. [Google Scholar]
- Biesbrock, A.R.; He, T.; Walters, P.A.; Bartizek, R.D. Clinical evaluation of the effects of a sonic toothbrush with ultrasound waveguide in disrupting plaque with and without bristle contact. Am. J. Dent. 2008, 21, 83–87. [Google Scholar] [PubMed]
- Biesbrock, A.R.; Walters, P.A.; Bartizek, R.D.; Goyal, C.R.; Qaqish, J.G. Plaque removal efficacy of an advanced rotation-oscillation power toothbrush versus a new sonic toothbrush. Am. J. Dent. 2008, 21, 185–188. [Google Scholar] [PubMed]
- Costa, M.R.; Silva, V.C.; Miqui, M.N.; Sakima, T.; Spolidorio, D.M.; Cirelli, J.A. Efficacy of ultrasonic, electric and manual toothbrushes in patients with fixed orthodontic appliances. Angle Orthod. 2007, 77, 361–366. [Google Scholar] [CrossRef]
- Goyal, C.R.; Qaqish, J.; He, T.; Grender, J.; Walters, P.; Biesbrock, A.R. A randomized 12-week study to compare the gingivitis and plaque reduction benefits of a rotation-oscillation power toothbrush and a sonic power toothbrush. J. Clin. Dent. 2009, 20, 93–98. [Google Scholar] [PubMed]
- Goyal, C.R.; Qaqish, J.G.; Sharma, N.C.; Warren, P.R.; Cugini, M.; Thompson, M.C. Plaque removal efficacy of a novel tooth wipe. J. Clin. Dent. 2005, 16, 44–46. [Google Scholar]
- Goyal, C.R.; Sharma, N.C.; Qaqish, J.G.; Cugini, M.A.; Thompson, M.C.; Warren, P.R. Efficacy of a novel brush head in the comparison of two power toothbrushes on removal of plaque and naturally occurring extrinsic stain. J. Dent. 2005, 33, 7–43. [Google Scholar] [CrossRef]
- Grossman, E.; Dembling, W.; Proskin, H.M. A comparative clinical investigation of the safety and efficacy of an oscillating/rotating electric toothbrush and a sonic toothbrush. J. Clin. Dent. 1995, 6, 108–112. [Google Scholar]
- Hanato, Y.; Kishimoto, T.; Ojima, M.; Matsuo, T.; Kanesaki, N.; Ryu, C.; Hanioka, T. Comparative study of plaque removal efficacy of twin-motor sonic toothbrush with floating bristles and conventional powered toothbrushes in posterior teeth. Am. J. Dent. 2005, 18, 237–240. [Google Scholar]
- Williams, K.; Haun, J.; Dockter, K.; Ferrante, A.; Bartizek, R.D.; Biesbrock, A.R. A plaque removal study comparing two advanced-design oscillating battery-powered toothbrushes. J. Clin. Dent. 2003, 14, 88–92. [Google Scholar]
- Hefti, A.F.; Stone, C. Power toothbrushes, gender, and dentin hypersensitivity. Clin. Oral Investig. 2000, 4, 91–97. [Google Scholar] [CrossRef]
- Klukowska, M.; Grender, J.M.; Goyal, C.R.; Qaqish, J.; Biesbrock, A.R. 8-week evaluation of anti-plaque and anti-gingivitis benefits of a unique multi-directional power toothbrush versus a sonic control toothbrush. Am. J. Dent. 2012, 25, 27A–32A. [Google Scholar]
- Klukowska, M.; Grender, J.M.; Conde, E.; Ccahuana-Vasquez, R.A.; Goyal, C.R. A randomized 12-week clinical comparison of an oscillating-rotating toothbrush to a new sonic brush in the reduction of gingivitis and plaque. J. Clin. Dent. 2014, 25, 26–31. [Google Scholar] [PubMed]
- Klukowska, M.; Grender, J.M.; Conde, E.; Goyal, C.R.; Qaqish, J. A six-week clinical evaluation of the plaque and gingivitis efficacy of an oscillating-rotating power toothbrush with a novel brush head utilizing angled CrissCross bristles versus a sonic toothbrush. J. Clin. Dent. 2014, 25, 6–12. [Google Scholar] [PubMed]
- Robinson, P.J.; Maddalozzo, D.; Breslin, S. A six-month clinical comparison of the efficacy of the Sonicare and the Braun Oral-B electric toothbrushes on improving periodontal health in adult periodontitis patients. J. Clin. Dent. 1997, 8, 4–9. [Google Scholar] [PubMed]
- Sharma, N.C.; Galustians, J.; Qaqish, J.; Cugini, M. A comparison of two electric toothbrushes with respect to plaque removal and subject preference. Am. J. Dent. 1998, 11, S29–S33. [Google Scholar] [PubMed]
- Sharma, N.C.; Lyle, D.M.; Qaqish, J.G.; Galustians, J. Evaluation of the plaque removal efficacy of three power toothbrushes. J. Int. Acad. Periodontol. 2006, 8, 83–88. [Google Scholar]
- Singh, G.; Mehta, D.S.; Chopra, S.; Khatri, M. Comparison of sonic and ionic toothbrush in reduction in plaque and gingivitis. J. Indian Soc. Periodontol. 2011, 15, 210–214. [Google Scholar] [CrossRef]
- Thienpont, V.; Dermaut, L.R.; Van Maele, G. Comparative study of 2 electric and 2 manual toothbrushes in patients with fixed orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 353–360. [Google Scholar] [CrossRef]
- Van der Weijden, G.A.; Timmerman, M.F.; Reijerse, E.; Snoek, C.M.; Van der Velden, U. Comparison of an oscillating/rotating electric toothbrush and a ‘sonic’ toothbrush in plaque-removing ability. A professional toothbrushing and supervised brushing study. J. Clin. Periodontol. 1996, 23, 407–411. [Google Scholar] [CrossRef]
- Williams, K.B.; Cobb, C.M.; Taylor, H.J.; Brown, A.R.; Bray, K.K. Effect of sonic and mechanical toothbrushes on subgingival microbial flora, A comparative in vivo scanning electron microscopy study of 8 subjects. Quintessence Int. 2001, 32, 147–154. [Google Scholar]
- Williams, K.; Rapley, K.; Huan, J.; Walters, P.; He, T.; Grender, J.; Biesbrock, A.R. A study comparing the plaque removal efficacy of an advanced rotation-oscillation power toothbrush to a new sonic toothbrush. J. Clin. Dent. 2008, 19, 154–158. [Google Scholar]
- Ccahuana-Vasquez, R.A.; Conde, E.; Grender, J.M.; Cunningham, P.; Qaqish, J.; Goyal, C.R. An Eight-Week Clinical Evaluation of an Oscillating-Rotating Power Toothbrush with a Brush Head Utilizing Angled Bristles Compared with a Sonic Toothbrush in the Reduction of Gingivitis and Plaque. J. Clin. Dent. 2015, 26, 80–85. [Google Scholar] [PubMed]
- Goyal, C.R.; Klukowska, M.; Grender, J.M.; Cunningham, P.; Qaqish, J. Evaluation of a new multi-directional power toothbrush versus a marketed sonic toothbrush on plaque and gingivitis efficacy. Am. J. Dent. 2012, 25, 21A–26A. [Google Scholar] [PubMed]
- Klukowska, M.; Grender, J.M.; Goyal, C.R.; Mandl, C.; Biesbrock, A.R. 12-week clinical evaluation of a rotation/oscillation power toothbrush versus a new sonic power toothbrush in reducing gingivitis and plaque. Am. J. Dent. 2012, 25, 287–292. [Google Scholar] [PubMed]
- Klukowska, M.; Grender, J.M.; Conde, E.; Goyal, C.R. A 12-week clinical comparison of an oscillating-rotating power brush versus a marketed sonic brush with self-adjusting technology in reducing plaque and gingivitis. J. Clin. Dent. 2013, 24, 55–61. [Google Scholar]
- Klukowska, M.; Grender, J.M.; Conde, E.; Ccahuana-Vasquez, R.A.; Ram Goyal, C. A randomized clinical trial evaluating gingivitis and plaque reduction of an oscillating-rotating power brush with a new brush head with angled bristles versus a marketed sonic brush with self-adjusting technology. Am. J. Dent. 2014, 27, 179–184. [Google Scholar]
- Patters, M.R.; Bland, P.S.; Shiloah, J.; Blankenship, J.A.; Scarbecz, M. Comparison of the Hydrabrush powered toothbrush with two commercially-available powered toothbrushes. J. Int. Acad. Periodontol. 2005, 7, 80–89. [Google Scholar]
- Ricci, M.; Marchisio, O.; Genovesi, A.M.; Gelpi, F.; Marconcini, S.; Barone, A.; Corega, C.; Bertossi, D.; Pardo, A.; Nocini, P.F.; et al. Comparison between oscillating-twisting rotating of brush head vs a characteristic sweeping bristles motion on reducing oral inflammation. Minerva Stomatol. 2014, 14. published online ahead of print. [Google Scholar]
- Schmalz, G.; Kiehl, K.; Schmickler, J.; Rinke, S.; Schmidt, J.; Krause, F.; Haak, R.; Ziebolz, D. No difference between manual and different power toothbrushes with and without specific instructions in young, oral healthy adults-results of a randomized clinical trial. Clin. Oral. Investig. 2018, 22, 1147–1155. [Google Scholar] [CrossRef]
- Schmickler, J.; Wurbs, S.; Wurbs, S.; Kramer, K.; Rinke, S.; Hornecker, E.; Mausberg, R.F.; Ziebolz, D. The influence of the utilization time of brush heads from different types of power toothbrushes on oral hygiene assessed over a 6-month observation period, A randomized clinical trial. Am. J. Dent. 2016, 29, 307–314. [Google Scholar]
- Starke, M.; Delaurenti, M.; Ward, M.; Souza, S.; Milleman, K.R.; Milleman, J.L. A Comparison of the Effect of Two Power Toothbrushes on the Gingival Health and Plaque Status of Subjects with Moderate Gingivitis. J. Clin. Dent. 2017, 28, A29–A35. [Google Scholar]
- Williams, K.; Rapley, K.; Haun, J.; Walters, P.; He, T.; Grender, J.; Biesbrock, A.R. Comparison of rotation/oscillation and sonic power toothbrushes on plaque and gingivitis for 10 weeks. Am. J. Dent. 2009, 22, 345–349. [Google Scholar] [PubMed]
- Zimmer, S.; Strauss, J.; Bizhang, M.; Krage, T.; Raab, W.H.; Barthel, C. Efficacy of the Cybersonic in comparison with the Braun 3D Excel and a manual toothbrush. J. Clin. Periodontol. 2005, 32, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane. Handbook for Systematic Reviews of Interventions; JohnWiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Van der Weijden, F.A.; Slot, D.E. Efficacy of homecare regimens for mechanical plaque removal in managing gingivitis—A meta review. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S77–S91. [Google Scholar] [CrossRef]
- Hansen, F.; Gjermo, P. The plaque-removal effect of four toothbrushing methods. Scand. J. Dent. Res. 1971, 79, 502–506. [Google Scholar] [PubMed]
- Newman, M.G.; Caton, J.G.; Gunsolley, J.C. The use of the evidence- based approach in a periodontal therapy contemporary science workshop. Ann. Periodontol. 2003, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nr. | References | Exclusion Motivation |
|---|---|---|
| 1 | Bader HI, Boyd RL. Comparative efficacy of a rotary and a sonic powered toothbrush on improving gingival health in treated adult periodontitis patients. Am J Dent. 1999 Jun;12(3):143-7. [18] | Year of publication |
| 2 | Biesbrock AR, Bartizek RD, Gerlach RW, Terézhalmy GT. Oral hygiene regimens, plaque control, and gingival health: a two-month clinical trial with antimicrobial agents. J Clin Dent. 2007;18(4):101-5. [19] | Short follow-up: single brushing |
| 3 | Biesbrock AR, He T, Walters PA, Bartizek RD. Clinical evaluation of the effects of a sonic toothbrush with ultrasound waveguide in disrupting plaque with and without bristle contact. Am J Dent. 2008 Apr;21(2):83-7. [20] | Comparison between the same sonic toothbrush with the power turned on vs turned off |
| 4 | Biesbrock AR, Walters PA, Bartizek RD, Goyal CR, Qaqish JG. Plaque removal efficacy of an advanced rotation-oscillation power toothbrush versus a new sonic toothbrush. Am J Dent. 2008 Jun;21(3):185-8. [21] | Short follow-up |
| 5 | Costa MR, Silva VC, Miqui MN, Sakima T, Spolidorio DM, Cirelli JA. Efficacy of ultrasonic, electric and manual toothbrushes in patients with fixed orthodontic appliances. Angle Orthod. 2007 Mar;77(2):361-6. doi: 10.2319/0003-3219(2007)077[0361:EOUEAM]2.0.CO [22]; 2. | Orthodontic patients aged between 12 and 18 years old |
| 6 | Goyal CR, Qaqish J, He T, Grender J, Walters P, Biesbrock AR. A randomized 12-week study to compare the gingivitis and plaque reduction benefits of a rotation-oscillation power toothbrush and a sonic power toothbrush. J Clin Dent. 2009;20(3):93-8. [23] | Data appeared to duplicate another study |
| 7 | Goyal CR, Qaqish JG, Sharma NC, Warren PR, Cugini M, Thompson MC. Plaque removal efficacy of a novel tooth wipe. J Clin Dent. 2005;16(2):44-6. [24] | Short follow-up: single brushing |
| 8 | Goyal CR, Sharma NC, Qaqish JG, Cugini MA, Thompson MC, Warren PR. Efficacy of a novel brush head in the comparison of two power toothbrushes on removal of plaque and naturally occurring extrinsic stain. J Dent. 2005 Jun;33S1:37-43. [25] | Not following all inclusion criteria because it is focused on dental stains and not on plaque or gingival inflammation |
| 9 | Grossman E, Dembling W, Proskin HM. A comparative clinical investigation of the safety and efficacy of an oscillating/rotating electric toothbrush and a sonic toothbrush. J Clin Dent. 1995;6(1):108-12. [26] | Year of publication |
| 10 | Hanato Y, Kishimoto T, Ojima M, Matsuo T, Kanesaki N, Ryu C, Hanioka T. Comparative study of plaque removal efficacy of twin-motor sonic toothbrush with floating bristles and conventional powered toothbrushes in posterior teeth. Am J Dent. 2005 Aug;18(4):237-40. [27] | Short follow-up: single brushing |
| 11 | Williams K, Haun J, Dockter K, Ferrante A, Bartizek RD, Biesbrock AR. A plaque removal study comparing two advanced-design oscillating battery-powered toothbrushes. J Clin Dent. 2003;14(4):88-92. [28] | Short follow-up: single brushing |
| 12 | Hefti AF, Stone C. Power toothbrushes, gender, and dentin hypersensitivity. Clin Oral Investig. 2000 Jun;4(2):91-7. doi: 10.1007/s007840050122. [29] | Not following all inclusion criteria because it is focused on hypersensitivity and not on plaque or gingival inflammation |
| 13 | Klukowska M, Grender JM, Goyal CR, Qaqish J, Biesbrock AR. 8-week evaluation of anti-plaque and anti-gingivitis benefits of a unique multi-directional power toothbrush versus a sonic control toothbrush. Am J Dent. 2012 Sep;25 Spec No A(A):27A-32A. [30] | First step, after 8 weeks evaluation included the same study of 12 weeks |
| 14 | Klukowska M, Grender JM, Conde E, Ccahuana-Vasquez RA, Goyal CR. A randomized 12-week clinical comparison of an oscillating-rotating toothbrush to a new sonic brush in the reduction of gingivitis and plaque. J Clin Dent. 2014;25(2):26-31. [31] | Data appeared to duplicate another study |
| 15 | Klukowska M, Grender JM, Conde E, Goyal CR, Qaqish J. A six-week clinical evaluation of the plaque and gingivitis efficacy of an oscillating-rotating power toothbrush with a novel brush head utilizing angled CrissCross bristles versus a sonic toothbrush. J Clin Dent. 2014;25(2):6-12. [32] | First step, after 6 weeks evaluation, included study of 12 weeks |
| 16 | Robinson PJ, Maddalozzo D, Breslin S. A six-month clinical comparison of the efficacy of the Sonicare and the Braun Oral-B electric toothbrushes on improving periodontal health in adult periodontitis patients. J Clin Dent. 1997;8(1 Spec No):4-9. [33] | Year of publication |
| 17 | Sharma NC, Galustians J, Qaqish J, Cugini M. A comparison of two electric toothbrushes with respect to plaque removal and subject preference. Am J Dent. 1998 Sep;11(Spec No):S29-33. [34] | Short follow-up |
| 18 | Sharma NC, Lyle DM, Qaqish JG, Galustians J. Evaluation of the plaque removal efficacy of three power toothbrushes. J Int Acad Periodontol. 2006 Jul;8(3):83-8. [35] | Short follow-up: single brushing |
| 19 | Singh G, Mehta DS, Chopra S, Khatri M. Comparison of sonic and ionic toothbrush in reduction in plaque and gingivitis. J Indian Soc Periodontol. 2011 Jul;15(3):210-4. doi: 10.4103/0972-124X.85662. [36] | It is focused on the comparison of sonic toothbrush with ionic toothbrush |
| 20 | Thienpont V, Dermaut LR, Van Maele G. Comparative study of 2 electric and 2 manual toothbrushes in patients with fixed orthodontic appliances. Am J Orthod Dentofacial Orthop. 2001 Oct;120(4):353-60. doi: 10.1067/mod.2001.116402. [37] | Orthodontic patients |
| 22 | Van der Weijden GA, Timmerman MF, Reijerse E, Snoek CM, Van der Velden U. Comparison of an oscillating/rotating electric toothbrush and a ‘sonic’ toothbrush in plaque-removing ability. A professional toothbrushing and supervised brushing study. J Clin Periodontol. 1996 Apr;23(4):407-11. doi: 10.1111/j.1600-051x.1996.tb00565.x. [38] | Short follow-up |
| 22 | Williams KB, Cobb CM, Taylor HJ, Brown AR, Bray KK. Effect of sonic and mechanical toothbrushes on subgingival microbial flora: a comparative in vivo scanning electron microscopy study of 8 subjects. Quintessence Int. 2001 Feb;32(2):147-54. [39] | Not following all inclusion criteria because it is focused on subgingival microbial and not on plaque or gingival inflammation |
| 23 | Williams K, Rapley K, Huan J, Walters P, He T, Grender J, Biesbrock AR. A study comparing the plaque removal efficacy of an advanced rotation-oscillation power toothbrush to a new sonic toothbrush. J Clin Dent. 2008;19(4):154-8. [40] | Short follow-up and not following all inclusion criteria |
| Nr. | References | Patients | Age Range of Patients | SAH | ORH | Plaque Index | Gingival Index | Follow-Up Period And Frequency Use |
|---|---|---|---|---|---|---|---|---|
| 1 | Ccahuana-Vasquez RA. [41] | 148 = 75 (OR) + 73 (SA) | >18 years old—43.9 (SD = 11.30) | Sonicare DiamondClean | Oral-B Professional Care 1000 | Rustogi Modified Navy Plaque Index (RMNPI) | Modified Gingival Index (MGI) Gingival Bleeding Index (GBI) | 8 weeks Twice/day |
| 2 | Goyal CR. [42] | 130 = 65 (OR) + 65 (SA) | >18 years old—42.1 (SD = 11.20) | Philips Sonicare Essence 5500 | Oral-B Professional Deep Sweep | Rustogi Modified Navy Plaque Index (RMNPI) | Modified Gingival Index (MGI) Gingival Bleeding Index (GBI) | 4 weeks Twice/day |
| 3 | Klukowska M. [43] | 130 = 65 (OR) + 65 (SA) | >18 years old—44.7 | Sonicare DiamondClean | Oral-B Triumph with SmartGuide | Rustogi Modified Navy Plaque Index (RMNPI) | Modified Gingival Index (MGI) Gingival Bleeding Index (GBI) | 12 weeks Twice/day |
| 4 | Klukowska M. [44] | 127 = 62 (OR) + 65 (SA) | >18 years old—36.2 (12.02) | Colgate ProClinical A1500 | Oral-B Triumph with SmartGuide | Rustogi Modified Navy Plaque Index (RMNPI) | Modified Gingival Index (MGI) Gingival Bleeding Index (GBI) | 12 weeks Twice/day |
| 5 | Klukowska M. [45] | 130 = 65 (OR) + 65 (SA) | >18 years old—36.2 (12.87) | Colgate ProClinical A1500 | Oral-B Pro 7000 SmartSeries with SmartGuide with Oral-B CrossAction brush head, D34/EB50 | Rustogi Modified Navy Plaque Index (RMNPI) | Modified Gingival Index (MGI) Gingival Bleeding Index (GBI) | 6 weeks Twice/day |
| 6 | Patters MR. [46] | 70 = 35 (OR) + 35 (SA) | >18 years old | Sonicare PLUS | Braun Oral-B 3D Excel, model D17525 | Plaque Index (PI) | Modified Gingival Index (MGI) | 12 weeks Twice/day |
| 7 | Ricci M. [47] | 30 = 15 (OR) + 15 (SA) | >18 years old—35.8 (10.02) | Philips Sonicare | Oral B power toothbrush | Plaque Index (PI) | Full Mouth Bleeding Score (FMBS) | 4 weeks Twice/day |
| 8 | Schmalz G. [48] | 25 = 12 (OR) + 13 (SA) | >18 years old—28.5 (10.2) | Philips Sonicare | Oral B ProfessionalCare 7000 | Quigley-Hein plaque index (QHI) | Gingival Index (GI) Papilla Bleeding Index (PBI), | 12 weeks Twice/day |
| 9 | Schmickler J. [49] | 284 = 142 (OR) + 142 (SA) | >18years old—65 | Differed types of oscillating/ rotating toothbrushes | Differed types of sonic action toothbrushes | Quigley-Hein plaque index (QHI), | Papilla Bleeding Index (PBI), and Gingival Index (GI) | 24 weeks Twice/day |
| 10 | Starke M. [50] | 179 = 90 (OR) + 89 (SA) | >18 years old—42.2 (12.2) | Philips Sonicare DiamondClean | Oral-B 7000 | Modified Plaque Index (MPI) | Gingival Bleeding Index (GBI) | 6 weeks Twice/day |
| 11 | Williams K. [51] | 80 = 40 (OR) + 40 (SA) | >18 years old—34.1 (12.3) | Sonicare FlexCare | Oral-B Triumph | Turesky Modification of the Quigley-Hein Plaque Index | Löe-Silness Gingivitis Index | 10 weeks Twice/day |
| 12 | Zimmer S. [52] | 100 = 50 (OR)+ 50 (SA) | 18 > years old < 30 | Philips SoniCare | Oral-B® Professional Care 7000 | Turesky Modification of the Quigley-Hein Plaque Index | Gingival Index (GI) Loë-Silness Papillary Bleeding Index | 12 weeks Twice/day |
| Nr. | References | Better Clinical Results in: | Significance (p < 0.05) | Conclusion |
|---|---|---|---|---|
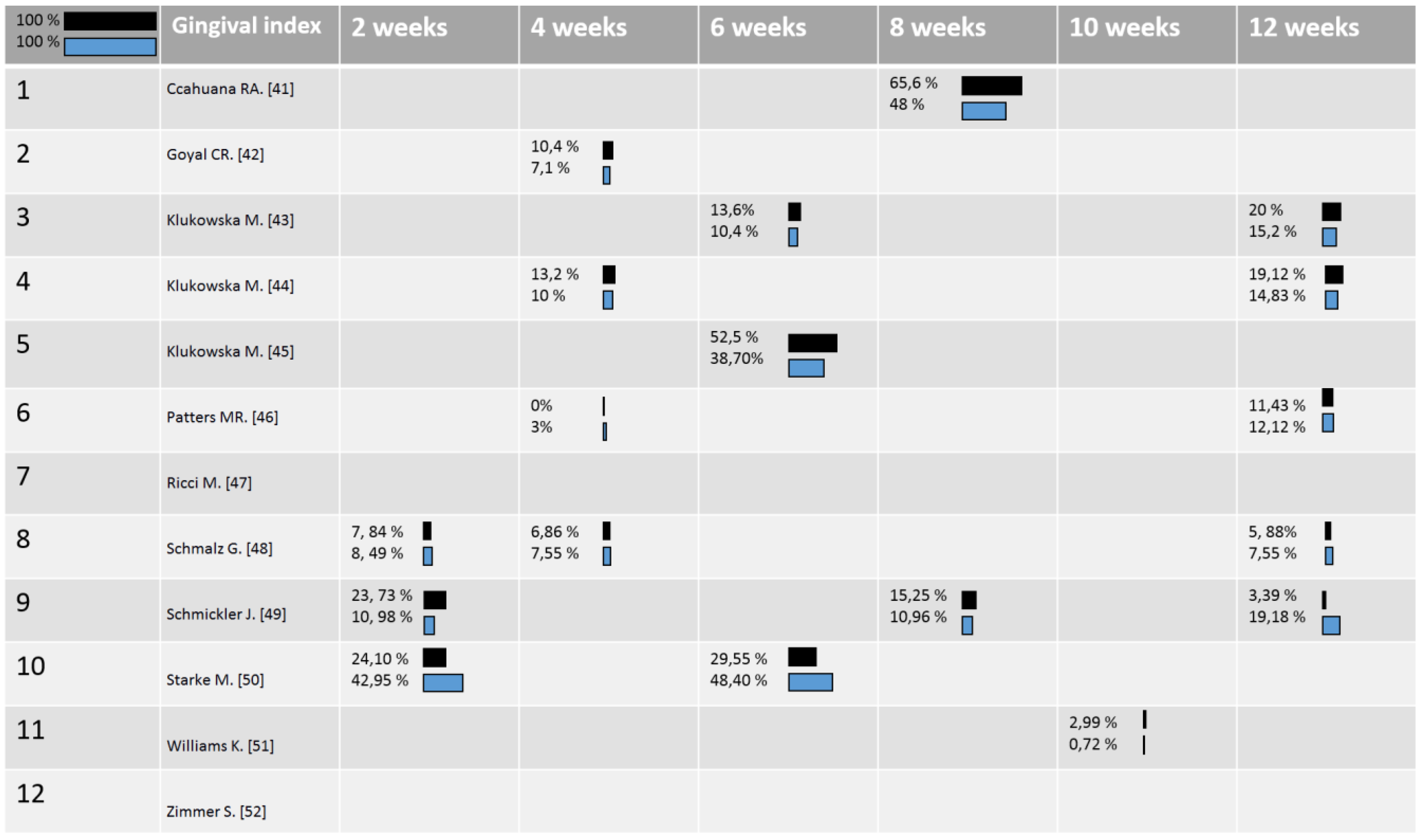
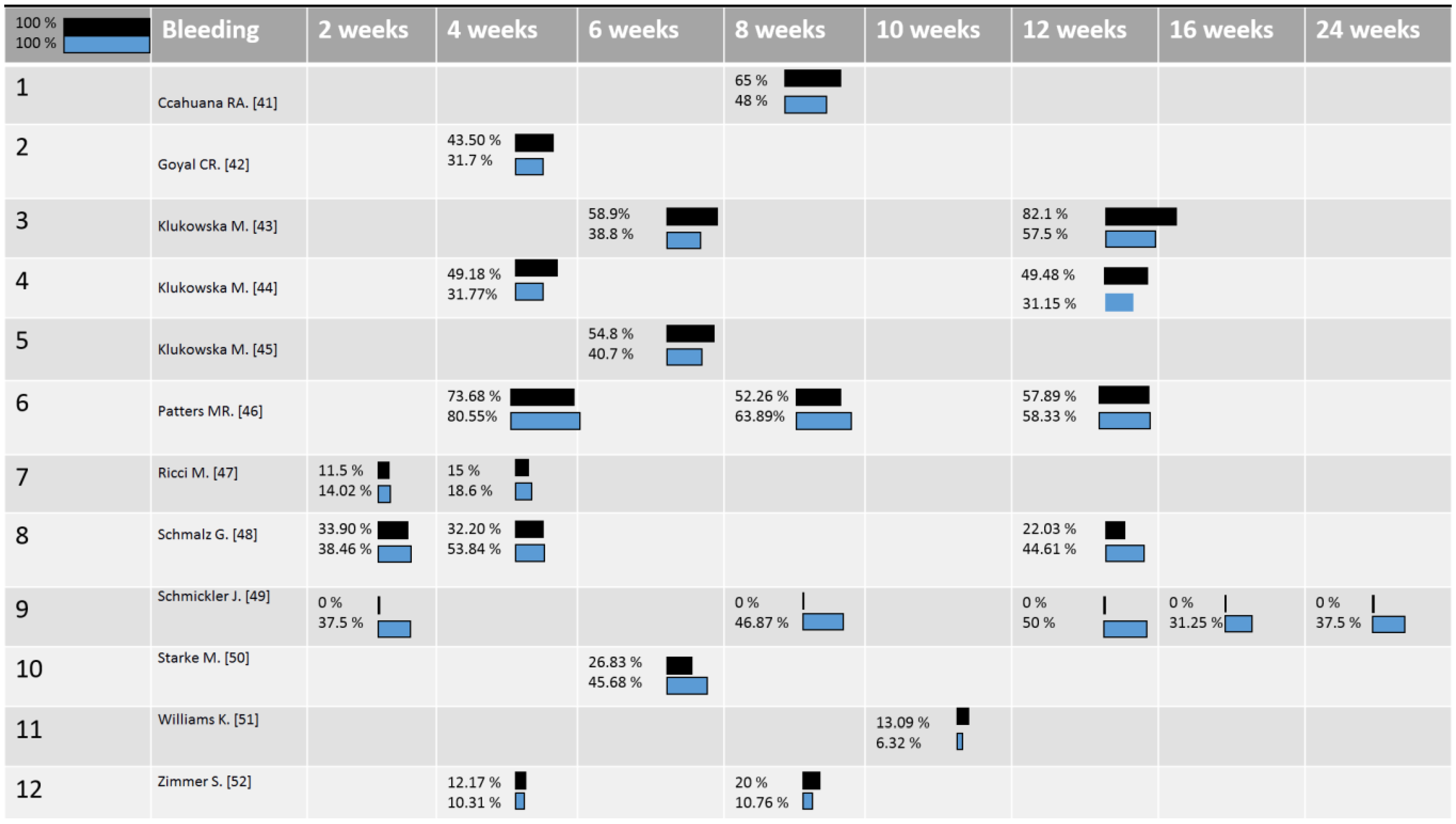
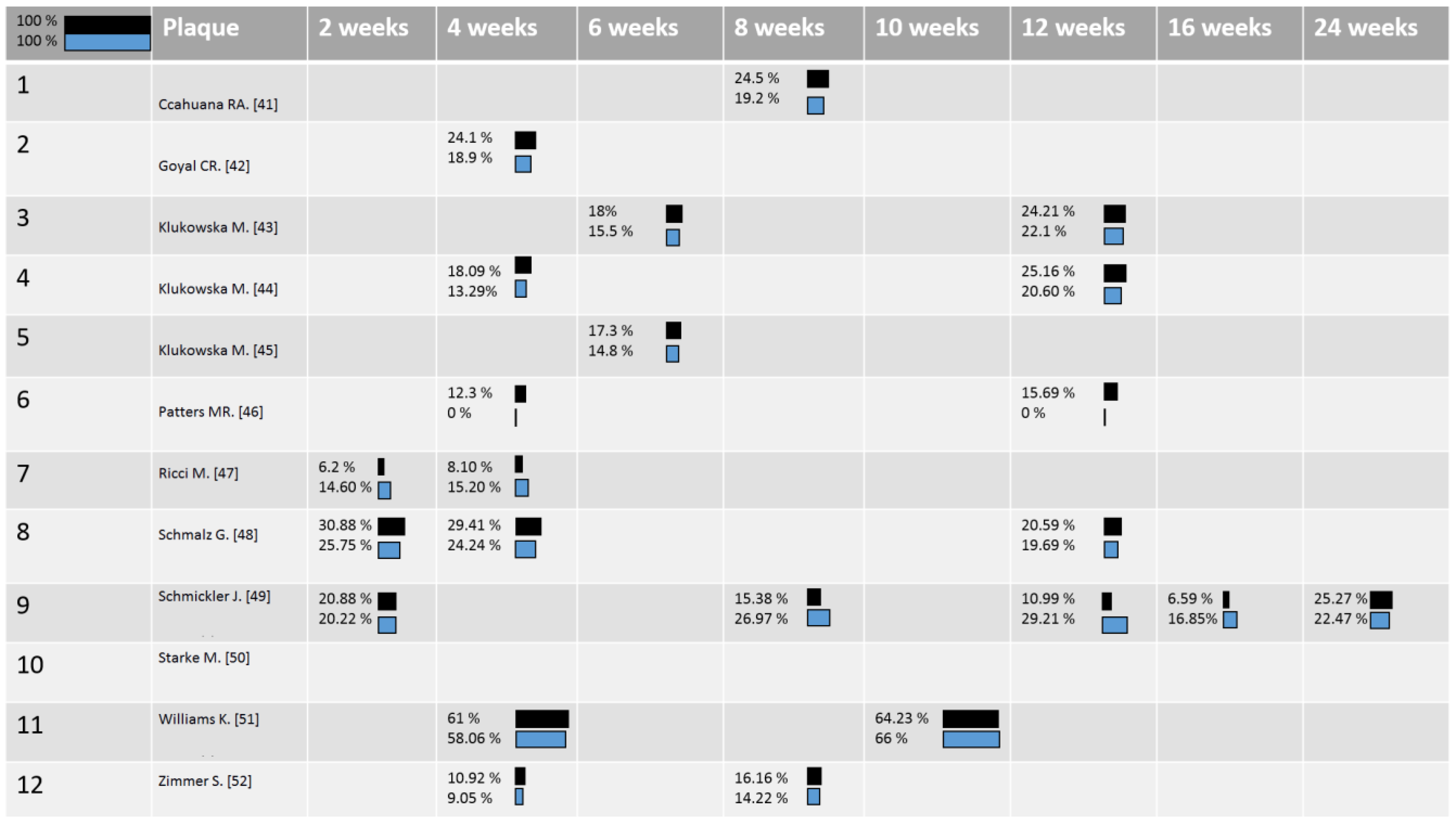
| 1 | Ccahuana-Vasquez RA. [41] | OR | No | Both types of toothbrush had significant results on clinical parameters compared to baseline (p < 0.001) but no significant differences were reported between OR and SA. |
| 2 | Goyal CR. [42] | OR | YES | Both types of toothbrush had significant results on clinical parameters compared to baseline (p < 0.001). Moreover, it is declared in the results that OR significantly reduced Gingival Index and bleeding, 40—50 % greater, compared to the SA, nevertheless the statics and p-value is not clear.* |
| 3 | Klukowska M. [43] | OR | YES | Both types of toothbrush had significant results on clinical parameters compared to baseline (p < 0.001). Moreover, it is declared in the results that OR reduced Gingival Index and bleeding significantly greater compared to the SA, but the statics and p-value is not clear. * |
| 4 | Klukowska M. [44] | OR | YES | Both types of toothbrush had significant results on clinical parameters compared to baseline (p < 0.001). Moreover, it is declared in the results that OR reduced Gingival Index and bleeding significantly greater compared to the SA, but the statics and p-value is not clear. * |
| 5 | Klukowska M. [45] | OR | YES | Both types of toothbrush had significant results on clinical parameters compared to baseline (p < 0.001). Moreover, it is declared in the results that OR reduced Gingival Index and bleeding significantly greater compared to the SA, but the statics and p-value is not clear. * |
| 6 | Patters MR. [46] | / | / | The OR group differed significantly from the SA group in mean Plaque Index at 4 and 12 weeks (p < 0.05) while SA was significantly greater in Gingival Index at 4 weeks. In total, OR had better but not significant clinical outcomes. |
| 7 | Ricci M. [47] | SA | YES | Both types of toothbrush had significant results on clinical parameters compared to baseline (p < 0.001). Moreover, it is declared in the results that SA significantly reduced Plaque Index and bleeding score compared to the OR, with a p value < 0.05, but data are not reported completely in the study. |
| 8 | Schmalz G. [48] | SA | / | Both types of toothbrush had significant results on clinical parameters compared to baseline (p < 0.05). Moreover, it is declared that significant differences were found for same parameters, although the changes were just minor. SA groups shown a constant decrease in Gingival Index, plaque and bleeding score while in the OR group the decrease was major at the beginning of observation period. |
| 9 | Schmickler J. [49] | SA | YES | The SA toothbrush had a significant better influence on Gingival Index and bleeding over OR group if the toothbrush is not replaced after a period of 4 months. Both type of toothbrush head loss the effectiveness in removing plaque after a period of 16—24 weeks. |
| 10 | Starke M. [50] | SA | YES | SA toothbrush was statistically superior to the OR in reducing gingival inflammation, gingival bleeding, after a timing of 14 and 42 days of home use. |
| 11 | Williams K. [51] | OR | YES | OR toothbrush had significant efficient results in reducing plaque and gingival inflammation but the data are reported incompletely. |
| 12 | Zimmer S. [52] | OR | NO | OR and SA toothbrush had significant better results than manual toothbrush in reducing plaque and bleeding but differences between the two powered toothbrushes was not significative. |
| Nr. | References | Conclusion |
|---|---|---|
| 1 | Ccahuana-Vasquez RA. [41] | 4 authors out of 6 (Dr. Ccahuana-Vasquez, Dr. Conde, Dr. Grender and Ms. Cunningham are employees of Procter & Gamble that supported the study and own the company Oral-B). Dr. Goyal and Mr. Qaqish have no conflict. |
| 2 | Goyal CR. [42] | 3 authors out of 5 (Dr. Klukowska, Dr. Grender, and Ms. Cunningham are employees of Procter & Gamble that supported the study and own the company Oral-B). Dr. Goyal and Mr. Qaqish have no conflict. |
| 3 | Klukowska M. [43] | 4 authors out of 5 (Dr. Klukowska, Dr. Grender, Biesbrock, and Mandl are employees of Procter & Gamble that supported the study and own the company Oral-B). Dr. Goyal has no conflict. |
| 4 | Klukowska M. [44] | 3 authors out of 4 (Dr. Klukowska, Dr. Grender, and Conde are employees of Procter & Gamble that supported the study and own the company Oral-B). Dr. Goyal has no conflict. |
| 5 | Klukowska M. [45] | 4 authors out of 5 (Dr. Klukowska, Dr. Grender, Ms. Conde, and Dr. Ccahuana-Vasquez are employees of Procter & Gamble that supported the study and own the company Oral-B). Dr. Goyal has no conflict. |
| 6 | Patters MR. [46] | This study was funded by a grant for Oralbotic Research, Inc. (company relative to the third group of treatment: powered toothbrush Hydrabrush®) |
| 7 | Ricci M. [47] | No conflict of interest |
| 8 | Schmalz G. [48] | No conflict of interest |
| 9 | Schmickler J. [49] | No conflict of interest |
| 10 | Starke M. [50] | This study was funded by Philips |
| 11 | Williams K. [51] | 4 authors out of 7 (Walters, Tao He, Julie Grender, and Biesbrock are employees of Procter & Gamble that supported the study and own the company Oral-B). Dr. Williams, Rapley, and Haun have no conflict. |
| 12 | Zimmer S. [52] | No conflict |
| Quality Assessment | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Nr. | References | Selection Generation | Allocation Concealement | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias | Study Quality |
| 1 | Ccahuana-Vasquez RA. [41] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | High Risk | Fair Quality |
| 2 | Goyal CR. [42] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | High Risk | Fair Quality |
| 3 | Klukowska M. [43] | Low Risk | Low Risk | Low Risk | Unclear Risk | Low Risk | Low Risk | High Risk | Fair Quality |
| 4 | Klukowska M. [44] | Low Risk | Low Risk | Low Risk | Unclear Risk | Low Risk | Low Risk | High Risk | Fair Quality |
| 5 | Klukowska M. [45] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | High Risk | Fair Quality |
| 6 | Patters MR. [46] | Low Risk | Low Risk | Low Risk | Unclear Risk | Unclear Risk | High Risk | High Risk | Poor quality |
| 7 | Ricci M. [47] | Unclear Risk | Low Risk | Low Risk | Unclear Risk | Unclear Risk | High Risk | Unclear Risk | Poor quality |
| 8 | Schmalz G. [48] | Low Risk | Low Risk | Low Risk | Unclear Risk | Low Risk | Low Risk | Low Risk | Good quality |
| 9 | Schmickler J. [49] | Low Risk | Low Risk | Low Risk | Unclear Risk | Low Risk | Low Risk | Low Risk | Good quality |
| 10 | Starke M. [50] | Low Risk | Low Risk | Low Risk | Unclear Risk | High Risk | High Risk | High Risk | Poor quality |
| 11 | Williams K. [51] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | High Risk | Fair Quality |
| 12 | Zimmer S. [52] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk | Good quality |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.M.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1468. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041468
Preda C, Butera A, Pelle S, Pautasso E, Chiesa A, Esposito F, Oldoini G, Scribante A, Genovesi AM, Cosola S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. International Journal of Environmental Research and Public Health. 2021; 18(4):1468. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041468
Chicago/Turabian StylePreda, Camilla, Andrea Butera, Silvia Pelle, Eleonora Pautasso, Alessandro Chiesa, Francesca Esposito, Giacomo Oldoini, Andrea Scribante, Anna Maria Genovesi, and Saverio Cosola. 2021. "The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review" International Journal of Environmental Research and Public Health 18, no. 4: 1468. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041468