
Mapping Research Conducted on Long-Term Care Facilities for Older People in Brazil: A Scoping Review

 ,
,  , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
- Describe the type and quality of empirical research conducted in Brazilian LTCFs for those aged over 60 years;
- Identify the topic areas of published research;
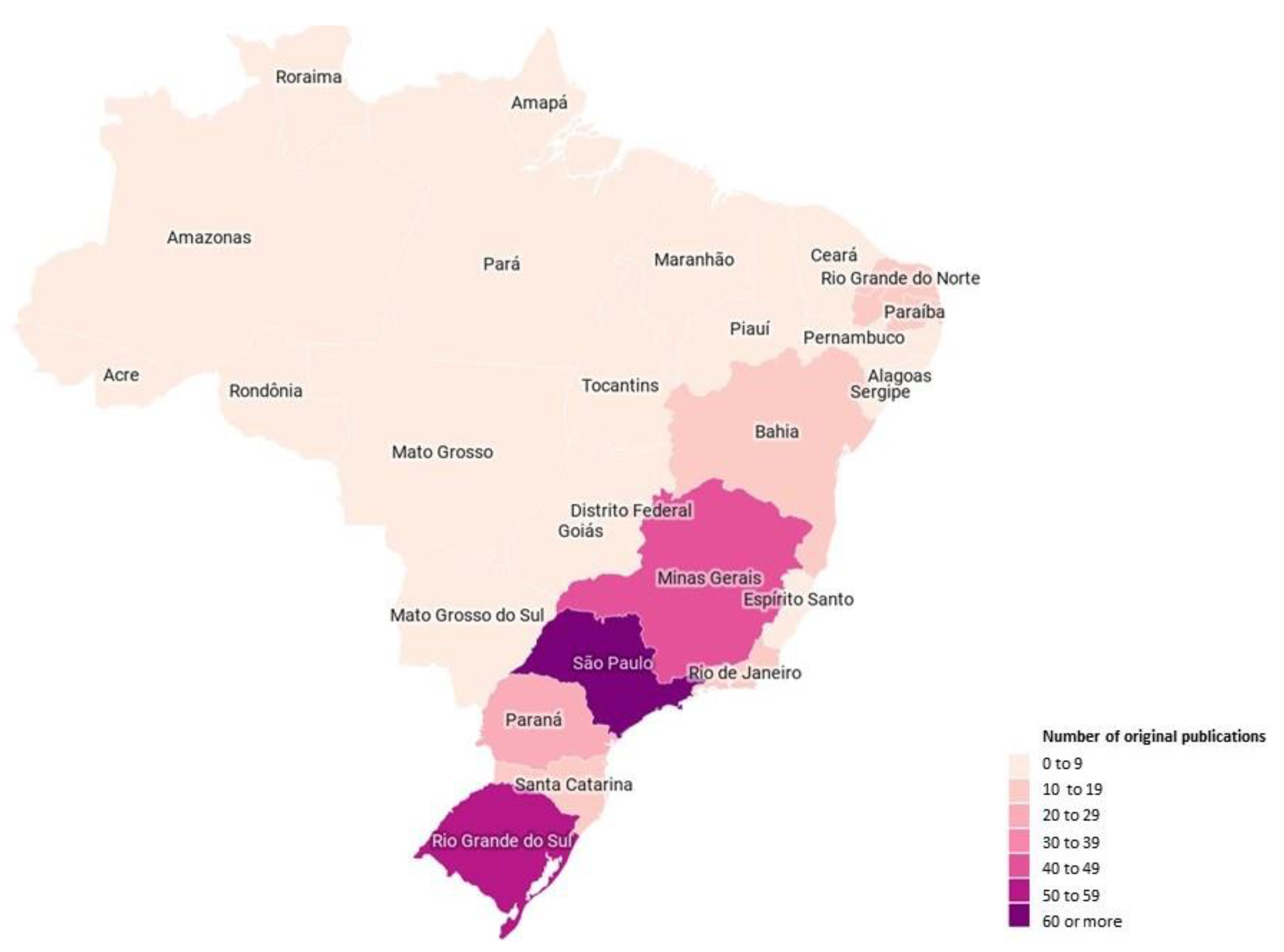
- Map the regions in Brazil where this research was conducted;
- Identify current knowledge gaps.
2. Methods
Eligibility Criteria
- Were empirical original research published in scientific journals;
- Investigated LTCF residents (older people aged 60 years and above as per/in line with the Brazilian definition of older people), their families, the LTCF workforce (e.g., healthcare professionals, care staff, and management-level staff), or LTCF organizations.
3. Results
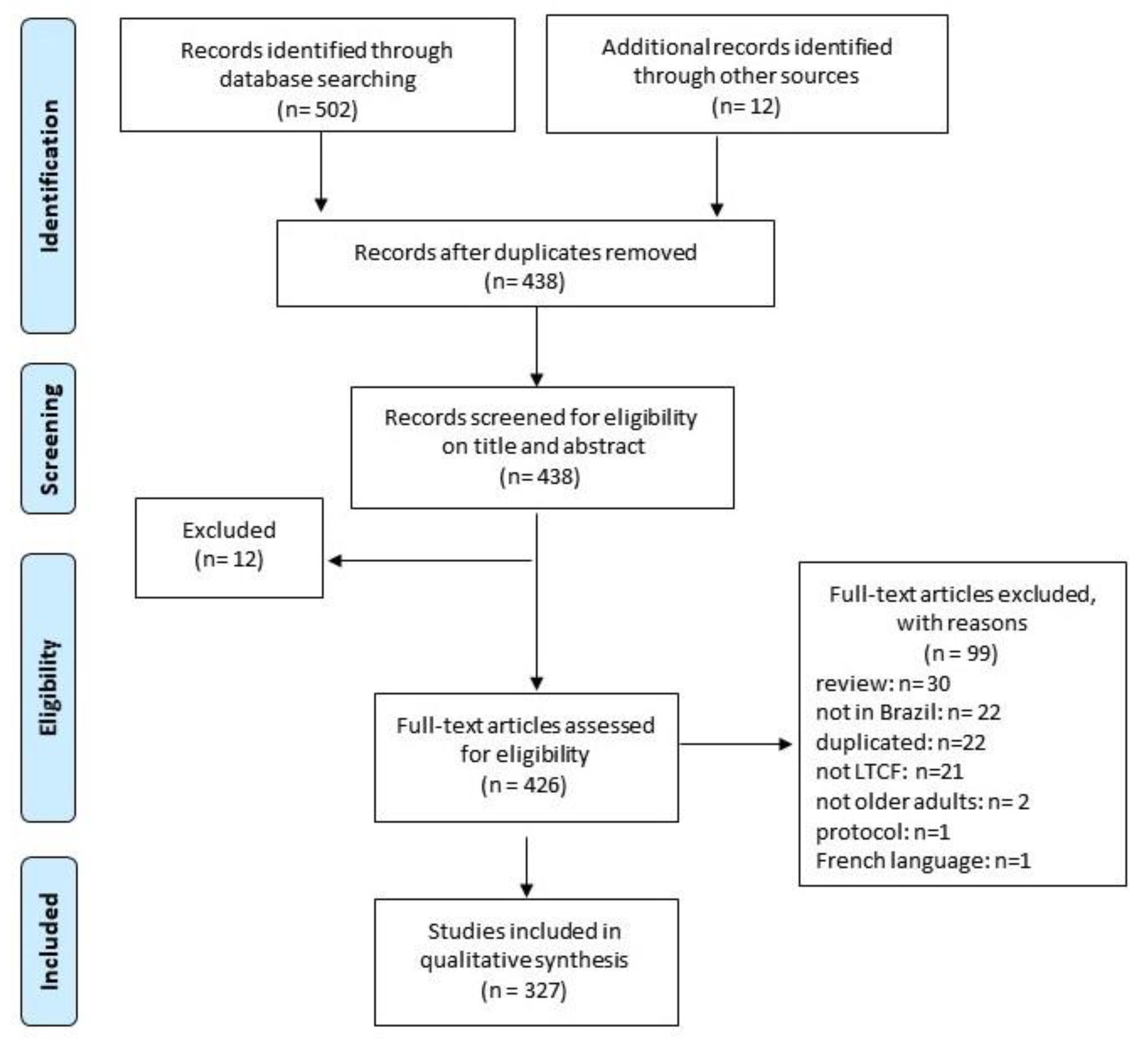
3.1. Study Inclusion
3.2. Features of Included Studies
3.3. Characteristics of Included LTCFs
3.4. Research Topic Areas
3.5. Methodological Appraisal
4. Discussion
5. Conclusions and Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Regional Office for South-East Asia. Ageing and Health. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 5 February 2018).
- Pot, A.M.; Briggs, A.M.; Beard, J.R. The Sustainable Development Agenda Needs to Include Long-Term Care. J. Am. Med. Dir. Assoc. 2018, 19, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.R.; Officer, A.M.; Cassels, A.K. The World Report on Ageing and Health. GERONT 2016, 56, S163–S166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Committee on Population; Division of Behavioral and Social Sciences and Education; National Academies of Sciences, Engineering and Medicine. Future Directions for the Demography of Aging: Proceedings of a Workshop; Hayward, M.D., Majmundar, M.K., Eds.; National Academies Press: Washington, DC, USA, 2018; p. 25064. ISBN 978-0-309-47410-8. [Google Scholar]
- Roquete, F.F.; Batista, C.C.R.F.; Arantes, R.C.; Roquete, F.F.; Batista, C.C.R.F.; Arantes, R.C. Care and Management Demands of Long-Term Care Facilities for the Elderly in Brazil: An Integrative Review (2004–2014). Rev. Bras. Geriatr. Gerontol. 2017, 20, 286–299. [Google Scholar] [CrossRef]
- Camarano, A.A.; Kanso, S. As instituições de longa permanência para idosos no Brasil. Rev. Bras. Estud. Popul. 2010, 27, 232–235. [Google Scholar] [CrossRef] [Green Version]
- Jacinto, A.F.; Achterberg, W.; Wachholz, P.A.; Dening, T.; Harrison Dening, K.; Devi, R.; Oliveira, D.; Everink, I.; Gaiolla, P.A.; Villas Bôas, P.J.F.; et al. Using international collaborations to shape research and innovation into care homes in brazil: A white paper. J. Nurs. Home Res. Sci. 2020, 6, 109–113. [Google Scholar] [CrossRef]
- Wachholz, P.A.; Moreira, V.G.; Oliveira, D.; Watanabe, H.A.W.; Boas, P.J.F.V. Occurrence of infection and mortality by covid-19 in care homes for older people in brazil. In Occurrence of Infection and Mortality by Covid-19 in Care Homes for Older People in Brazil; Botucatu Medical School-São Paulo State University: Botucatu, Brazil, 2020. [Google Scholar] [CrossRef]
- Tolson, D.; Rolland, Y.; Andrieu, S.; Aquino, J.P.; Beard, J.; Benetos, A.; Berrut, G.; Coll-Planas, L.; Dong, B.; Forette, F.; et al. International Association of Gerontology and Geriatrics: A Global Agenda for Clinical Research and Quality of Care in Nursing Homes. J. Am. Med. Dir. Assoc. 2011, 12, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, V.; Wood, F.; Hood, K. Establishing a Set of Research Priorities in Care Homes for Older People in the UK: A Modified Delphi Consensus Study with Care Home Staff. Age Ageing 2016, 46, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Wachholz, P.A.; Ricci, N.A.; Hinsliff-Smith, K.; Devi, R.; Shepherd, V.; VillasBoas, P.J.F.; Jacinto, A.F.; Watanabe, H.A.W.; Oliveira, D.; Gordon, A.L. Research on Long-Term Care Homes for Older People in Brazil: Protocol for a Scoping Review. East Midl. Res. Ageing Netw. 2019, 32, 1–16. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, M.; Godfrey, C.; McInerney, P.; Soares, C.; Khalil, H.; Parker, D. The Joanna Briggs Institute Reviewers’ Manual 2015 Methodology for JBI Scoping Reviews; The Joanna Briggs Institute, Ed.; The Joanna Briggs Institute: Adelaide, Australia, 2015. [Google Scholar]
- Trapé, T.L.; Campos, R.O. The Mental Health Care Model in Brazil: Analyses of the Funding, Governance Processes, and Mechanisms of Assessment. Rev. Saude Publica 2017, 51, 19. [Google Scholar] [CrossRef] [PubMed]
- Pluye, P.; Robert, E.; Cargo, M.; Bartlett, G. Mixed methods appraisal tool (MMAT) version 2018. Regist. Copyr. 2018, 1148552, 10. [Google Scholar]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; et al. Improving the Content Validity of the Mixed Methods Appraisal Tool: A Modified e-Delphi Study. J. Clin. Epidemiol. 2019, 111, 49–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) Version 2018 for Information Professionals and Researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Erlingsson, C.; Brysiewicz, P. A Hands-on Guide to Doing Content Analysis. Afr. J. Emerg. Med. 2017, 7, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Sun, Z.; He, L.; Liu, F.; Jing, X. Global Long-Term Care Research: A Scientometric Review. Int. J. Environ. Res. Public Health 2019, 16, 2077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bressan, V.; Cadorin, L.; Bianchi, M.; Barisone, M.; Rossi, S.; Bagnasco, A.; Carnevale, F.; Sasso, L. Research in Italian nursing practice: An extensive review of literature. Prof. Inferm. 2019, 72, 77–88. [Google Scholar] [CrossRef]
- Medeiros, M.; Souza, P.H. The State and Income Inequality in Brazil; Discussion Paper; IPEA-Instituto de Pesquisa Econômica Aplicada: Rio de Janeiro, Brazil, 2015. Available online: http://repositorio.ipea.gov.br/bitstream/11058/5182/1/DiscussionPaper_194.pdf (accessed on 10 September 2020).
- Goodman, C.; Davies, S. ENRICH: A New Innovation to Facilitate Dementia Research in Care Homes. Br. J. Community Nurs. 2012, 17, 277. [Google Scholar] [CrossRef] [PubMed]
- Giacomin, K.C. Frente Nacional de Fortalecimento ás Instituições de Longa Permanência Para Idosos. Available online: https://sbgg.org.br/wp-content/uploads/2020/06/Relato%CC%81rio-final-FN_fichaC.pdf (accessed on 25 October 2020).



{kind=link}
{kind=link}
| Qualitative (n = 67) | Descriptive (n = 82) | Non-Randomized (n = 159) | RCT (n = 6) | Mixed Methods (n = 11) | |
|---|---|---|---|---|---|
| Publication Date | |||||
| 1999–2009 | 11 (16.4%) | 19 (23.1%) | 24 (15.1%) | 1 (16.6%) | 5 (45.5%) |
| 2010–2015 | 42 (62.6%) | 45 (54.9%) | 83 (52.2%) | 1 (16.6%) | 5 (45.5%) |
| ≥2016 | 14 (20.9%) | 18 (21.9%) | 52 (32.7%) | 4 (66.8%) | 1 (9.0%) |
| Language | |||||
| English | 6 (8.9%) | 15 (18.3%) | 47 (29.5%) | 1 (16.6%) | 2 (18.2%) |
| Portuguese | 46 (68.7%) | 51 (62.2%) | 73 (45.9%) | 3 (50.0%) | 7 (63.6%) |
| At least Portuguese/English | 15 (22.4%) | 16 (19.5%) | 39 (24.6%) | 2 (33.4%) | 2 (18.2%) |
| Geographic area * | |||||
| North | 1 (1.5%) | 0 | 4 (2.5%) | 0 | 0 |
| Northeast | 13 (19.4%) | 21 (25.6%) | 32 (20.1%) | 1 (16.6%) | 0 |
| South | 29 (43.2%) | 17 (20.7%) | 35 (22.0%) | 3 (50.0%) | 7 (63.6%) |
| Southeast | 14 (20.9%) | 34 (41.5%) | 65 (40.9%) | 0 | 4 (36.4%) |
| Midwest | 4 (5.9%) | 6 (7.3%) | 16 (10.0%) | 1 (16.6%) | 0 |
| ≥2 geographic area | 3 (4.5%) | 2 (2.4%) | 3 (1.9%) | 0 | 0 |
| NR | 3 (4.5%) | 2 (2.4%) | 4 (2.5%) | 1 (16.6%) | 0 |
| 1st Author Institution | |||||
| Public University | 44 (65.7%) | 59 (71.9%) | 106 (66.7%) | 4 (66.8%) | 6 (54.5%) |
| Private University | 19 (28.3%) | 17 (20.7%) | 33 (20.7%) | 2 (33.2%) | 5 (45.5%) |
| Health Service | 2 (3.0%) | 2 (2.4%) | 6 (3.8%) | 0 | 0 |
| Governmental Agency | 0 | 1 (1.2%) | 1 (0.6%) | 0 | 0 |
| Others | 2 (3.0%) | 2 (2.4%) | 1 (0.6%) | 0 | 0 |
| NR | 0 | 1 (1.2%) | 2 (1.2%) | 0 | 0 |
| Ethical approval † | |||||
| Yes | 59 (88.0%) | 64 (78.0%) | 132 (83.0%) | 5 (83.4%) | 8 (72.7%) |
| NR | 8 (12.0%) | 18 (22.0%) | 27 (17.0%) | 1 (16.6%) | 3 (27.3%) |
| Qualitative (n = 67) | Descriptive (n = 82) | Non-Randomized (n = 159) | RCT (n = 6) | Mixed Methods (n = 11) | |
|---|---|---|---|---|---|
| Type of setting | |||||
| Profit | 2 (3.0%) | 0 | 1 (0.6%) | 0 | 0 |
| Non-profit | 32 (47.7%) | 31 (37.8%) | 59 (37.1%) | 3 (50.0%) | 1 (9.0%) |
| Both | 12 (17.9%) | 17 (20.7%) | 36 (22.6%) | 0 | 5 (45.5%) |
| NR | 21 (31.4%) | 34 (41.5%) | 63 (39.6%) | 3 (50.0%) | 5 (45.5%) |
| Setting Location | |||||
| Rural | 1 (1.5%) | 0 | 1 (0.6%) | 0 | 0 |
| Urban | 43 (64.2%) | 42 (51.2%) | 94 (59.1%) | 2 (33.2%) | 8 (72.7%) |
| Both | 0 | 5 (6.1%) | 8 (5.0%) | 0 | 0 |
| NR | 23 (34.3%) | 35 (42.7%) | 56 (35.3%) | 4 (66.8%) | 3 (27.2%) |
| Number of LTCF | |||||
| 1 | 46 (68.7%) | 35 (42.1%) | 60 (37.7%) | 3 (50.0%) | 5 (45.5%) |
| 2–5 | 9 (13.4%) | 19 (22.9%) | 37 (23.2%) | 3 (50.0%) | 1 (9.0%) |
| 6–10 | 8 (11.9%) | 12 (15.6%) | 25 (15.7%) | 0 | 0 |
| ≥11 | 3 (4.5%) | 08 (9.7%) | 22 (13.8%) | 0 | 4 (36.5%) |
| NR/NA | 1 (1.5%) | 08 (9.7%) | 15 (9.4%) | 0 | 1 (9.0%) |
| (Min–Max, mean, median) | (0–52, 3.7, 1) | (1–156, 10.1, 2) | (1–125,6.4, 2) | (1–5, 2.0, 1.5) | (1–52, 14.4, 1) |
| Sample composition | |||||
| Older adults | 33 (49.2%) | 64 (78.0%) | 133 (83.6%) | 6 (100%) | 5 (45.5%) |
| Total (Min–Max, mean, median) | Total = 428 (2–59, 12.9, 10) | Total = 11,358 (1–2184, 177.4, 76) | Total = 22.747 (4–3903, 171.0, 81.0) | Total = 164 (13–37, 27.3, 30) | Total = 204 (8–55, 40.8, 43) |
| Family | 1 (1.5%) | 0 | 0 | 0 | 0 |
| Total (Min–Max, mean, median) | Total = 6 | ||||
| Staff | 19 (28.3%) | 7 (8.5%) | 7 (4.4%) | 0 | 3 (27.2%) |
| Total (Min–Max, mean, median) | Total = 337 (7–40, 17.7, 16) | Total = 411 (12–181, 58.7, 38.5) | Total = 459 (22–181, 65.5, 45) | Total = 281 (38–181, 93.6, 62) | |
| LTCF characteristics | 3 (4.4%) | 7 (8.5%) | 2 (1.3%) | 0 | 0 |
| Total (Min–Max, mean, median) | Total = 59 (1–52, 19.6, 6) | 199 (4–156, 28.4, 7.5) | Total = 80 (29–51, 40.0, 40) | ||
| Managers and stakeholders | 3 (4.4%) | 1 (1.2%) | 0 | 0 | |
| Total (Min–Max, mean, median) | Total = 18 (5–7, 6.0, 6) | Total = 67 | |||
| Older adults × Non-institutionalized older adults | 0 | 2 (2.4%) | 15 (9.4%) | 0 | 1 (9.0%) |
| Total (Min–Max, mean, median) | Total = 192 (15–177, 96.0, 96) × Total = 273 (30–243, 136.5, 136.5) | Total = 1180 (14–393, 78.7, 42) × Total = 16,839 (14–598, 112.6, 76) | Total = 30 × Total = 30 | ||
| Older adults × Staff | 2 (3.0%) | 1 (1.2%) | 2 (1.3%) | 0 | 2 (18.3%) |
| Total (Min–Max, mean, median) | Total = 13 (3–10, 6.5, 6.5) × Total = 25 (9–16, 12.5, 12.5) | Total = 62 × Total = 33 | Total = 57 (11–46, 28.5,28.5) × Total = 40 (15–25, 20.0, 20) | Total = 314 (6–308,157.0, 157) × Total = 50 (7–43, 25.0, 25.0) | |
| Older adults × Family | 1 (1.5%) | ||||
| Total (Min–Max, mean, median) | Total = 3 × Total = 3 | ||||
| Older adults × Managers | 3 (4.4%) | ||||
| Total (Min–Max, mean, median) | Total = 27 (8–11, 13.5, 8) × Total = 17 (3–7, 8.5, 7) | ||||
| Family × Staff | 1 (1.5%) | ||||
| Total (Min–Max, mean, median) | Total = 13 × Total = 19 | ||||
| Managers × Staff | 1 (1.5%) | ||||
| Total (Min–Max, mean, median) | Total = 20 × Total = 36 |
| Screening Questions (for All Types) | Qualitative (n = 67) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Are there clear research questions? | Do the collected data allow to address the research questions? | Is the qualitative approach appropriate to answer the research question? | Are the qualitative data collection methods adequate to address the research question? | Are the findings adequately derived from the data? | Is the interpretation of results sufficiently substantiated by data? | Is there coherence between qualitative data sources, collection, analysis, and interpretation? | ||||||||||||||
| Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C |
| 62 | 5 | - | 53 | 9 | 5 | 56 | 6 | 5 | 38 | 7 | 22 | 40 | 3 | 24 | 37 | 6 | 24 | 37 | 11 | 19 |
| Quantitative randomized controlled trials (n = 6) | ||||||||||||||||||||
| Is randomization appropriately performed? | Are the groups comparable at baseline? | Are there complete outcome data? | Are outcome assessors blinded to the intervention provided? | Did the participants adhere to the assigned intervention? | ||||||||||||||||
| Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C |
| 6 | - | - | 5 | - | 1 | 1 | 1 | 4 | 4 | - | 2 | 3 | 2 | 1 | 2 | 3 | 1 | 2 | 1 | 3 |
| Quantitative non- randomized (n = 159) | ||||||||||||||||||||
| Are the participants representative of the target population? | Are measurements appropriate regarding both the outcome and intervention (or exposure)? | Are there complete outcome data? | Are the confounders accounted for in the design and analysis? | During the study period, is the intervention administered (or exposure occurred) as intended? | ||||||||||||||||
| Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C |
| 156 | 3 | - | 140 | 6 | 13 | 57 | 47 | 55 | 120 | 19 | 20 | 126 | 7 | 26 | 56 | 58 | 45 | 120 | 15 | 24 |
| Quantitative descriptive (n = 82) | ||||||||||||||||||||
| Is the sampling strategy relevant to address the research question? | Is the sample representative of the target population? | Are the measurements appropriate? | Is the risk of nonresponse bias low? | Is the statistical analysis appropriate to answer the research question? | ||||||||||||||||
| Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C |
| 78 | 3 | 1 | 64 | 11 | 7 | 37 | 21 | 24 | 32 | 31 | 19 | 61 | 9 | 12 | 29 | 12 | 41 | 58 | 8 | 16 |
| Mixed methods (n = 11) | ||||||||||||||||||||
| Is there an adequate rationale for using a mixed methods design to address the research question? | Are the different components of the study effectively integrated to answer the research question? | Are the outputs of the integration of qualitative and quantitative components adequately interpreted? | Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? | Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | ||||||||||||||||
| Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C | Y | N | C |
| 11 | - | - | 7 | 1 | 3 | 7 | 1 | 3 | 6 | 4 | 1 | 6 | 4 | 1 | 3 | 2 | 6 | 6 | 4 | 1 |
| Category with most of the studies with YES | ||||||||||||||||||||
| Category with most of the studies with NO | ||||||||||||||||||||
| Category with most of the studies with CANNOT DETERMINE | ||||||||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wachholz, P.A.; De Oliveira, D.C.; Hinsliff-Smith, K.; Devi, R.; Villas Boas, P.J.F.; Shepherd, V.; Jacinto, A.F.; Watanabe, H.A.W.; Gordon, A.L.; Ricci, N.A. Mapping Research Conducted on Long-Term Care Facilities for Older People in Brazil: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 1522. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041522
Wachholz PA, De Oliveira DC, Hinsliff-Smith K, Devi R, Villas Boas PJF, Shepherd V, Jacinto AF, Watanabe HAW, Gordon AL, Ricci NA. Mapping Research Conducted on Long-Term Care Facilities for Older People in Brazil: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(4):1522. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041522
Chicago/Turabian StyleWachholz, Patrick Alexander, Deborah Cristina De Oliveira, Kathryn Hinsliff-Smith, Reena Devi, Paulo José Fortes Villas Boas, Victoria Shepherd, Alessandro Ferrari Jacinto, Helena Akemi Wada Watanabe, Adam Lee Gordon, and Natalia Aquaroni Ricci. 2021. "Mapping Research Conducted on Long-Term Care Facilities for Older People in Brazil: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 4: 1522. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041522