
Diet and Health Benefits Associated with In-Home Eating and Sharing Meals at Home: A Systematic Review



Abstract
:1. Introduction
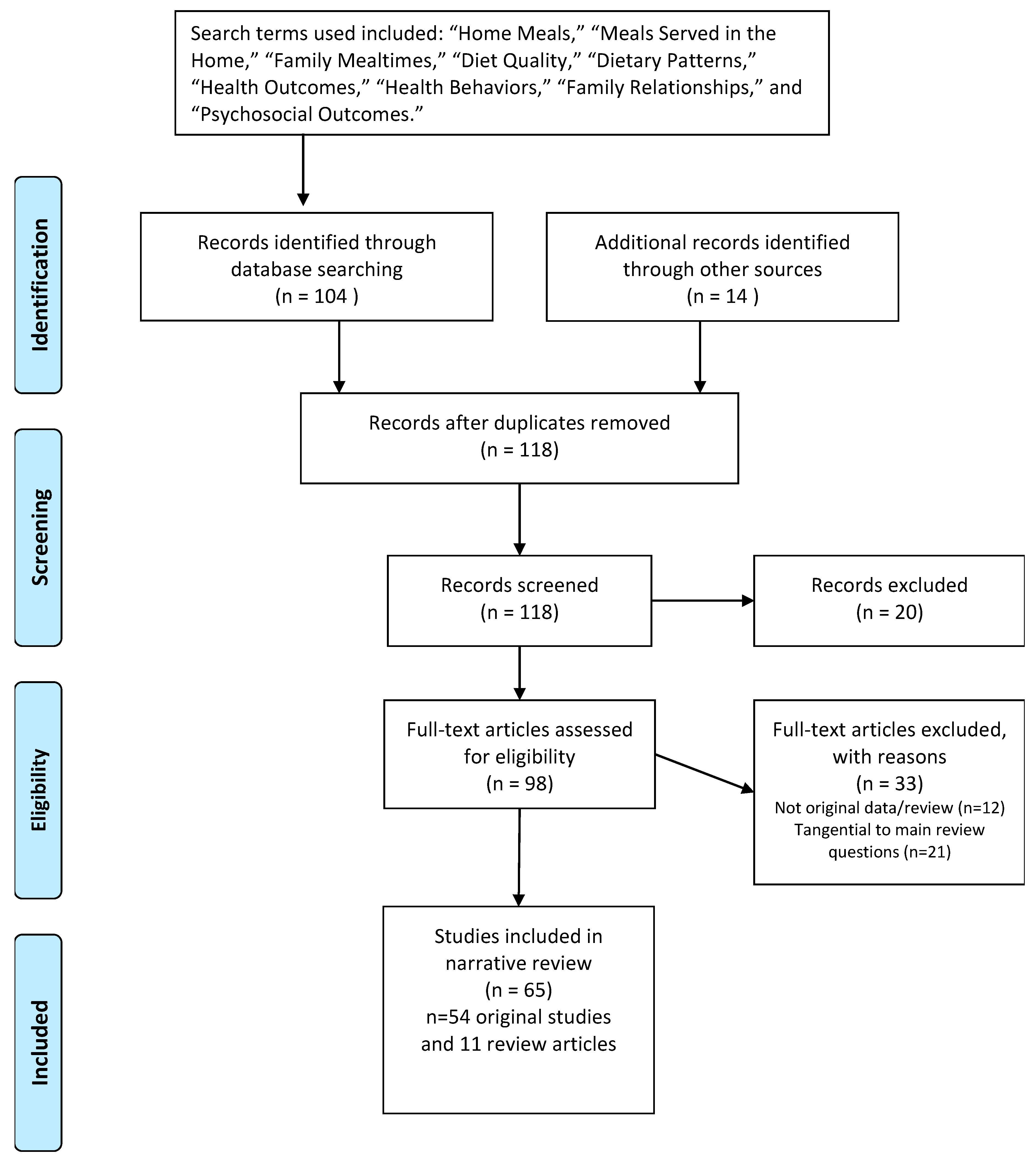
2. Materials and Methods
2.1. Terminology
2.1.1. Defining and Measuring In-Home Meals and Shared Meals at Home
2.1.2. Other Behaviors and Circumstances Closely Related to In-Home Meals and Shared Meals at Home
3. Results
3.1. Diet Quality and Meal Patterns
3.2. Health Outcomes

{kind=link}
| Author(s) and Year | Reference Number | Sample | Main Outcomes | Study Design |
|---|---|---|---|---|
| Health Outcomes | ||||
| Anderson and Whitaker (2010) | [20] | 8850 children aged 4 | Children who ate dinner with their families more than five nights per week were less likely to be obese. | Cross-Sectional |
| Berge et al. (2014) | [33] | 120 children aged 6–12 from low-income and minority communities | Positive family and parent-level interpersonal dynamics during family meals were associated with reduced risk of children being overweight. Positive family and parent-level food-related dynamics during family meals were associated with reduced risk of childhood obesity. | Cross-Sectional |
| Fiese et al. (2012) | [32] | 200 families with children aged 5–12 | Families with overweight or obese children spent less time on a family meal and spent less time in positive communication than families with children of a healthy weight. | Observational |
| Franko et al. (2008) | [28] | 2379 females tracked annually from age 9–19 | More frequent family meals from ages 9–11 predicted lower likelihood of bulimic symptoms, drive for thinness, and smoking behaviors during adolescence. Family cohesion mediated the relationships between family meals and risk of smoking behaviors. | Longitudinal |
| Gable et al. (2007) | [55] | 8549 children were followed from kindergarten through third grade | Children who ate fewer family meals during kindergarten and first grader were more likely to be overweight in third grade. | Longitudinal |
| Hammons and Fiese (2011) | [45] | 182,836 children and adolescents across 17 studies | Children and adolescents who ate meals with family 3 or more times per week had healthier weight status than those who ate fewer than 3 meals with family per week. | Meta-Analysis |
| Jones et al. (2014) | [63] | 337 preschool-age children | Children who participated in frequent family meals were more likely to get 10 or more hours of sleep per night. | Cross-Sectional |
| Kitzman-Ulrich et al. (2010) | [64] | Youth (elementary age–adolescents) who participated in weight loss, physical activity, or dietary interventions | Family functioning and parenting styles should be investigated as potential mediators of intervention outcomes in weight loss and physical activity interventions. | Systematic Review |
| Loth et al. (2015) | [62] | 2382 middle and high school students, Project EAT | Greater frequency of family meals was associated with decreased odds of engaging in unhealthy weight control behaviors in boys, and dieting, unhealthy and extreme weight control behaviors in girls. | Cross-Sectional |
| McCurdy et al. (2014) | [31] | 164 low-income, preschool-aged children and their mothers | Maternal presence when the child ate was associated with lower BMI z-scores for children. | Cross-Sectional |
| Munoz et al. (2007) | [61] | 134 female undergraduate students | Overall family stability was a more comprehensive predictor or bulimia symptom than family meal frequency alone. | Cross-Sectional Retrospective |
| Neumark-Sztainer et al. (2008) | [60] | 2516 adolescents, Project EAT | Adolescent girls who ate five or more meals per week with their families in middle school were less likely to engage in extreme weight control behaviors five years later. | Longitudinal |
| Piazza-Waggoner, et al. (2011) | [65] | 56 families with obese and non-obese children | Parents and caregivers of obese children reported greater mealtime challenges and a less positive mealtime environment than caregivers of non-obese children. There were no differences in observed mealtime interactions in families with obese and non-obese children. | Observational |
| Rollins et al. (2010) | [56] | 16,770 children aged 6–11 (national sample) | Family meals were protective against obesity in non-Hispanic White children and non-Hispanic Black boys, were a marginal risk factor for obesity for Hispanic boys living in low-education households. | Cross-Sectional |
| Sen (2006) | [58] | 5041 youth aged 12–15 (national sample) | Family meal frequency at age 12 was associated with healthier weight status at age 12 and age 15 for White participants. No associations between family meal frequency and weight status for Black and Hispanic participants. | Cross-Sectional |
| Skeer and Ballard (2013) | [57] | Families with adolescent children | Frequent family meals were associated with decreased risk for overweight and obesity in females. | Literature Review |
| Taveras et al. (2005) | [59] | 14,431 children aged 9–14 (national sample) | Children who ate dinner with their families most days or everyday were less likely to be overweight than children who ate dinner with their families never or some days. | Longitudinal |
| Utter et al. (2008) | [50] | 3245 adolescents (national sample) | Frequency of family meals was not significantly related to BMI when demographics were included in the model. | Cross-Sectional |
| Wansink and van Kleef (2014) | [30] | 190 parents and 148 children in third-sixth grade | Families who regularly ate dinner in the dining room or kitchen had lower BMIs (for both adults and children). Helping cook dinner was associated with higher BMI for females and remaining at the table until everyone is finished eating was associated with lower BMI for males. | Cross-Sectional |
3.3. Psychosocial Outcomes
3.4. Family Relationships
3.5. Correlates of In-Home Eating and Shared Meals
3.6. Interventions to Increase Shared Meals at Home
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramey, V.A. Time Spent in Home Production in the Twentieth-Century United States: New Estimates from Old Data. J. Econ. Hist. 2009, 69, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; CMullany, E.; Biryukov, S.; Abbafati, C.; FeredeAbera, S.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- James, W.P.T. WHO recognition of the global obesity epidemic. Int. J. Obes. 2008, 32, S120–S126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, M.B.; Robson, S.M.; Stark, L.J. A Review of the Structural Characteristics of Family Meals with Children in the United States. Adv. Nutr. 2016, 7, 627–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenberg, M.E.; Olson, R.E.; Neumark-Sztainer, D.; Story, M.; Bearinger, L.H. Correlations Between Family Meals and Psychosocial Well-being Among Adolescents. Arch. Pediatr. Adolesc. Med. 2004, 158, 792–796. [Google Scholar] [CrossRef] [Green Version]
- Sen, B.P.; Goldfarb, S.; Tarver, W.L. Family structure and risk behaviors: The role of the family meal in assessing likelihood of adolescent risk behaviors. Psychol. Res. Behav. Manag. 2014, 7, 53–66. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, M.E.; Neumark-Sztainer, D.; A Fulkerson, J.; Story, M.T. Family Meals and Substance Use: Is There a Long-Term Protective Association? J. Adolesc. Health 2008, 43, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Siddaway, A.P.; Wood, A.M.; Hedges, L.V. How to Do a Systematic Review: A Best Practice Guide for Conducting and Reporting Narrative Reviews, Meta-Analyses, and Meta-Syntheses. Annu. Rev. Psychol. 2019, 70, 747–770. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, R.F.; Leary, M.R. Writing Narrative Literature Reviews. Rev. Gen. Psychol. 1997, 1, 311–320. [Google Scholar] [CrossRef]
- A O’Dwyer, N.; Gibney, M.J.; Burke, S.J.; McCarthy, S.N. The influence of eating location on nutrient intakes in Irish adults: Implications for developing food-based dietary guidelines. Public Health Nutr. 2005, 8, 258–265. [Google Scholar] [CrossRef]
- Couch, S.C.; Glanz, K.; Zhou, C.; Sallis, J.F.; Saelens, B.E. Home Food Environment in Relation to Children’s Diet Quality and Weight Status. J. Acad. Nutr. Diet. 2014, 114, 1569–1579.e1. [Google Scholar] [CrossRef] [Green Version]
- Fulkerson, J.A.; Larson, N.; Horning, M.; Neumark-Sztainer, D. A Review of Associations Between Family or Shared Meal Frequency and Dietary and Weight Status Outcomes Across the Lifespan. J. Nutr. Educ. Behav. 2014, 46, 2–19. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Hannan, P.J.; Story, M.; Croll, J.; Perry, C. Family meal patterns: Associations with sociodemographic characteristics and improved dietary intake among adolescents. J. Am. Diet. Assoc. 2003, 103, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Fulkerson, J.A.; Kubik, M.Y.; Story, M.; Lytle, L.; Arcan, C. Are There Nutritional and Other Benefits Associated with Family Meals Among At-Risk Youth? J. Adolesc. Health 2009, 45, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Burgess-Champoux, T.L.; Larson, N.; Neumark-Sztainer, D.; Hannan, P.J.; Story, M. Are Family Meal Patterns Associated with Overall Diet Quality during the Transition from Early to Middle Adolescence? J. Nutr. Educ. Behav. 2009, 41, 79–86. [Google Scholar] [CrossRef]
- Chan, J.C.; Sobal, J. Family meals and body weight. Analysis of multiple family members in family units. Appetite 2011, 57, 517–524. [Google Scholar] [CrossRef]
- Feldman, S.; Eisenberg, M.E.; Neumark-Sztainer, D.; Story, M.T. Associations between Watching TV during Family Meals and Dietary Intake Among Adolescents. J. Nutr. Educ. Behav. 2007, 39, 257–263. [Google Scholar] [CrossRef]
- Fink, S.K.; Racine, E.F.; Mueffelmann, R.E.; Dean, M.N.; Herman-Smith, R. Family Meals and Diet Quality Among Children and Adolescents in North Carolina. J. Nutr. Educ. Behav. 2014, 46, 418–422. [Google Scholar] [CrossRef]
- Fitzpatrick, E.; Edmunds, L.S.; Dennison, B.A. Positive Effects of Family Dinner Are Undone by Television Viewing. J. Am. Diet. Assoc. 2007, 107, 666–671. [Google Scholar] [CrossRef]
- Anderson, S.E.; Whitaker, R.C. Household Routines and Obesity in US Preschool-Aged Children. Pediatrics 2010, 125, 420–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appelhans, B.M.; Waring, M.E.; Schneider, K.L.; Pagoto, S.L. Food preparation supplies predict children’s family meal and home-prepared dinner consumption in low-income households. Appetite 2014, 76, 1–8. [Google Scholar] [CrossRef]
- Bauer, K.W.; Hearst, M.O.; Escoto, K.H.; Berge, J.M.; Neumark-Sztainer, D. Parental employment and work-family stress: Associations with family food environments. Soc. Sci. Med. 2012, 75, 496–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berge, J.M.; MacLehose, R.F.; Loth, K.A.; Eisenberg, M.E.; Fulkerson, J.A.; Neumark-Sztainer, D. Family meals. Associations with weight and eating behaviors among mothers and fathers. Appetite 2012, 58, 1128–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulkerson, J.A.; Neumark-Sztainer, D.; Story, M.T. Adolescent and Parent Views of Family Meals. J. Am. Diet. Assoc. 2006, 106, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.X.; Baquero, B.; Arredondo, E.M.; Campbell, N.; Larios, S.; Elder, J.P. Association Between Family Variables and Mexican American Children’s Dietary Behaviors. J. Nutr. Educ. Behav. 2007, 39, 62–69. [Google Scholar] [CrossRef]
- Fulkerson, J.A.; Pasch, K.E.; Stigler, M.H.; Farbakhsh, K.; Perry, C.L.; Komro, K.A. Longitudinal assoications between family dinner and adolescent perceptions of parent-child communicaiton among racially diverse urban youth. J. Fam. Psychol. 2010, 24, 261–270. [Google Scholar] [CrossRef] [Green Version]
- Crawford, D.; Ball, K.; Mishra, G.D.; Salmon, J.; Timperio, A. Which food-related behaviours are associated with healthier intakes of fruits and vegetables among women? Public Health Nutr. 2007, 10, 256–265. [Google Scholar] [CrossRef] [Green Version]
- Franko, D.L.; Thompson, U.; Affenito, S.G.; Barton, B.; Striegel-Moore, R.H.; Weissman, R.S. What mediates the relationship between family meals and adolescent health issues. Health Psychol. 2008, 27 (Suppl. S109), S109–S117. [Google Scholar] [CrossRef]
- Mills, S.; White, M.; Robalino, S.; Wrieden, W.; Brown, H.; Adams, J. Systematic review of the health and social determinants and outcomes of home cooking: Protocol. Syst. Rev. 2015, 4, 35. [Google Scholar] [CrossRef] [Green Version]
- Wansink, B.; van Kleef, E. Dinner rituals that correlate with child and adult. BMI Obes. 2014, 22, 91–95. [Google Scholar]
- McCurdy, K.; Gorman, K.S.; Kisler, T.; Metallinos-Katsaras, M.-K. Associations between family food behaviors, maternal depression, and child weight among low-income children. Appetite 2014, 79, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Fiese, B.H.; Hammons, A.; Grigsby-Toussaint, D. Family mealtimes: A contextual approach to understanding childhood obesity. Econ. Hum. Biol. 2012, 10, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Berge, J.M.; Rowley, S.; Trofholz, A.; Hanson, C.; Rueter, M.; MacLehose, R.F.; Neumark-Sztainer, D. Childhood obseity and interpersonal dynamics during family meals. Pediatrics 2014, 134, 923–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergmeier, H.; Skouteris, H.; Hetherington, M.M. Systematic research review of observational approaches used to evaluate mother-child mealtime interactions during preschool years. Am. J. Clin. Nutr. 2014, 101, 7–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiese, B.H.; Jones, B.L.; Jarick, J.M. Family Mealtime Dynamics and Food Consumption: An Experimental Approach to Understanding Distractions. Couple Fam. Psychol. Res. Pr. 2015, 4, 199–211. [Google Scholar] [CrossRef]
- Larson, N.I.; Perry, C.L.; Story, M.; Neumark-Sztainer, D. Food Preparation by Young Adults Is Associated with Better Diet Quality. J. Am. Diet. Assoc. 2006, 106, 2001–2007. [Google Scholar] [CrossRef]
- Larson, N.I.; Neumark-Sztainer, D.; Hannan, P.J.; Story, M. Family Meals during Adolescence Are Associated with Higher Diet Quality and Healthful Meal Patterns during Young Adulthood. J. Am. Diet. Assoc. 2007, 107, 1502–1510. [Google Scholar] [CrossRef]
- Chu, Y.L.; Storey, K.E.; Veugelers, P.J. Involvement in Meal Preparation at Home Is Associated with Better Diet Quality Among Canadian Children. J. Nutr. Educ. Behav. 2014, 46, 304–308. [Google Scholar] [CrossRef]
- Haapalahti, M.; Mykkanen, H.; Tikkanen, S.; Kokkonen, J. Meal patterns and food use in 10- to 11-year-old Finnish children. Public Health Nutr. 2003, 6, 365–370. [Google Scholar] [CrossRef] [Green Version]
- Burke, S.; McCarthy, S.; O’Neill, J.; Hannon, E.; Kiely, M.; Flynn, A.; Gibney, M. An examination of the influence of eating location on the diets of Irish children. Public Health Nutr. 2007, 10, 599–607. [Google Scholar] [CrossRef] [Green Version]
- Sweetman, C.; McGowan, L.; Croker, H.; Cooke, L. Characteristics of family mealtimes affecting children’s vegetable consumption and liking. J. Am. Diet. Assoc. 2011, 111, 269–273. [Google Scholar] [CrossRef]
- Naska, A.; Katsoulis, M.; Orfanos, P.; Lachat, C.; Gedrich, K.; Rodrigues, S.S.P.; Freisling, H.; Kolsteren, P.; Engeset, D.; Lopes, C.; et al. Eating out is different from eating at home among individuals who occasionally eat out. A cross-sectional study among middle-aged adults from eleven European countries. Br. J. Nutr. 2015, 113, 1951–1964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flores, G.; Tomany-Korman, S.C.; Olson, L. Does disadvantage start at home? Racial and ethnic disparities in health-related early childhood home routines and safety practices. Arch. Pediatr. Adolesc. Med. 2005, 159, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Gillman, M.W.; Rifas-Shiman, S.L.; Frazier, A.L.; Rockett, H.R.; Camargo, C.A., Jr.; Field, A.E.; Berkey, C.S.; Colditz, G.A. Family dinner and diet quality among older children and adolescents. Arch. Fam. Med. 2000, 9, 235–240. [Google Scholar] [CrossRef]
- Hammons, A.; Fiese, B.H. Is frequency of shared family meals related to the nutritional health of children and adolescents? A meta-analysis. Pediatrics 2011, 127, 1565–1574. [Google Scholar] [CrossRef] [Green Version]
- Martin-Biggers, J.; Spaccarotella, K.; Berhaupt-Glickstein, A.; Hongu, N.; Worobey, J.; Byrd-Bredbenner, C. Come and Get It! A Discussion of Family Mealtime Literature and Factors Affecting Obesity Risk1–3. Adv. Nutr. 2014, 5, 235–247. [Google Scholar] [CrossRef] [Green Version]
- Patrick, H.; Nicklas, T.A. A Review of Family and Social Determinants of Children’s Eating Patterns and Diet Quality. J. Am. Coll. Nutr. 2005, 24, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Poti, J.M.; Popkin, B.M. Trends in Energy Intake among US Children by Eating Location and Food Source, 1977–2006. J. Am. Diet. Assoc. 2011, 111, 1156–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surjadi, F.F.; Takeuchi, D.T.; Umoren, J. Racial and Ethnic Differences in Longitudinal Patterns of Family Mealtimes: Link to Adolescent Fruit and Vegetable Consumption. J. Nutr. Educ. Behav. 2017, 49, 244–249.e1. [Google Scholar] [CrossRef] [PubMed]
- Utter, J.; Scragg, R.; Schaaf, D.; Ni Mhurchu, C. Relationships between frequency of family meals, BMI and nutritional aspects of the home food environment among New Zealand adolescents. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 50. [Google Scholar] [CrossRef] [Green Version]
- Videon, T.M.; Manning, C.K. Influences on adolescent eating patterns: The importance of family meals. J. Adolesc. Health 2003, 32, 365–373. [Google Scholar] [CrossRef]
- Woodruff, S.J.; Hanning, R.M. A Review of Family Meal Influence on Adolescents’ Dietary Intake. Can. J. Diet. Pr. Res. 2008, 69, 14–22. [Google Scholar] [CrossRef]
- Woodruff, S.J.; Hanning, R.M. Associations Between Family Dinner Frequency and Specific Food Behaviors Among Grade Six, Seven, and Eight Students from Ontario and Nova Scotia. J. Adolesc. Health 2009, 44, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Welsh, E.M.; French, S.A.; Wall, M. Examining the Relationship Between Family Meal Frequency and Individual Dietary Intake: Does Family Cohesion Play a Role? J. Nutr. Educ. Behav. 2011, 43, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Gable, S.; Chang, Y.; Krull, J.L. Television Watching and Frequency of Family Meals Are Predictive of Overweight Onset and Persistence in a National Sample of School-Aged Children. J. Am. Diet. Assoc. 2007, 107, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Rollins, B.Y.; Belue, R.Z.; Francis, L.A. The beneficial effect of family meals on obesity differs by race, sex, and household education: The national survey on children’s health. J. Am. Diet. Assoc. 2010, 110, 1335–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skeer, M.R.; Ballard, E.L. Are family meals as good for youth as we think they are? A review of the literature on family meals as they pertain to adolescent risk protection. J. Youth Adolesc. 2013, 42, 943–963. [Google Scholar] [CrossRef] [PubMed]
- Sen, B.P. Frequency of Family Dinner and Adolescent Body Weight Status: Evidence from the National Longitudinal Survey of Youth, 1997. Obesity 2006, 14, 2266–2276. [Google Scholar] [CrossRef] [PubMed]
- Taveras, E.M.; Rifas-Shiman, S.L.; Berkey, C.S.; Rockett, H.R.; Field, A.E.; Frazier, A.L.; Colditz, G.A.; Gillman, M.W. Family Dinner and Adolescent Overweight. Obes. Res. 2005, 13, 900–906. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Eisenberg, M.E.; Fulkerson, J.A.; Story, M.; Larson, N.I. Family meals and disordered eating in adolescents: Longitudinal findings from project EAT. Arch. Pediatr. Adolesc. Med. 2008, 162, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Munoz, D.J.; Israel, A.C.; Anderson, E.A. The Relationship of Family Stability and Family Mealtime Frequency with Bulimia Symptomatology. Eat. Disord. 2007, 15, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Loth, K.; Wall, M.; Choi, C.-W.; Bucchianeri, M.M.; Quick, V.; Larson, N.; Neumark-Sztainer, D. Family meals and disordered eating in adolescents: Are the benefits the same for everyone? Int. J. Eat. Disord. 2015, 48, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.L.; Fiese, B.H. Parent routines, child routines, and family demogrpahics associated with obesity in parents and preschool-aged children. Front. Psychol. 2014, 5. [Google Scholar] [CrossRef] [Green Version]
- Kitzman-Ulrich, H.; Wilson, D.K.; George, S.M.S.; Lawman, H.; Segal, M.; Fairchild, A. The Integration of a Family Systems Approach for Understanding Youth Obesity, Physical Activity, and Dietary Programs. Clin. Child Fam. Psychol. Rev. 2010, 13, 231–253. [Google Scholar] [CrossRef] [Green Version]
- Piazza-Waggoner, C.; Modi, A.C.; Ingerski, L.M.; Wu, Y.P.; Zeller, M.H.; Zeller, C.P.-W.C.M.M.I.P.W.H. Distress at the Dinner Table? Observed Mealtime Interactions among Treatment-Seeking Families of Obese Children. Child. Obes. 2011, 7, 385–391. [Google Scholar] [CrossRef] [Green Version]
- Sen, B.P. The relationship between frequency of family dinner and adolescent problem behaviors after adjusting for other family characteristics. J. Adolesc. 2010, 33, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, J.; Huet, C.; Dubé, L. Emotional reinforcement as a protective factor for healthy eating in home settings. Am. J. Clin. Nutr. 2011, 94, 254–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumark-Sztainer, D.; Wall, M.; Story, M.; Fulkerson, J.A. Are family meal patterns associated with disordered eating behaviors among adolescents? J Adolesc Health. 2004, 35, 350–359. [Google Scholar] [CrossRef]
- Spagnola, M.; Fiese, B.H. Family Routines and Rituals. Infants Young Child 2007, 20, 284–299. [Google Scholar] [CrossRef] [Green Version]
- Czaja, J.; Hartmann, A.; Rief, W.; Hilbert, A. Mealtime family interactions in home environments of children with loss of control eating. Appetite 2011, 56, 587–593. [Google Scholar] [CrossRef]
- Skeer, M.R.; Yantsides, K.E.; Eliasziw, M.; Tracy, M.R.; Carlton-Smith, A.R.; Spirito, A. Sociodemographic characteristics associated with frequency and duration of eating family meals: A cross-sectional analysis. SpringerPlus 2016, 5, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Fulkerson, J.A.; Story, M.T.; Mellin, A.; Leffert, N.; Neumark-Sztainer, D.; French, S.A. Family Dinner Meal Frequency and Adolescent Development: Relationships with Developmental Assets and High-Risk Behaviors. J. Adolesc. Health 2006, 39, 337–345. [Google Scholar] [CrossRef]
- Caraher, M.; Dixon, P.; Lang, T.; Carr-Hill, R. The state of cooking in England: The relationship of cooking skills to food choice. Br. Food J. 1999, 101, 590–609. [Google Scholar] [CrossRef]
- Smith, L.P.; Ng, S.W.; Popkin, B.M. Trends in US home food preparation and consumption: Analysis of national nutrition surveys and time use studies from 1965–1966 to 2007–2008. Nutr. J. 2013, 12, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sisson, S.B.; Sheffield-Morris, A.; Spicer, P.; Lora, K.; Latorre, C. Influence of family structure on obesogenic behaviors and placement of bedroom Tvs of American children: National survey of children’s health 2007. Prev. Med. 2014, 61, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Mancino, L.; Newman, C. Who has time to cook? May 2007; Report No. 40. Available online: https://www.ers.usda.gov/webdocs/publications/45797/11722_err40_1_.pdf?v=41056. (accessed on 12 October 2020).
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, 5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, D.B.; Birkett, D.; Evens, C.; Pickering, S. Promoting Family Meals in WIC: Lessons Learned from a Statewide Initiative. J. Nutr. Educ. Behav. 2006, 38, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Fulkerson, J.A.; Friend, S.; Flattum, C.; Horning, M.L.; Draxten, M.; Neumark-Sztainer, D.; Gurvich, O.; Story, M.T.; Garwick, A.; Kubik, M.Y. Promoting healthful family meals to prevent obesity: HOME Plus, a randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Robson, S.M.; Stough, C.O.; Stark, L.J. The impact of a pilot cooking intervention for parent-child dyads on the consumption of foods prepared away from home. Appetite 2016, 99, 177–184. [Google Scholar] [CrossRef]
- Miller, A.; Franzen-Castle, L.; Trina, A.; Krehbiel, M.; Colby, S.; Kattelmann, K.; Olfert, M.D.; Mathews, D.; White, A.A. Food-related behavior and intake of adult main meal preparers of 9–10 year-old children participating in iCook 4-H: A five-state childhood obesity prevention pilot study. Appetite 2016, 101, 163–170. [Google Scholar] [CrossRef] [Green Version]

| Author(s) and Year | Reference Number | Sample | Main Outcomes | Study Design |
|---|---|---|---|---|
| Diet Quality & Meal Patterns | ||||
| Ayala et al. (2007) | [25] | 167 Mexican American children, 8–18 years old and their mothers | Number of family meals positively associated with fiber intake. | Cross-Sectional |
| Burgess-Champoux et al. (2009) | [15] | 677 adolescents, Project EAT | Five or more family meals per week associated with increased sodium intake for females, but not males. Five or more family meals per week during the first wave of the study was associated with frequency of breakfast, lunch, and dinner meals for males, and only breakfast and dinner for females five year later. | Longitudinal |
| Burke et al. (2007) | [40] | 594 Irish children, 5–12 years | Reported fiber and micronutrient intake were higher during eating occasions inside the home compared to outside of the home. | Cross-Sectional |
| Chu et al. (2014) | [38] | 3398 Canadian children, 10–11 years | Higher frequency of involvement in home meal preparation was associated with higher diet quality index scores. Children who were involved in meal preparation daily ate 1 more serving/day of vegetables and fruit compared with children who never helped. | Cross-Sectional |
| Fink et al. (2014) | [18] | 1992 children (age 0 to 19 years) | Five or more family meals per week associated with less sugar-sweetened beverage intake among younger and older children, greater vegetable intake among older children and adolescents, and greater fruit intake among adolescents. | Cross-Sectional |
| Fitzpatrick et al. (2007) | [19] | 1336 parents of children aged 1–4 participating in WIC | Number of days per week the family ate dinner together was positively associated with serving fruit and serving vegetables. | Cross-Sectional |
| Flores et al. (2005) | [43] | 2608 parents of children ages 4–35 months | Minority children less likely than whites to have consistent mealtimes, and more likely to never eat lunch or dinner with their families. The analyses also addressed home safety practices for young children, and found disparities with fewer practices in minority homes. | Cross-sectional |
| Fulkerson et al. (2009) | [14] | Racially diverse sample of 145 adolescents who attended alternative high school | Family dinner frequency was positively associated with breakfast consumption and fruit intake. | Cross-Sectional |
| Fulkerson et al. (2014) | [12] | Child, adolescent, or adult samples with findings related to family meals or commensal eating | Studies included in review found associations between family meal frequency and intake of fruits and vegetables, micronutrients, and breakfast, and decreased intake of soda, higher-fat foods, unhealthy snacks and cakes, fried foods, and fast food. | Systematic Review |
| Gillman et al. (2000) | [44] | 16,202 youth aged 9–14 | Eating family dinner was associated with consuming more fruits and vegetables, less fried food and soda, less saturated and trans-fat, lower glycemic load, more fiber and micronutrients from food, and no material differences in red meat or snack foods. | Cross-Sectional |
| Haapalahti et al. (2003) | [39] | 404 Finnish children aged 10–11 | Children who ate family dinner regularly consumed less fast food and sweets but more juice than children who did not have regular family dinners. | Cross-Sectional |
| Hammons and Fiese (2011) | [45] | 182,836 children and adolescents across 17 studies | Children and adolescents who ate meals with family 3 or more times per week had healthier dietary patterns than those who ate fewer than 3 meals with family per week. | Meta-Analysis |
| Larson et al. (2006) | [36] | 1710 young adults aged 18–23, Project EAT | Young adults who reported frequent food preparation reported less frequent fast-food use and were more likely to meet dietary objectives for fat, calcium, fruit, vegetable, and whole-grain consumption. | Cross-Sectional |
| Larson et al. (2007) | [37] | 1710 young adults aged 18–23, Project EAT | Family meal frequency during adolescence predicted higher intakes of fruit, vegetables, dark-green and orange vegetables, and key nutrients and lower intakes of soft drinks during young adulthood. | Longitudinal |
| Martin-Biggers et al. (2014) | [46] | Families (with children) | More frequent family meals are associated with greater consumption of healthy foods in children, adolescents, and adults. Adolescents and children who consume fewer family meals consume more unhealthy food. | Literature Review |
| Naska et al. (2015) | [42] | 23,162 middle-aged European adults | Those who ate more foods outside of the home consumed more sweet and savoury bakery items, soft drinks, juices and other non-alcoholic beverages than those who ate more at home | Cross-Sectional |
| Neumark-Sztainer et al. (2003) | [13] | 4746 adolescents, Project EAT | Frequency of family meals was positively associated with intake of fruits, vegetables, grains, and calcium-rich foods and negatively associated with soft drink intake. Frequency of family meals was associated with consumption of energy, protein, calcium, iron, folate, fiber, and vitamins A, C, E, and B6. | Cross-Sectional |
| O’Dwyer et al. (2005) | [10] | 958 Irish adults aged 18–64 | Intakes of fiber, micronutrients, calories, protein, fat and carbohydrates were greater at home than away from home. | Cross-Sectional |
| Patrick and Nicklas (2005) | [47] | Families (with children) | Children who eat meals with their families generally consume more healthy foods and nutrients. Eating out is associated with higher intake of fat and calories than eating at home. | Literature Review |
| Poti and Popkin (2011) | [48] | 29,217 children aged 2–18 (national sample) | Between 1977 and 2006, children had an overall increase in energy intake corresponding with a decrease in frequency of eating at home (compared to outside of the home). | Longitudinal |
| Surjadi et al. (2017) | [49] | 6503 children were followed from kindergarten–eighth grade | Family meals in kindergarten and increase in family meal frequency over time both predicted healthier dietary intake in eighth grade among White and Black adolescents, but not among Hispanic or Asian adolescents. | Longitudinal |
| Sweetman et al. (2011) | [41] | 434 children aged 2–5 | Frequency of family mealtimes was unrelated to vegetable consumption or liking. | Cross-Sectional |
| Utter et al. (2008) | [50] | 3245 adolescents (national sample) | Frequency of family meals was associated with consuming five fruits and vegetables per day, eating breakfast, and bringing lunch from home. | Cross-Sectional |
| Videon and Manning (2003) | [51] | 18,177 adolescents (national sample) | Parental presence at family meals was associated with greater consumption of fruits, vegetables, dairy foods, and breakfast. | Cross-Sectional |
| Woodruff and Hanning (2008) | [52] | Families (with adolescent children) | Family meals were generally associated with improved dietary intake. | Systematic Review |
| Woodruff & Hanning (2009) | [53] | 3223 Canadian middle school students | Frequency of family meals was associated with breakfast consumption and decreased consumption of soft drinks. | Cross-Sectional |
| Author(s) and Year | Reference Number | Sample | Main Outcomes | Study Design |
|---|---|---|---|---|
| Psychosocial Outcomes | ||||
| Eisenberg et al. (2004) | [5] | 4746 adolescents, Project EAT | Frequency of family meals was related to decreased risk for depressive symptoms, low GPA, suicide involvement, and tobacco, alcohol, and marijuana use after controlling for family connectedness. | Cross-Sectional |
| Eisenberg et al. (2008) | [7] | 806 adolescents, Project EAT | Family meal frequency at age 12 was associated with lower odds of smoking, alcohol use, and marijuana use at age 17 for females. Family meals were not associated with substance use for males. | Longitudinal |
| Franko et al. (2008) | [28] | 2379 females tracked annually from age 9–19 | More frequent family meals from ages 9–11 predicted lower likelihood of smoking during adolescence. | Longitudinal |
| Fulkerson et al. (2009) | [14] | Racially diverse sample of 145 adolescents who attended alternative high school | Family dinner frequency was negatively associated with depressive symptoms. | Cross-Sectional |
| Goldfarb et al. (2014) | [6] | Adolescents | Family meals were associated with decreased risk for alcohol and marijuana use, sexual activity, depression and suicidal behaviors and ideation, violence and delinquency, and increased overall wellbeing, but these associations were less likely to be statistically significant when measures of family connectedness were included. | Systematic Review |
| Lu et al. (2011) | [67] | 160 non-obese adult women | Meals eaten at home were followed by less worry and more positive emotions than meals eaten away from home. | Observational |
| Neumark-Sztainer et al. (2004) | [68] | 4746 adolescents, Project EAT | Adolescents who reported frequent family meals, high priority for family meals, and more structure in family meal environment were less likely to engage in disordered eating. | Longitudinal |
| Sen (2010) | [66] | 6748 children aged 12–16 (national sample) | Frequency of family meals was related to decreased substance use and running away for females, and decreased incidence of drinking, physical violence, property destruction, stealing, and running away from home for males. | Cross-Sectional |
| Skeer and Ballard (2013) | [57] | Families with adolescent children | Frequent family meals were associated with decreased substance use, aggressive and violent behavior, poor school performance, sexual behavior, mental health problems, and disordered eating behaviors. | Literature Review |
| Author(s) and Year | Reference Number | Sample | Main Outcomes | Study Design |
|---|---|---|---|---|
| Family Relationships | ||||
| Czaja et al. (2011) | [70] | 74 families with children aged 8–13 | Children who demonstrated loss of control eating were more likely to come from families that had less healthy patterns of communication, interpersonal involvement, and family functioning during an observed family meal than children who did not have loss of control eating. | Observational |
| Fiese et al. (2012) | [32] | 200 families with children aged 5–12 | Families with overweight or obese children spent less time on a family meal and spent less time in positive communication than families with children of a healthy weight. | Observational |
| Fiese (2006) | [69] | Families with children | Family meals are one family routine that promote health and wellbeing, in part through the positive contributions they make to family relationships and functioning. | Review/Synthesis |
| Franko et al. (2008) | [28] | 2379 females tracked annually from age 9–19 | More frequent family meals from ages 9–11 predicted greater family cohesion and coping skills when children were 18–19 years old. | Longitudinal |
| Fulkerson et al. (2006) | [72] | 902 adolescents, Project EAT | Adolescents and parents both reported high levels of communication and enjoyment of family meals. Younger adolescents reported higher importance of eating together than older adolescents. | Cross-Sectional |
| Fulkerson et al. (2010) | [26] | 4750 racially diverse, low-income adolescents | Frequency of family meals was associated with adolescent perceptions of parent–child communication over time. | Longitudinal |
| Welsh et al. (2011) | [54] | 152 adults and 75 adolescents from 90 households | Family meal frequency was positively correlated with perceived family cohesion. | Cross-Sectional |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glanz, K.; Metcalfe, J.J.; Folta, S.C.; Brown, A.; Fiese, B. Diet and Health Benefits Associated with In-Home Eating and Sharing Meals at Home: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1577. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041577
Glanz K, Metcalfe JJ, Folta SC, Brown A, Fiese B. Diet and Health Benefits Associated with In-Home Eating and Sharing Meals at Home: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(4):1577. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041577
Chicago/Turabian StyleGlanz, Karen, Jessica J. Metcalfe, Sara C. Folta, Alison Brown, and Barbara Fiese. 2021. "Diet and Health Benefits Associated with In-Home Eating and Sharing Meals at Home: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 4: 1577. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041577