
Clinical Knowledge Supported Acute Kidney Injury (AKI) Risk Assessment Model for Elderly Patients


Abstract
:1. Introduction
- (1)
- explore the interrelationships between the risk factors that might induce AKI in elderly patients;
- (2)
- identify the relative influence of each criterion on the risk assessment of AKI;
- (3)
- provide precautionary guidance for elderly patients to reduce their potential AKI. risk.
2. Materials and Research Methods
2.1. Materials
2.2. Research Methods
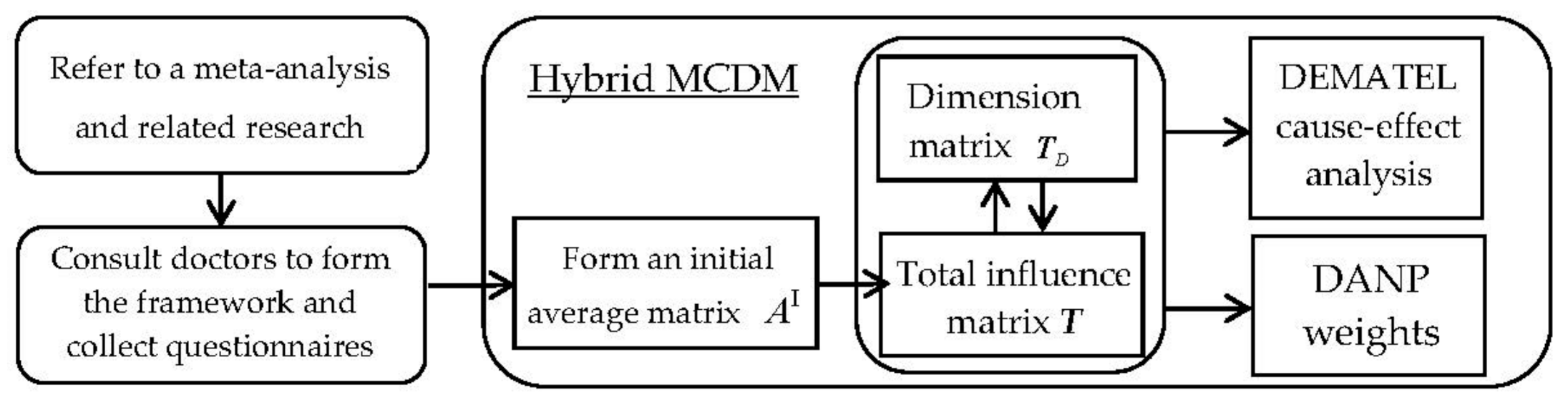
2.2.1. DEMATEL Technique
2.2.2. DEMATEL-Based ANP (DANP)
3. AKI Risk Assessment Model for Elderly Patients
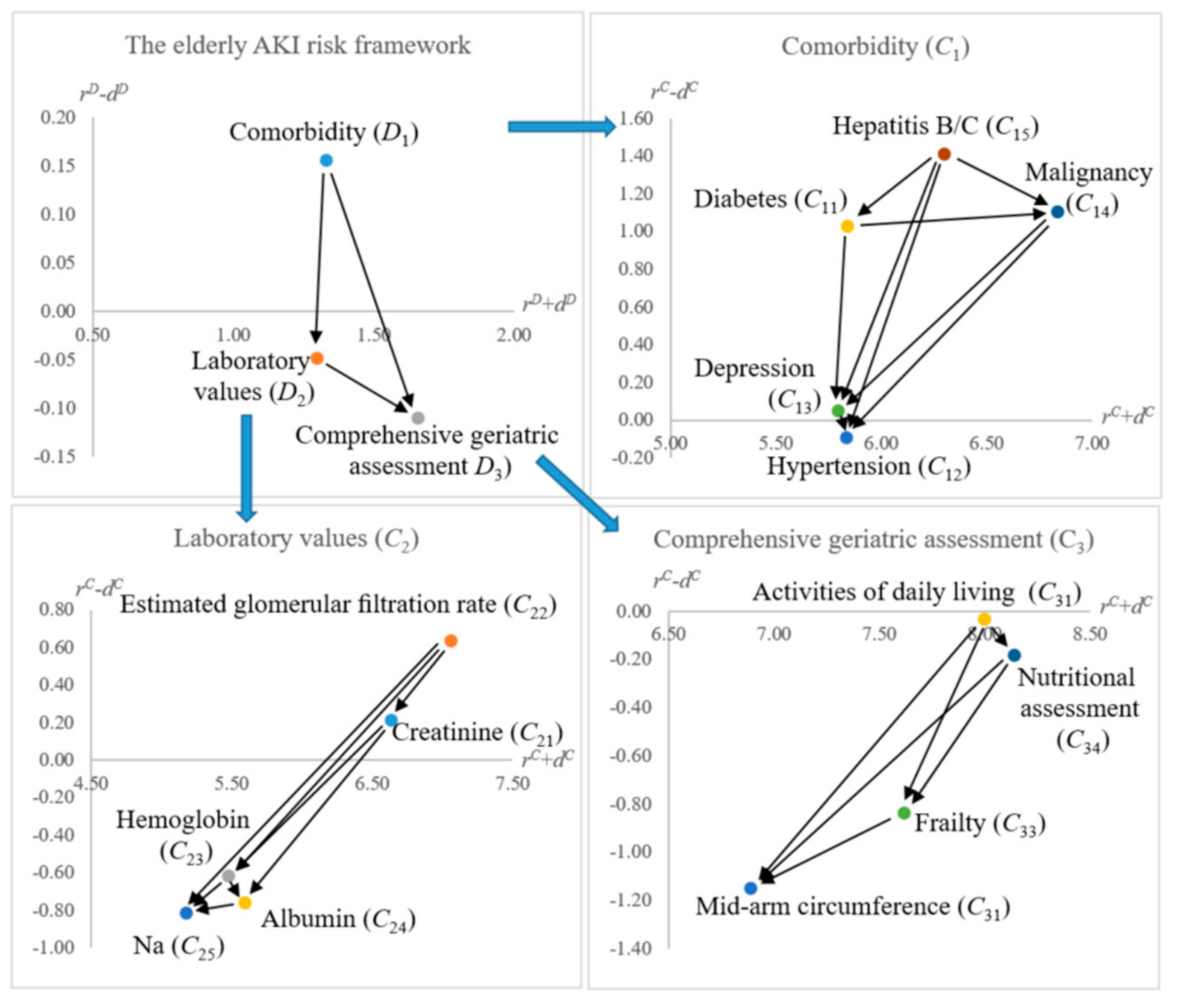
3.1. DEMATEL Analysis
3.2. DEMATEL-Based ANP (DANP) Weights
4. Discussions
5. Conclusions
- (1)
- Identified the influential relationships among the AKI risk assessment model for elderly patients.
- (2)
- Obtained the influential weights of the AKI evaluation criteria from ten experienced doctors.
- (3)
- Proposed a flexible method (experience-based weighting) to follow a hospital’s policy to form a decision support system (or termed as a knowledge-based system).
- (4)
- This study has shed light on integrating multiple research approaches (e.g., statistics and MCDM) to assist medical decision-making in practice.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| D1 | D2 | D3 | |
|---|---|---|---|
| D1 | 0.197 | 0.239 | 0.307 |
| D2 | 0.163 | 0.196 | 0.266 |
| D3 | 0.226 | 0.237 | 0.309 |
| C11 | C12 | C13 | C14 | C15 | C21 | C22 | C23 | C24 | C25 | C31 | C32 | C33 | C34 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C11 | 0.036 | 0.053 | 0.051 | 0.048 | 0.049 | 0.046 | 0.043 | 0.047 | 0.046 | 0.044 | 0.055 | 0.054 | 0.051 | 0.054 |
| C12 | 0.065 | 0.049 | 0.059 | 0.056 | 0.053 | 0.064 | 0.059 | 0.059 | 0.054 | 0.070 | 0.062 | 0.063 | 0.059 | 0.062 |
| C13 | 0.059 | 0.054 | 0.045 | 0.065 | 0.057 | 0.053 | 0.055 | 0.054 | 0.053 | 0.051 | 0.062 | 0.062 | 0.069 | 0.061 |
| C14 | 0.059 | 0.061 | 0.058 | 0.045 | 0.066 | 0.053 | 0.059 | 0.054 | 0.053 | 0.051 | 0.059 | 0.062 | 0.063 | 0.061 |
| C15 | 0.047 | 0.047 | 0.052 | 0.051 | 0.040 | 0.046 | 0.046 | 0.047 | 0.054 | 0.045 | 0.055 | 0.051 | 0.051 | 0.054 |
| C21 | 0.068 | 0.070 | 0.068 | 0.065 | 0.065 | 0.048 | 0.068 | 0.067 | 0.064 | 0.076 | 0.063 | 0.063 | 0.063 | 0.063 |
| C22 | 0.068 | 0.070 | 0.068 | 0.065 | 0.065 | 0.069 | 0.049 | 0.067 | 0.064 | 0.076 | 0.063 | 0.063 | 0.063 | 0.063 |
| C23 | 0.065 | 0.056 | 0.059 | 0.067 | 0.064 | 0.067 | 0.066 | 0.048 | 0.061 | 0.056 | 0.060 | 0.060 | 0.060 | 0.060 |
| C24 | 0.062 | 0.064 | 0.068 | 0.064 | 0.070 | 0.063 | 0.065 | 0.075 | 0.054 | 0.058 | 0.062 | 0.062 | 0.062 | 0.062 |
| C25 | 0.059 | 0.062 | 0.058 | 0.061 | 0.058 | 0.066 | 0.065 | 0.056 | 0.069 | 0.047 | 0.059 | 0.059 | 0.059 | 0.059 |
| C31 | 0.103 | 0.101 | 0.106 | 0.102 | 0.101 | 0.103 | 0.105 | 0.105 | 0.101 | 0.107 | 0.080 | 0.095 | 0.105 | 0.104 |
| C32 | 0.103 | 0.101 | 0.099 | 0.099 | 0.102 | 0.103 | 0.102 | 0.106 | 0.106 | 0.096 | 0.105 | 0.078 | 0.105 | 0.105 |
| C33 | 0.107 | 0.106 | 0.106 | 0.106 | 0.105 | 0.110 | 0.110 | 0.110 | 0.105 | 0.112 | 0.109 | 0.114 | 0.082 | 0.109 |
| C34 | 0.099 | 0.105 | 0.102 | 0.105 | 0.104 | 0.109 | 0.109 | 0.104 | 0.113 | 0.111 | 0.107 | 0.113 | 0.108 | 0.083 |
References
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Berk, R.A.; Adler, D.A. Statistical assumptions as empirical commitments. In Law, Punishment, and Social Control: Essays in Honor of Sheldon Messinger, 2nd ed.; Aldine de Gruyter: New York, NY, USA, 2003; pp. 235–254. [Google Scholar]
- Shen, K.Y.; Zavadskas, E.K.; Tzeng, G.H. Updated discussions on ‘Hybrid multiple criteria decisionmaking methods: A review of applications for sustainability issues’. Econ. Res. Ekon. Istraživanja 2018, 31, 1437–1452. [Google Scholar] [CrossRef]
- Stojčić, M.; Zavadskas, E.K.; Pamučar, D.; Stević, Ž.; Mardani, A. Application of MCDM methods in sustainability engineering: A literature review 2008–2018. Symmetry 2019, 11, 350. [Google Scholar] [CrossRef] [Green Version]
- Zavadskas, E.K.; Turskis, Z.; Kildienė, S. State of art surveys of overviews on MCDM/MADM methods. Technol. Econ. Dev. Econ. 2014, 20, 165–179. [Google Scholar] [CrossRef] [Green Version]
- Greco, S.; Figueira, J.; Ehrgott, M. Multiple Criteria Decision Analysis-State of the Art Surveys; Springer: New York, NY, USA, 2016. [Google Scholar]
- Gabus, A.; Fontela, E. World Problems, An Invitation to Further Thought within The Framework of DEMATEL; Geneva Research Centre of the Battelle Memorial Institute: Geneva, Switzerland, 1972. [Google Scholar]
- Lee, H.S.; Tzeng, G.H.; Yeih, W.; Wang, Y.J.; Yang, S.C. Revised DEMATEL: Resolving the infeasibility of DEMATEL. Appl. Math. Model. 2013, 37, 6746–6757. [Google Scholar] [CrossRef]
- Saaty, T.L. The Analytic Network Process; RWS Publications: Pittsburgh, PA, USA, 1996. [Google Scholar]
- Shen, K.Y.; Yan, M.R.; Tzeng, G.H. Combining VIKOR-DANP model for glamor stock selection and stock performance improvement. Knowl. Based Syst. 2014, 58, 86–97. [Google Scholar] [CrossRef]
- Khan, S.; Maqbool, A.; Haleem, A.; Khan, M.I. Analyzing critical success factors for a successful transition towards circular economy through DANP approach. Manag. Environ. Qual. Int. J. 2020, 31, 505–529. [Google Scholar] [CrossRef]
- Landoni, G.; Bove, T.; Székely, A.; Comis, M.; Rodseth, R.; Pasero, D.; Ponschab, M.; Mucchetti, M.; Azzolini, M.L.; Caramelli, F.; et al. Reducing mortality in acute kidney injury patients: Systematic review and international web-based survey. J. Cardiothorac. Vasc. Anesthesia 2013, 27, 1384–1398. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Lameire, N.; KDIGO AKI Guideline Work Group. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO Summary (Part 1). Crit. Care 2013, 17, 204–215. [Google Scholar] [CrossRef] [Green Version]
- Jiesisibieke, Z.L.; Tung, T.H.; Xu, Q.Y.; Chen, P.E.; Hsu, S.Y.; Liu, Y.; Chien, C.W. Association of acute kidney injury with frailty in elderly population: A systematic review and meta-analysis. Ren. Fail. 2019, 41, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.L.; Lin, M.J. Group Decision Making under Multiple Criteria: Methods and Applications; Springer: Berlin/Heidelberg, Germany, 2012; Volume 281. [Google Scholar]
- Bigna, J.J.R.; Um, L.N.; Nansseu, J.R.N. A comparison of quality of abstracts of systematic reviews including meta-analysis of randomized controlled trials in high-impact general medicine journals before and after the publication of PRISMA extension for abstracts: A systematic review and meta-analysis. Syst. Rev. 2016, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Kader, K.; Girard, T.D.; Brummel, N.E.; Saunders, C.T.; Blume, J.D.; Clark, A.J.; Vincz, A.J.; Ely, E.W.; Jackson, J.C.; Bell, S.P.; et al. Acute kidney injury and subsequent frailty status in survivors of critical illness: A secondary analysis. Critical Care Medicine 2018, 46, e380. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.H.; Lee, S.W.; Kim, S.-W.; Ahn, S.Y.; Yu, M.-Y.; Kim, K.-I.; Chin, H.J.; Na, K.Y.; Chae, N.-W.; Kim, S. Frailty as a predictor of acute kidney injury in hospitalized elderly patients: A single center, retrospective cohort study. PLoS ONE 2016, 11, e0156444. [Google Scholar] [CrossRef] [PubMed]
- Morton, S.; Isted, A.; Avery, P.; Wang, J. Is frailty a predictor of outcomes in elderly inpatients with acute kidney injury? A prospective cohort study. Am. J. Med. 2018, 131, 1251–1256.e2. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.; Phelan, H.; Hassan, A.; Orouji Jokar, T.; O’Keeffe, T.; Azim, A.; Gries, L.; Kulvatunyou, N.; Latifi, R.; Rhee, P. The impact of frailty on failure-to-rescue in geriatric trauma patients: A prospective study. J. Trauma Acute Care Surg. 2016, 81, 1150–1155. [Google Scholar] [CrossRef]
- Esterhuizen, T.M.; Thabane, L. Con: Meta-analysis: Some key limitations and potential solutions. Nephrol. Dial. Transplant. 2016, 31, 882–885. [Google Scholar] [CrossRef] [Green Version]
- Kashani, K.B.; Macedo, E.; Burdmann, E.A.; Hooi, L.S.; Khullar, D.; Bagga, A.; Chakravarthi, R.; Mehta, R. Acute kidney injury risk assessment: Differences and similarities between resource-limited and resource-rich countries. Kidney Int. Rep. 2017, 2, 519–529. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Thokala, P.; Devlin, N.; Marsh, K.; Baltussen, R.; Boysen, M.; Kalo, Z.; Longrenn, T.; Mussen, F.; Peacock, S.; Watkins, J.; et al. Multiple criteria decision analysis for health care decision making—an introduction: Report 1 of the ISPOR MCDA Emerging Good Practices Task Force. Value Health 2016, 19, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Hansen, P.; Hendry, A.; Naden, R.; Ombler, F.; Stewart, R. A new process for creating points systems for prioritising patients for elective health services. Clin. Governance: Int. J. 2012, 17, 200–209. [Google Scholar] [CrossRef]
- Johnson, S.R.; Naden, R.P.; Fransen, J.; Hoogen, F.V.D.; Pope, J.E.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Denton, C.P.; Distler, O.; et al. Multicriteria decision analysis methods with 1000Minds for developing systemic sclerosis classification criteria. J. Clin. Epidemiol. 2014, 67, 706–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Dolan, J. Shared decision-making—Transferring research into practice: The analytic hierarchy process (AHP). Patient Educ. Couns. 2008, 73, 418–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, L.D.; Fasolo, B.; Zafiropoulos, N.; Beyer, A. Is quantitative benefit–risk modelling of drugs desirable or possible? Drug Discov. Today 2011, 8, e3–e10. [Google Scholar] [CrossRef] [PubMed]
- Heiman, G.W. Research Methods in Psychology, 3rd ed.; Houghton Mifflin Company: Boston, MA, USA; New York, NY, USA, 2002. [Google Scholar]


| Ref | Country | Database Source | Research Subjects | Mean Age of Research Subjects | Duration | Key Findings |
|---|---|---|---|---|---|---|
| [18] | USA | Pubmed | 243 AKI 74 non-AKI | 57 (AKI) 56 (non-AKI) | 2007–2010 (4 years) | AKI was associated with higher frailty (Clinical Frailty Scale). |
| [19] | Korea | Pubmed | 183 (mild frail) 199 (moderate frail) 152 (severe frail) | 73.8 (mild frail) 76.5 (moderate frail) 79.0 (severe frail) | 2013 (1 year) | The frailest group indicated the highest AKI risk compared with the other groups. |
| [20] | UK | Pubmed | 31 AKI 133 non-AKI | 82.6 (AKI) 81.2 (non-AKI) | 2 weeks | Severe frailty was associated with AKI significantly (p = 0.01). |
| [21] | USA | Pubmed | 93 (non-frail) 139 (pre-frail) 136 (frail) | 68.52 (non-frail) 74.71 (pre-frail) 78.83 (frail) | 2013–2014 (2 years) | Frail patients were more likely to induce AKI (p = 0.03). |
| Dimensions | Criteria | Reference |
|---|---|---|
| Diabetes (C11) | [19,20] | |
| Hypertension (C12) | [19,20] | |
| Comorbidity | Depression (C13) | (from the doctors) |
| (D1) | Malignancy (C14) | [19,20] |
| Hepatitis B/C (C15) | (from the doctors) | |
| Creatinine (C21) | [19,20] | |
| Estimated glomerular filtration rate (C22) | [19] | |
| Laboratory Values | Hemoglobin (C23) | [19] |
| (D2) | Albumin (C24) | [19] |
| Na (C25) | [19] | |
| Comprehensive | Activities of daily living (C31) | [19] |
| Geriatric | Mid-arm circumference (C32) | [19] |
| Assessments | Frailty (C33) | [15,18,19,20,21] |
| (D3) | Nutritional assessment (C34) | [19] |
| C11 | C12 | C13 | C14 | C15 | C21 | C22 | C23 | C24 | C25 | C31 | C32 | C33 | C34 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C11 | 0.00 | 4.00 | 3.00 | 3.00 | 2.00 | 3.00 | 3.00 | 3.00 | 2.00 | 2.00 | 3.00 | 3.00 | 3.00 | 2.00 |
| C12 | 2.00 | 0.00 | 1.00 | 2.00 | 1.00 | 4.00 | 4.00 | 2.00 | 3.00 | 3.00 | 2.00 | 2.00 | 2.00 | 2.00 |
| C13 | 2.00 | 2.00 | 0.00 | 2.00 | 2.00 | 2.00 | 2.00 | 1.00 | 2.00 | 1.00 | 4.00 | 3.00 | 3.50 | 3.00 |
| C14 | 2.00 | 2.00 | 4.00 | 0.00 | 2.50 | 3.00 | 3.00 | 4.00 | 3.00 | 3.00 | 4.00 | 3.50 | 4.00 | 4.00 |
| C15 | 2.00 | 1.00 | 2.00 | 4.00 | 0.00 | 3.00 | 3.00 | 3.00 | 4.00 | 2.00 | 4.00 | 4.00 | 4.00 | 4.00 |
| C21 | 1.00 | 2.50 | 1.00 | 1.00 | 1.00 | 0.00 | 4.00 | 4.00 | 3.00 | 4.00 | 3.50 | 3.50 | 4.00 | 4.00 |
| C22 | 1.00 | 2.50 | 2.00 | 3.00 | 1.50 | 4.00 | 0.00 | 4.00 | 3.50 | 4.00 | 4.00 | 3.50 | 4.00 | 4.00 |
| C23 | 1.00 | 1.50 | 1.00 | 1.00 | 1.00 | 2.00 | 2.00 | 0.00 | 3.00 | 1.00 | 3.00 | 3.00 | 3.00 | 2.50 |
| C24 | 1.00 | 1.00 | 1.00 | 1.00 | 2.00 | 1.00 | 1.00 | 1.00 | 0.00 | 2.00 | 3.00 | 3.50 | 3.00 | 4.00 |
| C25 | 1.00 | 3.00 | 1.00 | 1.00 | 1.00 | 3.00 | 3.00 | 1.00 | 1.00 | 0.00 | 2.00 | 1.00 | 2.00 | 2.00 |
| C31 | 4.00 | 4.00 | 4.00 | 3.50 | 4.00 | 2.00 | 2.00 | 2.00 | 2.00 | 2.00 | 0.00 | 4.00 | 4.00 | 4.00 |
| C32 | 2.00 | 2.00 | 2.00 | 2.00 | 1.50 | 2.00 | 2.00 | 2.00 | 2.00 | 2.00 | 2.00 | 0.00 | 4.00 | 4.00 |
| C33 | 2.00 | 2.00 | 4.00 | 3.00 | 2.00 | 2.00 | 2.00 | 2.00 | 2.00 | 2.00 | 4.00 | 4.00 | 0.00 | 4.00 |
| C34 | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 | 4.00 | 4.00 | 4.00 | 0.00 |
| Dimensions | Criteria | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| C11 | 3.44 | 2.40 | 5.84 | 1.03 | |||||
| C12 | 2.87 | 2.96 | 5.83 | −0.09 | |||||
| D1 | 0.74 | 0.59 | 1.33 | 0.16 | C13 | 2.92 | 2.87 | 5.80 | 0.05 |
| C14 | 3.97 | 2.86 | 6.83 | 1.11 | |||||
| C15 | 3.85 | 2.44 | 6.29 | 1.41 | |||||
| C21 | 3.43 | 3.21 | 6.63 | 0.22 | |||||
| C22 | 3.85 | 3.21 | 7.06 | 0.64 | |||||
| D2 | 0.63 | 0.67 | 1.30 | −0.05 | C23 | 2.43 | 3.05 | 5.48 | −0.62 |
| C24 | 2.42 | 3.17 | 5.59 | −0.76 | |||||
| C25 | 2.18 | 2.99 | 5.17 | −0.81 | |||||
| C31 | 3.98 | 4.01 | 8.00 | −0.03 | |||||
| D3 | 0.77 | 0.88 | 1.66 | −0.11 | C32 | 2.87 | 4.02 | 6.89 | −1.15 |
| C33 | 3.39 | 4.22 | 7.61 | −0.83 | |||||
| C34 | 3.98 | 4.16 | 8.14 | −0.18 |
| D1 | D2 | D3 | |
|---|---|---|---|
| D1 | 0.27 | 0.32 | 0.41 |
| D2 | 0.26 | 0.31 | 0.43 |
| D3 | 0.29 | 0.31 | 0.40 |
| Dimensions | Dimensional Weights | Criteria | DANP Weights (%) |
|---|---|---|---|
| C11 | 4.92 | ||
| C12 | 6.00 | ||
| Comorbidity | 27.53% | C13 | 5.83 |
| (D1) | C14 | 5.80 | |
| C15 | 4.98 | ||
| C21 | 6.45 | ||
| Laboratory | C22 | 6.46 | |
| Values | 31.31% | C23 | 6.06 |
| (D2) | C24 | 6.34 | |
| C25 | 5.99 | ||
| Comprehensive | C31 | 10.05 | |
| Geriatric | 41.17% | C32 | 10.04 |
| Assessments | C33 | 10.59 (1st) | |
| (D3) | C34 | 10.48 (2nd) |
| DANP | C11 | C12 | C13 | C14 | C15 | C21 | C22 | C23 | C24 | C25 | C31 | C32 | C33 | C34 | Risk Level | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weights (%) | 4.92 | 6.00 | 5.83 | 5.80 | 4.98 | 6.45 | 6.46 | 6.06 | 6.34 | 5.99 | 10.05 | 10.04 | 10.59 | 10.48 | |||
| A | 9.00 | 8.00 | 8.00 | 2.00 | 1.00 | 6.00 | 5.00 | 4.00 | 6.00 | 7.00 | 8.00 | 8.00 | 9.00 | 6.00 | 6.50 | ||
| B | 2.00 | 7.00 | 8.00 | 2.00 | 1.00 | 4.00 | 3.00 | 4.00 | 5.00 | 7.00 | 5.00 | 8.00 | 7.00 | 5.00 | 5.16 | ||
| C | 7.00 | 6.00 | 2.00 | 2.00 | 1.00 | 5.00 | 2.00 | 3.00 | 2.00 | 4.00 | 7.00 | 5.00 | 5.00 | 5.00 | 4.25 | ||
| Groups | Clinical Experience | Number of Doctors | Weighting |
|---|---|---|---|
| G1 | >15 years | 1 | 50% |
| G2 | 10 to 15 years | 5 | 30% |
| G3 | <10 years | 4 | 20% |
| Original | C11 | C12 | C13 | C14 | C15 | C21 | C22 | C23 | C24 | C25 | C31 | C32 | C33 | C34 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DANP (%) | 4.92 | 6.00 | 5.83 | 5.80 | 4.98 | 6.45 | 6.46 | 6.06 | 6.34 | 5.99 | 10.05 | 10.04 | 10.59 | 10.48 |
| (Rank) | (14th) | (9th) | (11th) | (12th) | (13th) | (6th) | (5th) | (8th) | (7th) | (10th) | (3rd) | (4th) | (1st) | (2nd) |
| Re-calculated DANP (%) | 4.96 | 5.89 | 6.00 | 5.23 | 4.58 | 6.41 | 6.41 | 6.03 | 6.42 | 6.20 | 10.28 | 10.16 | 10.87 | 10.57 |
| (Rank) | (13th) | (11th) | (10th) | (12th) | (14th) | (6th) | (7th) | (9th) | (5th) | (8th) | (3rd) | (4th) | (1st) | (2nd) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, K.-Y.; Chuang, Y.-C.; Tung, T.-H. Clinical Knowledge Supported Acute Kidney Injury (AKI) Risk Assessment Model for Elderly Patients. Int. J. Environ. Res. Public Health 2021, 18, 1607. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041607
Shen K-Y, Chuang Y-C, Tung T-H. Clinical Knowledge Supported Acute Kidney Injury (AKI) Risk Assessment Model for Elderly Patients. International Journal of Environmental Research and Public Health. 2021; 18(4):1607. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041607
Chicago/Turabian StyleShen, Kao-Yi, Yen-Ching Chuang, and Tao-Hsin Tung. 2021. "Clinical Knowledge Supported Acute Kidney Injury (AKI) Risk Assessment Model for Elderly Patients" International Journal of Environmental Research and Public Health 18, no. 4: 1607. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041607