
Development International Classification of Functioning, Disability and Health Core Set for Post Total Knee Replacement Rehabilitation Program: Delphi-Based Consensus Study in Taiwan

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
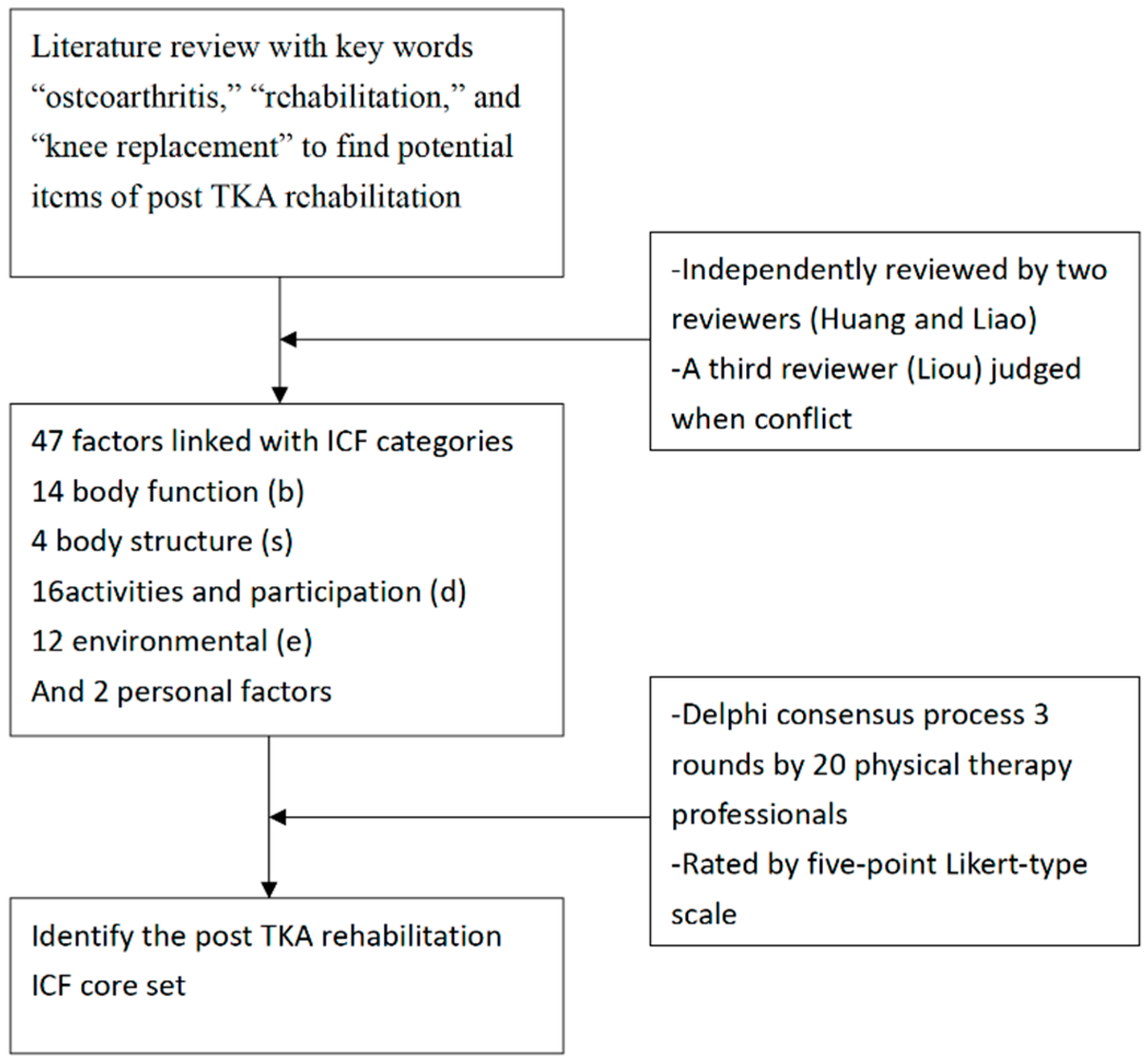
2.1. Study Design and Selection of ICF Categories
2.2. Consensus Procedure
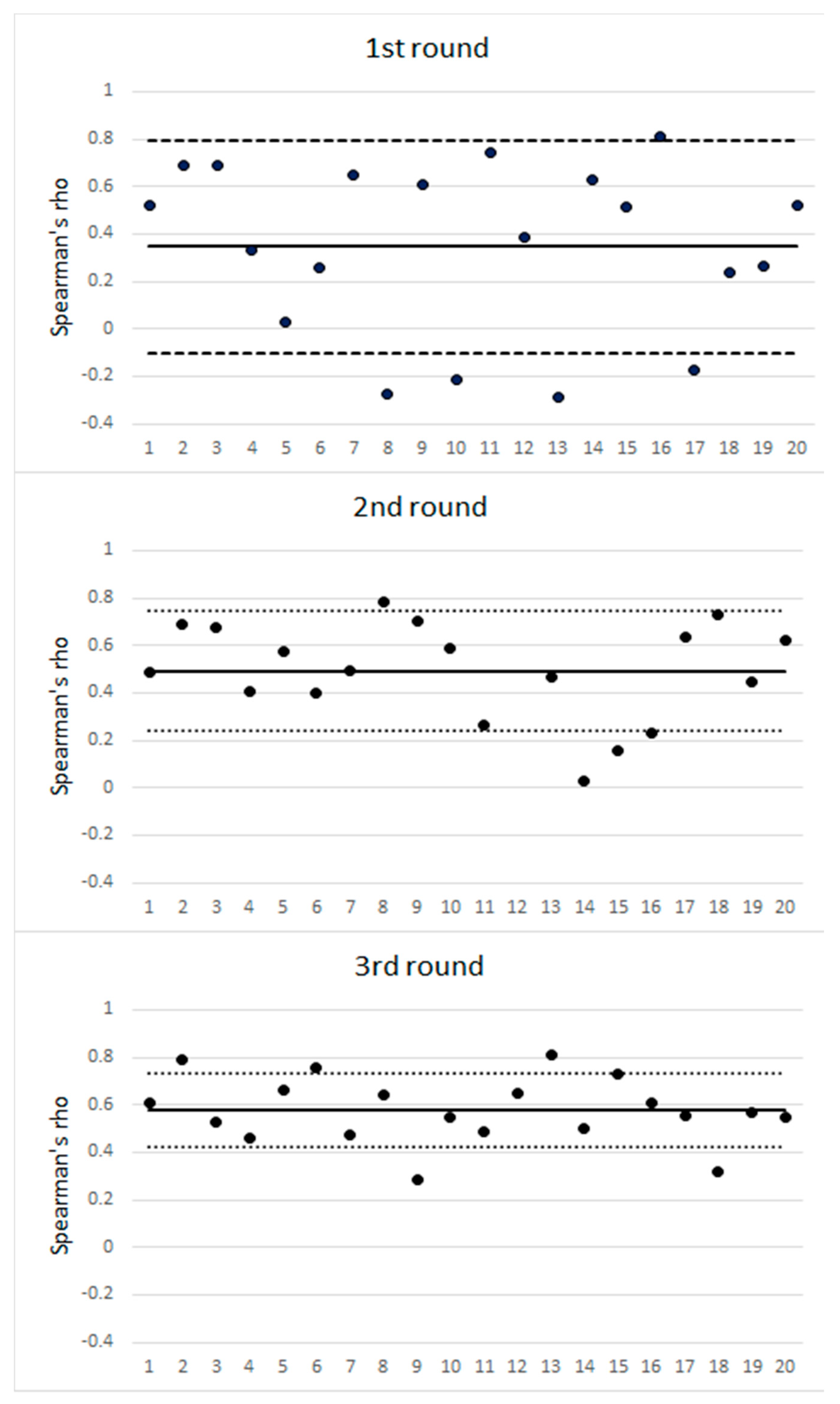
2.3. Data Analysis
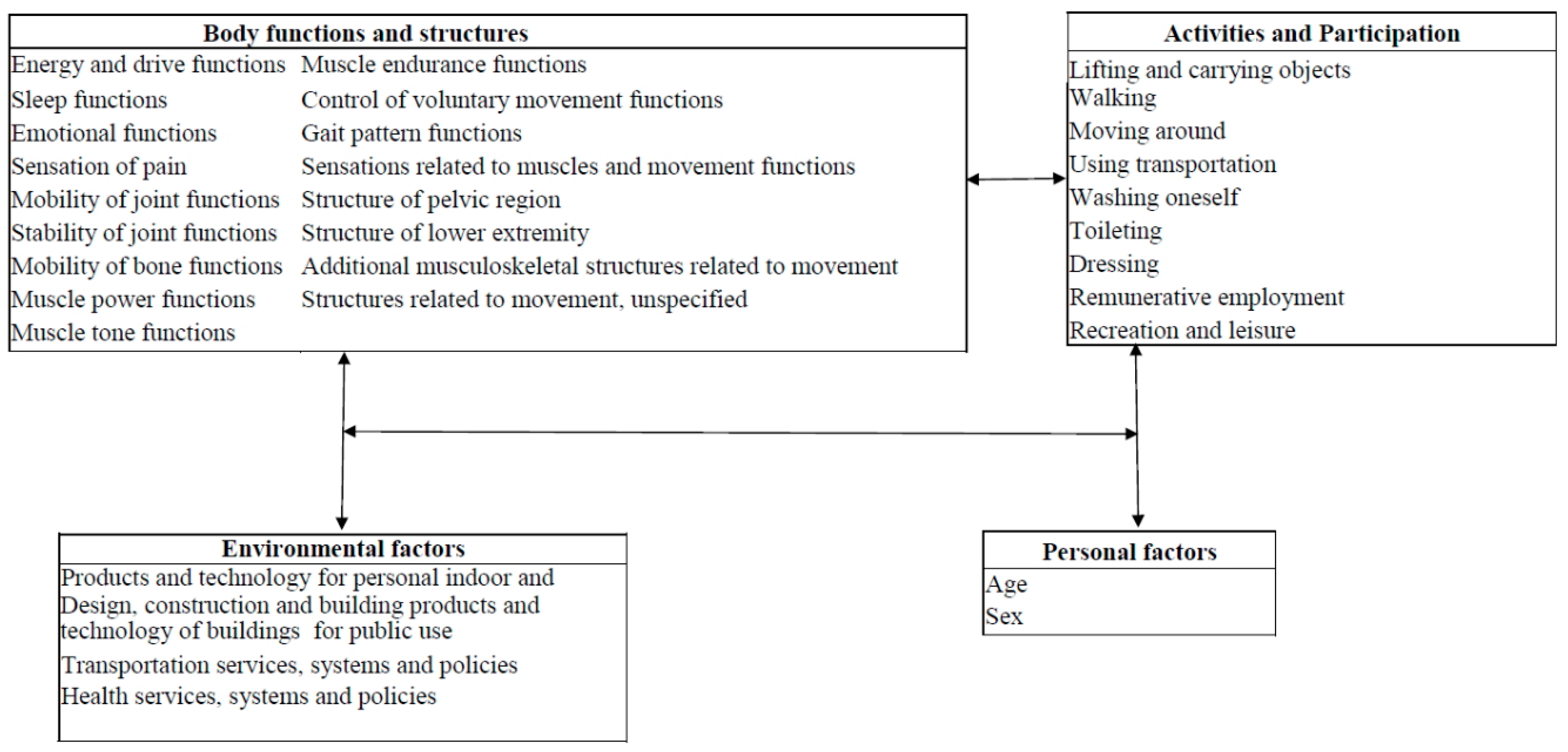
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| ICF Code | ICF Category Title | Round 1 | Round 2 | Round 3 |
|---|---|---|---|---|
| Body functions | ||||
| b130 | Energy and drive functions | 70 (25) | 90 (0) | 90 (0) |
| b134 | Sleep functions | 60 (20) | 75 (5) | 90 (0) |
| b152 | Emotional functions | 60 (30) | 70 (0) | 70 (0) |
| b280 | Sensation of pain | 70 (20) | 95 (0) | 95 (0) |
| b710 | Mobility of joint functions | 65 (20) | 95 (0) | 100 (0) |
| b715 | Stability of joint functions | 65 (15) | 100 (0) | 100 (0) |
| b720 | Mobility of bone functions | 65 (25) | 95 (5) | 75 (0) |
| b730 | Muscle power functions | 70 (20) | 100 (0) | 100 (0) |
| b735 | Muscle tone functions | 55 (15) | 65 (10) | 65 (5) |
| b740 | Muscle endurance functions | 65 (20) | 90 (0) | 90 (0) |
| b760 | Control of voluntary movement functions | 65 (20) | 95 (0) | 85 (5) |
| b765 | Involuntary movement functions | 15 (25) | 50 (0) | 55 (10) |
| b770 | Gait pattern functions | 70 (20) | 100 (0) | 90 (0) |
| b780 | Sensations related to muscles and movement functions | 75 (20) | 100 (0) | 95 (0) |
| s740 | Structure of pelvic region | 55 (20) | 95 (0) | 75 (0) |
| s750 | Structure of lower extremity | 60 (20) | 95 (0) | 95 (0) |
| s770 | Additional musculoskeletal structures related to movement | 65 (25) | 95 (0) | 90 (0) |
| s799 | Structures related to movement, unspecified | 65 (20) | 95 (0) | 90 (0) |
| Activities and participation | ||||
| d430 | Lifting and carrying objects | 70 (15) | 85 (10) | 75 (5) |
| d440 | Fine hand use | 25 (30) | 50 (30) | 30 (25) |
| d445 | Hand and arm use | 30 (25) | 50 (25) | 30 (20) |
| d450 | Walking | 75 (20) | 100 (0) | 100 (0) |
| d455 | Moving around | 70 (30) | 95 (0) | 80 (0) |
| d470 | Using transportation | 75 (15) | 85 (0) | 80 (5) |
| d475 | Driving | 65 (10) | 75 (5) | 50 (10) |
| d510 | Washing oneself | 60 (15) | 95 (5) | 75 (0) |
| d530 | Toileting | 70 (25) | 85 (5) | 85 (0) |
| d540 | Dressing | 65 (20) | 80 (10) | 75 (0) |
| d620 | Acquisition of goods and services | 40 (20) | 75 (10) | 30 (5) |
| d640 | Doing housework | 60 (5) | 70 (5) | 60 (0) |
| d660 | Assisting others | 40 (10) | 70 (10) | 35 (0) |
| d770 | Intimate relationships | 30 (20) | 70 (10) | 40 (5) |
| d850 | Remunerative employment | 70 (20) | 90 (0) | 95 (0) |
| d910 | Community life | 55 (20) | 85 (5) | 70 (0) |
| d920 | Recreation and leisure | 65 (10) | 90 (5) | 85 (0) |
| Environmental factors | ||||
| e120 | Products and technology for personal indoor and outdoor mobility and transportation | 75 (10) | 80 (0) | 95 (0) |
| e135 | Products and technology for employment | 55 (10) | 65 (0) | 70 (0) |
| e150 | Design, construction and building products and technology of buildings for public use | 45 (10) | 70 (10) | 80 (0) |
| e155 | Design, construction and building products and technology of buildings for private use | 45 (0) | 65 (5) | 65 (0) |
| e225 | Climate | 20 (25) | 30 (15) | 25 (20) |
| e310 | Immediate family | 45 (25) | 55 (5) | 30 (5) |
| e320 | Friends | 40 (25) | 65 (10) | 35 (0) |
| e450 | Individual attitudes of health professionals | 45 (25) | 55 (15) | 40 (15) |
| e460 | Societal attitudes | 60 (20) | 65 (10) | 65 (5) |
| e540 | Transportation services, systems and policies | 50 (10) | 75 (5) | 70 (0) |
| e575 | General social support services, systems and policies | 60 (5) | 80 (5) | 70 (0) |
| e580 | Health services, systems and policies | 75 (5) | 90 (0) | 80 (0) |
| Personal factors | ||||
| Age | 80 (5) | 90 (0) | 100 (0) | |
| Sex | 75 (10) | 80 (0) | 95 (0) | |
References
- Guccione, A.A.; Felson, D.T.; Anderson, J.J.; Anthony, J.M.; Zhang, Y.; Wilson, P.W.; Kelly-Hayes, M.; Wolf, P.A.; Kreger, B.E.; Kannel, W.B. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Am. J. Public Health 1994, 84, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Lapsley, H.M.; March, L.M.; Tribe, K.L.; Cross, M.J.; Brooks, P.M. Living with osteoarthritis: Patient expenditures, health status, and social impact. Arthritis Rheum. 2001, 45, 301–306. [Google Scholar] [CrossRef]
- Leyland, K.M.; Judge, A.; Javaid, M.K.; Diez-Perez, A.; Carr, A.; Cooper, C.; Arden, N.K.; Prieto-Alhambra, D. Obesity and the Relative Risk of Knee Replacement Surgery in Patients With Knee Osteoarthritis: A Prospective Cohort Study. Arthritis Rheumatol. 2016, 68, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Etkin, C.D.; Springer, B.D. The American Joint Replacement Registry-the first 5 years. Arthroplast. Today 2017, 3, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. Am. Vol. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Widmer, M.; Maravic, M.; Gomez-Barrena, E.; De Pina, M.D.F.; Manno, V.; Torre, M.; Walter, W.L.; et al. International survey of primary and revision total knee replacement. Int. Orthop. 2011, 35, 1783–1789. [Google Scholar] [CrossRef] [Green Version]
- Beard, D.J.; Davies, L.J.; Cook, J.A.; MacLennan, G.; Price, A.; Kent, S.; Hudson, J.; Carr, A.; Leal, J.; Campbell, H.; et al. The clinical and cost-effectiveness of total versus partial knee replacement in patients with medial compartment osteoarthritis (TOPKAT): 5-year outcomes of a randomised controlled trial. Lancet 2019, 394, 746–756. [Google Scholar] [CrossRef] [Green Version]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a self-administered outcome measure. J. Orthop Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Weigl, M.; Ewert, T.; Kleinschmidt, J.; Stucki, G. Measuring the outcome of health resort programs. J. Rheumatol. 2006, 33, 764–770. [Google Scholar]
- Weigl, M.; Cieza, A.; Harder, M.; Geyh, S.; Amann, E.; Kostanjsek, N.; Stucki, G. Linking osteoarthritis-specific health-status measures to the International Classification of Functioning, Disability, and Health (ICF). Osteoarthr. Cartil. 2003, 11, 519–523. [Google Scholar] [CrossRef] [Green Version]
- Stucki, G.; Melvin, J. The International Classification of Functioning, Disability and Health: A unifying model for the conceptual description of physical and rehabilitation medicine. J. Rehabil Med. 2007, 39, 286–292. [Google Scholar] [CrossRef] [Green Version]
- Yen, T.H.; Liou, T.H.; Chang, K.H.; Wu, N.N.; Chou, L.C.; Chen, H.C. Systematic review of ICF core set from 2001 to 2012. Disability Rehabil. 2014, 36, 177–184. [Google Scholar] [CrossRef]
- Cieza, A.; Ewert, T.; Ustun, T.B.; Chatterji, S.; Kostanjsek, N.; Stucki, G. Development of ICF Core Sets for patients with chronic conditions. J. Rehabil. Med. 2004, 44, 9–11. [Google Scholar]
- Graham, B.; Regehr, G.; Wright, J.G. Delphi as a method to establish consensus for diagnostic criteria. J. Clin. Epidemiol. 2003, 56, 1150–1156. [Google Scholar] [CrossRef]
- Cieza, A.; Geyh, S.; Chatterji, S.; Kostanjsek, N.; Ustun, B.; Stucki, G. ICF linking rules: An update based on lessons learned. J. Rehabil. Med. 2005, 37, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, F.; Ng, L.; Gonzalez, S.; Hale, T.; Turner-Stokes, L. Multidisciplinary rehabilitation programmes following joint replacement at the hip and knee in chronic arthropathy. Cochrane Database Syst. Rev. 2008, CD004957. [Google Scholar] [CrossRef] [PubMed]
- Hylkema, T.H.; Brouwer, S.; Stewart, R.E.; van Beveren, J.; Rijk, P.C.; Brouwer, R.W.; Bulstra, S.K.; Kuijer, P.; Stevens, M. Two-year recovery courses of physical and mental impairments, activity limitations, and participation restrictions after total knee arthroplasty among working-age patients. Disabil. Rehabil. 2020, 1–10. [Google Scholar] [CrossRef]
- Liao, C.D.; Chen, H.C.; Kuo, Y.C.; Tsauo, J.Y.; Huang, S.W.; Liou, T.H. Effects of Muscle Strength Training on Muscle Mass Gain and Hypertrophy in Older Adults With Osteoarthritis: A Systematic Review and Meta-Analysis. Arthritis Care Res. 2020, 72, 1703–1718. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.F.; Orozco, F.R.; Austin, L.S.; Post, Z.D.; Deirmengian, C.A.; Ong, A.C. Prospective Evaluation of Sleep Disturbances After Total Knee Arthroplasty. J. Arthroplast. 2016, 31, 330–332. [Google Scholar] [CrossRef]
- Kuwahara, W.; Nakanishi, K.; Kurumadani, H.; Shimada, N.; Asaeda, M.; Deie, M.; Adachi, N.; Sunagawa, T. Total knee arthroplasty for patients with medial knee osteoarthritis improves trunk movement during gait. J. Back Musculoskelet. Rehabil. 2019. [Google Scholar] [CrossRef]
- Kitagawa, A.; Yamamoto, J.; Toda, M.; Hashimoto, Y. Spinopelvic Alignment and Low Back Pain before and after Total Knee Arthroplasty. Asian Spine J. 2020. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; Twaij, H.; Giebaly, D.E.; Nizam, I.; Haddad, F.S. Enhanced recovery in total hip replacement: A clinical review. Bone Joint J. 2013, 95, 1587–1594. [Google Scholar] [CrossRef]
- Lavernia, C.J.; Alcerro, J.C.; Brooks, L.G.; Rossi, M.D. Mental health and outcomes in primary total joint arthroplasty. J. Arthroplast. 2012, 27, 1276–1282. [Google Scholar] [CrossRef] [PubMed]
- Bruyere, O.; Ethgen, O.; Neuprez, A.; Zegels, B.; Gillet, P.; Huskin, J.P.; Reginster, J.Y. Health-related quality of life after total knee or hip replacement for osteoarthritis: A 7-year prospective study. Arch. Orthop Trauma Surg. 2012, 132, 1583–1587. [Google Scholar] [CrossRef] [PubMed]
- Dreinhofer, K.; Stucki, G.; Ewert, T.; Huber, E.; Ebenbichler, G.; Gutenbrunner, C.; Kostanjsek, N.; Cieza, A. ICF Core Sets for osteoarthritis. J. Rehabil Med. 2004, 44, 75–80. [Google Scholar] [CrossRef] [PubMed]



| ICF Code | ICF Category Title | Round 1 | Round 2 | Round 3 |
|---|---|---|---|---|
| Body functions | ||||
| b130 | Energy and drive functions | 3.7 (1.3) | 4.3 (0.7) | 4.1 (0.5) |
| b134 | Sleep functions | 3.6 (1.3) | 4.0 (1.0) | 4.1 (0.6) |
| b152 | Emotional functions | 3.5 (1.3) | 4.1 (0.8) | 4.0 (0.8) |
| b280 | Sensation of pain | 4.0 (1.3) | 4.6 (0.6) | 4.5 (0.6) |
| b710 | Mobility of joint functions | 4.0 (1.4) | 4.7 (0.6) | 4.8 (0.4) |
| b715 | Stability of joint functions | 4.0 (1.3) | 4.6 (0.5) | 4.6 (0.5) |
| b720 | Mobility of bone functions | 3.7 (1.3) | 4.5 (0.8) | 4.2 (0.8) |
| b730 | Muscle power functions | 4.0 (1.4) | 4.7 (0.5) | 4.6 (0.5) |
| b735 | Muscle tone functions | 3.6 (1.1) | 4.0 (1.1) | 4.0 (0.9) |
| b740 | Muscle endurance functions | 3.8 (1.4) | 4.5 (0.7) | 4.4 (0.7) |
| b760 | Control of voluntary movement functions | 3.7 (1.3) | 4.5 (0.6) | 4.2 (0.8) |
| b765 | Involuntary movement functions | 2.9 (0.9) | 3.6 (0.6) | 3.8 (1.0) |
| b770 | Gait pattern functions | 3.6 (1.4) | 4.6 (0.5) | 4.3 (0.7) |
| b780 | Sensations related to muscles and movement functions | 3.8 (1.2) | 4.5 (0.5) | 4.4 (0.6) |
| s740 | Structure of pelvic region | 3.4 (1.2) | 4.4 (0.6) | 4.1 (0.8) |
| s750 | Structure of lower extremity | 3.7 (1.3) | 4.5 (0.6) | 4.4 (0.6) |
| s770 | Additional musculoskeletal structures related to movement | 3.7 (1.4) | 4.5 (0.6) | 4.1 (0.6) |
| s799 | Structures related to movement, unspecified | 3.7 (1.3) | 4.5 (0.6) | 4.2 (0.6) |
| Activities and participation | ||||
| d430 | Lifting and carrying objects | 3.8 (1.0) | 4.3 (1.0) | 4.1 (0.9) |
| d440 | Fine hand use | 2.9 (1.2) | 3.4 (1.2) | 3.2 (1.1) |
| d445 | Hand and arm use | 3.1 (1.1) | 3.5 (1.1) | 3.2 (1.0) |
| d450 | Walking | 4.1 (1.4) | 4.7 (0.5) | 4.7 (0.5) |
| d455 | Moving around | 3.6 (1.5) | 4.6 (0.6) | 4.4 (0.8) |
| d470 | Using transportation | 3.9 (1.3) | 4.4 (0.7) | 4.0 (0.8) |
| d475 | Driving | 3.7 (1.0) | 4.1 (0.9) | 3.5 (0.8) |
| d510 | Washing oneself | 3.7 (1.2) | 4.4 (0.7) | 4.0 (0.7) |
| d530 | Toileting | 3.8 (1.3) | 4.3 (0.9) | 4.2 (0.7) |
| d540 | Dressing | 3.8 (1.2) | 4.1 (1.1) | 4.0 (0.7) |
| d620 | Acquisition of goods and services | 3.3 (0.9) | 4.0 (0.9) | 3.3 (0.6) |
| d640 | Doing housework | 3.7 (1.0) | 4.1 (1.0) | 3.7 (0.7) |
| d660 | Assisting others | 3.3 (0.7) | 3.9 (0.9) | 3.5 (0.7) |
| d770 | Intimate relationships | 3.1 (0.9) | 3.8 (0.9) | 3.4 (0.7) |
| d850 | Remunerative employment | 3.8 (1.2) | 4.5 (0.7) | 4.2 (0.5) |
| d910 | Community life | 3.5 (0.9) | 4.1 (0.9) | 3.8 (0.6) |
| d920 | Recreation and leisure | 3.8 (0.9) | 4.3 (0.8) | 4.1 (0.6) |
| Environmental factors | ||||
| e120 | Products and technology for personal indoor and outdoor mobility and transportation | 3.9 (1.0) | 4.2 (0.7) | 4.3 (0.6) |
| e135 | Products and technology for employment | 3.6 (0.8) | 3.8 (0.7) | 3.9 (0.7) |
| e150 | Design, construction and building products and technology of buildings for public use | 3.4 (0.8) | 3.8 (0.9) | 4.0 (0.6) |
| e155 | Design, construction and building products and technology of buildings for private use | 3.6 (0.7) | 3.8 (0.8) | 3.7 (0.6) |
| e225 | Climate | 3.0 (0.7) | 3.3 (0.9) | 3.2 (1.0) |
| e310 | Immediate family | 3.2 (1.2) | 3.7 (1.0) | 3.5 (0.9) |
| e320 | Friends | 3.3 (1.0) | 3.7 (1.0) | 3.6 (0.8) |
| e450 | Individual attitudes of health professionals | 3.2 (1.2) | 3.6 (1.0) | 3.5 (1.0) |
| e460 | Societal attitudes | 3.5 (1.1) | 3.7 (1.0) | 3.8 (0.8) |
| e540 | Transportation services, systems, and policies | 3.6 (1.1) | 4.0 (0.9) | 4.0 (0.8) |
| e575 | General social support services, systems, and policies | 3.7 (0.7) | 4.0 (0.8) | 3.9 (0.7) |
| e580 | Health services, systems, and policies | 4.0 (0.8) | 4.2 (0.6) | 4.2 (0.7) |
| Personal factors | ||||
| Age | 4.6 (0.6) | 4.7 (0.6) | 4.8 (0.4) | |
| Sex | 4.2 (1.0) | 4.1 (0.7) | 4.1 (0.6) | |
| ICF Domain | ICF Core Set for OA | ICF Core Set for Post TKA Replacement |
|---|---|---|
| Body functions and structure | ||
| b130 Energy and drive functions | x | x |
| b134 Sleep functions | x | x |
| b152 Emotional functions | x | x |
| b280 Sensation of pain | x | x |
| b710 Mobility of joint functions | x | x |
| b715 Stability of joint functions | x | x |
| b720 Mobility of bone functions | x | x |
| b730 Muscle power functions | x | x |
| b735 Muscle tone functions | x | x |
| b740 Muscle endurance functions | x | x |
| b760 Control of voluntary movement functions | x | x |
| b770 Gait pattern functions | x | x |
| b780 Sensations related to muscles and movement functions | x | x |
| s720 Structure of shoulder region | x | |
| s730 Structure of upper extremity | x | |
| s740 Structure of pelvic region | x | x |
| s750 Structure of lower extremity | x | x |
| s770 Additional musculoskeletal structures related to movement | x | x |
| s799 Structures related to movement, unspecified | x | x |
| Activity and Participation | ||
| d410 Changing basic body position | x | |
| d415 Maintaining a body position | x | |
| d430 Lifting and carrying objects | x | x |
| d440 Fine hand use | x | |
| d445 Hand and arm use | x | |
| d450 Walking | x | x |
| d455 Moving around | x | x |
| d470 Using transportation | x | x |
| d475 Driving | x | |
| d510 Washing oneself | x | x |
| d530 Toileting | x | x |
| d540 Dressing | x | x |
| d620 Acquisition of goods and services | x | |
| d640 Doing housework | x | |
| d660 Assisting others | x | |
| d770 Intimate relationships | x | |
| d850 Remunerative employment | x | x |
| d910 Community Life | x | |
| d920 Recreation and leisure | x | x |
| Environmental factor | ||
| e110 Products or substances for personal consumption | x | |
| e115 Products and technology for personal use in daily living | x | |
| e120 Products and technology for personal indoor and outdoor mobility and transportation | x | x |
| e135 Products and technology for employment | x | |
| e150 Design, construction and building products and technology of buildings for public use | x | x |
| e155 Design, construction and building products and technology of buildings for private use | x | |
| e225 Climate | x | |
| e310 Immediate family | x | |
| e320 Friends | x | |
| e340 Personal care providers and personal assistants | x | |
| e355 Health professionals | x | |
| e410 Individual attitudes of immediate family members | x | |
| e450 Individual attitudes of health professionals | x | |
| e460 Societal attitudes | x | |
| e540 Transportation services, systems and policies | x | x |
| e575 General social support services, systems and policies | x | |
| e580 Health services, systems and policies | x | x |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.-W.; Chen, Y.-W.; Escorpizo, R.; Liao, C.-D.; Liou, T.-H. Development International Classification of Functioning, Disability and Health Core Set for Post Total Knee Replacement Rehabilitation Program: Delphi-Based Consensus Study in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 1630. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041630
Huang S-W, Chen Y-W, Escorpizo R, Liao C-D, Liou T-H. Development International Classification of Functioning, Disability and Health Core Set for Post Total Knee Replacement Rehabilitation Program: Delphi-Based Consensus Study in Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(4):1630. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041630
Chicago/Turabian StyleHuang, Shih-Wei, Yi-Wen Chen, Reuben Escorpizo, Chun-De Liao, and Tsan-Hon Liou. 2021. "Development International Classification of Functioning, Disability and Health Core Set for Post Total Knee Replacement Rehabilitation Program: Delphi-Based Consensus Study in Taiwan" International Journal of Environmental Research and Public Health 18, no. 4: 1630. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041630