
Stress and Cardiometabolic Disease Risk for Indigenous Populations throughout the Lifespan

 ,
,
Abstract
:1. Introduction
Stress–CMD Relationship
2. Methods
3. Historical Trauma and CMD
- (1)
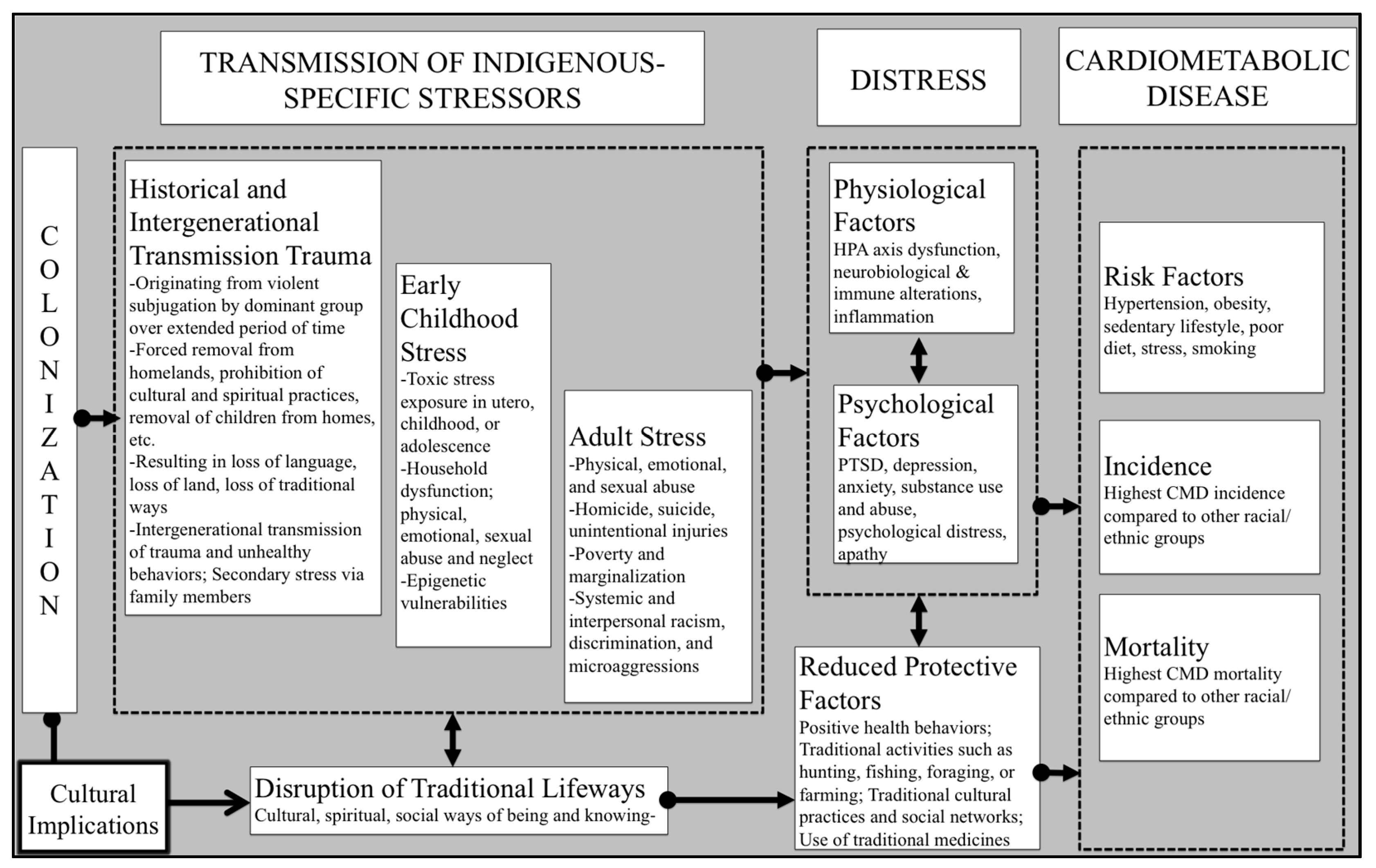
- Physiological Stress. One conceptualization of historical trauma is as an ongoing stressor that taxes the body physiologically, similar to other stressors. Specifically, this model proposes that historical trauma creates contemporary distress, which may be displayed through symptoms of PTSD, anxiety, or depression, taxes regulatory systems, including the HPA axis and balance between sympathetic and parasympathetic nervous systems, and results in the development of CVD risk factors, including insulin resistance [80]. In particular, Lefler and Belt illuminate that, “diabetes needs to be considered a manifestation of intergenerational PTSD” [80], p.73. This stress may additionally be transmitted intergenerationally through epigenetics, resulting in health risks being passed from parents to children through generations [59,81,82].
- (2)
- Disruption of Food Systems, Medicines, and Traditional Lifeways. Through a variety of contributors (e.g., forced European farming methods, prohibition of traditional ecological methods and beliefs, forced relocation, introduction of European animals and plants, environmental degradation), Indigenous people have significantly different diet and exercise patterns compared to pre-colonization food activities including hunting, fishing, foraging, and traditional farming. Thus, prohibition of traditional foodways is directly linked to an increased sedentary lifestyle [83]. Government-sponsored food programs have replaced traditional foods that may have protected Indigenous people from metabolic disease [83], including tepary beans (Tohono O’odham), salmon (Yup’ik) [84] and Jerusalem artichoke and persimmons (Cherokee) [85], with foods that are high in simple sugars and saturated fats [86], leading to increased rates of obesity, hypertension, diabetes, and heart disease [87]. Additionally, remedies and ceremonies used in traditional medicine to treat diabetes and heart disease, such as the use of hawthorn or sumac leaves to lower blood pressure and glucose [88,89,90], were prohibited in the US until recently (Indian Freedom of Religion Act of 1978), resulting in the carry-over of stigma against practicing traditional spirituality today [91]. One study specifically implicated the loss of traditional Indigenous CMD prevention practices among Pacific Northwest AIs in the effect of historical trauma on increased risk for CMD [92].
- (3)
- Intergenerational Transmission of Stress and Trauma. Through a process called trauma transmission, family members or those with close relationships to someone with PTSD may develop symptoms that mirror PTSD without any primary traumatic experience, called secondary stress [93]. Specifically, in marital and parent–child relationships, as partners or children learn about the traumatic event, they emotionally experience the event and begin to mirror the symptomology of the PTSD victim [94]. The trauma transmission model [95] specifies that partners use not only sympathy, but empathy for their partner’s experience, resulting in a realistic experience of the trauma themselves. Therefore, the closer the relationship, the more at risk one is for developing secondary trauma, especially for those living together. While most research on secondary trauma is in military families, researchers have begun to look to this model as an explanatory model for the passing of trauma and trauma symptoms to subsequent generations of Indigenous families [96].
- (3a)
- Intergenerational Transmission of Poverty. Colonization aimed to prevent and terminate Indigenous lifeways including community, family, and parenting values and practices to make way for Western European ideals. For instance, residential schools aimed to shift Indigenous parenting styles due to military and religious influences. In addition, residential schools purposefully created a low socioeconomic class of Indigenous people given that these schools trained students to work in the lowest-paying jobs available. Today, the experience of poverty, including homelessness and lack of unemployment, are both prevalent for Indigenous populations and relate to negative health outcomes [97,98]. It is important to note that poverty is also intergenerational. The intergenerational transmission of poverty describes the pattern of parental poverty experienced by a child persisting into the child’s own adulthood, which is influenced by a complex set of positive and negative factors such as private transmission of capital (e.g., inheritance of land and money), public transmission of resources (e.g., low investment in education of low-income neighborhoods), and behavioral traits (e.g., learned habits around wealth accumulation) from one generation to the next. Parental poverty status influences children’s resiliency and human capital development (e.g., educational performance and social development), contributing to the intergenerational transmission of poverty. Additionally, the costs of ill health and healthcare may be enough to ensure persistent poverty and are a driver of downward economic mobility demonstrating a bidirectional association between poverty and health status [99]. Therefore, it appears that health status and poverty may be linked through intergenerational transmission of trauma experiences for Indigenous people.
- (3b)
- Intergenerational Transmission of CMD Risk Behaviors. The stress of experiencing increased thoughts of historical trauma and loss are additionally related to an increase in CMD risk behaviors. For example, mothers are more likely to smoke during pregnancy if their mother or grandmother attended residential school compared to those who did not have family member residential school attendance [100], which puts babies at risk for low birth weight and subsequent cardiometabolic disease [101,102]. In addition, violence and militaristic parenting styles were taught through colonial practices including boarding schools. Therefore, intergenerational trauma may be perpetuated by learned harmful parenting techniques and worsened parent–child relationships, which negatively affects the child via the adverse childhood experiences mechanism [96]. This may lead the child to adopt personal unhealthful behaviors, including dysfunctional parenting practices, which in turn leads to adverse childhood experiences in their offspring.
4. Early Childhood Stress and CMD
5. Adulthood Stress and Trauma and CMD
6. Existing Interventions and Actionable Solutions
6.1. Addressing Historical Trauma
6.2. Reducing Childhood Stressors
6.3. Reducing Trauma and Discrimination
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xu, J.; Kochanek, K.; Murphy, S.; Tejada-Vera, B. Deaths: Final data for 2007. Natl. Vital. Stat. Rep. 2010, 58, 1–19. [Google Scholar] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.; Fullerton, H.J. Heart disease and stroke statistics-2016 update: A report from the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef]
- Galloway, J.M. Cardiovascular health among American Indians and Alaska Natives: Successes, challenges, and potentials. Am. J. Prev. Med. 2005, 29, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Howard, B.V.; Lee, E.T.; Cowan, L.D.; Devereux, R.B.; Galloway, J.M.; Go, O.T.; Howard, W.J.; Rhoades, E.R.; Robbins, D.C.; Sievers, M.L.; et al. Rising tide of cardiovascular disease in American Indians. The Strong Heart Study. Circulation 1999, 99, 2389–2395. [Google Scholar] [CrossRef] [Green Version]
- Heron, M. Deaths: Leading causes for 2016. Natl. Vital. Stat. Rep. 2018, 67, 1–76. [Google Scholar]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S. Executive summary: Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 2014, 129, 399–410. [Google Scholar] [CrossRef]
- Veazie, M.; Ayala, C.; Schieb, L.; Dai, S.; Henderson, J.A.; Cho, P. Trends and Disparities in Heart Disease Mortality Among American Indians/Alaska Natives, 1990–2009. Am. J. Public Health 2014, 104, S359–S367. [Google Scholar] [CrossRef] [PubMed]
- Williams, W.M. Racial Inequities in Cardiovascular Disease in New Zealand. Divers. Equal. Health Care 2017, 14, 23. [Google Scholar] [CrossRef] [Green Version]
- Aluli, N.E.; Reyes, P.W.; Brady, S.K.; Tsark, J.U.; Jones, K.L.; Mau, M.; Howard, W.J.; Howard, B.V. All-cause and CVD mortality in Native Hawaiians. Diabetes Res. Clin. Pract. 2010, 89, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Penm, E. Cardiovascular Disease and Its Associated Risk Factors in Aboriginal and Torres Strait Islander Peoples 2004-05; AIHW: Canberra, Australia, 2008. [Google Scholar]
- Tjepkema, M.; Wilkins, R.; Goedhuis, N.; Pennock, J. Cardiovascular disease mortality among First Nations people in Canada, 1991–2001. Chronic Dis. Inj. Can. 2012, 32, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Deen, J.F.; Adams, A.K.; Fretts, A.; Jolly, S.; Navas-Acien, A.; Devereux, R.B.; Buchwald, D.; Howard, B.V. Cardiovascular Disease in American Indian and Alaska Native Youth: Unique Risk Factors and Areas of Scholarly Need. J. Am. Heart Assoc. 2017, 6, e007576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ferranti, S.; Gauvreau, K.; Ludwig, D.; Neufeld, E.; Newburger, J.; Nader, R. Prevalence of the metabolic syndrome in American adolescents: Findings from the Third National Health and Nutrition Examination Survey. ACC Curr. J. Rev. 2005, 14, 95. [Google Scholar] [CrossRef]
- Grundy, S.M.; Brewer, H.B.; Cleeman, J.I.; Smith, S.C.; Lenfant, C.; National Heart, Lung, and Blood Institute; American Heart Association. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Chinali, M.; de Simone, G.; Roman, M.J.; Best, L.G.; Lee, E.T.; Russell, M.; Howard, B.V.; Devereux, R.B. Cardiac markers of pre-clinical disease in adolescents with the metabolic syndrome: The strong heart study. J. Am. Coll. Cardiol. 2008, 52, 932–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gami, A.S.; Witt, B.J.; Howard, D.E.; Erwin, P.J.; Gami, L.A.; Somers, V.K.; Montori, V.M. Metabolic syndrome and risk of incident cardiovascular events and death: A systematic review and meta-analysis of longitudinal studies. J. Am. Coll. Cardiol. 2007, 49, 403–414. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.W.; D’Agostino, R.B.; Parise, H.; Sullivan, L.; Meigs, J.B. Metabolic Syndrome as a Precursor of Cardiovascular Disease and Type 2 Diabetes Mellitus. Circulation 2005, 112, 3066–3072. [Google Scholar] [CrossRef]
- Steptoe, A.; Kivimäki, M. Stress and cardiovascular disease. Nat. Rev. Cardiol. 2012, 9, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Kivimäki, M. Stress and Cardiovascular Disease: An Update on Current Knowledge. Annu. Rev. Public Health 2013, 34, 337–354. [Google Scholar] [CrossRef] [PubMed]
- Scott, K.M. Association of Childhood Adversities and Early-Onset Mental Disorders With Adult-Onset Chronic Physical Conditions. Arch. Gen. Psychiatry 2011, 68, 838–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bomhof-Roordink, H.; Seldenrijk, A.; Van Hout, H.P.; Van Marwijk, H.W.; Diamant, M.; Penninx, B.W. Associations between life stress and subclinical cardiovascular disease are partly mediated by depressive and anxiety symptoms. J. Psychosom. Res. 2015, 78, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Anda, R.F.; Felitti, V.J.; Dube, S.R.; Williamson, D.F.; Thompson, T.J.; Loo, C.M.; Giles, W.H. The interrelatedness of multiple forms of childhood abuse, neglect, and household dysfunction. Child Abus. Negl. 2004, 28, 771–784. [Google Scholar] [CrossRef] [PubMed]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. REPRINT OF: Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 2019, 56, 774–786. [Google Scholar] [CrossRef] [PubMed]
- Korkeila, J.; Vahtera, J.; Korkeila, K.; Kivimäki, M.; Sumanen, M.; Koskenvuo, K.; Koskenvuo, M. Childhood adversities as predictors of incident coronary heart disease and cerebrovascular disease. Heart 2010, 96, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Dougall, L.A.; Baum, A. Stress, health, and illness. In Handbook of Health Psychology; Baum, A., Revenson, T.A., Singer, J., Eds.; Psychology Press: New York, NY, USA, 2012; pp. 53–78. [Google Scholar]
- Beckham, J.C.; Taft, C.T.; Vrana, S.R.; Feldman, M.E.; Barefoot, J.C.; Moore, S.D.; Mozley, S.L.; Butterfield, M.I.; Calhoun, P.S. Ambulatory monitoring and physical health report in Vietnam veterans with and without chronic posttraumatic stress disorder. J. Trauma. Stress 2003, 16, 329–335. [Google Scholar] [CrossRef]
- Dragoş, D.; Tănăsescu, M.D. The effect of stress on the defense systems. J. Med. Life 2010, 3, 10–18. [Google Scholar]
- McEwen, B.S. Brain on stress: How the social environment gets under the skin. Proc. Natl. Acad. Sci. USA 2012, 109, 17180–17185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hjemdahl, P.; Rosengren, A.; Steptoe, A. Stress and Cardiovascular Disease; Springer: Berlin/Heidelberg, Germany, 2013; pp. 1–390. [Google Scholar]
- Guyll, M.; Matthews, K.A.; Bromberger, J.T. Discrimination and unfair treatment: Relationship to cardiovascular reactivity among African American and European American women. Health Psychol. 2001, 20, 315. [Google Scholar] [CrossRef]
- Bremner, V.V.a.J.D. Psychiatric and Behavioral Aspects of Cardiovascular Disease. In Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine; Zipes, D.P., Ed.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 1889–1897. [Google Scholar]
- Lockwood, K.G.; Marsland, A.L.; Matthews, K.A.; Gianaros, P.J. Perceived discrimination and cardiovascular health disparities: A multisystem review and health neuroscience perspective. Ann. N. Y. Acad. Sci. 2018, 1428, 170–207. [Google Scholar] [CrossRef]
- Gianaros, P.J.; Marsland, A.L.; Kuan, D.C.-H.; Schirda, B.L.; Jennings, J.R.; Sheu, L.K.; Hariri, A.R.; Gross, J.J.; Manuck, S.B. An Inflammatory Pathway Links Atherosclerotic Cardiovascular Disease Risk to Neural Activity Evoked by the Cognitive Regulation of Emotion. Biol. Psychiatry 2014, 75, 738–745. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Janicki-Deverts, D.; Miller, G.E. Psychological Stress and Disease. JAMA 2007, 298, 1685–1687. [Google Scholar] [CrossRef] [PubMed]
- Sajadieh, A.; Nielsen, O.W.; Rasmussen, V.; Hein, H.O.; Abedini, S.; Hansen, J.F. Increased heart rate and reduced heart-rate variability are associated with subclinical inflammation in middle-aged and elderly subjects with no apparent heart disease. Eur. Heart J. 2004, 25, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Haffner, S.M. Pre-diabetes, insulin resistance, inflammation and CVD risk. Diabetes Res. Clin. Pract. 2003, 61, S9–S18. [Google Scholar] [CrossRef]
- Mathieu, P.; Lemieux, I.; Després, J.-P. Obesity, Inflammation, and Cardiovascular Risk. Clin. Pharmacol. Ther. 2010, 87, 407–416. [Google Scholar] [CrossRef]
- Cohen, B.E.; Edmondson, D.; Kronish, I.M. State of the Art Review: Depression, Stress, Anxiety, and Cardiovascular Disease. Am. J. Hypertens. 2015, 28, 1295–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosengren, A.; Hawken, S.; Ôunpuu, S.; Sliwa, K.; Zubaid, M.; Almahmeed, W.A.; Blackett, K.N.; Sitthi-Amorn, C.; Sato, H.; Yusuf, S. Association of psychosocial risk factors with risk of acute myocardial infarction in 11 119 cases and 13 648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 953–962. [Google Scholar] [CrossRef]
- Abramson, J.; Berger, A.; Krumholz, H.M.; Vaccarino, V. Depression and Risk of Heart Failure Among Older Persons With Isolated Systolic Hypertension. Arch. Intern. Med. 2001, 161, 1725–1730. [Google Scholar] [CrossRef] [Green Version]
- Elderon, L.; Whooley, M.A. Depression and Cardiovascular Disease. Prog. Cardiovasc. Dis. 2013, 55, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Joynt, K.E.; Whellan, D.J.; O’Connor, C.M. Depression and cardiovascular disease: Mechanisms of interaction. Biol. Psychiatry 2003, 54, 248–261. [Google Scholar] [CrossRef]
- Dyball, D.; Evans, S.; Boos, C.J.; Stevelink, S.A.M.; Fear, N.T. The association between PTSD and cardiovascular disease and its risk factors in male veterans of the Iraq/Afghanistan conflicts: A systematic review. Int. Rev. Psychiatry 2019, 31, 34–48. [Google Scholar] [CrossRef]
- Shah, A.J.; Lampert, R.; Goldberg, J.; Veledar, E.; Bremner, J.D.; Vaccarino, V. Posttraumatic Stress Disorder and Impaired Autonomic Modulation in Male Twins. Biol. Psychiatry 2013, 73, 1103–1110. [Google Scholar] [CrossRef] [Green Version]
- Sumner, J.A.; Kubzansky, L.D.; Elkind, M.S.V.; Roberts, A.L.; Agnew-Blais, J.; Chen, Q.; Cerdá, M.; Rexrode, K.M.; Rich-Edwards, J.W.; Spiegelman, D.; et al. Trauma Exposure and Posttraumatic Stress Disorder Symptoms Predict Onset of Cardiovascular Events in Women. Circulation 2015, 132, 251–259. [Google Scholar] [CrossRef]
- Perdue, T. The Cherokee Nation and the Trail of Tears; Green, M.D., Ed.; Viking: New York, NY, USA, 2007. [Google Scholar]
- Indian Health Service. Disparities. 2018. Available online: http://www.ihs.gov/newsroom/index.cfm/factsheets/disparities/ (accessed on 26 January 2021).
- American Psychiatric Association. Mental Health Disparities: American Indians and Alaskan Natives. 2010. Available online: http://www.integration.samhsa.gov/workforce/mental_health_disparities_american_indian_and_alaskan_natives.pdf (accessed on 26 January 2021).
- United States Sentencing Commission. Native Americans in the Federal Offender Population. 2015. Available online: http://www.ussc.gov/sites/default/files/pdf/research-and-publications/quick-facts/Quick_Facts_Native_American_Offenders.pdf (accessed on 26 January 2021).
- Walls, M.L.; Gonzalez, J.; Gladney, T.; Onello, E. Unconscious Biases: Racial Microaggressions in American Indian Health Care. J. Am. Board Fam. Med. 2015, 28, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Walls, M.L.; Whitbeck, L.B. The Intergenerational Effects of Relocation Policies on Indigenous Families. J. Fam. Issues 2012, 33, 1272–1293. [Google Scholar] [CrossRef] [Green Version]
- Bullock, A.; Bell, R.A. Stress, trauma, and coronary heart disease among native americans. Am. J. Public Health 2005, 95, 2122–2123. [Google Scholar] [CrossRef]
- Manson, S.M.; Beals, J.; Klein, S.A.; Croy, C.D.; the AI-SUPERPFP Team. Social Epidemiology of Trauma Among 2 American Indian Reservation Populations. Am. J. Public Health 2005, 95, 851–859. [Google Scholar] [CrossRef]
- Sawchuk, C.N.; Roy-Byrne, P.; Goldberg, J.; Manson, S.; Noonan, C.; Beals, J.; Buchwald, D. The relationship between post-traumatic stress disorder, depression and cardiovascular disease in an American Indian tribe. Psychol. Med. 2005, 35, 1785–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, L.; Beals, J.; Whitesell, N.R.; Roubideaux, Y.; Manson, S.M.; Team, A.-S. Stress burden and diabetes in two American Indian reservation communities. Diabetes Care 2007, 31, 427–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccarino, V.; Goldberg, J.; Rooks, C.; Shah, A.J.; Veledar, E.; Faber, T.L.; Votaw, J.R.; Forsberg, C.W.; Bremner, J.D. Post-traumatic stress disorder and incidence of coronary heart disease: A twin study. J. Am. Coll. Cardiol. 2013, 62, 970–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, T.D.; Smith, L.T. Decolonizing Methodologies: Research and Indigenous Peoples; University of Otago Press: New York, NY, USA, 1999. [Google Scholar]
- Department of Economic and Social Affairs Indigenous Peoples. United Nations Declaration on the Rights of Indigenous Peoples. 2007. Available online: https://www.un.org/development/desa/indigenouspeoples/declaration-on-the-rights-of-indigenous-peoples.html (accessed on 26 January 2021).
- Kinser, P.A.; Lyon, D.E. A conceptual framework of stress vulnerability, depression, and health outcomes in women: Potential uses in research on complementary therapies for depression. Brain Behav. 2014, 4, 665–674. [Google Scholar] [CrossRef]
- Warne, D.; Lajimodiere, D. American Indian health disparities: Psychosocial influences. Soc. Pers. Psychol. Compass 2015, 9, 567–579. [Google Scholar] [CrossRef]
- Heart, M.Y.H.B. The Historical Trauma Response Among Natives and Its Relationship with Substance Abuse: A Lakota Illustration. J. Psychoact. Drugs 2003, 35, 7–13. [Google Scholar] [CrossRef]
- Sotero, M.M. A conceptual model of historical trauma: Implications for public health practice and research. J. Health Disparities Res. Pract. 2006, 1, 93–108. [Google Scholar]
- Whitbeck, L.B.; Crawford, D.M. Gestational Risks and Psychiatric Disorders Among Indigenous Adolescents. Community Ment. Health J. 2009, 45, 62–72. [Google Scholar] [CrossRef] [Green Version]
- Myhra, L.L. “It Runs in the Family”: Intergenerational Transmission of Historical Trauma among Urban American Indians and Alaska Natives in Culturally Specific Sobriety Maintenance Programs. Am. Indian Alsk. Nativ. Ment. Health Res. 2011, 18, 17–40. [Google Scholar] [CrossRef]
- Mohatt, N.V.; Thompson, A.B.; Thai, N.D.; Tebes, J.K. Historical trauma as public narrative: A conceptual review of how history impacts present-day health. Soc. Sci. Med. 2014, 106, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Crawford, A. “The trauma experienced by generations past having an effect in their descendants”: Narrative and historical trauma among Inuit in Nunavut, Canada. Transcult. Psychiatry 2013, 51, 339–369. [Google Scholar] [CrossRef] [PubMed]
- Daley, T.C. Perceptions and Congruence of Symptoms and Communication among Second-generation Cambodian Youth and Parents: A Matched-control Design. Child Psychiatry Hum. Dev. 2006, 37, 39–53. [Google Scholar] [CrossRef]
- Gone, J.P.; Trimble, J.E. American Indian and Alaska Native Mental Health: Diverse Perspectives on Enduring Disparities. Annu. Rev. Clin. Psychol. 2012, 8, 131–160. [Google Scholar] [CrossRef]
- Walters, K.L.; Mohammed, S.A.; Evans-Campbell, T.; Beltrán, R.E.; Chae, D.H.; Duran, B. Bodies don’t just tell stories, they tell histories: Embodiment of historical trauma among American Indians and Alaska Natives. Du Bois Rev. 2011, 8, 179–189. [Google Scholar] [CrossRef] [Green Version]
- Whitbeck, L.B.; Adams, G.W.; Hoyt, D.R.; Chen, X. Conceptualizing and Measuring Historical Trauma Among American Indian People. Am. J. Community Psychol. 2004, 33, 119–130. [Google Scholar] [CrossRef]
- Yehuda, R.; Engel, S.M.; Brand, S.R.; Seckl, J.; Marcus, S.M.; Berkowitz, G.S. Transgenerational Effects of Posttraumatic Stress Disorder in Babies of Mothers Exposed to the World Trade Center Attacks during Pregnancy. J. Clin. Endocrinol. Metab. 2005, 90, 4115–4118. [Google Scholar] [CrossRef] [Green Version]
- Yehuda, R.; Halligan, S.L.; Grossman, R. Childhood trauma and risk for PTSD: Relationship to intergenerational effects of trauma, parental PTSD, and cortisol excretion. Dev. Psychopathol. 2001, 13, 733–753. [Google Scholar] [CrossRef]
- Kramer, M.R.; Black, N.C.; Matthews, S.A.; James, S.A. The legacy of slavery and contemporary declines in heart disease mortality in the U.S. South. SSM Popul. Health 2017, 3, 609–617. [Google Scholar] [CrossRef]
- Nagata, D.K.; Trierweiler, S.J.; Talbot, R. Long-term effects of internment during early childhood on third-generation Japanese Americans. Am. J. Orthopsychiatry 1999, 69, 19–29. [Google Scholar] [CrossRef]
- Duran, E.; Duran, B.; Heart, M.Y.H.B.; Horse-Davis, S.Y. Healing the American Indian soul wound. In International Handbook of Multigenerational Legacies of Trauma; Danieli, Y., Ed.; Plenum Press: New York, NY, USA, 1998; pp. 341–354. [Google Scholar]
- Bombay, A.; Matheson, K.; Anisman, H. The intergenerational effects of Indian Residential Schools: Implications for the concept of historical trauma. Transcult. Psychiatry 2014, 51, 320–338. [Google Scholar] [CrossRef] [Green Version]
- Bear, U.R.; the AI-SUPERPFP Team; Beals, J.; Kaufman, C.E.; Manson, S.M. Boarding School Attendance and Physical Health Status of Northern Plains Tribes. Appl. Res. Qual. Life 2017, 13, 633–645. [Google Scholar] [CrossRef]
- Bear, U.R.; Ai-Superpfp the AI-SUPERPFP Team; Croy, C.D.; Kaufman, C.E.; Thayer, Z.M.; Manson, S.M. The relationship of five boarding school experiences and physical health status among Northern Plains Tribes. Qual. Life Res. 2017, 27, 153–157. [Google Scholar] [CrossRef]
- Lefler, J.L.; Belt, R. Historical Trauma, Stress, and Diabetes a Modern Model among the Eastern Band of Cherokees; University of Alabama Press: Tuscaloosa, AL, USA, 2009; pp. 61–78. [Google Scholar]
- Bird, A. Perceptions of epigenetics. Nature 2007, 447, 396–398. [Google Scholar] [CrossRef]
- Radley, J.J.; Kabbaj, M.; Jacobson, L.; Heydendael, W.; Yehuda, R.; Herman, J.P. Stress risk factors and stress-related pathology: Neuroplasticity, epigenetics and endophenotypes. Stress 2011, 14, 481–497. [Google Scholar] [CrossRef] [Green Version]
- Lefler, L.J.; Fox, S.L.; Altman, H.M.; Belt, T.; Townsend, R.; Hamilton, M.D.; Belt, R.; Cozzo, D.; James, J. The effect of traditional dietary practices on contemporary diseases among the Eastern Band of Cherokee Indians. In Under the Rattlesnake: Cherokee Health and Resiliency; Lefler, L.J., Ed.; University of Alabama Press: Tuscaloosa, AL, USA, 2009; pp. 79–101. [Google Scholar]
- Makhoul, Z.; Kristal, A.R.; Gulati, R.D.; Luick, B.; Bersamin, A.; O’Brien, D.; Hopkins, S.E.; Stephensen, C.B.; Stanhope, K.L.; Havel, P.J.; et al. Associations of obesity with triglycerides and C-reactive protein are attenuated in adults with high red blood cell eicosapentaenoic and docosahexaenoic acids. Eur. J. Clin. Nutr. 2011, 65, 808–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butt, M.S.; Sultan, M.T.; Aziz, M.; Naz, A.; Ahmed, W.; Kumar, N.; Imran, M. Persimmon (Diospyros kaki) fruit: Hidden phytochemicals and health claims. EXCLI J. 2015, 14, 542–561. [Google Scholar]
- Warne, D.; Wescott, S. Social Determinants of American Indian Nutritional Health. Curr. Dev. Nutr. 2019, 3, 12–18. [Google Scholar]
- Wiedman, D. Native American Embodiment of the Chronicities of Modernity: Reservation Food, Diabetes, and the Metabolic Syndrome among the Kiowa, Comanche, and Apache. Med. Anthr. Q. 2012, 26, 595–612. [Google Scholar] [CrossRef]
- Wang, J.; Xiong, X.; Feng, B. Effect ofCrataegusUsage in Cardiovascular Disease Prevention: An Evidence-Based Approach. Evid. Based Complement. Altern. Med. 2013, 2013, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Walker, A.F.; Marakis, G.; Simpson, E.; Hope, J.L.; Robinson, P.A.; Hassanein, M.; Simpson, H.C.R. Hypotensive effects of hawthorn for patients with diabetes taking prescription drugs: A randomised controlled trial. Br. J. Gen. Pract. 2006, 56, 437–443. [Google Scholar]
- Rahideh, S.T.; Shidfar, F.; Khandozi, N.; Rajab, A.; Hosseini, S.P.; Mirtaher, S.M. The effect of sumac (Rhus coriaria L.) powder on insulin resistance, malondialdehyde, high sensitive C-reactive protein and paraoxonase 1 activity in type 2 diabetic patients. J. Res. Med. Sci. 2014, 19, 933–938. [Google Scholar]
- Department of the Interior. Rules Governing the Court of Indian Offenses. 1883. Available online: https://rclinton.files.wordpress.com/2007/11/code-of-indian-offenses.pdf (accessed on 26 January 2021).
- Beltran, R.; Schultz, K.; Fernandez, A.R.; Walters, K.L.; Duran, B.; Evans-Campbell, T. From Ambivalence to Revitalization: Negotiating Cardiovascular Health Behaviors Related to Environmental and Historical Trauma in a Northwest American Indian Community. Am. Indian Alsk. Nativ. Ment. Health Res. 2018, 25, 103–128. [Google Scholar] [CrossRef]
- Goff, B.S.N.; Smith, D.B. Systemic traumatic stress: The couple adaptation to traumatic stress model. J. Marital. Fam. Ther. 2005, 31, 145–157. [Google Scholar] [CrossRef] [Green Version]
- Dirkzwager, A.J.E.; Bramsen, I.; Adèr, H.; Van Der Ploeg, H.M. Secondary Traumatization in Partners and Parents of Dutch Peacekeeping Soldiers. J. Fam. Psychol. 2005, 19, 217–226. [Google Scholar] [CrossRef]
- Figley, C.R. A five-phase treatment of post-traumatic stress disorder in families. J. Trauma. Stress 1988, 1, 127–141. [Google Scholar] [CrossRef]
- Palacios, F.J.; Portillo, C.J. Understanding native women’s health: Historical legacies. J. Transcult. Nurs. 2009, 20, 15–27. [Google Scholar] [CrossRef] [PubMed]
- National Law Center on Homelessness and Poverty. Racism, Homelessness, and COVID-19. 2020. Available online: https://nlchp.org/wp-content/uploads/2020/05/Racism-Homelessness-and-COVID-19-Fact-Sheet-_Final_2.pdf (accessed on 26 January 2021).
- Austin, A. Native Americans and Jobs: The Challenge and the Promise. 2013. Available online: https://www.epi.org/publication/bp370-native-americans-jobs/ (accessed on 26 January 2021).
- Bird, K. The Intergenerational Transmission of Poverty: An Overview. SSRN Electron. J. 2010. [Google Scholar] [CrossRef]
- First Nations Information Governance Centre. Chapter 36: Prenatal Health. First Nations Regional Health Survey (RHS) (2008/10): National Report on the Adult, Youth, and Children Living in First Nations Communities 2012. Available online: https://fnigc.ca/sites/default/files/docs/first_nations_regional_health_survey_rhs_2008-10_-_national_report.pdf (accessed on 26 January 2021).
- Kaijser, M.; Bonamy, A.-K.E.; Akre, O.; Cnattingius, S.; Granath, F.; Norman, M.; Ekbom, A. Perinatal Risk Factors for Diabetes in Later Life. Diabetes 2008, 58, 523–526. [Google Scholar] [CrossRef] [Green Version]
- Kajantie, E.; Osmond, C.; Barker, D.J.; Eriksson, J.G. Preterm Birth—A Risk Factor for Type 2 Diabetes?: The Helsinki Birth Cohort Study. Diabetes Care 2010, 33, 2623–2625. [Google Scholar] [CrossRef] [Green Version]
- Zhu, P.; Tao, F.; Hao, J.; Sun, Y.; Jiang, X. Prenatal life events stress: Implications for preterm birth and infant birthweight. Am. J. Obstet. Gynecol. 2010, 203, 34.e1–34.e8. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.E.; Gooze, R.A.; Lemeshow, S.; Whitaker, R.C. Quality of Early Maternal-Child Relationship and Risk of Adolescent Obesity. Pediatrics 2011, 129, 132–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klingensmith, W.C., 3rd; Noonan, C.; Goldberg, J.H.; Buchwald, D.; Kimball, J.T.; Manson, S.M. Decreased perfusion in the lateral wall of the left ventricle in PET/CT studies with 13N-ammonia: Evaluation in healthy adults. J. Nucl. Med. Technol. 2009, 37, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Suglia, S.F.; Koenen, K.C.; Boynton-Jarrett, R.; Chan, P.S.; Clark, C.J.; Danese, A.; Faith, M.S.; Goldstein, B.I.; Hayman, L.L.; Isasi, C.R.; et al. Childhood and Adolescent Adversity and Cardiometabolic Outcomes: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e15–e28. [Google Scholar] [CrossRef]
- Gilbert, L.K.; Breiding, M.J.; Merrick, M.T.; Thompson, W.W.; Ford, D.C.; Dhingra, S.S.; Parks, S.E. Childhood adversity and adult chronic disease: An update from ten states and the District of Columbia, 2010. Am. J. Prev. Med. 2015, 48, 345–349. [Google Scholar] [CrossRef]
- Rich-Edwards, J.W.; Mason, S.; Rexrode, K.; Spiegelman, N.; Hibert, E.; Kawachi, I.; Jun, H.J.; Wright, R.J. Physical and sexual abuse in childhood as predictors of early-onset cardiovascular events in women. Circulation 2012, 126, 920–927. [Google Scholar] [CrossRef] [Green Version]
- Loucks, E.B.; Almeida, N.D.; Taylor, S.E.; Matthews, K.A. Childhood Family Psychosocial Environment and Coronary Heart Disease Risk. Psychosom. Med. 2011, 73, 563–571. [Google Scholar] [CrossRef] [Green Version]
- Anda, R.F.; Felitti, V.J.; Bremner, J.D.; Walker, J.D.; Whitfield, C.; Perry, B.D.; Dube, S.R.; Giles, W.H. The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Warne, D.; Dulacki, K.; Spurlock, M.; Meath, T.; Davis, M.M.; Wright, B.; McConnell, K.J. Adverse Childhood Experiences (ACE) among American Indians in South Dakota and Associations with Mental Health Conditions, Alcohol Use, and Smoking. J. Health Care Poor Underserved 2017, 28, 1559–1577. [Google Scholar] [CrossRef]
- Koss, M.P.; Yuan, N.P.; Dightman, D.; Prince, R.J.; Polacca, M.; Sanderson, B.; Goldman, D. Adverse childhood exposures and alcohol dependence among seven Native American tribes. Am. J. Prev. Med. 2003, 25, 238–244. [Google Scholar] [CrossRef]
- Kenney, M.K.; Singh, G.K. Adverse Childhood Experiences among American Indian/Alaska Native Children: The 2011–2012 National Survey of Children’s Health. Scientifica 2016, 2016, 1–14. [Google Scholar] [CrossRef]
- Brockie, T.N.; Dana-Sacco, G.; Wallen, G.R.; Wilcox, H.C.; Campbell, J.C. The relationship of adverse childhood experiences to PTSD, depression, poly-drug use and suicide attempt in Reservation-based Native American adolescents and young adults. Am. J. Community Psychol. 2015, 55, 411–421. [Google Scholar] [CrossRef]
- McQuaid, R.J.; Bombay, A.; McInnis, O.A.; Matheson, K.; Anisman, H. Childhood adversity, perceived discrimination, and coping strategies in relation to depressive symptoms among First Nations adults in Canada: The moderating role of unsupportive social interactions from ingroup and outgroup members. Cult. Divers. Ethn. Minor. Psychol. 2015, 21, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Brayboy, J.B.M.; Lomawaima, K.T. Why don’t more Indians do better in school? The battle between U.S. schooling & American Indian/Alaska native education. Daedalus 2018, 147, 82–94. [Google Scholar]
- Eason, A.E.; Brady, L.M.; Fryberg, S.A. Reclaiming Representations & Interrupting the Cycle of Bias Against Native Americans. Daedalus 2018, 147, 70–81. [Google Scholar] [CrossRef]
- Powers, K.; Potthoff, S.J.; Bearinger, L.H.; Resnick, M.D. Does Cultural Programming Improve Educational Outcomes for American Indian Youth? J. Am. Indian Educ. 2003, 42, 17–49. [Google Scholar]
- U.S. Department of Education and Office of Civil Rights. 2013–2014 Civil Rights Data Collection: A First Look. 2016. Available online: https://www2.ed.gov/about/offices/list/ocr/docs/CRDC2013-14-first-look.pdf (accessed on 26 January 2021).
- Interagency Working Group on Youth Programs. American Indian and Alaska Native (AI/AN) Youth: Juvenile Justice. Youth Topics 2020. Available online: https://youth.gov/youth-topics/american-indian-alaska-native-youth/juvenile-justice (accessed on 26 January 2021).
- Chung, R.J.; Touloumtzis, C.; Gooding, H. Staying Young at Heart: Cardiovascular Disease Prevention in Adolescents and Young Adults. Curr. Treat. Options Cardiovasc. Med. 2015, 17, 61. [Google Scholar] [CrossRef] [Green Version]
- Child Trends Databank. Foster Care. 2018. Available online: https://www.childtrends.org/indicators/foster-care (accessed on 26 January 2021).
- Turney, K.; Wildeman, C. Mental and Physical Health of Children in Foster Care. Pediatrics 2016, 138, e20161118. [Google Scholar] [CrossRef] [Green Version]
- Steele, J.S.; Buchi, K.F. Medical and Mental Health of Children Entering the Utah Foster Care System. Pediatrics 2008, 122, e703–e709. [Google Scholar] [CrossRef] [PubMed]
- Yajnik, C.S.; Godbole, K.; Otiv, S.R.; Lubree, H.G. Fetal Programming of Type 2 Diabetes: Is sex important? Diabetes Care 2007, 30, 2754–2755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yajnik, C.S. Fetal Programming of Diabetes: Still So Much to Learn! Diabetes Care 2010, 33, 1146–1148. [Google Scholar] [CrossRef] [Green Version]
- Gaillard, R. Maternal obesity during pregnancy and cardiovascular development and disease in the offspring. Eur. J. Epidemiol. 2015, 30, 1141–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boney, C.M. Metabolic Syndrome in Childhood: Association With Birth Weight, Maternal Obesity, and Gestational Diabetes Mellitus. Pediatrics 2005, 115, e290–e296. [Google Scholar] [CrossRef] [Green Version]
- Gaillard, R.; Steegers, E.A.P.; Duijts, L.; Felix, J.F.; Hofman, A.; Franco, O.H.; Jaddoe, V.W.V. Childhood cardiometabolic outcomes of maternal obesity during pregnancy: The Generation R Study. Hypertension 2014, 63, 683–691. [Google Scholar] [CrossRef] [Green Version]
- Tan, H.C.; Roberts, J.; Catov, J.; Krishnamurthy, R.; Shypailo, R.; Bacha, F. Mother’s pre-pregnancy BMI is an important determinant of adverse cardiometabolic risk in childhood. Pediatr. Diabetes 2015, 16, 419–426. [Google Scholar] [CrossRef] [Green Version]
- Galliano, D.; Bellver, J. Female obesity: Short- and long-term consequences on the offspring. Gynecol. Endocrinol. 2013, 29, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Drake, A.J.; Reynolds, R.M. Impact of maternal obesity on offspring obesity and cardiometabolic disease risk. Reproduction 2010, 140, 387–398. [Google Scholar] [CrossRef]
- Zamora-Kapoor, A.; Nelson, L.; Buchwald, D. Maternal correlates of body mass index in American Indian/Alaska Native and White adolescents: Differences between mother/son and mother/daughter pairs. Eat. Behav. 2016, 20, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Lindberg, S.M.; Adams, A.K.; Prince, R.J. Early predictors of obesity and cardiovascular risk among American Indian children. Matern. Child Health J. 2012, 16, 1879–1886. [Google Scholar] [CrossRef] [Green Version]
- Dabelea, D.; Hanson, R.L.; Lindsay, R.S.; Pettitt, D.J.; Imperatore, G.; Gabir, M.M.; Roumain, J.; Bennett, P.H.; Knowler, W.C. Intrauterine exposure to diabetes conveys risks for type 2 diabetes and obesity: A study of discordant sibships. Diabetes 2000, 49, 2208–2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catalano, P.M.; Presley, L.; Minium, J.; Mouzon, S.H.-D. Fetuses of Obese Mothers Develop Insulin Resistance in Utero. Diabetes Care 2009, 32, 1076–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferland-McCollough, D.; Fernandeztwinn, D.S.; Cannell, I.G.; David, H.P.; Warner, M.; Vaag, A.; Borkjensen, J.; Brons, C.; Gant, T.W.; Willis, A.E.; et al. Programming of adipose tissue miR-483-3p and GDF-3 expression by maternal diet in type 2 diabetes. Cell Death Differ. 2012, 19, 1003–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godfrey, K.M.; Sheppard, A.; Gluckman, P.D.; Lillycrop, K.A.; Burdge, G.C.; McLean, C.; Rodford, J.; Slater-Jefferies, J.L.; Garratt, E.; Crozier, S.R.; et al. Epigenetic Gene Promoter Methylation at Birth Is Associated With Child’s Later Adiposity. Diabetes 2011, 60, 1528–1534. [Google Scholar] [CrossRef] [Green Version]
- Whincup, P.H.; Kaye, S.J.; Owen, C.G.; Huxley, R.; Cook, D.G.; Anazawa, S.; Barrett-Connor, E.; Bhargava, S.K.; Birgisdottir, B.E.; Carlsson, S. Birth weight and risk of type 2 diabetes: A systematic review. JAMA 2008, 300, 2886–2897. [Google Scholar]
- Leunissen, R.W.J.; Kerkhof, G.F.; Stijnen, T.; Hokken-Koelega, A. Timing and Tempo of First-Year Rapid Growth in Relation to Cardiovascular and Metabolic Risk Profile in Early Adulthood. JAMA 2009, 301, 2234–2242. [Google Scholar] [CrossRef] [Green Version]
- Luyckx, V.A.; Brenner, B.M. Low birth weight, nephron number, and kidney disease. Kidney Int. 2005, 68, S68–S77. [Google Scholar] [CrossRef] [Green Version]
- Raglan, G.B.; Lannon, S.M.; Jones, K.M.; Schulkin, J. Racial and Ethnic Disparities in Preterm Birth Among American Indian and Alaska Native Women. Matern. Child Health J. 2015, 20, 16–24. [Google Scholar] [CrossRef]
- Kuhle, S.; Maguire, B.; Ata, N.; MacInnis, N.; Dodds, L. Birth Weight for Gestational Age, Anthropometric Measures, and Cardiovascular Disease Markers in Children. J. Pediatr. 2017, 182, 99–106. [Google Scholar] [CrossRef]
- Weaver, L.T. Rapid growth in infancy: Balancing the interests of the child. J. Pediatr. Gastroenterol. Nutr. 2006, 43, 428–432. [Google Scholar] [CrossRef]
- Rosay, A. Violence against American Indian and Alaska Native Women and Men: 2010 Findings from the National Intimate Partner and Sexual Violence Survey; National Institute of Justice research report; U.S. Department of Justice, Office of Justice Programs: Washington, DC, USA, 2016. [Google Scholar]
- Barlow, A.; Mullany, B.; Neault, N.; Goklish, N.; Billy, T.; Hastings, R.; Lorenzo, S.; Kee, C.; Lake, K.; Redmond, C.; et al. Paraprofessional-Delivered Home-Visiting Intervention for American Indian Teen Mothers and Children: 3-Year Outcomes From a Randomized Controlled Trial. Am. J. Psychiatry 2015, 172, 154–162. [Google Scholar] [CrossRef]
- Robin, R.W.; Chester, B.; Rasmussen, J.K.; Jaranson, J.M.; Goldman, D. Prevalence and Characteristics of Trauma and Posttraumatic Stress Disorder in a Southwestern American Indian Community. Am. J. Psychiatry 1997, 154, 1582–1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Sonnega, A.; Bromet, E.; Hughes, M.; Nelson, C.B. Posttraumatic Stress Disorder in the National Comorbidity Survey. Arch. Gen. Psychiatry 1995, 52, 1048–1060. [Google Scholar] [CrossRef]
- Sancar, F.; Abbasi, J.; Bucher, K. Mortality Among American Indians and Alaska Natives. JAMA 2018, 319, 112. [Google Scholar] [CrossRef]
- Oetzel, J.; Duran, B. Intimate partner violence in American Indian and/or Alaska Native communities: A social ecological framework of determinants and interventions. Am. Indian Alsk. Nativ. Ment. Health Res. 2004, 11, 49–68. [Google Scholar] [CrossRef]
- Evans-Campbell, T.; Lindhorst, T.; Huang, B.; Walters, K.L. Interpersonal Violence in the Lives of Urban American Indian and Alaska Native Women: Implications for Health, Mental Health, and Help-Seeking. Am. J. Public Health 2006, 96, 1416–1422. [Google Scholar] [CrossRef]
- Deer, S. Relocation revisted: Sex trafficking of Native women in the United States. William Mitchell Law Rev. 2010, 36, 64. [Google Scholar]
- Hardy, A.; Brown-Rice, K. Violence and Residual Associations Among Native Americans Living on Tribal Lands. Prof. Couns. 2016, 6, 328–343. [Google Scholar] [CrossRef] [Green Version]
- Smith, A. Not an indian tradition: The sexual colonization of native peoples. Hypatia 2003, 18, 70. [Google Scholar] [CrossRef]
- Stumblingbear-Riddle, G.P.; Burlew, A.K.; Gaztambide, D.; Madore, M.R.; Neville, H.; Joseph, G. Standing with our American Indian and Alaska Native women, girls, and two-spirit people: Exploring the impact of and resources for survivors of human trafficking. J. Indig. Res. 2019, 7, 1. [Google Scholar]
- Males, M. Who Are Police Killing? 2014. Available online: http://www.cjcj.org/news/8113 (accessed on 26 January 2021).
- Chartrand, V. Unsettled Times: Indigenous Incarceration and the Links between Colonialism and the Penitentiary in Canada. Can. J. Criminol. Crim. Justice 2019, 61, 67–89. [Google Scholar] [CrossRef]
- Wijesekere, G. Incarceration of Indigenous and non-Indigenous adults, 1991–2001: Trends and differentials. Aust. Aborig. Stud. 2004, 2004, 54. [Google Scholar]
- Jeffries, S.; Bond, C.E. The Impact of Indigenous Status on Adult Sentencing: A Review of the Statistical Research Literature From the United States, Canada, and Australia. J. Ethn. Crim. Justice 2012, 10, 223–243. [Google Scholar] [CrossRef] [Green Version]
- Bassett, D.; Buchwald, D.; Manson, S. Posttraumatic stress disorder and symptoms among American Indians and Alaska Natives: A review of the literature. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 49, 417–433. [Google Scholar] [CrossRef]
- Beals, J.; Belcourt-Dittloff, A.; Garroutte, E.M.; Croy, C.; Jervis, L.L.; Whitesell, N.R.; Mitchell, C.M.; Manson, S.M.; Team, A.-S. Trauma and conditional risk of posttraumatic stress disorder in two American Indian reservation communities. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 895–905. [Google Scholar] [CrossRef] [Green Version]
- Aronson, B.D.; Palombi, L.C.; Walls, M.L. Rates and consequences of posttraumatic distress among American Indian adults with type 2 diabetes. J. Behav. Med. 2016, 39, 694–703. [Google Scholar] [CrossRef]
- Goetz, M.; Shah, A.; Goldberg, J.; Cheema, F.; Shallenberger, L.; Murrah, N.V.; Bremner, J.D.; Vaccarino, V. Posttraumatic stress disorder, combat exposure, and carotid intima-media thickness in male twins. Am. J. Epidemiol. 2014, 180, 989–996. [Google Scholar] [CrossRef] [Green Version]
- Burg, M.M.; Soufer, R. Post-traumatic Stress Disorder and Cardiovascular Disease. Curr. Cardiol. Rep. 2016, 18, 94. [Google Scholar] [CrossRef]
- Kibler, J.L.; Ma, M.; Tursich, M.; Malcolm, L.; Llabre, M.M.; Greenbarg, R.; Gold, S.N.; Beckham, J.C. Cardiovascular risks in relation to posttraumatic stress severity among young trauma-exposed women. J. Affect. Disord. 2018, 241, 147–153. [Google Scholar] [CrossRef]
- Lee, S.Y.; Park, C.L.; Pescatello, L.S. How trauma influences cardiovascular responses to stress: Contributions of posttraumatic stress and cognitive appraisals. J. Behav. Med. 2020, 43, 131–142. [Google Scholar] [CrossRef]
- Burnette, C.E.; Ka’Apu, K.; Scarnato, J.M.; Liddell, J. Cardiovascular Health among U.S. Indigenous Peoples: A Holistic and Sex-Specific Systematic Review. J. Evid. Based Soc. Work. 2020, 17, 24–48. [Google Scholar] [CrossRef]
- Thayer, Z.; Barbosa-Leiker, C.; McDonell, M.; Nelson, L.; Buchwald, D.; Manson, S. Early life trauma, post-traumatic stress disorder, and allostatic load in a sample of American Indian adults. Am. J. Hum. Biol. 2017, 29. [Google Scholar] [CrossRef] [Green Version]
- Tehee, M.; Buchwald, D.; Booth-LaForce, C.; Omidpanah, A.; Manson, S.M.; Goins, R.T. Traumatic Stress, Social Support, and Health Among Older American Indians: The Native Elder Care Study. J. Gerontol. Ser. B 2017, 74, 908–917. [Google Scholar] [CrossRef]
- Goins, R.T.; Noonan, C.; Gonzales, K.; Winchester, B.; Bradley, V.L. Association of depressive symptomology and psychological trauma with diabetes control among older American Indian women: Does social support matter? J. Diabetes Its Complicat. 2017, 31, 669–674. [Google Scholar] [CrossRef] [Green Version]
- Potter, L.N.; Brondolo, E.; Smyth, J.M. Biopsychosocial correlates of discrimination in daily life: A review. Stigma Health 2019, 4, 38–61. [Google Scholar] [CrossRef]
- Wylie, L.; McConkey, S. Insiders’ Insight: Discrimination against Indigenous Peoples through the Eyes of Health Care Professionals. J. Racial Ethn. Health Disparities 2018, 6, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Shear, S.B.; Knowles, R.T.; Soden, G.J.; Castro, A.J. Manifesting Destiny: Re/presentations of Indigenous Peoples in K–12 U.S. History Standards. Theory Res. Soc. Educ. 2015, 43, 68–101. [Google Scholar] [CrossRef]
- Wayne, J. An incomplete history: Representation of American Indians in state social studies standards. J. Am. Indian Educ. 2009, 48, 18–32. [Google Scholar]
- Chandler, P.T.; Branscombe, A.; Mayshack, M. Mom, have you ever seen a real Indian? The intersection of personal identity and social studies education. Soc. Stud. Rev. 2013, 52, 85–91. [Google Scholar]
- Gutierrez-Gomez, C.; Pauly, N. Early Childhood Curriculum Related to American Indians: Appropriate or Not? Child. Educ. 2006, 82, 201–206. [Google Scholar] [CrossRef]
- Pewewardy, C. Fluff and Feathers: Treatment of American Indians in the Literature and the Classroom. Equity Excel. Educ. 1998, 31, 69–76. [Google Scholar] [CrossRef]
- Brophy, J. Elementary students learn about Native Americans: The development of knowledge and empathy. Soc. Educ. 1999, 63, 39–45. [Google Scholar]
- Merino, M.-E.; Mellor, D.J.; Saiz, J.L.; Quilaqueo, D. Perceived discrimination amongst the indigenous Mapuche people in Chile: Some comparisons with Australia. Ethn. Racial Stud. 2009, 32, 802–822. [Google Scholar] [CrossRef]
- First Nations Development Institute and Echo Hawk Consulting. Research Findings: Compilation of All Research. Reclaiming Native Truth: A Project to Dispel America’s Myths and Misconceptions 2018. 2020. Available online: https://rnt.firstnations.org/wp-content/uploads/2018/06/FullFindingsReport-screen.pdf (accessed on 26 January 2021).
- Miller, A.; Ross, S.D. They Are Not Us: Framing of American Indians by theBoston Globe. Howard J. Commun. 2004, 15, 245–259. [Google Scholar] [CrossRef]
- Fryberg, S.A.; Markus, H.R.; Oyserman, D.; Stone, J.M. Of Warrior Chiefs and Indian Princesses: The Psychological Consequences of American Indian Mascots. Basic Appl. Soc. Psychol. 2008, 30, 208–218. [Google Scholar] [CrossRef]
- Mays, V.M.; Cochran, S.D.; Barnes, N.W. Race, Race-Based Discrimination, and Health Outcomes Among African Americans. Annu. Rev. Psychol. 2007, 58, 201–225. [Google Scholar] [CrossRef] [Green Version]
- Sittner, K.J.; Greenfield, B.L.; Walls, M.L. Microaggressions, diabetes distress, and self-care behaviors in a sample of American Indian adults with type 2 diabetes. J. Behav. Med. 2018, 41, 122–129. [Google Scholar] [CrossRef]
- Thayer, Z.M.; Blair, I.V.; Buchwald, D.S.; Manson, S.M. Racial discrimination associated with higher diastolic blood pressure in a sample of American Indian adults. Am. J. Phys. Anthr. 2017, 163, 122–128. [Google Scholar] [CrossRef]
- Walls, M.L.; Sittner, K.J.; Aronson, B.D.; Forsberg, A.K.; Whitbeck, L.B.; Al’Absi, M. Stress Exposure and Physical, Mental, and Behavioral Health among American Indian Adults with Type 2 Diabetes. Int. J. Environ. Res. Public Health 2017, 14, 1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, R.; Tobias, M.; Jeffreys, M.; Waldegrave, K.; Karlsen, S.; Nazroo, J. Effects of self-reported racial discrimination and deprivation on Māori health and inequalities in New Zealand: Cross-sectional study. Lancet 2006, 367, 2005–2009. [Google Scholar] [CrossRef]
- Eliassen, B.-M.; Melhus, M.; Hansen, K.L.; Broderstad, A.R. Marginalisation and cardiovascular disease among rural Sami in Northern Norway: A population-based cross-sectional study. BMC Public Health 2013, 13, 1–522. [Google Scholar] [CrossRef] [Green Version]
- Everson-Rose, S.A.; Lewis, T.T. Psychosocial Factors and Cardiovascular Diseases. Annu. Rev. Public Health 2005, 26, 469–500. [Google Scholar] [CrossRef]
- Whitbeck, L.B.; McMorris, B.J.; Hoyt, D.R.; Stubben, J.D.; LaFromboise, T. Perceived Discrimination, Traditional Practices, and Depressive Symptoms among American Indians in the Upper Midwest. J. Health Soc. Behav. 2002, 43, 400–418. [Google Scholar] [CrossRef]
- Bals, M.; Turi, A.L.; Skre, I.; Kvernmo, S. Internalization symptoms, perceived discrimination, and ethnic identity in indigenous Sami and non-Sami youth in Arctic Norway. Ethn. Health 2010, 15, 165–179. [Google Scholar] [CrossRef] [Green Version]
- Parker, M.; Duran, B.; Walters, K. The Relationship Between Bias-Related Victimization and Generalized Anxiety Disorder Among American Indian and Alaska Native Lesbian, Gay, Bisexual, Transgender, Two-Spirit Community Members. Int. J. Indig. Health 2017, 12, 64–83. [Google Scholar] [CrossRef] [Green Version]
- Hartshorn, K.J.S.; Whitbeck, L.B.; Hoyt, D.R. Exploring the Relationships of Perceived Discrimination, Anger, and Aggression among North American Indigenous Adolescents. Soc. Ment. Health 2012, 2, 53–67. [Google Scholar] [CrossRef] [Green Version]
- Day, A.; Davey, L.; Wanganeen, R.; Casey, S.; Howells, K.; Nakata, M. Symptoms of trauma, perceptions of discrimination, and anger: A comparison between Australian indigenous and nonindigenous prisoners. J. Interpers. Violence 2008, 23, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Cormack, D.; Tobias, M.; Yeh, L.-C.; Talamaivao, N.; Minster, J.; Timutimu, R. The pervasive effects of racism: Experiences of racial discrimination in New Zealand over time and associations with multiple health domains. Soc. Sci. Med. 2012, 74, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Currie, C.L.; Copeland, J.L.; Metz, G.A. Childhood racial discrimination and adult allostatic load: The role of Indigenous cultural continuity in allostatic resiliency. Soc. Sci. Med. 2019, 241, 112564. [Google Scholar] [CrossRef]
- Shepherd, C.C.; Li, J.; Cooper, M.N.; Hopkins, K.D.; Farrant, B.M. The impact of racial discrimination on the health of Australian Indigenous children aged 5–10 years: Analysis of national longitudinal data. Int. J. Equity Health 2017, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Carpio, M.V. The lost generation: American Indian women and sterilization abuse. Soc. Justice 2004, 31, 40–53. [Google Scholar]
- Rutecki, G.W. Forced sterilization of native Americans: Later twentieth century physician cooperation with national eugenic policies? Ethics Med. 2011, 27, 33–42. [Google Scholar]
- Pacheco, C.M.; Daley, S.M.; Brown, T.; Filippi, M.; Greiner, K.A.; Daley, C.M. Moving Forward: Breaking the Cycle of Mistrust Between American Indians and Researchers. Am. J. Public Health 2013, 103, 2152–2159. [Google Scholar] [CrossRef]
- Browne, A.J.; Fiske, J.-A. First Nations women’s encounters with mainstream health care services. West. J. Nurs. Res. 2001, 23, 126–147. [Google Scholar] [CrossRef]
- Kitching, G.T.; Firestone, M.; Schei, B.; Wolfe, S.; Bourgeois, C.; O’Campo, P.; Rotondi, M.; Nisenbaum, R.; Maddox, R.; Smylie, J. Unmet health needs and discrimination by healthcare providers among an Indigenous population in Toronto, Canada. Can. J. Public Health 2020, 111, 40–49. [Google Scholar] [CrossRef] [Green Version]
- Puumala, S.E.; Burgess, K.M.; Kharbanda, A.B.; Zook, H.G.; Castille, D.M.; Pickner, W.J.; Payne, N.R. The Role of Bias by Emergency Department Providers in Care for American Indian Children. Med. Care 2016, 54, 562–569. [Google Scholar] [CrossRef] [Green Version]
- Hulen, E.; Hardy, L.J.; Teufel-Shone, N.; Sanderson, P.R.; Schwartz, A.L.; Begay, R.C. Community Based Participatory Research (CBPR): A Dynamic Process of Health care, Provider Perceptions and American Indian Patients’ Resilience. J. Health Care Poor Underserved 2019, 30, 221–237. [Google Scholar] [CrossRef]
- Nesoff, E.D.; Brownstein, J.N.; Veazie, M.; O’Leary, M.; Brody, E.A. Time-to-Treatment for Myocardial Infarction: Barriers and Facilitators Perceived by American Indians in Three Regions. J. Community Health 2016, 42, 129–138. [Google Scholar] [CrossRef]
- Call, K.T.; McAlpine, D.D.; Johnson, P.J.; Beebe, T.J.; McRae, J.A.; Song, Y. Barriers to Care Among American Indians in Public Health Care Programs. Med. Care 2006, 44, 595–600. [Google Scholar] [CrossRef]
- Cerón, A.; Ruano, A.L.; Sánchez, S.; Chew, A.S.; Díaz, D.; Hernández, A.; Flores, W. Abuse and discrimination towards indigenous people in public health care facilities: Experiences from rural Guatemala. Int. J. Equity Health 2016, 15, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, A.; Fleming, K.; Markwick, N.; Morrison, T.; Lagimodiere, L.; Kerr, T.; Society, W.A.H.R. “They treated me like crap and I know it was because I was Native”: The healthcare experiences of Aboriginal peoples living in Vancouver’s inner city. Soc. Sci. Med. 2017, 178, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Gonzales, K.L.; Harding, A.K.; Lambert, W.E.; Fu, R.; Henderson, W.G. Perceived Experiences of Discrimination in Health Care: A Barrier for Cancer Screening Among American Indian Women with Type 2 Diabetes. Women’s Health Issues 2013, 23, e61–e67. [Google Scholar] [CrossRef] [Green Version]
- Trivedi, A.N.; Ayanian, J.Z. Perceived discrimination and use of preventive health services. J. Gen. Intern. Med. 2006, 21, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzales, K.L.; Lambert, W.E.; Fu, R.; Jacob, M.; Harding, A.K. Perceived Racial Discrimination in Health Care, Completion of Standard Diabetes Services, and Diabetes Control Among a Sample of American Indian Women. Diabetes Educ. 2014, 40, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Burgess, D.J.; Ding, Y.; Hargreaves, M.; Van Ryn, M.; Phelan, S. The Association between Perceived Discrimination and Underutilization of Needed Medical and Mental Health Care in a Multi-Ethnic Community Sample. J. Health Care Poor Underserved 2008, 19, 894–911. [Google Scholar] [CrossRef]
- Chambers, R.A.; Rosenstock, S.; Neault, N.; Kenney, A.; Richards, J.; Begay, K.; Blackwater, T.; Laluk, O.; Duggan, C.; Reid, R.; et al. A home-visiting diabetes prevention and management program for American Indian youth: The together on diabetes trial. Diabetes Educ. 2015, 41, 729–747. [Google Scholar] [CrossRef]
- Ducharme-Smith, K.; Rosenstock, S.; Garcia-Larsen, V.; Larzelere, F.; Chambers, R.; Kenney, A.; Reid, R.; Nelson, L.; Richards, J.; Begay, M.; et al. Quality of Diet and Cardio-Metabolic Outcomes in Native American Adolescents Participating in the Together on Diabetes Home-Visiting Program. Curr. Dev. Nutr. 2020, 4, 180. [Google Scholar] [CrossRef]
- Rosas, L.G.; Vasquez, J.J.; Naderi, R.; Jeffery, N.; Hedlin, H.; Qin, F.; LaFromboise, T.; Megginson, N.; Pasqua, C.; Flores, O.; et al. Development and evaluation of an enhanced diabetes prevention program with psychosocial support for urban American Indians and Alaska natives: A randomized controlled trial. Contemp. Clin. Trials 2016, 50, 28–36. [Google Scholar] [CrossRef]
- Mendham, A.E.; Duffield, R.; Marino, F.; Coutts, A.J. A 12-week sports-based exercise programme for inactive Indigenous Australian men improved clinical risk factors associated with type 2 diabetes mellitus. J. Sci. Med. Sport 2015, 18, 438–443. [Google Scholar] [CrossRef]
- Canuto, K.; Cargo, M.; Li, M.; D’Onise, K.; Esterman, A.; McDermott, R. Pragmatic randomised trial of a 12-week exercise and nutrition program for Aboriginal and Torres Strait Islander women: Clinical results immediate post and 3 months follow-up. BMC Public Health 2012, 12, 933. [Google Scholar] [CrossRef] [Green Version]
- Tobe, S.W.; Pylypchuk, G.; Wentworth, J.; Kiss, A.; Szalai, J.P.; Perkins, N.; Hartman, S.; Ironstand, L.; Hoppe, J. Effect of nurse-directed hypertension treatment among First Nations people with existing hypertension and diabetes mellitus: The Diabetes Risk Evaluation and Microalbuminuria (DREAM 3) randomized controlled trial. Can. Med. Assoc. J. 2006, 174, 1267–1271. [Google Scholar] [CrossRef] [Green Version]
- Whitegoat, W.; Vu, J.; Thompson, K.; Gallagher, J. Mental Health in Diabetes Prevention and Intervention Programs in American Indian/Alaska Native Communities. Wash. Univ. J. Am. Indian Alsk. Nativ. Health 2015, 1, 4. [Google Scholar]
- Scarton, J.L.; de Groot, M. Emotional and behavioral aspects of diabetes in American Indians/Alaska Natives: A systematic literature review. Health Educ. Behav. 2017, 44, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Indian Health Service. Special Diabetes Program for Indians (SDPI). 2020. Available online: https://www.ihs.gov/sdpi/ (accessed on 26 January 2021).
- Mohatt, N.V.; Fok, C.C.T.; Burket, R.; Henry, D.; Allen, J. Assessment of awareness of connectedness as a culturally-based protective factor for Alaska native youth. Cult. Divers. Ethn. Minor. Psychol. 2011, 17, 444–455. [Google Scholar] [CrossRef] [Green Version]
- Durie, M. Whaiora: Māori Health Development; Oxford University Press: Oxford, UK, 1994. [Google Scholar]
- Warne, D. Traditional perspectives on child and family health. Paediatr. Child Health 2005, 10, 542–544. [Google Scholar] [CrossRef] [Green Version]
- Whalen, D.H.; Moss, M.; Baldwin, D. Healing through language: Positive physical health effects of indigenous language use. F1000Research 2016, 5, 852. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.; Rasmus, S. Yup’ik Communities Turn to Indigenous Knowledge to Prevent Risk for Youth Suicide and Alcohol Abuse. 2018. Available online: https://nimhd.nih.gov/news-events/features/community-health/yupik-community.html (accessed on 26 January 2021).
- Qungasvik (Toolbox) Training and Teachings Manual. 2017. Available online: http://www.qungasvik.org/preview/ (accessed on 26 January 2021).
- Carlson, A.E.; Aronson, B.D.; Unzen, M.; Lewis, M.; Benjamin, G.J.; Walls, M.L. Apathy and Type 2 Diabetes among American Indians: Exploring the Protective Effects of Traditional Cultural Involvement. J. Health Care Poor Underserved 2017, 28, 770–783. [Google Scholar] [CrossRef] [Green Version]
- Garroutte, E.M.; Goldberg, J.; Beals, J.; Herrell, R.; Manson, S.M.; The AI-SUPERPFP Team. Spirituality and attempted suicide among American Indians. Soc. Sci. Med. 2003, 56, 1571–1579. [Google Scholar] [CrossRef]
- Coe, K.; Attakai, A.; Papenfuss, M.; Giuliano, A.; Martin, L.; Nuvayestewa, L. Traditionalism and its relationship to disease risk and protective behaviors of women living on the hopi reservation. Health Care Women Int. 2004, 25, 391–410. [Google Scholar] [CrossRef]
- Davis, R.A. Coping with diabetes and generational trauma in Salish tribal communities. Fourth World J. 2013, 12, 45. [Google Scholar]
- Narayan, K.M.; Hoskin, M.; Kozak, D.; Kriska, A.M.; Hanson, R.L.; Pettitt, D.J.; Nagi, D.K.; Bennett, P.H.; Knowler, W.C. Randomized clinical trial of lifestyle interventions in Pima Indians: A pilot study. Diabet. Med. 1998, 15, 66–72. [Google Scholar] [CrossRef]
- Kaholokula, J.K.; Look, M.; Mabellos, T.; Zhang, G.; De Silva, M.; Yoshimura, S.; Solatorio, C.; Wills, T.; Seto, T.B.; Sinclair, K.A. Cultural Dance Program Improves Hypertension Management for Native Hawaiians and Pacific Islanders: A Pilot Randomized Trial. J. Racial Ethn. Health Disparities 2017, 4, 35–46. [Google Scholar] [CrossRef] [Green Version]
- Choi, W.S.; Beebe, L.A.; Nazir, N.; Kaur, B.; Hopkins, M.; Talawyma, M.; Shireman, T.I.; Yeh, H.; Greiner, K.A.; Daley, C.M. All nations breath of life: A randomized trial of smoking cessation for American Indians. Am. J. Prev. Med. 2016, 51, 743–751. [Google Scholar] [CrossRef] [Green Version]
- Jobe, J.B.; Adams, A.K.; Henderson, J.A.; Karanja, N.; Lee, E.T.; Walters, K.L. Community-Responsive Interventions to Reduce Cardiovascular Risk in American Indians. J. Prim. Prev. 2012, 33, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Debruyn, L.; Fullerton, L.; Satterfield, D.; Frank, M. Integrating Culture and History to Promote Health and Help Prevent Type 2 Diabetes in American Indian/Alaska Native Communities: Traditional Foods Have Become a Way to Talk About Health. Prev. Chronic Dis. 2020, 17, E12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, M.E.; Myhra, L.L.; Vieaux, L.E.; Sly, G.; Anderson, A.; Marshall, K.E.; Marshall, E.J.; The Remember the Removal Alumni Association. Evaluation of a Native Youth Leadership Program Grounded in Cherokee Culture: The Remember the Removal Program. Am. Indian Alsk. Nativ. Ment. Health Res. 2019, 26, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Sama-Miller, E.; Akers, L.; Mraz-Esposito, A.; Coughlin, R.; Zukiewicz, M. Home Visiting Evidence of Effectiveness Review: Executive Summary. 2019. Available online: https://www.mathematica.org/our-publications-and-findings/publications/september-2019-home-visiting-evidence-of-effectiveness-review-executive-summary (accessed on 26 January 2021).
- Gaynair, G.; Friedman, M. Tribal Home Visiting: Cultural Traditions Offer Protective Force. 2018. Available online: https://www.urban.org/features/tribal-home-visiting-cultural-traditions-offer-protective-force (accessed on 26 January 2021).
- Barlow, A.; Varipatis-Baker, E.; Speakman, K.; Ginsburg, G.; Friberg, I.; Goklish, N.; Cowboy, B.; Fields, P.; Hastings, R.; Pan, W.; et al. Home-visiting intervention to improve child care among American Indian adolescent mothers: A randomized trial. Arch. Pediatr. Adolesc. Med. 2006, 160, 1101–1107. [Google Scholar] [CrossRef] [Green Version]
- Barlow, A.; Mullany, B.; Neault, N.; Compton, S.; Carter, A.; Hastings, R.; Billy, T.; Coho-Mescal, V.; Lorenzo, S.; Walkup, J.T. Effect of a Paraprofessional Home-Visiting Intervention on American Indian Teen Mothers’ and Infants’ Behavioral Risks: A Randomized Controlled Trial. Am. J. Psychiatry 2013, 170, 83–93. [Google Scholar] [CrossRef]
- Haroz, E.E.; Ingalls, A.; Kee, C.; Goklish, N.; Neault, N.; Begay, M.; Barlow, A. Informing Precision Home Visiting: Identifying Meaningful Subgroups of Families Who Benefit Most from Family Spirit. Prev. Sci. 2019, 20, 1244–1254. [Google Scholar] [CrossRef]
- Walkup, J.T.; Barlow, A.; Mullany, B.C.; Pan, W.; Goklish, N.; Hasting, R.; Cowboy, B.; Fields, P.; Baker, E.V.; Speakman, K.; et al. Randomized Controlled Trial of a Paraprofessional-Delivered In-Home Intervention for Young Reservation-Based American Indian Mothers. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 591–601. [Google Scholar] [CrossRef]
- Esposito, A.M.; del Grosso, P.; Kleinman, R.; Sama-Miller, E.; Paulsell, D. Assessing the Evidence of Effectiveness of Home Visiting Program Models Implemented in Tribal Communities. 2014. Available online: https://www.mathematica.org/our-publications-and-findings/publications/assessing-the-evidence-of-effectiveness-of-home-visiting-program-models-implemented-in-tribal-communities (accessed on 26 January 2021).
- Oxford, M.; Booth-LaForce, C.; Echo-Hawk, A.; Madesclaire, O.; Parrish, L.; Widner, M.; Petras, A.; Abrahamson-Richards, T.; Nelson, K.; Buchwald, D.; et al. Promoting First Relationships®: Implementing a Home Visiting Research Program in Two American Indian Communities. Can. J. Nurs. Res. 2020, 52, 149–156. [Google Scholar] [CrossRef]
- Novins, D.; Meyer, A.; Beltangady, M. Contextual issues for implementation and evaluation of home-visitation programs for american indian and alaska native communities: An introduction to the tribal maternal, infant, and early childhood home visiting program. Child Adolesc. Soc. Work. J. 2018, 39, 259–264. [Google Scholar] [CrossRef]
- Costello, E.J.; Compton, S.N.; Keeler, G.; Angold, A. Relationships between Poverty and Psychopathology: A Natural Experiment. JAMA 2003, 290, 2023–2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamsen, C.; Schroeder, S.; Lemire, S.; Carter, P. Education, Income, and Employment and Prevalence of Chronic Disease Among American Indian/Alaska Native Elders. Prev. Chronic Dis. 2018, 15, 37. [Google Scholar] [CrossRef] [Green Version]
- Foxworth, R.; Liu, A.H.; Sokhey, A.E. Incorporating Native American History into the Curriculum: Descriptive Representation or Campaign Contributions? Soc. Sci. Q. 2015, 96, 955–969. [Google Scholar] [CrossRef]
- New Zealand Government, M.o.E. New Zealand Education System Overview; New Zealand Government, M.o.E.: Wellington, New Zealand, 2015. [Google Scholar]
- Martinez, D. School Culture and American Indian Educational Outcomes. Procedia Soc. Behav. Sci. 2014, 116, 199–205. [Google Scholar] [CrossRef] [Green Version]
- Papps, E.; Ramsden, I. Cultural Safety in Nursing: The New Zealand Experience. Int. J. Qual. Health Care 1996, 8, 491–497. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, D.-A.L.; Kamaka, M.L.; Kaulukukui, C.M. An Innovative Approach to Developing a Cultural Competency Curriculum; Efforts at the John A. Burns School of Medicine, Department of Native Hawaiian Health. Hawaii Med. J. 2011, 70, 15–19. [Google Scholar] [PubMed]
- McElfish, P.A.; Moore, R.; Buron, B.; Hudson, J.; Long, C.R.; Purvis, R.S.; Schulz, T.K.; Rowland, B.; Warmack, T.S. Integrating Interprofessional Education and Cultural Competency Training to Address Health Disparities. Teach. Learn. Med. 2018, 30, 213–222. [Google Scholar] [CrossRef]
- Lee, W.K.; Harris, C.C.D.; Mortensen, K.A.; Long, L.M.; Sugimoto-Matsuda, J. Enhancing student perspectives of humanism in medicine: Reflections from the Kalaupapa service learning project. BMC Med. Educ. 2016, 16, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, M.; Prunuske, A. The Development of an Indigenous Health Curriculum for Medical Students. Acad. Med. 2017, 92, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Lewis, M.E. The Effects of an Indigenous Health Curriculum for Medical Students. Med. Sci. Educ. 2020, 30, 891–903. [Google Scholar] [CrossRef]
- Ambrose, A.J.H.; Andaya, J.M.; Yamada, S.; Maskarinec, G.G. Social Justice in Medical Education: Strengths and Challenges of a Student-Driven Social Justice Curriculum. Hawai’i J. Med. Public Health 2014, 73, 244–250. [Google Scholar]
- Bakshi, S.; James, A.; Hennelly, M.O.; Karani, R.; Palermo, A.-G.; Jakubowski, A.; Ciccariello, C.; Atkinson, H. The Human Rights and Social Justice Scholars Program: A Collaborative Model for Preclinical Training in Social Medicine. Ann. Glob. Health 2015, 81, 290–297. [Google Scholar] [CrossRef]
- Coria, A.; McKelvey, T.G.; Charlton, P.; Woodworth, M.; Lahey, T. The Design of a Medical School Social Justice Curriculum. Acad. Med. 2013, 88, 1442–1449. [Google Scholar] [CrossRef]
- Hixon, A.L.; Yamada, S.; Farmer, P.E.; Maskarinec, G.G. Social justice: The heart of medical education. Soc. Med. 2013, 7, 161. [Google Scholar]
- Schiff, T.; Rieth, K. Projects in Medical Education: “Social Justice In Medicine” A Rationale for an Elective Program as Part of the Medical Education Curriculum at John A. Burns School of Medicine. Hawai’i J. Med. Public Health 2012, 71, 64–67. [Google Scholar]
- The Leaders in Indigenous Medical Education (LIME) Network. Pedagogical Principles & Approach. 2016. Available online: https://www.limenetwork.net.au/resources-lime-publications/curriculum-framework/pedagogical-principles-approach/ (accessed on 26 January 2021).
- Dumbrill, G.C.; Green, J. Indigenous Knowledge in the Social Work Academy. Soc. Work. Educ. 2008, 27, 489–503. [Google Scholar] [CrossRef]
- Burnette, C.E.; Figley, C.R. Historical Oppression, Resilience, and Transcendence: Can a Holistic Framework Help Explain Violence Experienced by Indigenous People? Soc. Work 2016, 62, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Belone, L.; Orosco, A.; Damon, E.; Smith-McNeal, W.; Rae, R.; Sherpa, M.L.; Myers, O.B.; Omeh, A.O.; Wallerstein, N. The piloting of a culturally centered American Indian family prevention program: A CBPR partnership between Mescalero Apache and the University of New Mexico. Public Health Rev. 2017, 38, 1–13. [Google Scholar] [CrossRef]
- Warne, D.; Frizzell, L.B. American Indian health policy: Historical trends and contemporary issues. Am. J. Public Health 2014, 104, S263–S267. [Google Scholar] [CrossRef]

{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewis, M.E.; Volpert-Esmond, H.I.; Deen, J.F.; Modde, E.; Warne, D. Stress and Cardiometabolic Disease Risk for Indigenous Populations throughout the Lifespan. Int. J. Environ. Res. Public Health 2021, 18, 1821. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041821
Lewis ME, Volpert-Esmond HI, Deen JF, Modde E, Warne D. Stress and Cardiometabolic Disease Risk for Indigenous Populations throughout the Lifespan. International Journal of Environmental Research and Public Health. 2021; 18(4):1821. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041821
Chicago/Turabian StyleLewis, Melissa E., Hannah I. Volpert-Esmond, Jason F. Deen, Elizabeth Modde, and Donald Warne. 2021. "Stress and Cardiometabolic Disease Risk for Indigenous Populations throughout the Lifespan" International Journal of Environmental Research and Public Health 18, no. 4: 1821. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041821