
Increased Risk of Migraine in Patients with Chronic Periodontitis: A Population-Based Cohort Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
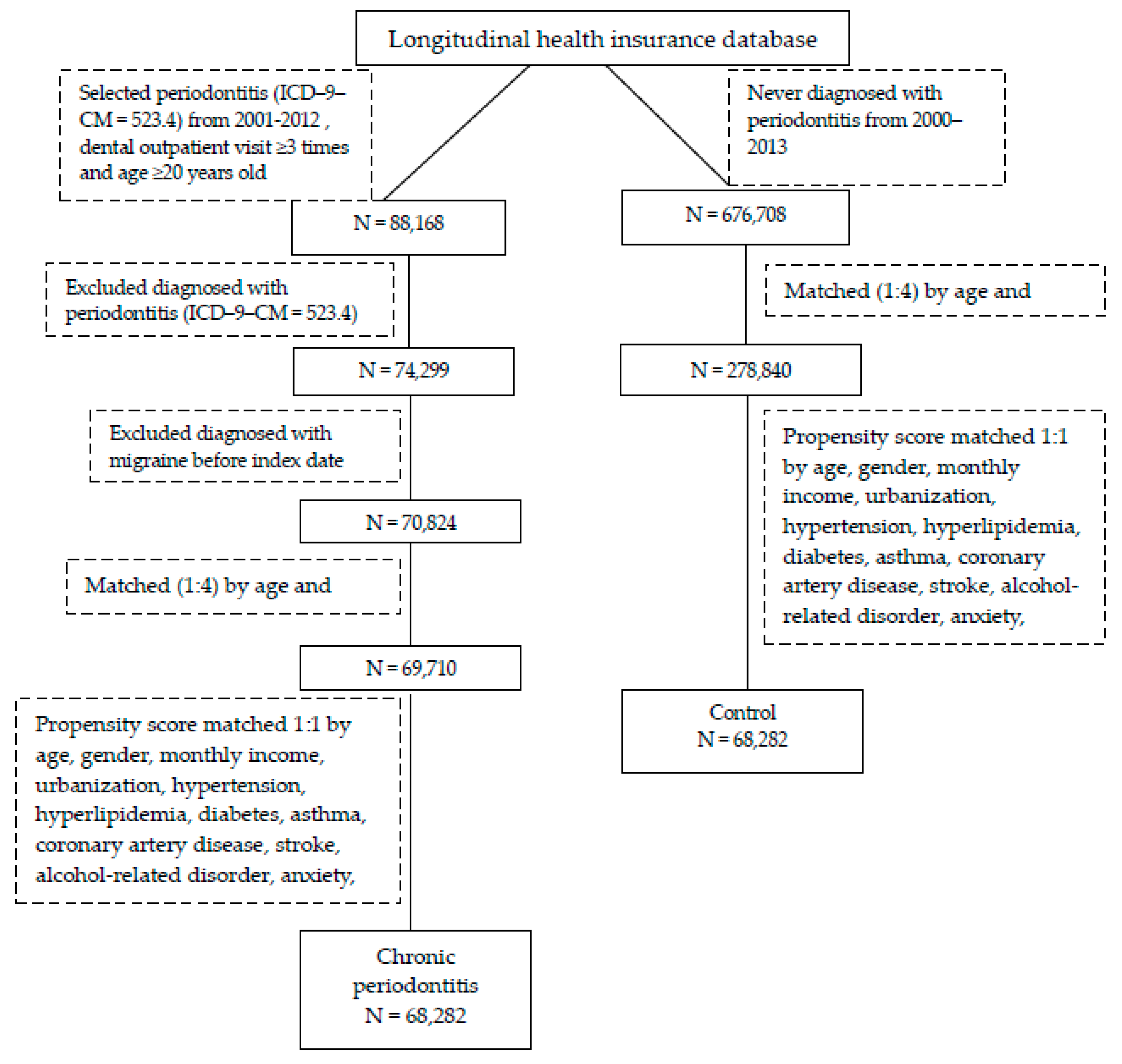
2.2. Study Design and Sampled Participants
2.3. Outcome Measurement and Comorbidities
2.4. Statistical Analysis
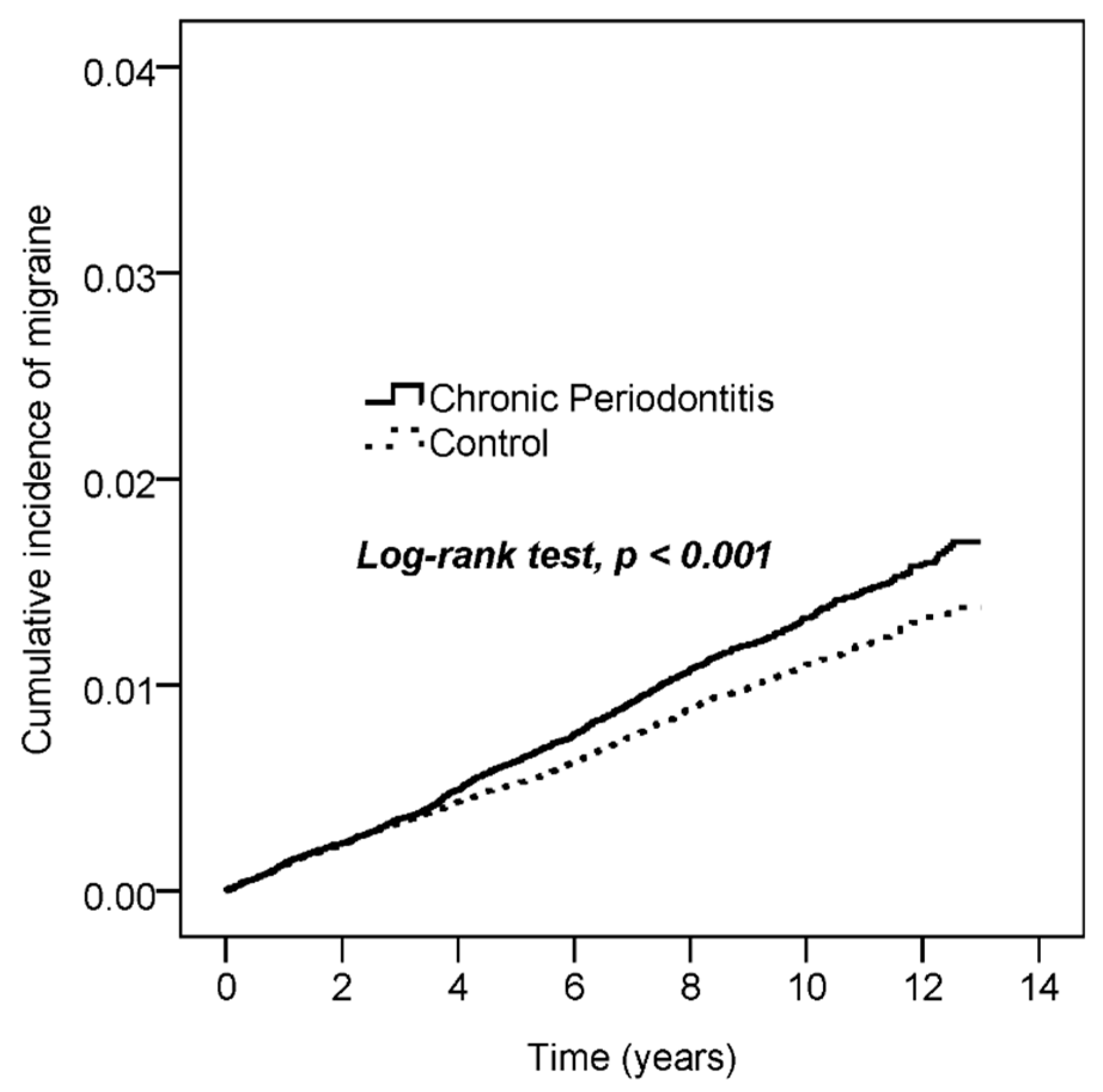
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Noseda, R.; Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, cortical spreading depression, sensitization, and modulation of pain. Pain 2013, 154, 44–53. [Google Scholar] [CrossRef] [Green Version]
- Charles, A. The evolution of a migraine attack—A review of recent evidence. Headache 2013, 53, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.J.; Fuh, J.L.; Young, Y.H.; Lu, S.R.; Shia, B.C. Prevalence of migraine in Taipei, Taiwan: A population-based survey. Cephalalgia 2000, 20, 566–572. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathew, N.T. Pathophysiology of chronic migraine and mode of action of preventive medications. Headache 2011, 51, 84–92. [Google Scholar] [CrossRef]
- Egeberg, A.; Mallbris, L.; Gislason, G.H.; Skov, L.; Hansen, P.R. Increased risk of migraine in patients with psoriasis: A Danish nationwide cohort study. J. Am. Acad. Dermatol. 2015, 73, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Schurks, M.; Rist, P.M.; Bigal, M.E.; Buring, J.E.; Lipton, R.B.; Kurth, T. Migraine and cardiovascular disease: Systematic review and meta-analysis. BMJ 2009, 339, 3914. [Google Scholar] [CrossRef] [Green Version]
- Risal, A.; Manandhar, K.; Holen, A.; Steiner, T.J.; Linde, M. Comorbidities of psychiatric and headache disorders in Nepal: Implications from a nationwide population-based study. J. Headache Pain 2016, 17, 45. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.C.; Su, N.Y.; Huang, J.Y.; Lee, S.S.; Chang, Y.C. Trends in the prevalence of periodontitis in Taiwan from 1997 to 2013: A nationwide population-based retrospective study. Medicine 2017, 96, 8585. [Google Scholar] [CrossRef]
- Su, N.Y.; Huang, J.Y.; Hu, C.J.; Yu, H.C.; Chang, Y.C. Increased risk of periodontitis in patients with psoriatic disease: A nationwide population-based retrospective cohort study. PeerJ 2017, 5, 4064. [Google Scholar]
- Tong, C.; Wang, Y.H.; Chang, Y.C. Increased risk of carotid atherosclerosis in male patients with chronic periodontitis: A nationwide population-based retrospective cohort study. Int. J. Environ. Res. Public Health 2019, 16, 2635. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.K.; Wang, Y.H.; Chang, Y.C. Chronic periodontitis is associated with the risk of bipolar disorder: A population-based cohort study. Int. J. Environ. Res. Public Health 2020, 17, 3466. [Google Scholar] [CrossRef] [PubMed]
- Ameijeira, P.; Leira, Y.; Domínguez, C.; Leira, R.; Blanco, J. Association between periodontitis and chronic migraine: A case-control study. Odontology 2019, 107, 90–95. [Google Scholar] [CrossRef]
- Leira, Y.; Pozo-Rosich, P.; Torres-Ferrús, M.; Orlandi, M.; Láinez, J.M.; Álvaro, L.C.; Monzón, M.J.; Guerrero, Á.; García-Azorín, D.; Belvís, R.; et al. Self-reported periodontitis and migraine: Results from a multicenter, cross-sectional survey in Spain. Odontology 2019, 107, 530–535. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Administration, Ministry of Health and Welfare, Taiwan. National Health Insurance Annual Report 2014–2015; National Health Insurance Administration, Ministry of Health and Welfare: Taiwan, 2014.
- Yang, L.C.; Suen, Y.J.; Wang, Y.H.; Lin, T.C.; Yu, H.C.; Chang, Y.C. The association of periodontal treatment and decreased pneumonia: A nationwide population-based cohort study. Int. J. Environ. Res. Public Health 2020, 17, 356. [Google Scholar] [CrossRef] [Green Version]
- Tseng, C.F.; Chen, K.H.; Yu, H.C.; Huang, F.M.; Chang, Y.C. Dental amalgam fillings and multiple sclerosis: A nationwide population-based case-control study in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 2637. [Google Scholar] [CrossRef] [Green Version]
- National Health Insurance Research Database. Data Subsets. Available online: https://nhird.nhri.org.tw/en/Data_Subsets.html (accessed on 30 November 2020).
- Stewart, W.; Shechter, A.; Rasmussen, B.K. Migraine prevalence. A review of population-based studies. Neurology 1994, 44, 17–23. [Google Scholar]
- Lipton, R.B.; Bigal, M.E. Migraine: Epidemiology, impact, and risk factors for progression. Headache 2005, 4, 3–13. [Google Scholar] [CrossRef]
- Van Os, H.J.A.; Mulder, I.A.; Broersen, A.; Algra, A.; van der Schaaf, I.C.; Kappelle, L.J.; Velthuis, B.K.; Terwindt, G.M.; Schonewille, W.J.; Visser, M.C.; et al. Migraine and cerebrovascular atherosclerosis in patients with ischemic stroke. Stroke 2017, 48, 1973–1975. [Google Scholar] [CrossRef]
- Rist, P.M.; Tzourio, C.; Kurth, T. Associations between lipid levels and migraine: Cross-sectional analysis in the epidemiology of vascular ageing study. Cephalalgia 2011, 31, 1459–1465. [Google Scholar] [CrossRef] [Green Version]
- Amouroux, R.; Rousseau-Salvador, C. Anxiety and depression in children and adolescents with migraine: A review of the literature. Encephale 2008, 34, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Moldofsky, H. Sleep and pain. Sleep Med. Rev. 2001, 5, 385–396. [Google Scholar] [CrossRef] [Green Version]
- Procaccini, C.; Jirillo, E.; Matarese, G. Leptin as an immunomodulator. Mol. Aspects Med. 2012, 33, 35–45. [Google Scholar] [CrossRef]
- Karthikeyan, B.V.; Pradeep, A.R. Gingival crevicular fluid and serum: Their relationship to periodontal health and disease. J. Clin. Periodontol. 2007, 34, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Rubino, E.; Vacca, A.; Govone, F.; Gai, A.; Boschi, S.; Zucca, M.; De Martino, P.; Gentile, S.; Pinessi, L.; Rainero, I. Investigating the role of adipokines in chronic migraine. Cephalalgia 2017, 37, 1067–1073. [Google Scholar] [CrossRef]
- Leira, Y.; Ameijeira, P.; Domínguez, C.; Leira, R.; Blanco, J. The role of leptin as a biomarker in the relationship between periodontitis and chronic migraine. J. Clin. Periodontol. 2017, 44, 1208–1214. [Google Scholar] [CrossRef]
- Olesen, J.; Burstein, R.; Ashina, M.; Tfelt-Hansen, P. Origin of pain in migraine: Evidence for peripheral sensitisation. Lancet Neurol. 2009, 8, 679–690. [Google Scholar] [CrossRef]
- Markowitz, S.; Saito, K.; Moskowitz, M.A. Neurogenically mediated leakage of plasma protein occurs from blood vessels in dura mater but not brain. J. Neurosci. 1987, 7, 4129–4136. [Google Scholar] [CrossRef] [Green Version]
- Lassen, L.H.; Haderslev, P.A.; Jacobsen, V.B.; Iversen, H.K.; Sperling, B.; Olensen, J. CGRP may play a causative role in migraine. Cephalalgia 2002, 22, 54–61. [Google Scholar] [CrossRef]
- Schneider, H.G.; Lam, Q.T. Procalcitonin for the clinical laboratory: A review. Pathology 2007, 39, 383–390. [Google Scholar] [CrossRef]
- Becker, K.L.; Snider, R.; Nylen, E.S. Procalcitonin assay in systemic inflammation, infection, and sepsis: Clinical utility and limitations. Crit. Care Med. 2008, 36, 941–952. [Google Scholar] [CrossRef]
- Leira, Y.; Ameijeira, P.; Domínguez, C.; Leira, R.; Blanco, J. High serum procalcitonin levels in patients with periodontitis and chronic migraine. J. Periodontol. 2018, 89, 1069–1074. [Google Scholar] [CrossRef]
- Leira, Y.; Ameijeira, P.; Domínguez, C.; López-Arias, E.; Ávila-Gómez, P.; Pérez-Mato, M.; Sobrino, T.; Campos, F.; D’Aiuto, F.; Leira, R.; et al. Periodontal inflammation is related to increased serum calcitonin gene-related peptide levels in patients with chronic migraine. J. Periodontol. 2019, 90, 1088–1095. [Google Scholar] [CrossRef]
- Tietjen, G.E.; Khubchandani, J.; Herial, N.; Palm-Meinders, I.H.; Koppen, H.; Terwindt, G.M.; van Buchem, M.A.; Launer, L.J.; Ferrari, M.D.; Kruit, M.C. Migraine and vascular disease biomarkers: A population-based case-control study. Cephalalgia 2018, 38, 511–518. [Google Scholar] [CrossRef]
- Ceylan, M.; Bayraktutan, O.F.; Becel, S.; Atis, Ö.; Yalcin, A.; Kotan, D. Serum levels of pentraxin-3 and other inflammatory biomarkers in migraine: Association with migraine characteristics. Cephalalgia 2016, 36, 518–525. [Google Scholar] [CrossRef]
- Leira, Y.; Rodríguez-Yáñez, M.; Arias, S.; López-Dequidt, I.; Campos, F.; Sobrino, T.; D’Aiuto, F.; Castillo, J.; Blanco, J. Periodontitis is associated with systemic inflammation and vascular endothelial dysfunction in lacunar infarct patients. J. Periodontol. 2019, 90, 465–474. [Google Scholar] [CrossRef]
- Leira, Y.; Ameijeira, P.; Domínguez, C.; López-Arias, E.; Ávila-Gómez, P.; Pérez-Mato, M.; Sobrino, T.; Campos, F.; D’Aiuto, F.; Leira, R.; et al. Severe periodontitis is linked with increased peripheral levels of sTWEAK and PTX3 in chronic migraineurs. Clin. Oral. Investig. 2020, 24, 597–606. [Google Scholar] [CrossRef]
- Malfertheiner, P. The intriguing relationship of Helicobacter pylori infection and acid secretion in peptic ulcer disease and gastric cancer. Dig. Dis. 2011, 29, 459–464. [Google Scholar] [CrossRef]
- Ozdemir, A.; Mas, M.R.; Sahin, S.; Saglamkaya, U.; Ateskan, U. Detection of Helicobacter pylori colonization in dental plaques and tongue scrapings of patients with chronic gastritis. Quintessence Int. 2001, 32, 131–134. [Google Scholar]
- Wei, X.; Zhao, H.Q.; Ma, C.; Zhang, A.B.; Feng, H.; Zhang, D.; Liu, C. The association between chronic periodontitis and oral Helicobacter pylori: A meta-analysis. PLoS ONE 2019, 14, 225247. [Google Scholar] [CrossRef] [Green Version]
- Ren, Q.; Yan, X.; Zhou, Y.; Li, W.X. Periodontal therapy as adjunctive treatment for gastric Helicobacter pylori infection. Cochrane. Database Syst. Rev. 2016, 2, CD009477. [Google Scholar]
- Su, J.; Zhou, X.Y.; Zhang, G.X. Association between Helicobacter pylori infection and migraine: A meta-analysis. World J. Gastroenterol. 2014, 20, 14965–14972. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Chronic Periodontitis (N = 68,282) | Control (N = 68,282) | ||||
|---|---|---|---|---|---|
| n | % | n | % | p-Value | |
| Age | 0.960 | ||||
| 20–39 | 29,409 | 43.1 | 29,411 | 43.1 | |
| 40–64 | 32,425 | 47.5 | 32,453 | 47.5 | |
| ≥65 | 6448 | 9.4 | 6418 | 9.4 | |
| Mean ± SD | 43.7 ± 14.58 | 43.85 ± 14.42 | 0.051 | ||
| Gender | 0.758 | ||||
| Male | 32,884 | 48.2 | 32,827 | 48.1 | |
| Female | 35,398 | 51.8 | 35,455 | 51.9 | |
| Monthly income | 0.993 | ||||
| <NT$ 20,000 | 29,242 | 42.8 | 29,231 | 42.8 | |
| NT $20,000–40,000 | 21,008 | 30.8 | 21,028 | 30.8 | |
| >NT $40,000 | 18,032 | 26.4 | 18,023 | 26.4 | |
| Urbanization | 0.885 | ||||
| Urban | 46,450 | 68.0 | 46,510 | 68.1 | |
| Suburban | 18,049 | 26.4 | 18,027 | 26.4 | |
| Rural | 3783 | 5.5 | 3745 | 5.5 | |
| Hypertension | 8101 | 11.9 | 8136 | 11.9 | 0.770 |
| Hyperlipidemia | 3982 | 5.8 | 4004 | 5.9 | 0.800 |
| Diabetes | 3657 | 5.4 | 3652 | 5.3 | 0.952 |
| Asthma | 1036 | 1.5 | 1019 | 1.5 | 0.706 |
| Coronary artery disease | 2510 | 3.7 | 2517 | 3.7 | 0.920 |
| Stroke | 1127 | 1.7 | 1133 | 1.7 | 0.899 |
| Alcohol-related disorder | 137 | 0.2 | 124 | 0.2 | 0.421 |
| Anxiety | 1323 | 1.9 | 1303 | 1.9 | 0.694 |
| Depression | 927 | 1.4 | 898 | 1.3 | 0.494 |
| Psoriasis | 139 | 0.2 | 126 | 0.2 | 0.424 |
| Obesity | 106 | 0.2 | 85 | 0.1 | 0.128 |
| Insomnia | 1461 | 2.1 | 1402 | 2.1 | 0.265 |
| No. of Event | Observed Person-Years | ID | Crude HR | 95% CI | p Value | Adjusted HR † | 95% CI | p Value | |
|---|---|---|---|---|---|---|---|---|---|
| Chronic periodontitis | |||||||||
| No | 641 | 587,048 | 1.1 | 1 | 1 | ||||
| Yes | 785 | 593,115 | 1.3 | 1.21 | 1.09–1.35 | <0.001 | 1.21 | 1.09–1.34 | <0.001 |
| Age | |||||||||
| 20–39 | 647 | 522,177 | 1.2 | 1 | 1 | ||||
| 40–64 | 701 | 552,912 | 1.3 | 1.02 | 0.92–1.14 | 0.661 | 0.98 | 0.88–1.1 | 0.776 |
| ≥65 | 78 | 105,074 | 0.7 | 0.60 | 0.47–0.76 | <0.001 | 0.52 | 0.4–0.67 | <0.001 |
| Gender | |||||||||
| Male | 364 | 567,014 | 0.6 | 1 | 1 | ||||
| Female | 1062 | 613,149 | 1.7 | 2.70 | 2.4–3.04 | <0.001 | 2.69 | 2.38–3.04 | <0.001 |
| Monthly income | |||||||||
| <TWD 20,000 | 603 | 507,213 | 1.2 | 1 | 1 | ||||
| TWD 20,000–40,000 | 480 | 359,766 | 1.3 | 1.12 | 1–1.27 | 0.058 | 1.12 | 0.99–1.26 | 0.073 |
| >TWD 40,000 | 343 | 313,184 | 1.1 | 0.92 | 0.81–1.05 | 0.226 | 1.08 | 0.94–1.24 | 0.279 |
| Urbanization | |||||||||
| Urban | 943 | 802,066 | 1.2 | 1 | 1 | ||||
| Suburban | 398 | 313,350 | 1.3 | 1.08 | 0.96–1.21 | 0.197 | 1.10 | 0.97–1.23 | 0.128 |
| Rural | 85 | 64,747 | 1.3 | 1.12 | 0.89–1.39 | 0.330 | 1.13 | 0.9–1.41 | 0.290 |
| Hypertension | 151 | 129,261 | 1.2 | 0.97 | 0.82–1.14 | 0.683 | 0.91 | 0.74–1.11 | 0.358 |
| Hyperlipidemia | 101 | 60,017 | 1.7 | 1.43 | 1.17–1.75 | 0.001 | 1.57 | 1.25–1.97 | <0.001 |
| Diabetes | 64 | 57,293 | 1.1 | 0.92 | 0.72–1.19 | 0.535 | 0.84 | 0.64–1.1 | 0.213 |
| Asthma | 26 | 17,449 | 1.5 | 1.24 | 0.84–1.82 | 0.281 | 1.19 | 0.8–1.76 | 0.385 |
| Coronary artery disease | 54 | 41,251 | 1.3 | 1.09 | 0.83–1.43 | 0.542 | 1.16 | 0.86–1.55 | 0.331 |
| Stroke | 38 | 17,652 | 2.2 | 1.81 | 1.31–2.5 | <0.001 | 2.16 | 1.54–3.04 | <0.001 |
| Alcohol-related disorder | 4 | 1993 | 2.0 | 1.67 | 0.63–4.45 | 0.306 | 2.13 | 0.79–5.7 | 0.133 |
| Anxiety | 56 | 20,483 | 2.7 | 2.32 | 1.78–3.03 | <0.001 | 1.75 | 1.32–2.33 | <0.001 |
| Depression | 35 | 14,555 | 2.4 | 2.02 | 1.44–2.83 | <0.001 | 1.41 | 1–1.99 | 0.053 |
| Psoriasis | 5 | 2190 | 2.3 | 1.89 | 0.79–4.55 | 0.154 | 2.11 | 0.88–5.08 | 0.096 |
| Obesity | 1 | 1540 | 0.6 | 0.54 | 0.08–3.82 | 0.535 | 0.46 | 0.06–3.27 | 0.437 |
| Insomnia | 66 | 22,490 | 2.9 | 2.51 | 1.96–3.21 | <0.001 | 2.12 | 1.64–2.75 | <0.001 |
| Chronic Periodontitis (N = 68,282) | Control (N = 68,282) | p-Value | |
|---|---|---|---|
| Follow-up duration (years) | 8.69 ± 3.08 | 8.6 ± 3.1 | <0.001 |
| Time to migraine (years), N = 1426 | 5.05 ± 3.15 | 4.87 ± 3.23 | 0.280 |
| Heading | Chronic Periodontitis | Control | HR | 95% CI | p Value | ||
|---|---|---|---|---|---|---|---|
| N | No. of Event | N | No. of Event | ||||
| Age | |||||||
| 20–39 | 29,409 | 340 | 29,411 | 307 | 1.10 | 0.94–1.28 | 0.234 |
| 40–64 | 32,425 | 401 | 32,453 | 300 | 1.33 | 1.144–1.54 | <0.001 |
| ≥65 | 6448 | 44 | 6418 | 34 | 1.24 | 0.79–1.94 | 0.342 |
| Gender | |||||||
| Male | 32,884 | 219 | 32,827 | 145 | 1.50 | 1.21–1.85 | <0.001 |
| Female | 35,398 | 566 | 35,455 | 496 | 1.13 | 0.999–1.27 | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-K.; Yang, L.-C.; Wang, Y.-H.; Chang, Y.-C. Increased Risk of Migraine in Patients with Chronic Periodontitis: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 1921. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041921
Huang Y-K, Yang L-C, Wang Y-H, Chang Y-C. Increased Risk of Migraine in Patients with Chronic Periodontitis: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(4):1921. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041921
Chicago/Turabian StyleHuang, Yung-Kai, Li-Chiu Yang, Yu-Hsun Wang, and Yu-Chao Chang. 2021. "Increased Risk of Migraine in Patients with Chronic Periodontitis: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 18, no. 4: 1921. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041921