
Risk of Postoperative Bleeding in Tonsillectomy for Peritonsillar Abscess, as Opposed to in Recurrent and Chronic Tonsillitis—A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
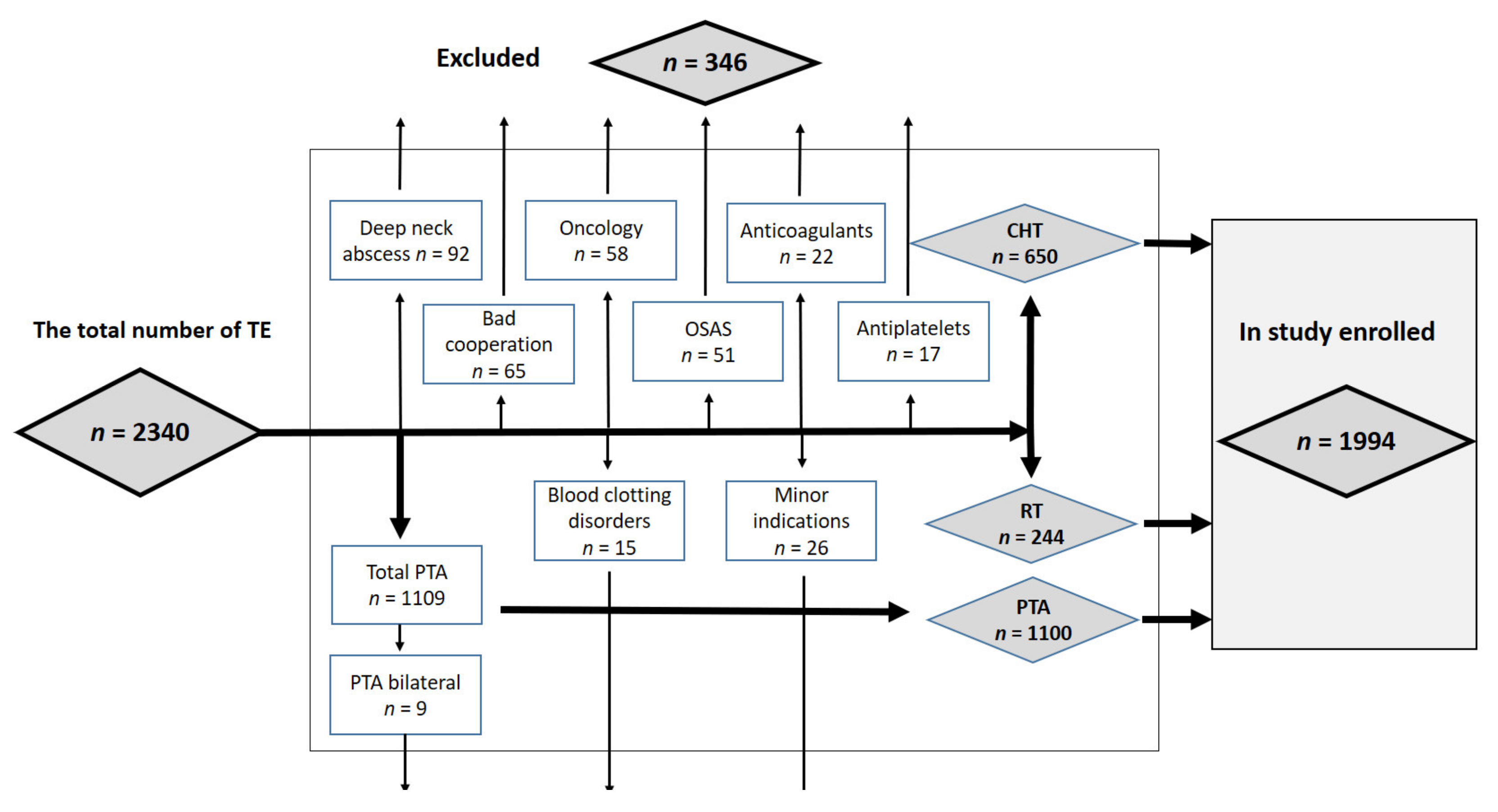
2.1. Group of Patients
2.2. Methods
2.3. Methodology of Stopping Bleeding
2.4. Statistical Methods
3. Results
4. Discussion
4.1. Differences in the Course of PTA and CHT + RT
4.2. Postoperative Bleeding
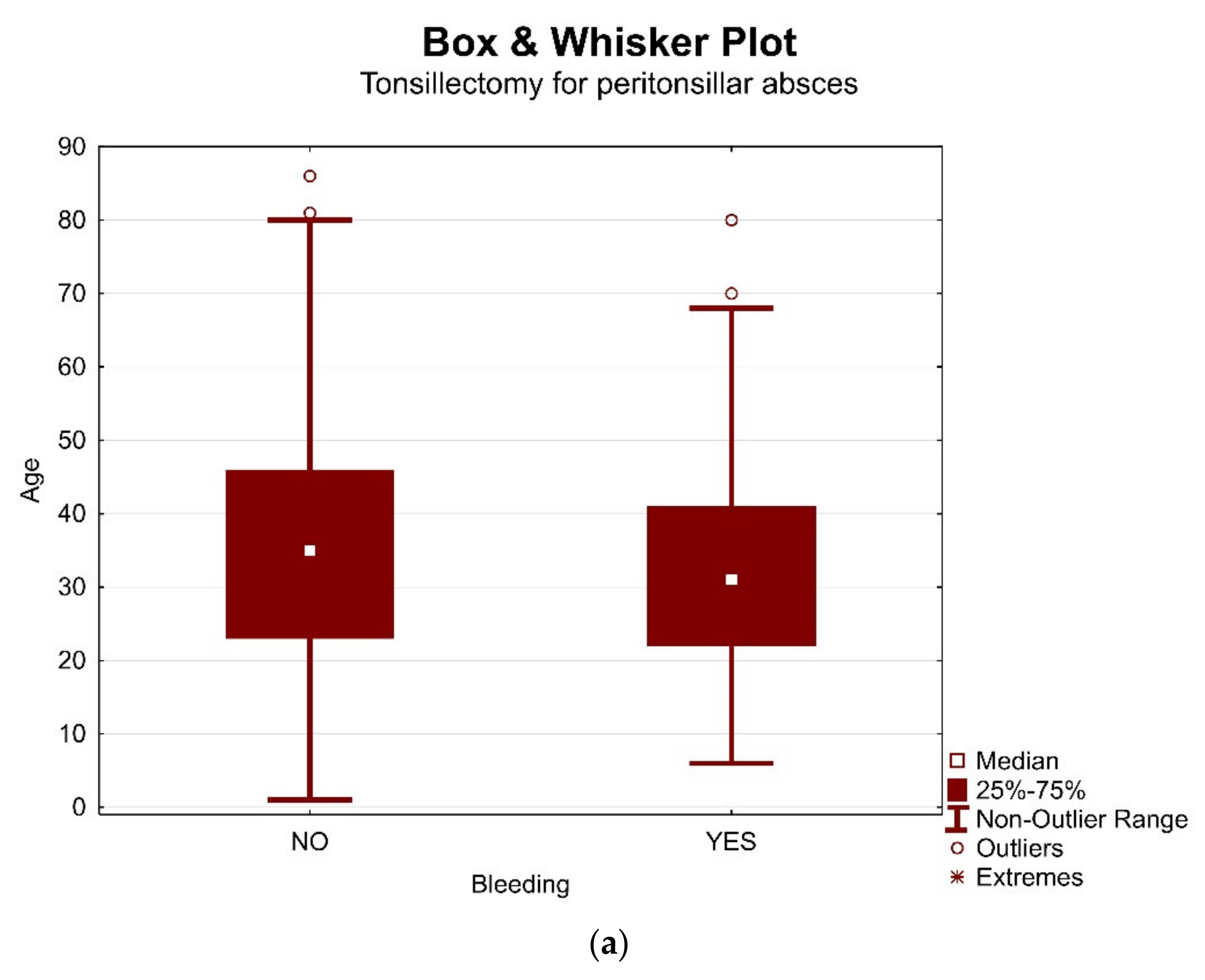
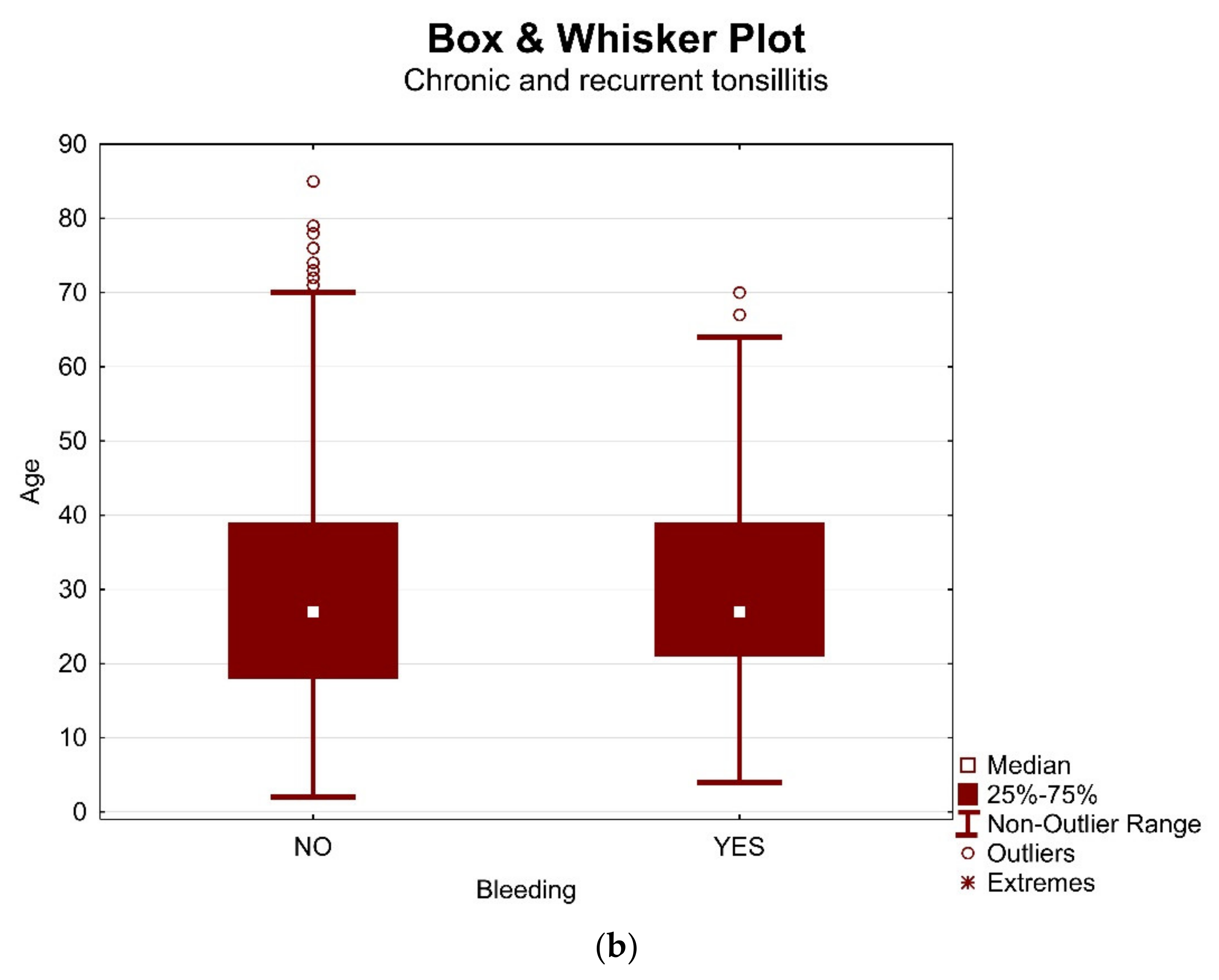
4.3. Age, Gender, Season and Side Dependence
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Darrow, D.H.; Siemens, C. Indications for tonsillectomy and adenoidectomy. Laryngoscope 2002, 112, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.H.; Straight, C.E.; Lehman, E.B.; Tanner, M.; Carr, M.M. Indications for tonsillectomy: A 10 year retrospective review. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 2151–2155. [Google Scholar] [CrossRef]
- Galindo Torres, B.P.; De Miguel García, F.; Whyte Orozco, J. Tonsillectomy in adults: Analysis of indications and complications. Auris Nasus Larynx 2018, 45, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Seshamani, M.; Vogtmann, E.; Gatwood, J.; Gibson, T.B.; Scanlon, D. Prevalence of complications from adult tonsillectomy and impact on health care expenditures. Otolaryngol. Head Neck Surg. 2014, 150, 574–581. [Google Scholar] [CrossRef]
- Ford, L.C.; Cruz, R.M. Bilateral glossopharyngeal nerve paralysis after tonsillectomy: Case report and anatomic study. Laryngoscope 2004, 114, 2196–2199. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.E.; Brewster, D.F.; Bernstein, P.E. Subcutaneous emphysema and pneumomediastinum complicating tonsillectomy. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 1324–1327. [Google Scholar] [CrossRef] [PubMed]
- Francis, D.O.; Fonnesbeck, C.; Sathe, N.; McPheeters, M.; Chinnadurai, S. Postoperative bleeding and associated utilization following tonsillectomy in children: A systematic review and meta-analysis. Otolaryngol. Head Neck Surg. 2017, 156, 442–455. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.K.; Lee, J.W.; Kim, M.G.; Ha, S.Y.; Lee, J.S.; Yeo, S.G. Analysis of prognostic factors for postoperative bleeding after tonsillectomy. Eur. Arch. Oto-Rhino-Laryngol. 2012, 269, 977–981. [Google Scholar] [CrossRef]
- Mitchell, R.B.; Archer, S.M.; Ishman, S.L.; Rosenfeld, R.M.; Coles, S.; Finestone, S.A.; Friedman, N.R.; Giordano, T.; Hildrew, D.M.; Kim, T.W.; et al. Clinical Practice Guideline: Tonsillectomy in Children (Update). Otolaryngol. Head Neck Surg. 2019, 160, 1–42. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Walsh, J.; Tunkel, D.E.; Boss, E.F.; Ryan, M.; Lee, A.H. Frequency of post-tonsillectomy hemorrhage relative to time of day. Laryngoscope 2020, 130, 1823–1827. [Google Scholar] [CrossRef]
- Attner, P.; Haraldsson, P.O.; Hemlin, C.; Hessén Söderman, A.C. A 4-year consecutive study of post-tonsillectomy haemorrhage. ORL 2009, 71, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Bitar, M.; Dunya, G.; Khalifee, E.; Muwakkit, S.; Barazi, R. Risk of post-operative hemorrhage after adenoidectomy and tonsillectomy: Value of the preoperative determination of partial thromboplastin time and prothrombin time. Int. J. Pediatr. Oto-Rhino-Laryngol. 2019, 116, 62–64. [Google Scholar] [CrossRef]
- Pribuišiene, R.; Šarauskas, V.; Kuzminiene, A.; Uloza, V. Correlation between throat-related symptoms and histological examination in adults with chronic tonsillitis. Medicina 2015, 51, 286–290. [Google Scholar] [CrossRef]
- Hoddeson, E.K.; Gourin, C.G. Adult tonsillectomy: Current indications and outcomes. Otolaryngol. Head Neck Surg. 2009, 140, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Kanesada, K.; Mogi, G. Bilateral Peritonsillar Abscesses. Auris Nasus Larynx 1981, 8, 35–39. [Google Scholar] [CrossRef]
- Papacharalampous, G.X.; Vlastarakos, P.V.; Kotsis, G.; Davilis, D.; Manolopoulos, L. Bilateral peritonsillar abscesses: A case presentation and review of the current literature with regard to the controversies in diagnosis and treatment. Case Rep. Med. 2011, 2011. [Google Scholar] [CrossRef]
- Slouka, D.; Hanakova, J.; Kostlivy, T.; Skopek, P.; Kubec, V.; Babuska, V. Epidemiological and Microbiological Aspects of the Peritonsillar Abscess. Int. J. Environ. Res. Public Health 2020, 17, 4020. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.H.; Anderson, K.E.; Willging, J.P.; Myer, C.M.; Shott, S.R.; Bratcher, G.O.; Cotton, R.T. Posttonsillectomy hemorrhage: What is it and what should be recorded? Arch. Otolaryngol. Head Neck Surg. 2001, 127, 1271–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, C.M.; Schubart, J.R.; Carr, M.M. Trends in the management of secondary post-tonsillectomy hemorrhage in children. Int. J. Pediatr. Otorhinolaryngol. 2018, 108, 196–201. [Google Scholar] [CrossRef]
- Komínek, P.; Chrobok, V.; Pellant, A.; Kraus, J.; Černý, V.; Betka, J. Bleeding after tonsillectomy—A review (epidemiology, risk factors, life threatening bleeding). Otorinolaryngol. Foniatr. 2014, 63, 41–49. [Google Scholar]
- Sowerby, L.J.; Hussain, Z.; Husein, M. The epidemiology, antibiotic resistance and post-discharge course of peritonsillar abscesses in London, Ontario. J. Otolaryngol. Head Neck Surg. 2013, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wikstén, J.; Blomgren, K.; Eriksson, T.; Guldfred, L.; Bratt, M.; Pitkäranta, A. Variations in treatment of peritonsillar abscess in four Nordic countries. Acta Otolaryngol. 2014, 134, 813–817. [Google Scholar] [CrossRef] [PubMed]
- Acharya, A.; Gurung, R.; Khanal, B.; Ghimire, A. Bacteriology and antibiotic Susceptibility pattern of peritonsillar abscess. J. Nepal Med. Assoc. 2010, 49, 139–142. [Google Scholar] [CrossRef]
- Albertz, N.; Nazar, G. Peritonsillar abscess: Treatment with immediate tonsillectomy—10 years of experience. Acta Otolaryngol. 2012, 132, 1102–1107. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, D. Retropharyngeal abscess: A clinical review. J. Laryngol. Otol. 1997, 111, 546–550. [Google Scholar] [CrossRef]
- Snow, N.; Lucas, A.E.; Grau, M.; Steiner, M. Purulent Mediastinal Abscess Secondary to Ludwig’s Angina. Arch. Otolaryngol. 1983, 109, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Parhiscar, A.; Har-El, G.H. El Deep neck abscess: A retrospective review of 210 cases. Ann. Otol. Rhinol. Laryngol. 2001, 110, 1051–1054. [Google Scholar] [CrossRef] [PubMed]
- Plank, L. Tonsillitis, Chronic. In Head and Neck Pathology. Encyclopedia of Pathology, 1st ed.; Volavsek, M., Ed.; Springer: Cham, Switzerland, 2016; pp. 497–501. [Google Scholar]
- Georgalas, C.C.; Tolley, N.S.; Narula, A. Tonsillitis. BMJ Clin. Evid. 2009, 2009, 0503. [Google Scholar]
- Uijen, J.H.; Bindels, P.J.; Schellevis, F.G.; Van Der Wouden, J.C. ENT problems in Dutch children: Trends in incidence rates, antibiotic prescribing and referrals 2002–2008. Scand. J. Prim. Health Care 2011, 29, 75–79. [Google Scholar] [CrossRef] [Green Version]
- Kvestad, E.; Kværner, K.J.; Røysamb, E.; Tambs, K.; Harris, J.R.; Magnus, P. Heritability of recurrent tonsillitis. Arch. Otolaryngol. Head Neck Surg. 2005, 131, 383–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baik, G.; Brietzke, S.E. Comparison of Pediatric Intracapsular Tonsillectomy and Extracapsular Tonsillectomy: A Cost and Utility Decision Analysis. Otolaryngol. Head Neck Surg. 2018, 158, 1113–1118. [Google Scholar] [CrossRef]
- Cohen, M.S.; Getz, A.E.; Isaacson, G.; Gaughan, J.; Szeremeta, W. Intracapsular vs. extracapsular tonsillectomy: A comparison of pain. Laryngoscope 2007, 117, 1855–1858. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Honda, N.; Saito, H. Advantage and disadvantage of KTP-532 laser tonsillectomy compared with conventional method. Auris Nasus Larynx 1999, 26, 447–452. [Google Scholar] [CrossRef]
- Slouka, D.; Polenik, P.; Hes, O.; Smid, D.; Slama, K.; Hosek, P.; Boudova, L. Can we improve clinical results of tonsillectomy using lasers? J. Appl. Biomed. 2016, 14, 35–40. [Google Scholar] [CrossRef]
- Lachanas, V.A.; Hajiioannou, J.K.; Karatzias, G.T.; Filios, D.; Koutsias, S.; Mourgelas, C. Comparison of LigaSure vessel sealing system, harmonic scalpel, and cold knife tonsillectomy. Otolaryngol. Head Neck Surg. 2007, 137, 385–389. [Google Scholar] [CrossRef]
- Toft, J.G.; Guldfred, L.-A.; Holmgaard Larsen, B.I.; Becker, B.C. Novel tonsillectomy technique. Ugeskr. Laeger 2009, 171, 45–49. [Google Scholar]
- Aksoy, F.; Ozturan, O.; Veyseller, B.; Yildirim, Y.S.; Demirhan, H. Comparison of radiofrequency and monopolar electrocautery tonsillectomy. J. Laryngol. Otol. 2010, 124, 180–184. [Google Scholar] [CrossRef]
- Bergler, W.; Huber, K.; Hammerschmitt, N.; Hörmann, K. Tonsillectomy with argon plasma coagulation (APC): Evaluation of pain and hemorrhage. Laryngoscope 2001, 111, 1423–1429. [Google Scholar] [CrossRef]
- Belloso, A.; Chidambaram, A.; Morar, P.; Timms, M.S. Coblation Tonsillectomy Versus Dissection Tonsillectomy: Postoperative Hemorrhage. Laryngoscope 2003, 113, 2010–2013. [Google Scholar] [CrossRef] [PubMed]
- Blum, D.J.; Neel, H.B. Current thinking on tonsillectomy and adenoidectomy. Compr. Ther. 1983, 9, 48–56. [Google Scholar]
- Jäckel, M.C.; Petzold, S.; Dimmer, V.; Mall, G.; Reck, R. Die mikrochirurgische tonsillektomie mit dem C02-laser: Eine analyse klinischer und morphologischer daten. HNO 2003, 51, 634–639. [Google Scholar] [CrossRef]
- Walker, R.A.; Syed, Z.A. Harmonic scalpel tonsillectomy versus electrocautery tonsillectomy: A comparative pilot study. Otolaryngol. Head Neck Surg. 2001, 125, 449–455. [Google Scholar] [CrossRef]
- Krishna, P.; LaPage, M.J.; Hughes, L.F.; Lin, S.Y. Current practice patterns in tonsillectomy and perioperative care. Int. J. Pediatr. Otorhinolaryngol. 2004, 68, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Baker, K. An overview of current techniques for tonsillectomy. ORL Head Neck Nurs. 2006, 24, 8–12. [Google Scholar]
- Fryckova, A.; Machalova, M.; Slapak, I. Bleeding after Tonsillectomy and Tonsillotomy in Children. Otorinolaryngol. Foniatr. 2012, 63, 29–33. [Google Scholar]
- Hopkins, C.; Geyer, M.; Topham, J. Post-tonsillectomy haemorrhage: A 7-year retrospective study. Eur. Arch. Oto-Rhino-Laryngol. 2003, 260, 454–455. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, S.; Tveterås, K. Post-tonsillectomy haemorrhage. A retrospective study of 1150 operations. Clin. Otolaryngol. Allied Sci. 1984, 9, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Myssiorek, D.; Alvi, A. Post-tonsillectomy hemorrhage: An assessment of risk factors. Int. J. Pediatr. Otorhinolaryngol. 1996, 37, 35–43. [Google Scholar] [CrossRef]
- Ikoma, R.; Sakane, S.; Niwa, K. Risk factors for post-tonsillectomy hemorrhage. Auris Nasus Larynx. 2014, 4, 376–379. [Google Scholar] [CrossRef]
- Giger, R.; Landis, B.N.; Dulguerov, P. Hemorrhage after quinsy tonsillectomy. Otolaryngol. Head Neck Surg. 2005, 5, 729–734. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Total | Gender | Age | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patients | % | Men | % | Women | % | p-Value M/W | Mean | Median | p-Value | |
| I (PTA) | 1100 | 55.17 | 642 | 58.36 | 458 | 41.64 | <0.0001 | 35.41 | 35 | <0.0001 |
| II (CHT + RT) | 894 | 44.83 | 372 | 41.61 | 522 | 58.39 | 29.54 | 27 | ||
| total | 1994 | 100 | 1014 | 50.85 | 980 | 49.15 | - | 31.81 | 30 | - |
| Diagnosis | Tonsillectomy | Side of Tonsillectomy | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | % | Bilateral | % | Unilateral | % | Left | % | Right | % | p-Value | |
| I (PTA) | 1100 | 38.71 | 0 | 0 | 1100 | 100 | 554 | 50.36 | 546 | 49.64 | 0.9920 |
| II (CHT + RT) | 1742 | 61.29 | 848 | 97.36 | 46 | 2.64 | 877 | 50.34 | 865 | 49.66 | |
| total | 2842 | 100 | 848 | 59.68 | 1146 | 40.32 | 1431 | 50.35 | 1411 | 49.65 | - |
| n | PTH | % | p-Value | Men | Women | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | PTH | % | Total | PTH | % | ||||||
| I (PTA) | 1100 | 107 | 9.73 | 0.9920 | 642 | 68 | 10.59 | 458 | 39 | 8.52 | 0.2519 |
| II (CHT + RT) | 1742 | 178 | 10.22 | 729 | 90 | 12.35 | 1013 | 88 | 8.69 | 0.0129 | |
| total | 2842 | 285 | 10.03 | - | 1371 | 158 | 11.52 | 1471 | 127 | 8.63 | 0.0104 |
| n | PTH | Right | % | Left | % | p-Value | |
|---|---|---|---|---|---|---|---|
| I (PTA) | 1100 | 107 | 56 | 10.26 | 51 | 9.21 | 0.5566 |
| II (CHT + RT) | 1742 | 178 | 93 | 10.75 | 85 | 9.69 | 0.4655 |
| total | 2842 | 285 | 149 | 52.28 | 136 | 47.72 | 0.3487 |
| Diagnosis | Finding of Bleeding | Degree of Bleeding and Therapy | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anamnestic or Insignificant | Significant | Observation and Hemostyptics | Compression and/or Coagulation - Local Anesthesia | Compression and/or Coagulation - General Anesthesia | ||||||||
| n | % | n | % | p-Value | n | % | n | % | n | % | p-Value | |
| I (PTA) | 20 | 18.69 | 87 | 81.31 | 0.7524 | 76 | 71.03 | 7 | 6.54 | 24 | 22.43 | 0.3045 |
| II (CHT + RT) | 36 | 20.22 | 142 | 79.78 | 129 | 72.47 | 5 | 2.81 | 44 | 24.72 | ||
| total | 56 | 19.65 | 229 | 80.35 | - | 205 | 71.93 | 12 | 4.21 | 68 | 23.86 | - |
| 1. PTH | 2. PTH | 3. PTH | |||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | p-Value | |
| I (PTA) | 107 | 9.73 | 11 | 11.28 | 1 | 0.93 | 0.5774 |
| II (CHT + RT) | 178 | 10.22 | 21 | 11.80 | 2 | 1.12 | |
| total | 285 | 10.03 | 32 | 11.23 | 3 | 1.05 | - |
| Group I (PTA) | Group II (CHT + RT) | |||||||
|---|---|---|---|---|---|---|---|---|
| Age | Total | PTH | % | p-Value | Total | PTH | % | p-Value |
| 0–4 | 12 | 0 | 0 | 0.6195 | 14 | 1 | 7.14 | 1.0000 |
| 5–9 | 43 | 3 | 6.98 | 0.7919 | 133 | 8 | 6.02 | 0.0959 |
| 10–14 | 47 | 4 | 8.51 | 1.0000 | 112 | 8 | 7.14 | 0.2666 |
| 15–19 | 90 | 8 | 8.89 | 0.7794 | 237 | 19 | 8.02 | 0.2287 |
| 20–24 | 115 | 18 | 15.65 | 0.0235 | 247 | 27 | 10.93 | 0.6896 |
| 25–29 | 105 | 12 | 11.43 | 0.5362 | 237 | 35 | 14.77 | 0.0128 |
| 30–34 | 137 | 17 | 12.41 | 0.2576 | 164 | 17 | 10.37 | 0.9477 |
| 35–39 | 154 | 13 | 8.44 | 0.5615 | 196 | 21 | 10.71 | 0.8077 |
| 40–44 | 98 | 9 | 9.18 | 0.8491 | 135 | 17 | 12.89 | 0.3430 |
| 45–49 | 70 | 6 | 8.57 | 0.7359 | 72 | 13 | 18.06 | 0.0249 |
| 50–54 | 74 | 8 | 10.81 | 0.7447 | 56 | 3 | 5.36 | 0.2222 |
| 55–59 | 53 | 3 | 5.66 | 0.3058 | 40 | 3 | 7.50 | 0.5658 |
| 60–64 | 41 | 2 | 4.88 | 0.4208 | 41 | 3 | 7.32 | 0.7931 |
| 65–69 | 30 | 2 | 6.67 | 0.7609 | 32 | 2 | 6.25 | 0.7657 |
| 70–74 | 17 | 1 | 5.88 | 1.0000 | 14 | 1 | 7.14 | 1.0000 |
| 75–79 | 10 | 0 | 0 | 0.6109 | 10 | 0 | 0 | 0.6116 |
| 80–84 | 3 | 1 | 33.33 | 0.2646 | 0 | 0 | 0 | - |
| 85–89 | 1 | 0 | 0 | 1.0000 | 2 | 0 | 0 | 1.0000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slouka, D.; Čejková, Š.; Hanáková, J.; Hrabačka, P.; Kormunda, S.; Kalfeřt, D.; Skálová, A.; Šimánek, V.; Kucera, R. Risk of Postoperative Bleeding in Tonsillectomy for Peritonsillar Abscess, as Opposed to in Recurrent and Chronic Tonsillitis—A Retrospective Study. Int. J. Environ. Res. Public Health 2021, 18, 1946. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041946
Slouka D, Čejková Š, Hanáková J, Hrabačka P, Kormunda S, Kalfeřt D, Skálová A, Šimánek V, Kucera R. Risk of Postoperative Bleeding in Tonsillectomy for Peritonsillar Abscess, as Opposed to in Recurrent and Chronic Tonsillitis—A Retrospective Study. International Journal of Environmental Research and Public Health. 2021; 18(4):1946. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041946
Chicago/Turabian StyleSlouka, David, Štěpánka Čejková, Jana Hanáková, Petr Hrabačka, Stanislav Kormunda, David Kalfeřt, Alena Skálová, Václav Šimánek, and Radek Kucera. 2021. "Risk of Postoperative Bleeding in Tonsillectomy for Peritonsillar Abscess, as Opposed to in Recurrent and Chronic Tonsillitis—A Retrospective Study" International Journal of Environmental Research and Public Health 18, no. 4: 1946. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041946