
Malaria in Cambodia: A Retrospective Analysis of a Changing Epidemiology 2006–2019



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.1.1. Malaria Data
2.1.2. Population Data and Maps
2.1.3. Untoward Events
2.2. Inclusion Criteria and Setting
2.3. Case Definition
- −
- had fever, chills, or sweats or two of the following: headache, nausea, vomiting, diarrhea, AND
- −
- any of the following: traveled to the forest in the previous month, had confirmed malaria in the past 28 days, traveled to a malaria-endemic area from a non-endemic area, or lived or worked around others with a recently confirmed malaria diagnosis [47].
2.4. Data Analysis
3. Results
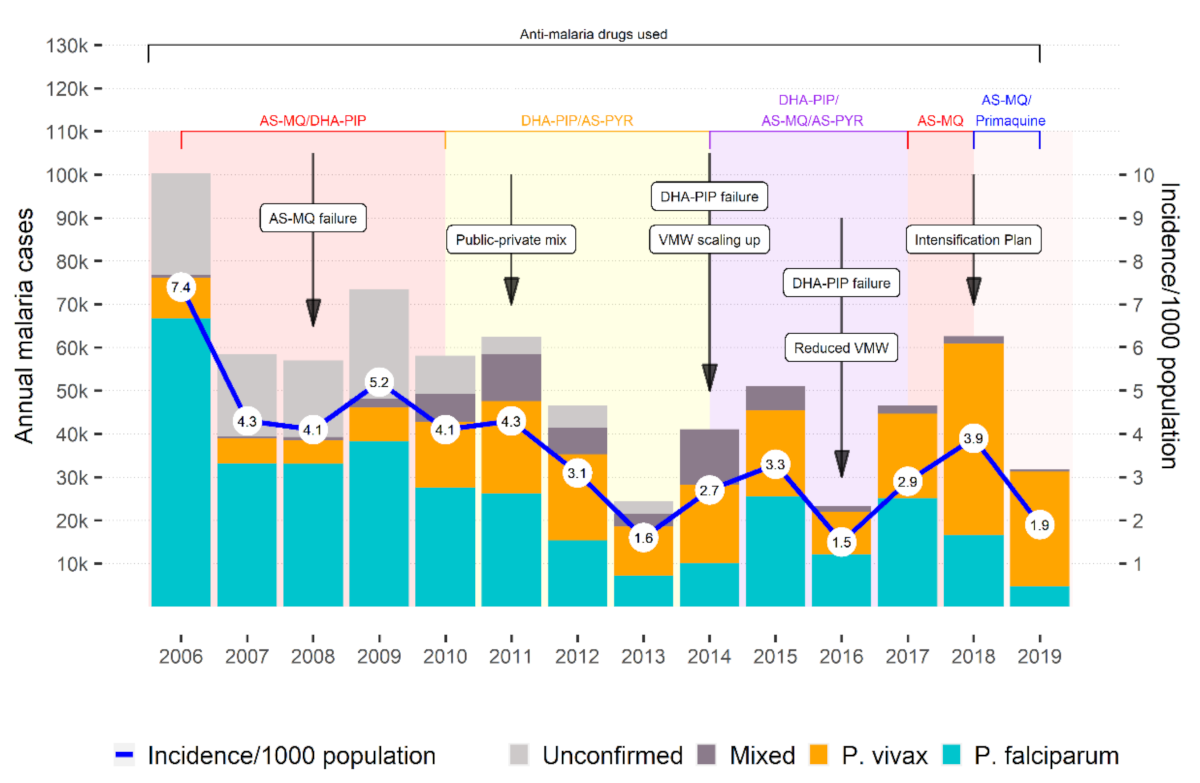
3.1. Overall Malaria Cases and Incidence Rate
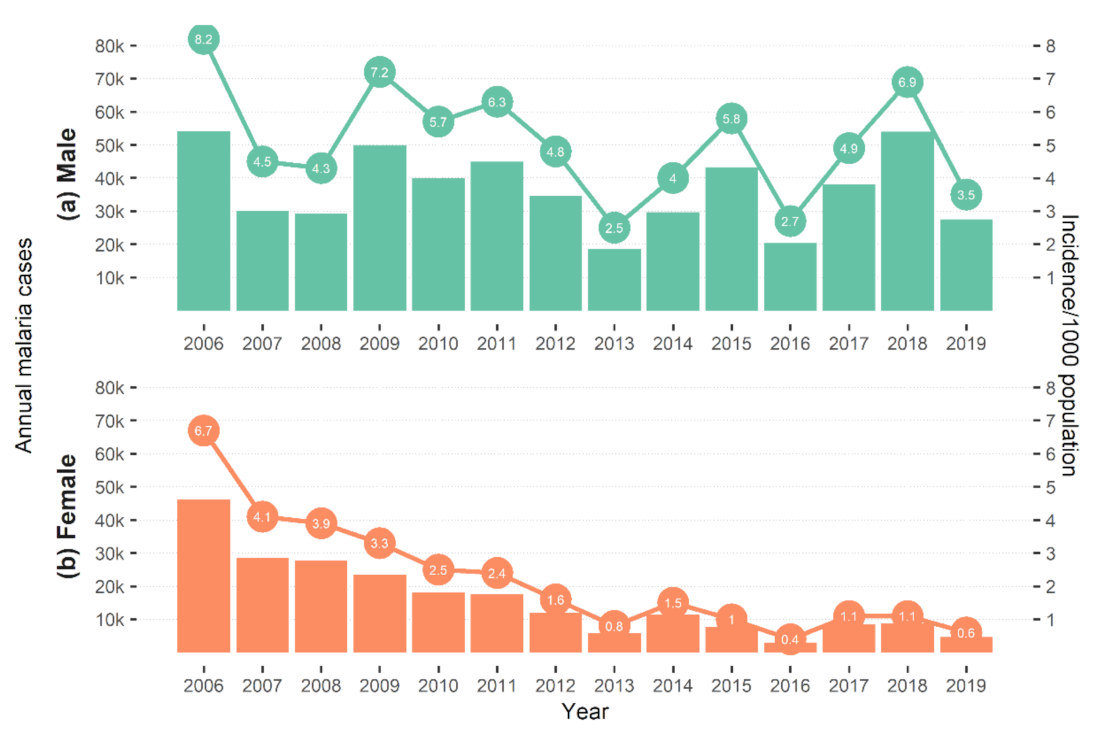
3.2. Incidence by Sex
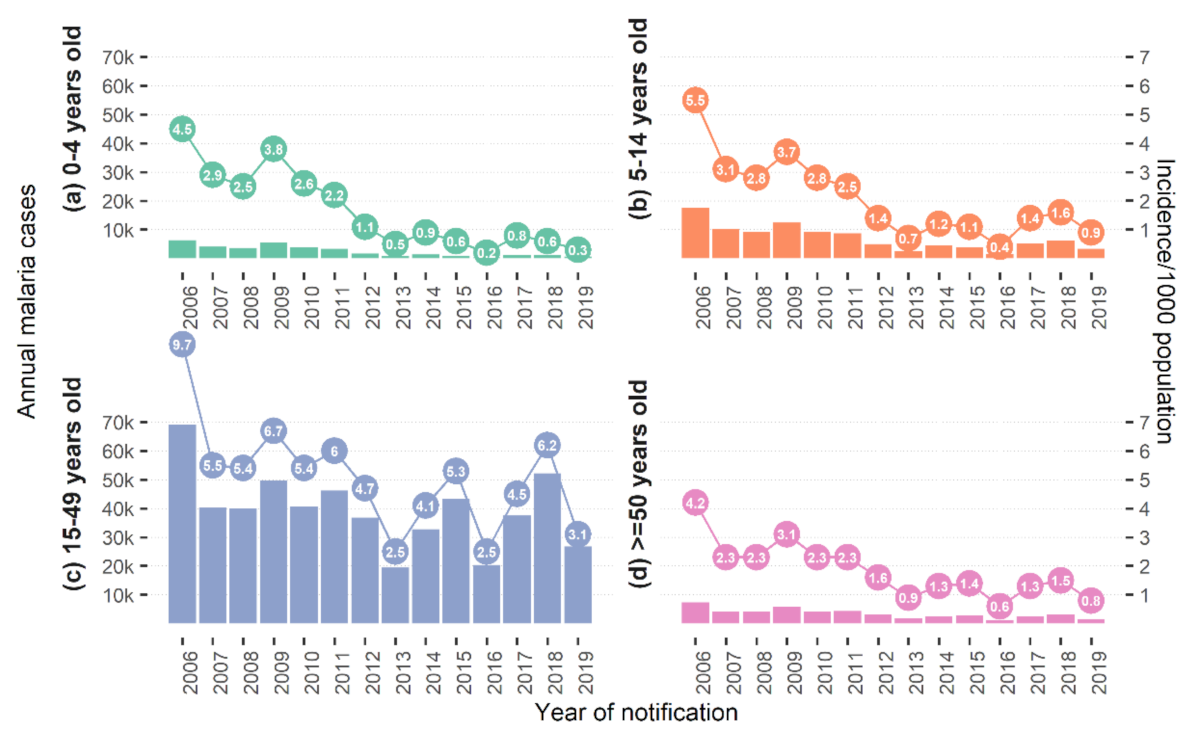
3.3. Incidence by Age Group
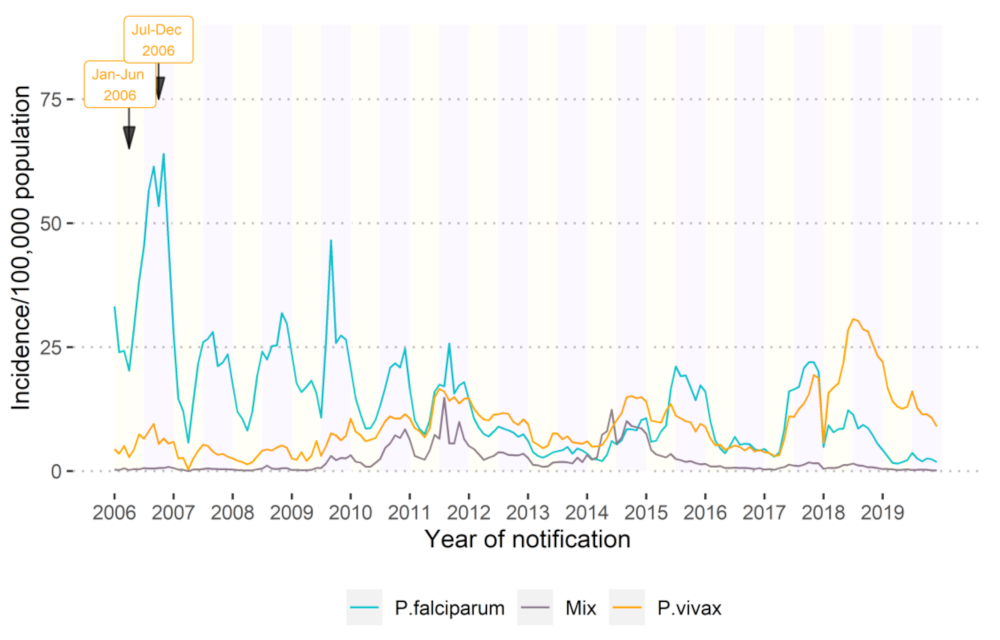
3.4. Seasonality
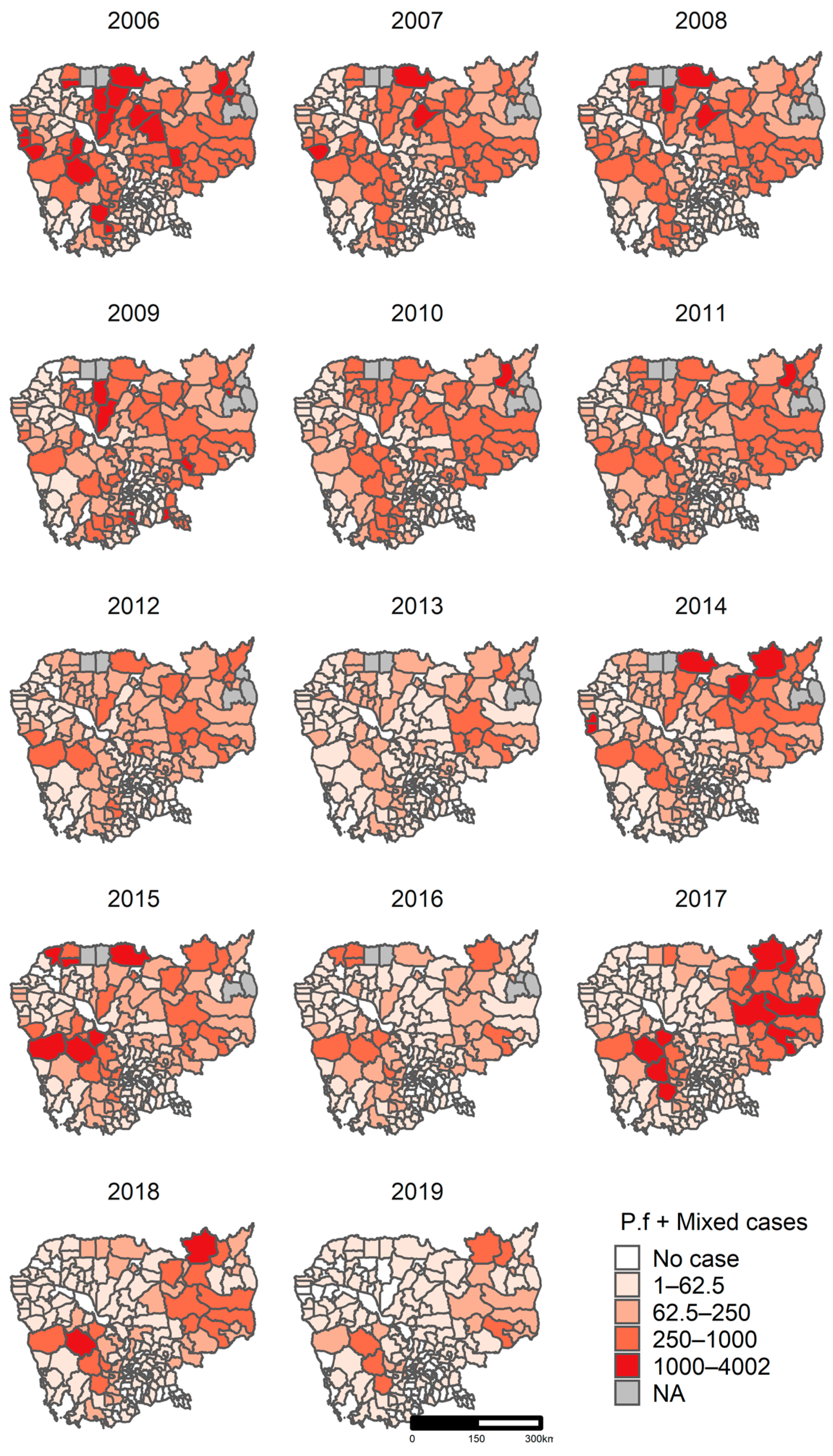
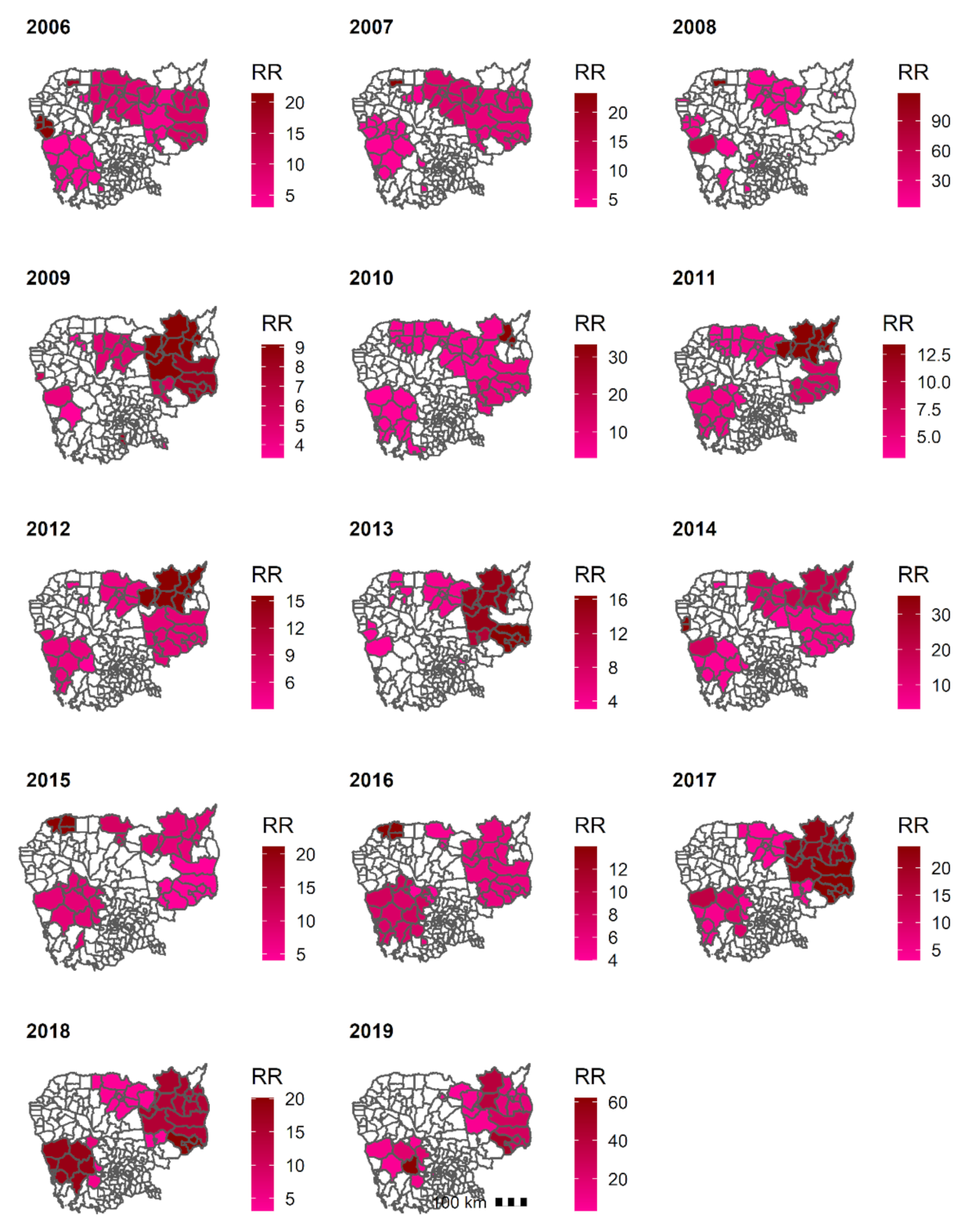
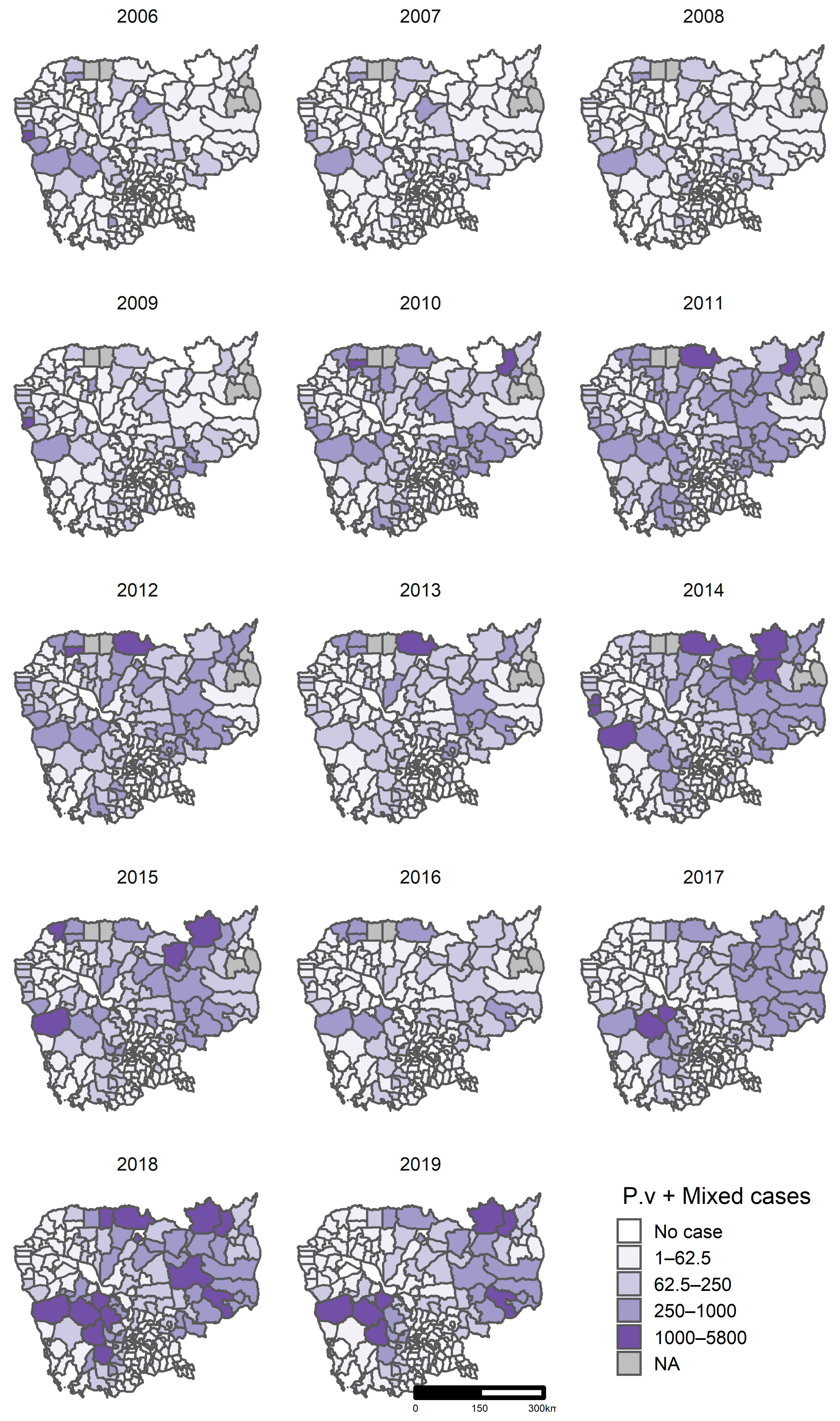
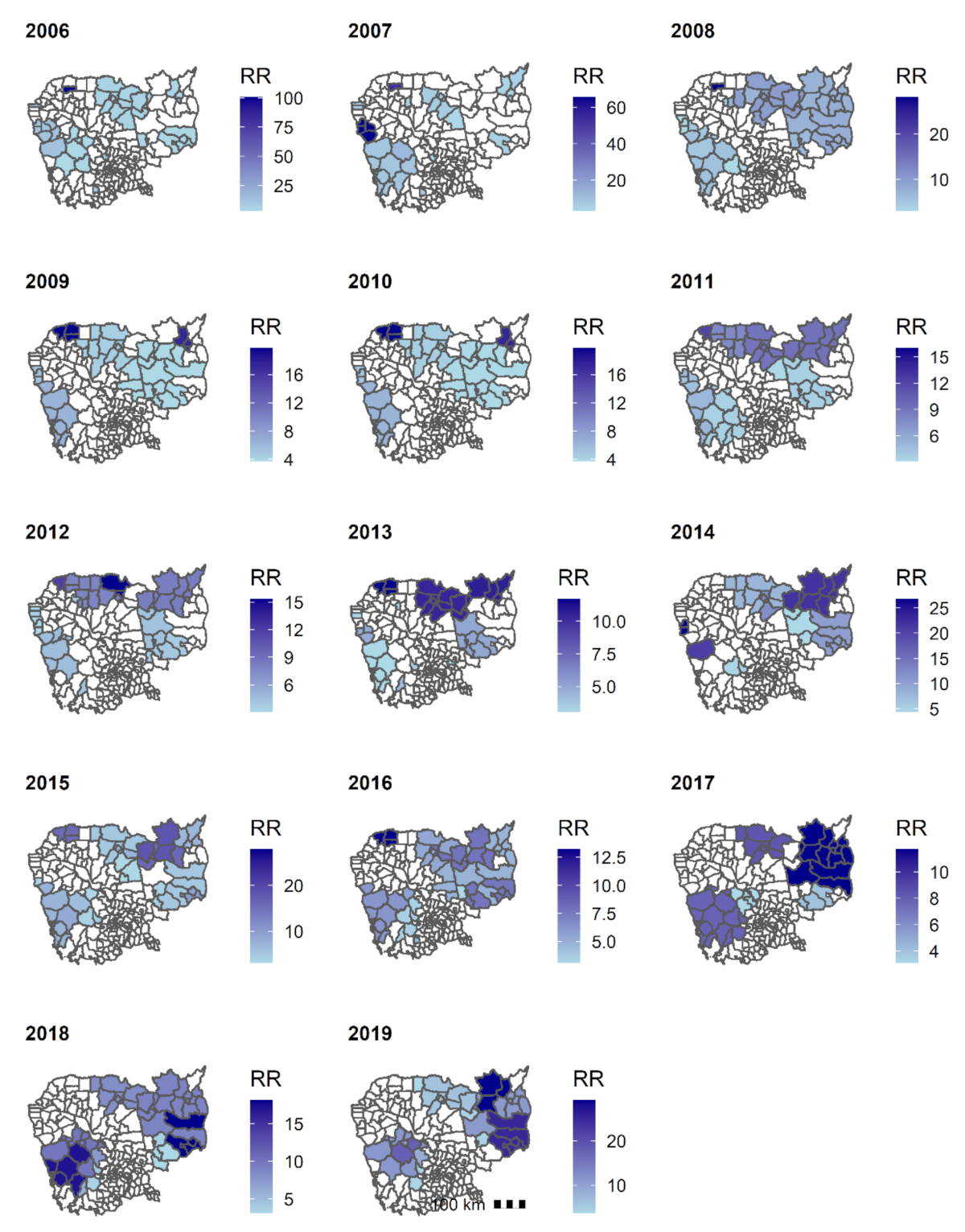
3.5. Geographical Distribution
3.5.1. Clusters of P. falciparum + Mixed
3.5.2. Clusters of P. vivax + Mixed
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Centers for Disease Control and Prevention (CDC) Malaria. Available online: https://www.cdc.gov/malaria/about/faqs.html (accessed on 15 August 2020).
- WHO. World Malaria Report; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization (WHO). WHO African Region. Available online: https://www.who.int/immunization/monitoring_surveillance/data/AFR/en/ (accessed on 28 August 2020).
- World Health Organization (WHO). WHO Western Pacific Region. Available online: https://www.who.int/westernpacific (accessed on 28 August 2020).
- World Health Organization (WHO). Region of the Americas. Available online: https://www.who.int/choice/demography/american_region/en/ (accessed on 29 August 2020).
- National Centre for Parasitology Entomology and Malaria Control (CNM). Cambodia Malaria Elimination Action Framework (2016–2020); CNM: Phnom Penh, Cambodia, 2016.
- National Centre for Parasitology Entomology and Malaria Control (CNM). National Malaria Porgram Review; CNM: Phnom Penh, Cambodia, 2019.
- St. Laurent, B.; Oy, K.; Miller, B.; Gasteiger, E.B.; Lee, E.; Sovannaroth, S.; Gwadz, R.W.; Anderson, J.M.; Fairhurst, R.M. Cow-baited tents are highly effective in sampling diverse Anopheles malaria vectors in Cambodia. Malar. J. 2016, 15, 440. [Google Scholar] [CrossRef] [Green Version]
- Durnez, L.; Mao, S.; Denis, L.; Roelants, P.; Sochantha, T.; Coosemans, M. Outdoor malaria transmission in forested villages of Cambodia. Malar. J. 2013, 12, 329. [Google Scholar] [CrossRef] [Green Version]
- Hii, J.; Rueda, L.M. Malaria vectors in the Greater Mekong Subregion: Overview of malaria vectors and remaining challenges. Southeast Asian J. Trop. Med. Public Health 2013, 44, 73–165, discussion 306–307. [Google Scholar]
- Bannister-Tyrrell, M.; Gryseels, C.; Sokha, S.; Dara, L.; Sereiboth, N.; James, N.; Thavrin, B.; Ly, P.; Soy Ty, K.; Peeters Grietens, K.; et al. Forest Goers and Multidrug-Resistant Malaria in Cambodia: An Ethnographic Study. Am. J. Trop. Med. Hyg. 2019, 100, 1170–1178. [Google Scholar] [CrossRef] [Green Version]
- Incardona, S.; Vong, S.; Chiv, L.; Lim, P.; Nhem, S.; Sem, R.; Khim, N.; Doung, S.; Mercereau-Puijalon, O.; Fandeur, T. Large-scale malaria survey in Cambodia: Novel insights on species distribution and risk factors. Malar. J. 2007, 6, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Centre for Parasitology Entomology and Malaria Control (CNM). The National Strategic Plan for Elimination of Malaria in the Kingdom of Cambodia 2011–2025; CNM: Phnom Penh, Cambodia, 2011.
- WHO. World Malaria Report; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- ACTwatch Cambodia 2009–2015 Reference Document. Available online: http://www.actwatch.info/projects/actwatch/cambodia (accessed on 21 November 2019).
- Group, A.C.; Phok, S.; Phanalasy, S.; Thein, S.T.; Likhitsup, A. Private sector opportunities and threats to achieving malaria elimination in the Greater Mekong Subregion: Results from malaria outlet surveys in Cambodia, the Lao PDR, Myanmar, and Thailand. Malar. J. 2017, 16, 180. [Google Scholar]
- Dondorp, A.M.; Fairhurst, R.M.; Slutsker, L.; Macarthur, J.R.; Breman, J.G.; Guerin, P.J.; Wellems, T.E.; Ringwald, P.; Newman, R.D.; Plowe, C.V. The threat of artemisinin-resistant malaria. N. Engl. J. Med. 2011, 365, 1073–1075. [Google Scholar] [CrossRef] [Green Version]
- Mahase, E. Malaria drugs left ineffective by spread of multidrug resistant parasites in southeast Asia. BMJ 2019, 366, l4807. [Google Scholar] [CrossRef]
- van der Pluijm, R.W.; Imwong, M.; Chau, N.H.; Hoa, N.T.; Thuy-Nhien, N.T.; Thanh, N.V.; Jittamala, P.; Hanboonkunupakarn, B.; Chutasmit, K.; Saelow, C.; et al. Determinants of dihydroartemisinin-piperaquine treatment failure in Plasmodium falciparum malaria in Cambodia, Thailand, and Vietnam: A prospective clinical, pharmacological, and genetic study. Lancet Infect. Dis. 2019, 19, 952–961. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, W.L.; Amato, R.; van der Pluijm, R.W.; Jacob, C.G.; Quang, H.H.; Thuy-Nhien, N.T.; Hien, T.T.; Hongvanthong, B.; Chindavongsa, K.; Mayxay, M.; et al. Evolution and expansion of multidrug-resistant malaria in southeast Asia: A genomic epidemiology study. Lancet Infect. Dis. 2019, 19, 943–951. [Google Scholar] [CrossRef]
- Imwong, M.; Hien, T.T.; Thuy-Nhien, N.T.; Dondorp, A.M.; White, N.J. Spread of a single multidrug resistant malaria parasite lineage (PfPailin) to Vietnam. Lancet Infect. Dis. 2017, 17, 1022–1023. [Google Scholar] [CrossRef]
- Imwong, M.; Suwannasin, K.; Kunasol, C.; Sutawong, K.; Mayxay, M.; Rekol, H.; Smithuis, F.M.; Hlaing, T.M.; Tun, K.M.; van der Pluijm, R.W.; et al. The spread of artemisinin-resistant Plasmodium falciparum in the Greater Mekong subregion: A molecular epidemiology observational study. Lancet Infect. Dis. 2017, 17, 491–497. [Google Scholar] [CrossRef] [Green Version]
- Denis, M.B.; Tsuyuoka, R.; Poravuth, Y.; Narann, T.S.; Seila, S.; Lim, C.; Incardona, S.; Lim, P.; Sem, R.; Socheat, D.; et al. Surveillance of the efficacy of artesunate and mefloquine combination for the treatment of uncomplicated falciparum malaria in Cambodia. Trop. Med. Int. Health TM IH 2006, 11, 1360–1366. [Google Scholar] [CrossRef] [PubMed]
- Noedl, H.; Se, Y.; Schaecher, K.; Smith, B.L.; Socheat, D.; Fukuda, M.M. Evidence of artemisinin-resistant malaria in western Cambodia. N. Engl. J. Med. 2008, 359, 2619–2620. [Google Scholar] [CrossRef]
- Lim, P.; Chim, P.; Sem, R.; Nemh, S.; Poravuth, Y.; Lim, C.; Seila, S.; Tsuyuoka, R.; Denis, M.B.; Socheat, D.; et al. In vitro monitoring of Plasmodium falciparum susceptibility to artesunate, mefloquine, quinine and chloroquine in Cambodia: 2001–2002. Acta Trop. 2005, 93, 31–40. [Google Scholar] [CrossRef]
- Bustos, M.D.; Wongsrichanalai, C.; Delacollette, C.; Burkholder, B. Monitoring antimalarial drug efficacy in the Greater Mekong Subregion: An overview of in vivo results from 2008 to 2010. Southeast Asian J. Trop. Med. Public Health 2013, 44, 201–230, discussion 306–307. [Google Scholar]
- Amaratunga, C.; Lim, P.; Suon, S.; Sreng, S.; Mao, S.; Sopha, C.; Sam, B.; Dek, D.; Try, V.; Amato, R.; et al. Dihydroartemisinin—piperaquine resistance in Plasmodium falciparum malaria in Cambodia: A multisite prospective cohort study. Lancet Infect. Dis. 2016, 16, 357–365. [Google Scholar] [CrossRef] [Green Version]
- Spring, M.D.; Lin, J.T.; Manning, J.E.; Vanachayangkul, P.; Somethy, S.; Bun, R.; Se, Y.; Chann, S.; Ittiverakul, M.; Sia-ngam, P.; et al. Dihydroartemisinin-piperaquine failure associated with a triple mutant including kelch13 C580Y in Cambodia: An observational cohort study. Lancet Infect. Dis. 2015, 15, 683–691. [Google Scholar] [CrossRef]
- Lon, C.; Manning, J.E.; Vanachayangkul, P.; So, M.; Sea, D.; Se, Y.; Gosi, P.; Lanteri, C.; Chaorattanakawee, S.; Sriwichai, S.; et al. Efficacy of two versus three-day regimens of dihydroartemisinin-piperaquine for uncomplicated malaria in military personnel in northern Cambodia: An open-label randomized trial. PLoS ONE 2014, 9, e93138. [Google Scholar] [CrossRef] [PubMed]
- Boyle, D. Dispute delays release of malaria money in Cambodia. Lancet 2015, 386, 1811. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Technical Strategy for Malaria 2016–2030; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Thacker, S.B.; Choi, K.; Brachman, P.S. The Surveillance of Infectious Diseases. JAMA 1983, 249, 1181–1185. [Google Scholar] [CrossRef]
- Aregawi, M.; Lynch, M.; Bekele, W.; Kebede, H.; Jima, D.; Taffese, H.S.; Yenehun, M.A.; Lilay, A.; Williams, R.; Thomson, M.; et al. Time series analysis of trends in malaria cases and deaths at hospitals and the effect of antimalarial interventions, 2001–2011, Ethiopia. PLoS ONE 2014, 9, e106359. [Google Scholar] [CrossRef] [PubMed]
- Comfort, A.B.; van Dijk, J.H.; Mharakurwa, S.; Stillman, K.; Gabert, R.; Korde, S.; Nachbar, N.; Derriennic, Y.; Musau, S.; Hamazakaza, P.; et al. Hospitalizations and costs incurred at the facility level after scale-up of malaria control: Pre-post comparisons from two hospitals in Zambia. Am. J. Trop. Med. Hyg. 2014, 90, 20–32. [Google Scholar] [CrossRef]
- Cissé, B.; Ba, E.H.; Sokhna, C.; Ndiaye, J.L.; Gomis, J.F.; Dial, Y.; Pitt, C.; Ndiaye, M.; Cairns, M.; Faye, E.; et al. Effectiveness of Seasonal Malaria Chemoprevention in Children under Ten Years of Age in Senegal: A Stepped-Wedge Cluster-Randomised Trial. PLoS Med. 2016, 13, e1002175. [Google Scholar] [CrossRef] [Green Version]
- Katureebe, A.; Zinszer, K.; Arinaitwe, E.; Rek, J.; Kakande, E.; Charland, K.; Kigozi, R.; Kilama, M.; Nankabirwa, J.; Yeka, A.; et al. Measures of Malaria Burden after Long-Lasting Insecticidal Net Distribution and Indoor Residual Spraying at Three Sites in Uganda: A Prospective Observational Study. PLoS Med. 2016, 13, e1002167. [Google Scholar] [CrossRef] [Green Version]
- Aregawi, M.; Malm, K.L.; Wahjib, M.; Kofi, O.; Allotey, N.K.; Yaw, P.N.; Abba-Baffoe, W.; Segbaya, S.; Owusu-Antwi, F.; Kharchi, A.T.; et al. Effect of anti-malarial interventions on trends of malaria cases, hospital admissions and deaths, 2005–2015, Ghana. Malar. J. 2017, 16, 177. [Google Scholar] [CrossRef]
- Ssempiira, J.; Kissa, J.; Nambuusi, B.; Kyozira, C.; Rutazaana, D.; Mukooyo, E.; Opigo, J.; Makumbi, F.; Kasasa, S.; Vounatsou, P. The effect of case management and vector-control interventions on space-time patterns of malaria incidence in Uganda. Malar. J. 2018, 17, 162. [Google Scholar] [CrossRef]
- Kenangalem, E.; Poespoprodjo, J.R.; Douglas, N.M.; Burdam, F.H.; Gdeumana, K.; Chalfein, F.; Prayoga; Thio, F.; Devine, A.; Marfurt, J.; et al. Malaria morbidity and mortality following introduction of a universal policy of artemisinin-based treatment for malaria in Papua, Indonesia: A longitudinal surveillance study. PLoS Med. 2019, 16, e1002815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lechthaler, F.; Matthys, B.; Lechthaler-Felber, G.; Likwela, J.L.; Mavoko, H.M.; Rika, J.M.; Mutombo, M.M.; Ruckstuhl, L.; Barczyk, J.; Shargie, E.; et al. Trends in reported malaria cases and the effects of malaria control in the Democratic Republic of the Congo. PLoS ONE 2019, 14, e0219853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tugume, A.; Muneza, F.; Oporia, F.; Kiconco, A.; Kihembo, C.; Kisakye, A.N.; Nsubuga, P.; Deogratias, S.; Yeka, A. Effects and factors associated with indoor residual spraying with Actellic 300 CS on malaria morbidity in Lira District, Northern Uganda. Malar. J. 2019, 18, 44. [Google Scholar] [CrossRef]
- Department of Planning and Health Information (DPHI). Health Information System Master Plan 2016–2020; DPHI: Phnom Penh, Cambodia, 2017. [Google Scholar]
- National Centre for Parasitology Entomology and Malaria Control (CNM). Malaria Information System; CNM: Phnom Penh, Cambodia, 2020.
- World Health Organization (WHO). WHO Malaria Terminology; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- OCHA. Cambodia Administrative Level 0–3 Population Statistics; OCHA: New York, NY, USA, 2019. [Google Scholar]
- National Institute of Statistics (NIS). Population Projections for Cambodia, 2008–2030; NIS: Phnom Penh, Cambodia, 2008.
- National Center for Parasitology Entomology and Malaria Control (CNM). National Treatment Guidelines for Malaria in Cambodia; CNM: Phnom Penh, Cambodia, 2014.
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Martin, K. SaTScan™, a Free Software That Analyzes Spatial, Temporal and Space-Time Data Using the Spatial, Temporal, or Space-Time Scan Statistics. Available online: https://www.satscan.org/ (accessed on 20 March 2019).
- Maude, R.J.; Nguon, C.; Ly, P.; Bunkea, T.; Ngor, P.; Canavati de la Torre, S.E.; White, N.J.; Dondorp, A.M.; Day, N.P.J.; White, L.J.; et al. Spatial and temporal epidemiology of clinical malaria in Cambodia 2004–2013. Malar. J. 2014, 13, 385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, H.-W.; Wang, L.-P.; Liang, S.; Liu, Y.-X.; Tong, S.-L.; Wang, J.-J.; Li, Y.-P.; Wang, X.-F.; Yang, H.; Ma, J.-Q.; et al. Change in Rainfall Drives Malaria Re-Emergence in Anhui Province, China. PLoS ONE 2012, 7, e43686. [Google Scholar] [CrossRef]
- Wardrop, N.A.; Barnett, A.G.; Atkinson, J.-A.; Clements, A.C.A. Plasmodium vivax malaria incidence over time and its association with temperature and rainfall in four counties of Yunnan Province, China. Malar. J. 2013, 12, 452. [Google Scholar] [CrossRef] [Green Version]
- Huang, F.; Zhou, S.; Zhang, S.; Wang, H.; Tang, L. Temporal correlation analysis between malaria and meteorological factors in Motuo County, Tibet. Malar. J. 2011, 10, 54. [Google Scholar] [CrossRef] [Green Version]
- Bomblies, A. Modeling the role of rainfall patterns in seasonal malaria transmission. Clim. Chang. 2012, 112, 673–685. [Google Scholar] [CrossRef]
- US Department of Interior. United States Geological Survey (USGS); U.S. Department of Interior: Washington, DC, USA, 2020.
- Sluydts, V.; Somony, H.; Coosemans, M.; Van Roey, K.; Gryseels, C.; Canier, L.; Kim, S.; Khim, N.; Sovannaroth, S.; Mean, V.; et al. Spatial clustering and risk factors of malaria infections in Ratanakiri Province, Cambodia. Malar. J. 2014, 13, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, U.S.; Mao, B.; Saphonn, V.; Bruce, J.; Meek, S.; Lines, J.; Cox, J. Cambodia Malaria Survey 2007; National Centre for Parasitology, Entomology and Malaria Control (CNM): Phnom Penh, Cambodia, 2007.
- Dysoley, L.; Rithea, L.; Bunkea, T.; Babu, S.; Sim, K.; Nguon, C.; Socheat, D.; Thompson, M.; Bruce, J.; de Beyl, C.Z.; et al. Cambodia Malaria Survey 2010; National Centre for Parasitology, Entomology and Malaria Control (CNM): Phnom Penh, Cambodia, 2010.
- Rekol, H.; Sovannaroth, S.; Dysoley, L.; Vanna, C.; Sokun, C.; Yeang, O.; Thavrin, B.K.; Montha, M.; Yom, Y.; Theasy, H.C.; et al. Cambodia Malaria Survey 2013; National Centre for Parasitology, Entomology and Malaria Control (CNM): Phnom Penh, Cambodia, 2013.
- National Centre for Parasitology, Entomology and Malaria Control (CNM). Cambodia Malaria Survey 2017; CNM: Phnom Penh, Cambodia, 2017.
- Jambou, R.; Legrand, E.; Niang, M.; Khim, N.; Lim, P.; Volney, B.; Ekala, M.T.; Bouchier, C.; Esterre, P.; Fandeur, T.; et al. Resistance of Plasmodium falciparum field isolates to in-vitro artemether and point mutations of the SERCA-type PfATPase6. Lancet 2005, 366, 1960–1963. [Google Scholar] [CrossRef]
- Khim, N.; Bouchier, C.; Ekala, M.T.; Incardona, S.; Lim, P.; Legrand, E.; Jambou, R.; Doung, S.; Puijalon, O.M.; Fandeur, T. Countrywide survey shows very high prevalence of Plasmodium falciparum multilocus resistance genotypes in Cambodia. Antimicrob. Agents Chemother. 2005, 49, 3147–3152. [Google Scholar] [CrossRef] [Green Version]
- Denis, M.B.; Tsuyuoka, R.; Lim, P.; Lindegardh, N.; Yi, P.; Top, S.N.; Socheat, D.; Fandeur, T.; Annerberg, A.; Christophel, E.M.; et al. Efficacy of artemether-lumefantrine for the treatment of uncomplicated falciparum malaria in northwest Cambodia. Trop. Med. Int. Health TM IH 2006, 11, 1800–1807. [Google Scholar] [CrossRef] [PubMed]
- Resistance to artemisinin derivatives along the Thai-Cambodian border. Relev. Epidemiol. Hebd. 2007, 82, 360.
- Shah, N.K.; Alker, A.P.; Sem, R.; Susanti, A.I.; Muth, S.; Maguire, J.D.; Duong, S.; Ariey, F.; Meshnick, S.R.; Wongsrichanalai, C. Molecular surveillance for multidrug-resistant Plasmodium falciparum, Cambodia. Emerg. Infect. Dis. 2008, 14, 1637–1640. [Google Scholar] [CrossRef]
- Wongsrichanalai, C.; Meshnick, S.R. Declining artesunate-mefloquine efficacy against falciparum malaria on the Cambodia-Thailand border. Emerg. Infect. Dis. 2008, 14, 716–719. [Google Scholar] [CrossRef] [PubMed]
- Antimalarial drug resistance, Thai-Cambodian border. Relev. Epidemiol. Hebd. 2009, 84, 94–95.
- Dondorp, A.M.; Nosten, F.; Yi, P.; Das, D.; Phyo, A.P.; Tarning, J.; Lwin, K.M.; Ariey, F.; Hanpithakpong, W.; Lee, S.J.; et al. Artemisinin resistance in Plasmodium falciparum malaria. N. Engl. J. Med. 2009, 361, 455–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, O.; Sié, A.; Meissner, P.; Schirmer, R.H.; Kouyaté, B. Artemisinin resistance on the Thai-Cambodian border. Lancet 2009, 374, 1419. [Google Scholar] [CrossRef]
- Rogers, W.O.; Sem, R.; Tero, T.; Chim, P.; Lim, P.; Muth, S.; Socheat, D.; Ariey, F.; Wongsrichanalai, C. Failure of artesunate-mefloquine combination therapy for uncomplicated Plasmodium falciparum malaria in southern Cambodia. Malar. J. 2009, 8, 10. [Google Scholar] [CrossRef] [Green Version]
- Yeung, S.; Socheat, D.; Moorthy, V.S.; Mills, A.J. Artemisinin resistance on the Thai-Cambodian border. Lancet 2009, 374, 1418–1419. [Google Scholar] [CrossRef]
- Duru, V.; Witkowski, B.; Ménard, D. Plasmodium falciparum Resistance to Artemisinin Derivatives and Piperaquine: A Major Challenge for Malaria Elimination in Cambodia. Am. J. Trop. Med. Hyg. 2016, 95, 1228–1238. [Google Scholar] [CrossRef]
- Population Services International and ACTwatch. Actwatch Outlet Survey Results: Cambodia 2009–2015; Population Services International and ACTwatch: Phnom Penh, Cambodia, 2016. [Google Scholar]
- Siv, S.; Roca-Feltrer, A.; Vinjamuri, S.B.; Bouth, D.M.; Lek, D.; Rashid, M.A.; By, N.P.; Popovici, J.; Huy, R.; Menard, D. Plasmodium vivax Malaria in Cambodia. Am. J. Trop. Med. Hyg. 2016, 95, 97–107. [Google Scholar] [CrossRef] [Green Version]
- Office of the Inspector General (OIG). Investigation Report: Global Fund Grants to CambodiaNational Centre for Parasitology Entomology and Malaria Control (CNM); OIG: Geneva, Switzerland, 2017. Available online: https://www.theglobalfund.org/media/5433/oig_gf-oig-17-004_report_en.pdf?u=637278311890000000 (accessed on 5 May 2020).
- Titthara, M. Mondulkiri logging crackdowns stun illegal industry. Khmer Times, 31 July 2019. [Google Scholar]
- Akulayi, L.; Alum, A.; Andrada, A.; Archer, J.; Arogundade, E.D.; Auko, E.; Badru, A.R.; Bates, K.; Bouanchaud, P.; Bruce, M.; et al. Evidence on anti-malarial and diagnostic markets in Cambodia to guide malaria elimination strategies and policies. Malar. J. 2017, 16, 171. [Google Scholar]
- Abba, K.; Kirkham, A.J.; Olliaro, P.L.; Deeks, J.J.; Donegan, S.; Garner, P.; Takwoingi, Y. Rapid diagnostic tests for diagnosing uncomplicated non-falciparum or Plasmodium vivax malaria in endemic countries. Cochrane Database System. Rev. 2014, 2014, Cd011431. [Google Scholar] [CrossRef] [Green Version]
- Chu, C.S.; White, N.J. Management of relapsing Plasmodium vivax malaria. Expert Rev. Anti Infect. Ther. 2016, 14, 885–900. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.R.; Watson, J.A.; Chu, C.S.; Puaprasert, K.; Duanguppama, J.; Day, N.P.J.; Nosten, F.; Neafsey, D.E.; Buckee, C.O.; Imwong, M.; et al. Resolving the cause of recurrent Plasmodium vivax malaria probabilistically. Nat. Commun. 2019, 10, 5595. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Control and Elimination of Plasmodium Vivax Malaria: Technical Brief; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Lu, G.; Liu, Y.; Beiersmann, C.; Feng, Y.; Cao, J.; Müller, O. Challenges in and lessons learned during the implementation of the 1-3-7 malaria surveillance and response strategy in China: A qualitative study. Infect. Dis. Poverty 2016, 5, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kheang, S.T.; Sovannaroth, S.; Barat, L.M.; Dysoley, L.; Kapella, B.K.; Po, L.; Nguon, S.; Gimnig, J.; Slot, R.; Samphornarann, T.; et al. Malaria elimination using the 1-3-7 approach: Lessons from Sampov Loun, Cambodia. BMC Public Health 2020, 20, 544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, M.C.; Donnelly, C.A.; Alpers, M.P.; Galinski, M.R.; Barnwell, J.W.; Walliker, D.; Day, K.P. Cross-Species Interactions Between Malaria Parasites in Humans. Science 2000, 287, 845. [Google Scholar] [CrossRef]
- Nagao, Y.; Kimura-Sato, M.; Chavalitshewinkoon-Petmitr, P.; Thongrungkiat, S.; Wilairatana, P.; Ishida, T.; Tan-Ariya, P.; de Souza, J.B.; Krudsood, S.; Looareesuwan, S. Suppression of Plasmodium falciparum by serum collected from a case of Plasmodium vivax infection. Malar. J. 2008, 7, 113. Available online: http://europepmc.org/abstract/MED/18582375; https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/pmid/18582375/pdf/?tool=EBI (accessed on 30 August 2020). [CrossRef] [PubMed] [Green Version]
- Whitehorn, J.; Coltart, C.; Manser, D.; Doherty, T. A mixed malaria infection: Is Plasmodium vivax good for you? Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 240–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haghdoost, A.A.; Alexander, N. Systematic review and meta-analysis of the interaction between Plasmodium falciparum and Plasmodium vivax in humans. J. Vector Borne Dis. 2007, 44, 33–43. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Number of Health Centers | Number of Hospitals | Total Malaria Case Notifications | Population (a) |
|---|---|---|---|---|
| 2006 | 1087 | 96 | 1183 | 13,474,489 |
| 2007 | 1087 | 96 | 1183 | 13,676,693 |
| 2008 | 1087 | 96 | 1183 | 13,880,509 |
| 2009 | 1087 | 96 | 1183 | 14,090,208 |
| 2010 | 1087 | 96 | 1183 | 14,308,740 |
| 2011 | 1087 | 96 | 1183 | 14,537,886 |
| 2012 | 1087 | 96 | 1183 | 14,776,866 |
| 2013 | 1087 | 96 | 1183 | 15,022,692 |
| 2014 | 1138 | 104 | 1242 | 15,270,790 |
| 2015 | 1148 | 107 | 1255 | 15,517,635 |
| 2016 | 1168 | 111 | 1279 | 15,762,370 |
| 2017 | 1195 | 116 | 1311 | 16,005,373 |
| 2018 | 1213 | 121 | 1334 | 16,245,454 |
| 2019 | 1225 | 125 | 1350 | 16,489,135 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chhim, S.; Piola, P.; Housen, T.; Herbreteau, V.; Tol, B. Malaria in Cambodia: A Retrospective Analysis of a Changing Epidemiology 2006–2019. Int. J. Environ. Res. Public Health 2021, 18, 1960. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041960
Chhim S, Piola P, Housen T, Herbreteau V, Tol B. Malaria in Cambodia: A Retrospective Analysis of a Changing Epidemiology 2006–2019. International Journal of Environmental Research and Public Health. 2021; 18(4):1960. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041960
Chicago/Turabian StyleChhim, Srean, Patrice Piola, Tambri Housen, Vincent Herbreteau, and Bunkea Tol. 2021. "Malaria in Cambodia: A Retrospective Analysis of a Changing Epidemiology 2006–2019" International Journal of Environmental Research and Public Health 18, no. 4: 1960. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041960