Comparison of the Effect on Fetal Growth of a Mixture of Atrazine and Nitrates in Drinking Water and of Active Tobacco Exposure during Pregnancy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area and Timeline
2.2. Data Collection
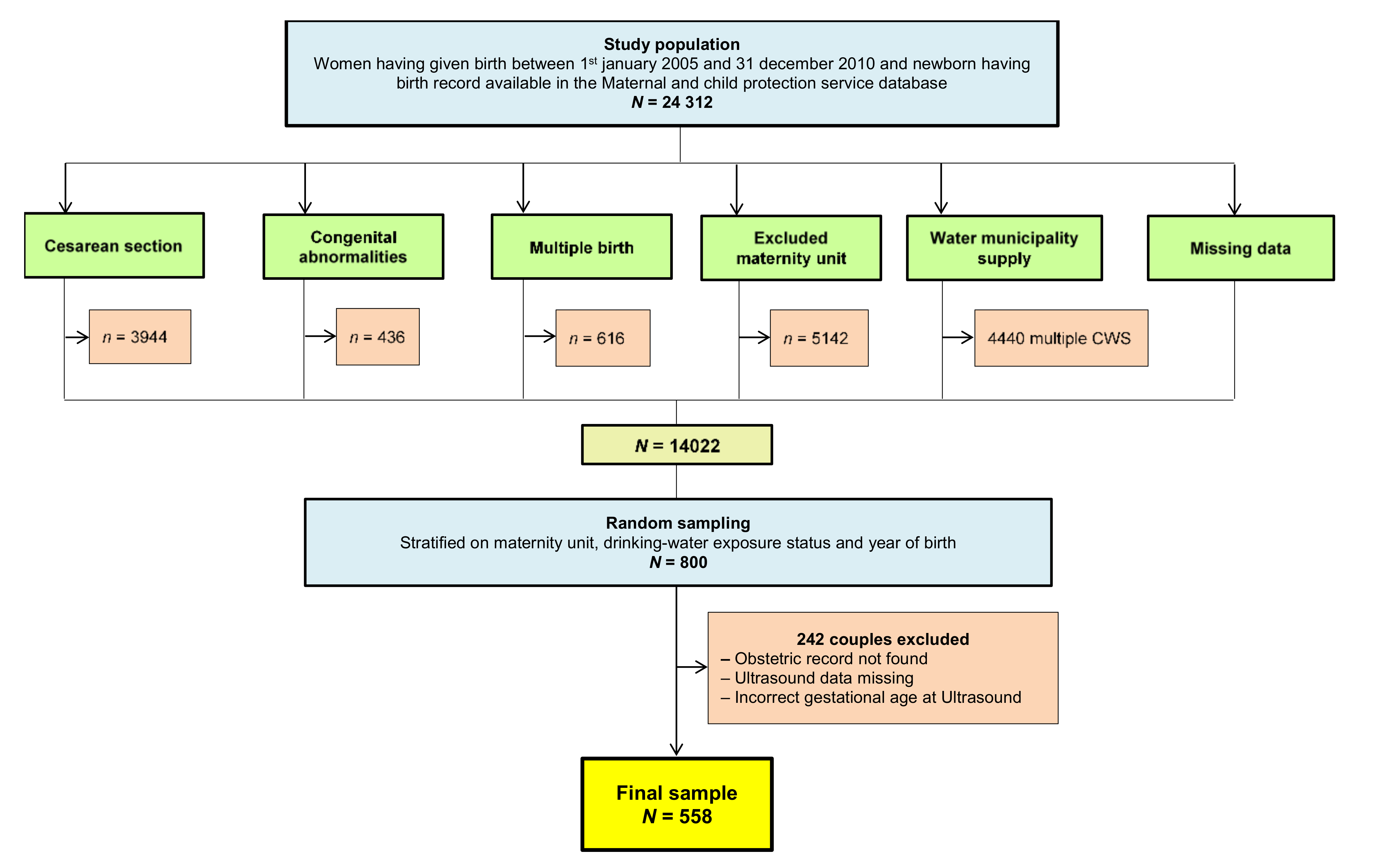
2.3. Population Study
2.4. Health Outcomes
2.5. Exposure Assessment
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barker, D.J.P. The Developmental Origins of Chronic Adult Disease. J. Am. Coll. Nutr. 2004, 93 (Suppl. 6), 26–33. [Google Scholar] [CrossRef]
- Mathews, T.J.; Miniño, A.M.; Osterman, M.J.K.; Strobino, D.M.; Guyer, B. Annual Summary of Vital Statistics: 2008. Pediatrics 2011, 127, 146–157. [Google Scholar] [CrossRef] [Green Version]
- Kramer, M.S. Determinants of Low Birth Weight: Methodological Assessment and Meta-Analysis. Bull. World Health Organ. 1987, 65, 663–737. [Google Scholar]
- Källén, K. The Impact of Maternal Smoking during Pregnancy on Delivery Outcome. Eur. J. Public Health 2001, 11, 329–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, M.S.; Séguin, L.; Lydon, J.; Goulet, L. Socio-Economic Disparities in Pregnancy Outcome: Why Do the Poor Fare so Poorly? Paediatr. Perinat. Epidemiol. 2000, 14, 194–210. [Google Scholar] [CrossRef] [PubMed]
- Abraham, M.; Alramadhan, S.; Iniguez, C.; Duijts, L.; Jaddoe, V.W.V.; Den Dekker, H.T.; Crozier, S.; Godfrey, K.M.; Hindmarsh, P.; Vik, T.; et al. A Systematic Review of Maternal Smoking during Pregnancy and Fetal Measurements with Meta-Analysis. PLoS ONE 2017, 12, e0170946. [Google Scholar] [CrossRef] [Green Version]
- Banderali, G.; Martelli, A.; Landi, M.; Moretti, F.; Betti, F.; Radaelli, G.; Lassandro, C.; Verduci, E. Short and Long Term Health Effects of Parental Tobacco Smoking during Pregnancy and Lactation: A Descriptive Review. J. Transl. Med. 2015, 13, 327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iñiguez, C.; Ballester, F.; Amorós, R.; Murcia, M.; Plana, A.; Rebagliato, M. Active and Passive Smoking during Pregnancy and Ultrasound Measures of Fetal Growth in a Cohort of Pregnant Women. J. Epidemiol. Community Health 2012, 66, 563–570. [Google Scholar] [CrossRef]
- Dušková, M.; Hruškovičová, H.; Simůnková, K.; Stárka, L.; Pařízek, A. The Effects of Smoking on Steroid Metabolism and Fetal Programming. J. Steroid Biochem. Mol. Biol. 2014, 139, 138–143. [Google Scholar] [CrossRef]
- Dane, A.J.; Havey, C.D.; Voorhees, K.J. The Detection of Nitro Pesticides in Mainstream and Sidestream Cigarette Smoke Using Electron Monochromator-Mass Spectrometry. Anal. Chem. 2006, 78, 3227–3233. [Google Scholar] [CrossRef] [PubMed]
- Almberg, K.S.; Turyk, M.E.; Jones, R.M.; Rankin, K.; Freels, S.; Stayner, L.T. Atrazine Contamination of Drinking Water and Adverse Birth Outcomes in Community Water Systems with Elevated Atrazine in Ohio, 2006–2008. Int. J. Environ. Res. Public Health 2018, 15, 1889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chevrier, C.; Limon, G.; Monfort, C.; Rouget, F.; Garlantézec, R.; Petit, C.; Durand, G.; Cordier, S. Urinary Biomarkers of Prenatal Atrazine Exposure and Adverse Birth Outcomes in the PELAGIE Birth Cohort. Environ. Health Perspect. 2011, 119, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Munger, R.; Isacson, P.; Hu, S.; Burns, T.; Hanson, J.; Lynch, C.F.; Cherryholmes, K.; Van Dorpe, P.; Hausler, W.J. Intrauterine Growth Retardation in Iowa Communities with Herbicide-Contaminated Drinking Water Supplies. Environ. Health Perspect. 1997, 105, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Ochoa-Acuna, H.; Frankenberger, J.; Hahn, L.; Carbajo, C. Drinking-Water Herbicide Exposure in Indiana and Prevalence of Small-for-Gestational-Age and Preterm Delivery. Environ. Health Perspect. 2009, 117, 1619–1624. [Google Scholar] [CrossRef] [Green Version]
- Villanueva, C.M.; Durand, G.; Coutte, M.B.; Chevrier, C.; Cordier, S. Atrazine in Municipal Drinking Water and Risk of Low Birth Weight, Preterm Delivery, and Small-for-Gestational-Age Status. Occup. Environ. Med. 2005, 62, 400–405. [Google Scholar] [CrossRef] [Green Version]
- Migeot, V.; Albouy-Llaty, M.; Carles, C.; Limousi, F.; Strezlec, S.; Dupuis, A.; Rabouan, S. Drinking-Water Exposure to a Mixture of Nitrate and Low-Dose Atrazine Metabolites and Small-for-Gestational Age (SGA) Babies: A Historic Cohort Study. Environ. Res. 2013, 122, 58–64. [Google Scholar] [CrossRef]
- Guillette, L.J. Endocrine Disrupting Contaminants—Beyond the Dogma. Environ. Health Perspect. 2006, 114 (Suppl. 1), 9–12. [Google Scholar] [CrossRef] [Green Version]
- Guillette, L.J.; Edwards, T.M. Is Nitrate an Ecologically Relevant Endocrine Disruptor in Vertebrates? Integr. Comp. Biol. 2005, 45, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Panesar, N.S.; Chan, K.W. Decreased Steroid Hormone Synthesis from Inorganic Nitrite and Nitrate: Studies in Vitro and in Vivo. Toxicol. Appl. Pharmacol. 2000, 169, 222–230. [Google Scholar] [CrossRef] [PubMed]
- McKinlay, R.; Plant, J.A.; Bell, J.N.B.; Voulvoulis, N. Endocrine Disrupting Pesticides: Implications for Risk Assessment. Environ. Int. 2008, 34, 168–183. [Google Scholar] [CrossRef] [PubMed]
- Silins, I.; Hogberg, J. Combined Toxic Exposures and Human Health: Biomarkers of Exposure and Effect. Int. J. Environ. Res. Public Health 2011, 8, 629–647. [Google Scholar] [CrossRef] [Green Version]
- Perez, J.; Domingues, I.; Soares, A.M.; Loureiro, S. Growth Rate of Pseudokirchneriella Subcapitata Exposed to Herbicides Found in Surface Waters in the Alqueva Reservoir (Portugal): A Bottom-up Approach Using Binary Mixtures. Ecotoxicology 2011, 20, 1167–1175. [Google Scholar] [CrossRef]
- Stayner, L.T.; Almberg, K.; Jones, R.; Graber, J.; Pedersen, M.; Turyk, M. Atrazine and Nitrate in Drinking Water and the Risk of Preterm Delivery and Low Birth Weight in Four Midwestern States. Environ. Res. 2017, 152, 294–303. [Google Scholar] [CrossRef]
- Hammoud, A.O.; Bujold, E.; Sorokin, Y.; Schild, C.; Krapp, M.; Baumann, P. Smoking in Pregnancy Revisited: Findings from a Large Population-Based Study. Am. J. Obstet. Gynecol. 2005, 192, 1856–1862. [Google Scholar] [CrossRef] [PubMed]
- Jaddoe, V.W.; Verburg, B.O.; de Ridder, M.A.; Hofman, A.; Mackenbach, J.P.; Moll, H.A.; Steegers, E.A.; Witteman, J.C. Maternal Smoking and Fetal Growth Characteristics in Different Periods of Pregnancy: The Generation R Study. Am. J. Epidemiol. 2007, 165, 1207–1215. [Google Scholar] [CrossRef] [Green Version]
- MacArthur, C.; Knox, E.G. Smoking in Pregnancy: Effects of Stopping at Different Stages. Br. J. Obstet. Gynaecol. 1988, 95, 551–555. [Google Scholar] [CrossRef]
- Hadlock, F.P.; Harrist, R.B.; Sharman, R.S.; Deter, R.L.; Park, S.K. Estimation of Fetal Weight with the Use of Head, Body, and Femur Measurements—A Prospective Study. Am. J. Obstet. Gynecol. 1985, 151, 333–337. [Google Scholar] [CrossRef]
- Collet, M.; Vilain, A. Les Certificats de Santé de l’Enfant Au Huitième Jour (CS8). Validités 2006 et 2007; Direction de La Recherche, Des Études, de L’évaluation et Des Statistiques: Paris, France, 2010. [Google Scholar]
- Iñiguez, C.; Ballester, F.; Estarlich, M.; Esplugues, A.; Murcia, M.; Llop, S.; Plana, A.; Amorós, R.; Rebagliato, M. Prenatal Exposure to Traffic-Related Air Pollution and Fetal Growth in a Cohort of Pregnant Women. Occup. Environ. Med. 2012, 69, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Hadlock, F.P.; Deter, R.L.; Harrist, R.B.; Park, S.K. Estimating Fetal Age: Computer-Assisted Analysis of Multiple Fetal Growth Parameters. Radiology 1984, 152, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Arrêté Du 24 Janvier 2005 Relatif Aux Conditions D’agrément Des Laboratoires Pour La Réalisation Des Prélèvements et Des Analyses Du Contrôle Sanitaire Des Eaux; JORF n°44 du 22 février 2005; Légifrance: Paris, France, 2005.
- Laird, N.M.; Ware, J.H. Random-Effects Models for Longitudinal Data. Biometrics 1982, 38, 963–974. [Google Scholar] [CrossRef]
- Gaillard, R.; de Ridder, M.A.J.; Verburg, B.O.; Witteman, J.C.M.; Mackenbach, J.P.; Moll, H.A.; Hofman, A.; Steegers, E.A.P.; Jaddoe, V.W.V. Individually Customised Fetal Weight Charts Derived from Ultrasound Measurements: The Generation R Study. Eur. J. Epidemiol. 2011, 26, 919–926. [Google Scholar] [CrossRef] [Green Version]
- Cardenas, A.; Lutz, S.M.; Everson, T.M.; Perron, P.; Bouchard, L.; Hivert, M.-F. Mediation by Placental DNA Methylation of the Association of Prenatal Maternal Smoking and Birth Weight. Am. J. Epidemiol. 2019, 188, 1878–1886. [Google Scholar] [CrossRef]
- Commissariat Général Au Développement Durable. Les Pesticides Dans Les Milieux Aquatiques Données 2007. N°26. Juillet. 2010. Available online: Https://Www.Google.Com/Url?Sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwiJgJLLu73rAhWC2eAKHQk4CE8QFjAAegQIAxAB&url=https%3A%2F%2Fwww.Statistiques.Developpement-Durable.Gouv.Fr%2Fsites%2Fdefault%2Ffiles%2F2019-01%2Fles-Pesticides-Dans-Les%2520milieux-Aquatiques-Etudes-et-Documents-26-Juillet2010.Pdf&usg=AOvVaw0ky6paMUNbHccb2D1AJcVD (accessed on 4 April 2012).
- Avis Du 27/11/01 Relatif Aux Détenteurs D’autorisation de Mise Sur Le Marché, Aux Distributeurs et Aux Utilisateurs de Produits Phytopharmaceutiques Contenant de L’atrazine, de La Simazine, de La Cyanazine, de L’amétryne Ou de La Terbuthylazine; JO N° 275 Du 27 Novembre 2001; Légifrance: Paris, France, 2001.
- Ardilly, P. Les Techniques de Sondage; Editions Technip: Paris, France, 2006. [Google Scholar]
- Blondel, B.; Kermarrec, M. Enquête Nationale Périnatale 2010. Les Naissances En 2010 et Leur Évolution Depuis 2003; Inserm: Paris, France, 2011. [Google Scholar]
- Vandenberg, L.N.; Colborn, T.; Hayes, T.B.; Heindel, J.J.; Jacobs, D.R., Jr.; Lee, D.-H.; Shioda, T.; Soto, A.M.; vom Saal, F.S.; Welshons, W.V.; et al. Hormones and Endocrine-Disrupting Chemicals: Low-Dose Effects and Nonmonotonic Dose Responses. Endocr. Rev. 2012, 33, 378–455. [Google Scholar] [CrossRef]
- Makris, K.C.; Andra, S.S. Limited Representation of Drinking-Water Contaminants in Pregnancy-Birth Cohorts. Sci. Total Environ. 2014, 468–469, 165–175. [Google Scholar] [CrossRef]
- Ferguson, K.K.; Meeker, J.D.; Cantonwine, D.E.; Mukherjee, B.; Pace, G.G.; Weller, D.; McElrath, T.F. Environmental Phenol Associations with Ultrasound and Delivery Measures of Fetal Growth. Environ. Int. 2018, 112, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Heil, S.H.; Higgins, S.T.; Bernstein, I.M.; Solomon, L.J.; Rogers, R.E.; Thomas, C.S.; Badger, G.J.; Lynch, M.E. Effects of Voucher-Based Incentives on Abstinence from Cigarette Smoking and Fetal Growth among Pregnant Women. Addiction 2008, 103, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Ribas-Fitó, N.; Ramón, R.; Ballester, F.; Grimalt, J.; Marco, A.; Olea, N.; Posada, M.; Rebagliato, M.; Tardón, A.; Torrent, M.; et al. Child Health and the Environment: The INMA Spanish Study. Paediatr. Perinat. Epidemiol. 2006, 20, 403–410. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Li, J.; Xia, W.; Li, Y.; Zhang, B.; Zhou, A.; Hu, J.; Li, C.; Zhao, H.; Jiang, M.; et al. The Association of Repeated Measurements of Prenatal Exposure to Triclosan with Fetal and Early-Childhood Growth. Environ. Int. 2018, 120, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.R. Endocrine Disruption: Developmental Picture Window. Env. Health Perspect. 2009, 117, A101. [Google Scholar] [CrossRef] [PubMed]
- Lepercq, J.; Boileau, P. Physiologie de La Croissance Foetale. EMC Gynecol. Obstet. 2005, 2, 199–208. [Google Scholar] [CrossRef]
- Bernstein, I.M.; Plociennik, K.; Stahle, S.; Badger, G.J.; Secker-Walker, R. Impact of Maternal Cigarette Smoking on Fetal Growth and Body Composition. Am. J. Obstet. Gynecol. 2000, 183, 883–886. [Google Scholar] [CrossRef]
- Menard, C.; Girard, D.; Lèon, C.; Beck, F. (dir) Baromètre Santé Environnement 2007; INPES: Saint-Denis, France, 2008; 420p. [Google Scholar]
- Zender, R.; Bachand, A.M.; Reif, J.S. Exposure to Tap Water during Pregnancy. J. Expo. Anal. Environ. Epidemiol. 2001, 11, 224–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albouy-Llaty, M.; Dupuis, A.; Grignon, C.; Strezlec, S.; Pierre, F.; Rabouan, S.; Migeot, V. Estimating Drinking-Water Ingestion and Dermal Contact with Water in a French Population of Pregnant Women: The EDDS Cohort Study. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 308–316. [Google Scholar] [CrossRef]
- Walter, S.D. The Ecologic Method in the Study of Environmental Health. I. Overview of the Method. Environ. Health Perspect. 1991, 94, 61–65. [Google Scholar] [PubMed]
- Tong, S. Migration Bias in Ecologic Studies. Eur. J. Epidemiol. 2000, 16, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Belanger, K. Review of Research on Residential Mobility during Pregnancy: Consequences for Assessment of Prenatal Environmental Exposures. J. Expo. Sci. Environ. Epidemiol. 2012, 22, 429–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodgson, S.; Lurz, P.W.W.; Shirley, M.D.F.; Bythell, M.; Rankin, J. Exposure Misclassification Due to Residential Mobility during Pregnancy. Int. J. Hyg. Environ. Health 2015, 218, 414–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slama, R.; Cordier, S. Impact of chemical and physical environmental factors on the course and outcome of pregnancy. J. Gynécologie Obstétrique Biol. Reprod. 2013, 42, 413–444. [Google Scholar] [CrossRef] [PubMed]
- Migeot, V.; Dupuis, A.; Cariot, A.; Albouy-Llaty, M.; Pierre, F.; Rabouan, S. Bisphenol a and Its Chlorinated Derivatives in Human Colostrum. Environ. Sci. Technol. 2013, 47, 13791–13797. [Google Scholar] [CrossRef]
- Venisse, N.; Grignon, C.; Brunet, B.; Thévenot, S.; Bacle, A.; Migeot, V.; Dupuis, A. Reliable Quantification of Bisphenol A and Its Chlorinated Derivatives in Human Urine Using UPLC-MS/MS Method. Talanta 2014, 125, 284–292. [Google Scholar] [CrossRef]
- Ferguson, K.K.; Meeker, J.D.; Cantonwine, D.E.; Chen, Y.-H.; Mukherjee, B.; McElrath, T.F. Urinary Phthalate Metabolite and Bisphenol A Associations with Ultrasound and Delivery Indices of Fetal Growth. Environ. Int. 2016, 94, 531–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoker, T.E.; Cooper, R.L. Distribution of 14C-Atrazine Following an Acute Lactational Exposure in the Wistar Rat. Reprod. Toxicol. 2007, 23, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Chevrier, C.; Serrano, T.; Lecerf, R.; Limon, G.; Petit, C.; Monfort, C.; Hubert-Moy, L.; Durand, G.; Cordier, S. Environmental Determinants of the Urinary Concentrations of Herbicides during Pregnancy: The PELAGIE Mother-Child Cohort (France). Environ. Int. 2014, 63, 11–18. [Google Scholar] [CrossRef]
- Mayhoub, F.; Berton, T.; Bach, V.; Tack, K.; Deguines, C.; Floch-Barneaud, A.; Desmots, S.; Stephan-Blanchard, E.; Chardon, K. Self-Reported Parental Exposure to Pesticide during Pregnancy and Birth Outcomes: The MecoExpo Cohort Study. PLoS ONE 2014, 9, e99090. [Google Scholar] [CrossRef]
- Perni, S.C.; Chervenak, F.A.; Kalish, R.B.; Magherini-Rothe, S.; Predanic, M.; Streltzoff, J.; Skupski, D.W. Intraobserver and Interobserver Reproducibility of Fetal Biometry. Ultrasound Obstet. Gynecol. 2004, 24, 654–658. [Google Scholar] [CrossRef]
- Verburg, B.O.; Mulder, P.G.H.; Hofman, A.; Jaddoe, V.W.V.; Witteman, J.C.M.; Steegers, E.A.P. Intra- and Interobserver Reproducibility Study of Early Fetal Growth Parameters. Prenat. Diagn. 2008, 28, 323–331. [Google Scholar] [CrossRef]
- Anderson, N.G.; Jolley, I.J.; Wells, J.E. Sonographic Estimation of Fetal Weight: Comparison of Bias, Precision and Consistency Using 12 Different Formulae. Ultrasound Obstet. Gynecol. 2007, 30, 173–179. [Google Scholar] [CrossRef]
- Geerts, L.; Widmer, T. Which Is the Most Accurate Formula to Estimate Fetal Weight in Women with Severe Preterm Preeclampsia? J. Matern. Neonatal Med. 2011, 24, 271–279. [Google Scholar] [CrossRef] [PubMed]
- U.S.A. Department of Health and Human Service. For Toxic Substances and Disease Registry Toxicological Profile for Atrazine. Available online: http://www.Atsdr.Cdc.Gov/Toxprofiles/Tp153.Pdf (accessed on 10 April 2013).
- Van den Berg, G.; van Eijsden, M.; Vrijkotte, T.G.M.; Gemke, R.J.B.J. Educational Inequalities in Perinatal Outcomes: The Mediating Effect of Smoking and Environmental Tobacco Exposure. PLoS ONE 2012, 7, e37002. [Google Scholar] [CrossRef] [Green Version]
- Sathyanarayana, S.; Focareta, J.; Dailey, T.; Buchanan, S. Environmental Exposures: How to Counsel Preconception and Prenatal Patients in the Clinical Setting. Am. J. Obstet. Gynecol. 2012, 207, 463–470. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics of The Study Population and Potential Confounders | Raw Results | Weighted Results * | ||||
|---|---|---|---|---|---|---|
| Missing Values | Total (N = 558) | Total (N = 9013) | ||||
| N | % | N | % | N | % | |
| Sex of the newborn | 0 | 0 | ||||
| Boy | 238 | 42.7 | 3893 | 43.2 | ||
| Girl | 320 | 57.4 | 5120 | 56.8 | ||
| Premature birth | 0 | 0 | ||||
| Yes | 16 | 2.9 | 282 | 3.1 | ||
| Household occupation | 5 | 1 | ||||
| Disadvantaged | 69 | 12.5 | 1157 | 13.0 | ||
| Moderately advantaged | 352 | 63.7 | 5932 | 66.5 | ||
| Advantaged | 132 | 23.9 | 1825 | 20.5 | ||
| Rural location of residence | 0 | 0 | ||||
| Yes | 206 | 36.9 | 2974 | 33.0 | ||
| Primiparity | 13 | 2 | ||||
| Yes | 215 | 39.5 | 3329 | 37.6 | ||
| Maternal age (years) | 0 | 0 | ||||
| <27 | 135 | 24.2 | 2211 | 24.5 | ||
| 27–29 | 124 | 22.2 | 2144 | 23.8 | ||
| 30–33 | 154 | 27.6 | 2497 | 27.7 | ||
| >33 | 145 | 26.0 | 2161 | 24.0 | ||
| Maternal body mass index (kg/m²) | 6 | 1 | ||||
| <18 | 24 | 4.4 | 395 | 4.5 | ||
| 18–24 | 376 | 68.1 | 5858 | 66.1 | ||
| 25–29 | 91 | 16.5 | 1605 | 18.1 | ||
| >29 | 61 | 11.1 | 1011 | 11.4 | ||
| History of low birthweight | 7 | 1 | ||||
| Yes | 20 | 3.6 | 314 | 3.5 | ||
| Gestational diabetes | 49 | 9 | ||||
| Yes | 42 | 8.3 | 685 | 8.3 | ||
| Season during second trimester | 0 | 0 | ||||
| Spring | 124 | 22.2 | 2131 | 23.6 | ||
| Summer | 146 | 26.2 | 2214 | 24.6 | ||
| Fall | 132 | 23.7 | 2193 | 24.3 | ||
| Winter | 156 | 28.0 | 2475 | 27.5 | ||
| Smoking during pregnancy | 50 | 9 | ||||
| Yes | 110 | 21.7 | 1665 | 20.5 | ||
| Mixture exposure in drinking water during the whole pregnancy | 0 | 0 | ||||
| Atrazine metabolites No and Nitrates < 18.14 mg/L | 66 | 11.8 | 1224 | 13.6 | ||
| Atrazine metabolites No and Nitrates 18.14–30.33 mg/L | 137 | 24.6 | 2679 | 29.7 | ||
| Atrazine metabolites No and Nitrates > 30.33 mg/L | 72 | 12.9 | 1279 | 14.2 | ||
| Atrazine metabolites Yes and Nitrates < 18.14 mg/L | 120 | 21.5 | 2532 | 28.1 | ||
| Atrazine metabolites Yes and Nitrates 18.14–30.33 mg/L | 54 | 9.7 | 538 | 6.0 | ||
| Atrazine metabolites Yes and Nitrates > 30.33 mg/L | 109 | 19.5 | 761 | 8.4 | ||
| Fetal Weight Evolution during Pregnancy According to Drinking Water Mixture Exposure and Active Tobacco Exposure before and after Adjustment for Available Confounders | Fetal Weight between Second Trimester and Birth & in Grams | |||||
|---|---|---|---|---|---|---|
| Unadjusted Analysis | Adjusted Analysis (N = 458) Model #1 | |||||
| Difference | 95%CI | p | Difference | 95%CI | p | |
| Weight evolution according to drinking-water mixture exposure during pregnancy in grams | 0.512 | 0.481 | ||||
| Atrazine metabolites No and Nitrates < 18.14 mg/L | 1 | 1 | ||||
| Atrazine metabolites No and Nitrates 18.14–30.33 mg/L | −0.60 | [−4.48; 3.28] | −0.76 | [−4.56; 3.04] | ||
| Atrazine metabolites No and Nitrates > 30.33 mg/L | −1.48 | [−6.03; 3.06] | −1.60 | [−6.06; 2.86] | ||
| Atrazine metabolites Yes and Nitrates < 18.14 mg/L | 1.98 | [−2.03; 5.99] | 1.85 | [−2.08; 5.79] | ||
| Atrazine metabolites Yes and Nitrates 18.14–30.33 mg/L | 0.02 | [−4.62; 4.66] | −0.17 | [−4.72; 4.38] | ||
| Atrazine metabolites Yes and Nitrates > 30.33 mg/L | 1.06 | [−2.99; 5.11] | 0.97 | [−3.01; 4.94] | ||
| Weight evolution according to smoking during pregnancy in grams | 0.010 | 0.009 | ||||
| No | 1 | 1 | ||||
| Yes | −3.48 | [−6.13; −0.83] | −3.46 | [−6.07; −0.85] | ||
| Season during the second trimester | 0.812 | 0.759 | ||||
| Summer | 1 | 1 | ||||
| Fall | −29.66 | [−90.53; 31.21] | −31.37 | [−91.21; 28.48] | ||
| Winter | −15.13 | [−73.63; 43.37] | −20.92 | [−79.78; 37.94] | ||
| Spring | −19.46 | [−82.84; 43.91] | −10.22 | [−72.78; 52.34] | ||
| Newborn gender | 0.004 | 0.005 | ||||
| Boy | 1 | 1 | ||||
| Girl | −64.62 | [−108.46; −20.78] | −62.26 | [−105.98; −18.55] | ||
| Maternal weight before pregnancy (kg) | 2.65 | [1.09; 4.22] | 0.001 | 2.48 | [0.91; 4.05] | 0.002 |
| Maternal age (years) | 0.614 | 0.901 | ||||
| <27 | −21.79 | [−85.43; 41.85] | 7.79 | [−58.33; 73.91] | ||
| 27–29 | 1 | 1 | ||||
| 29–33 | 4.42 | [−57.82; 66.66] | 16.44 | [−44.65; 77.53] | ||
| >33 | 19.89 | [−43.38; 83.16] | 23.01 | [−40.84; 86.86] | ||
| History of low birth weight | 0.579 | 0.483 | ||||
| No | 1 | 1 | ||||
| Yes | −34.01 | [−154.30; 86.28] | −43.64 | [−165.54; 78.26] | ||
| Household occupation | 0.842 | 0.987 | ||||
| Advantageous | 1 | 1 | ||||
| Moderately advantageous | 2.04 | [−50.36; 54.45] | −3.68 | [−55.72; 48.35] | ||
| Disadvantageous | −18.74 | [−97.09; 59.61] | −5.94 | [−86.70; 74.83] | ||
| Gestational diabetes | 0.108 | 0.169 | ||||
| No | 1 | 1 | ||||
| Yes | 63.25 | [−13.97; 140.47] | 53.76 | [−22.95; 130.46] | ||
| Rural location of residence at birth | 0.911 | 0.722 | ||||
| No | 1 | 1 | ||||
| Yes | −2.57 | [−47.72; 42.58] | −8.69 | [−56.66; 39.28] | ||
| Comparison of Non-Nested Models of Fetal Weight Evolution according to Active Tobacco Exposure and Drinking Water Mixture Exposure during Pregnancy | Fetal Weight between Second Trimester and Birth in Grams & (N = 458) | |||||
|---|---|---|---|---|---|---|
| Only Drinking-Water Exposure Model #2 AIC = 19,658.4 | Only Tobacco Exposure Model #3 AIC = 19,636.7 | |||||
| Difference | 95%CI | p | Difference | 95%CI | p | |
| Weight evolution according to mixture exposure in drinking water during pregnancy in grams | 0.506 | |||||
| Atrazine metabolites No and Nitrates < 18.14 mg/L | 1 | |||||
| Atrazine metabolites No and Nitrates 18.14–30.33 mg/L | −0.64 | [−4.46; 3.19] | ||||
| Atrazine metabolites No and Nitrates > 30.33 mg/L | −1.52 | [−6.00; 2.97] | ||||
| Atrazine metabolites Yes and Nitrates < 18.14 mg/L | 1.93 | [−2.02; 5.89] | ||||
| Atrazine metabolites Yes and Nitrates 18.14−30.33 mg/L | −0.03 | [−4.61; 4.55] | ||||
| Atrazine metabolites Yes and Nitrates > 30.33 mg/L | 0.98 | [−3.01; 4.98] | ||||
| Weight evolution according to smoking during pregnancy | 0.010 | |||||
| No | 1 | |||||
| Yes | −3.43 | [−6.05; −0.82] | ||||
| Season during second trimester | 0.779 | 0.776 | ||||
| Summer | 1 | 1 | ||||
| Fall | −31.44 | [−91.73; 28.85] | −29.55 | [−89.25; 30.15] | ||
| Winter | −19.72 | [−79.02; 39.58] | −21.55 | [−79.65; 36.54] | ||
| Spring | −13.96 | [−76.89; 48.97] | −9.55 | [−72.14; 53.04] | ||
| Newborn sex | 0.010 | 0.003 | ||||
| Boy | 1 | 1 | ||||
| Girl | −57.97 | [−101.90; −14.05] | −65.23 | [−108.87; −21.58] | ||
| Maternal weight before pregnancy (kg) | 2.51 | [0.93; 4.09] | 0.002 | 2.44 | [0.87; 4.01] | 0.002 |
| Maternal age (years) | 0.749 | 0.895 | ||||
| <27 | −8.98 | [−74.13; 56.17] | 7.24 | [−58.83; 73.30] | ||
| 27–29 | 1 | 1 | ||||
| 29–33 | 12.51 | [−48.96; 73.98] | 16.12 | [−45.03; 77.27] | ||
| >33 | 24.40 | [−39.93; 88.73] | 23.29 | [−40.06; 86.64] | ||
| History of low birth weight | 0.340 | 0.450 | ||||
| No | 1 | 1 | ||||
| Yes | −59.38 | [−181.49; 62.74] | −46.74 | [−167.99; 74.51] | ||
| Household occupation | 0.862 | 0.998 | ||||
| Advantageous | 1 | 1 | ||||
| Moderately advantageous | −6.58 | [−58.93; 45.77] | −0.58 | [−52.38; 51.23] | ||
| Disadvantageous | −22.24 | [−102.38; 57.90] | −2.29 | [−82.81; 78.23] | ||
| Gestational diabetes | 0.217 | 0.156 | ||||
| No | 1 | 1 | ||||
| Yes | 48.63 | [−28.54; 125.80] | 55.25 | [−21.10; 131.60] | ||
| Rural location of residence at birth | 0.791 | 0.692 | ||||
| No | 1 | 1 | ||||
| Yes | −6.51 | [−54.81; 41.79] | −9.04 | [−53.90; 35.82] | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carles, C.; Albouy-Llaty, M.; Dupuis, A.; Rabouan, S.; Migeot, V. Comparison of the Effect on Fetal Growth of a Mixture of Atrazine and Nitrates in Drinking Water and of Active Tobacco Exposure during Pregnancy. Int. J. Environ. Res. Public Health 2021, 18, 2200. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18042200
Carles C, Albouy-Llaty M, Dupuis A, Rabouan S, Migeot V. Comparison of the Effect on Fetal Growth of a Mixture of Atrazine and Nitrates in Drinking Water and of Active Tobacco Exposure during Pregnancy. International Journal of Environmental Research and Public Health. 2021; 18(4):2200. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18042200
Chicago/Turabian StyleCarles, Camille, Marion Albouy-Llaty, Antoine Dupuis, Sylvie Rabouan, and Virginie Migeot. 2021. "Comparison of the Effect on Fetal Growth of a Mixture of Atrazine and Nitrates in Drinking Water and of Active Tobacco Exposure during Pregnancy" International Journal of Environmental Research and Public Health 18, no. 4: 2200. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18042200