
Ascertainment Bias in a Historic Cohort Study of Residents in an Asbestos Manufacturing Community

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Timeframe for Establishing Cohort
2.2. Assembling of the 1930 Ambler Residents Cohort
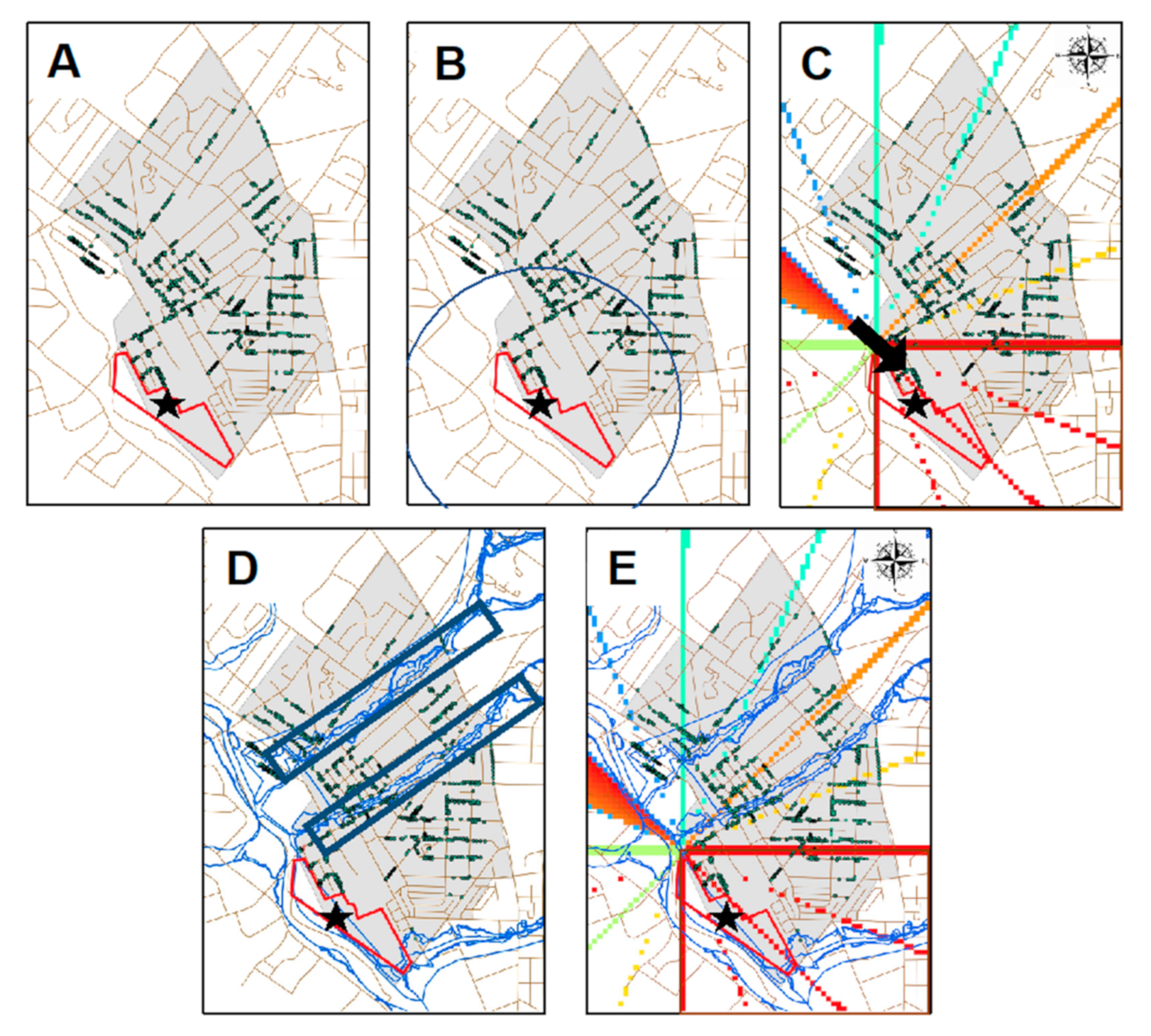
2.3. The Exposure Riskscape
2.4. Identifying Potential Community Asbestos Exposure Pathways
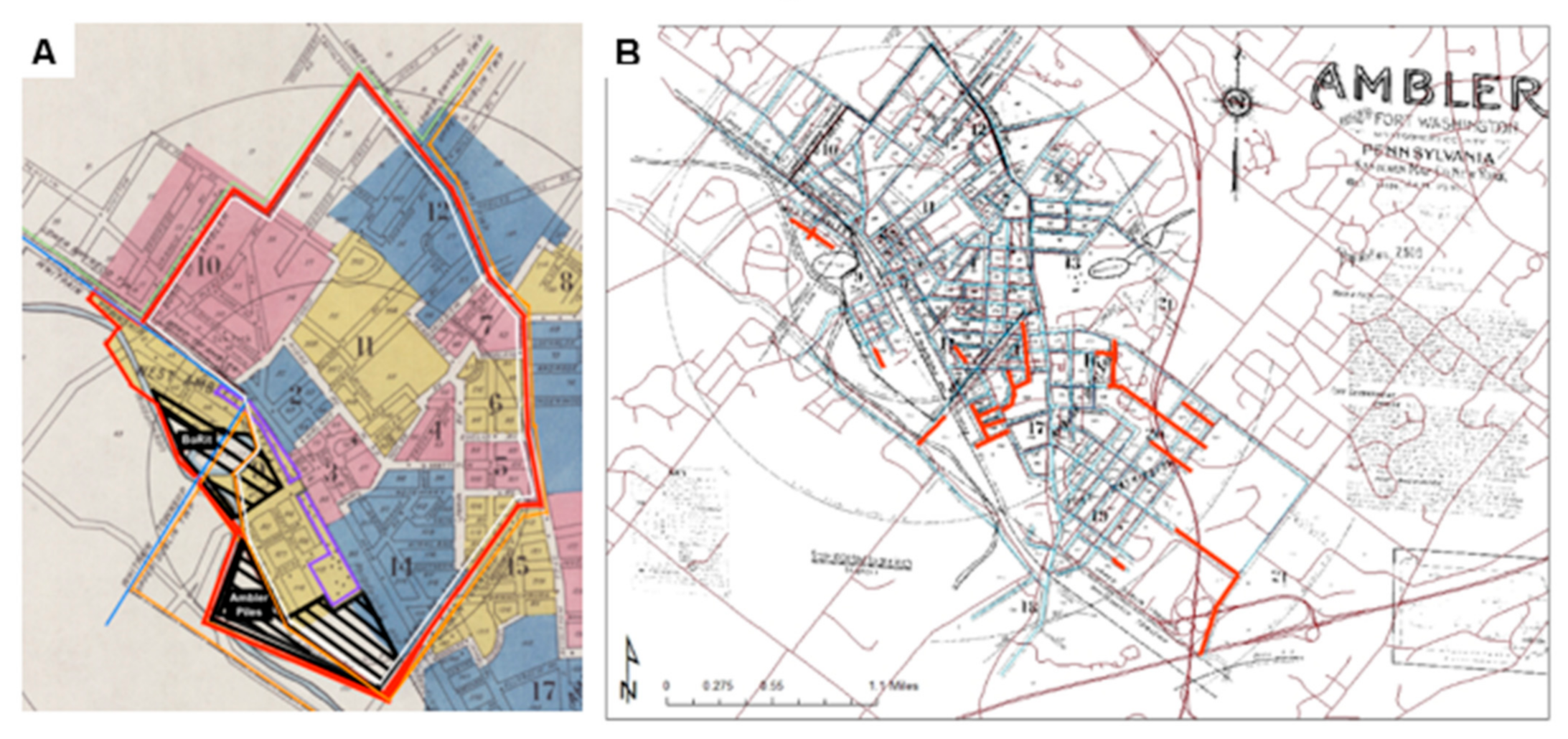
2.5. Reconstructing and Geocoding the Historic Ambler Riskscape
2.6. Classifying Amber Residents’ Exposure Status
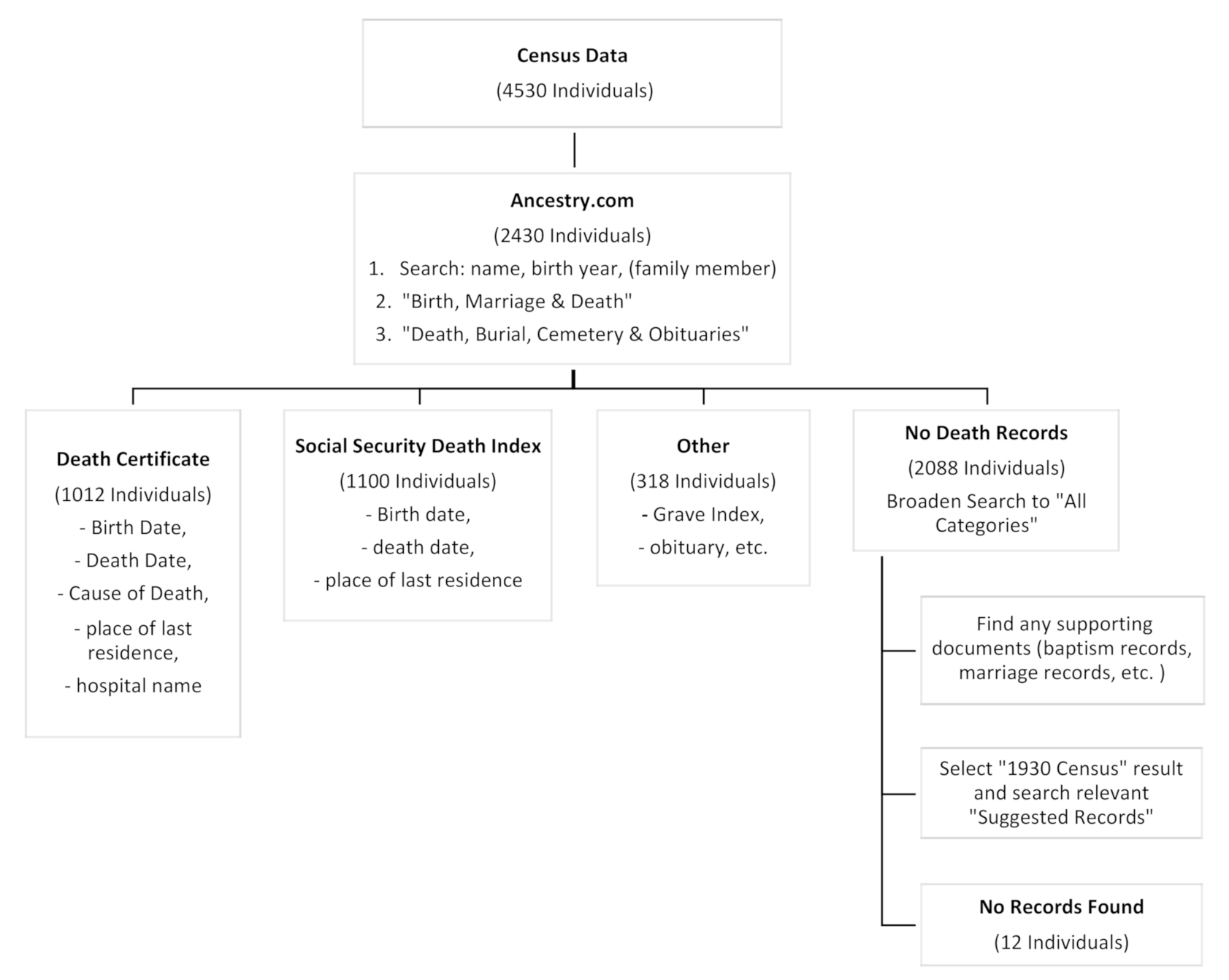
2.7. Determination of Date, Age Location and Cause of Death
3. Results
3.1. Cohort Demographics and Exposure Subgroups
3.2. Characterizing Lifestyle/Behavioral Exposures
- Playing or socializing on asbestos waste piles particularly as a child or adolescent;
- Socialization with asbestos workers (wearing dusty clothing, no hair washing or showering) after work in public venues including bars;
- Picnicking or socializing near asbestos piles as an adult;
- Outdoor sports and gardening
- Using asbestos-containing objects for cooking;
- Flooding into basements with contaminated water from plant or ACM waste sites;
- Eating produce from gardens with contaminated soil.
3.3. Comparison of Present and Historic Maps
3.4. Mortality Data Acquisition within the Cohort
3.5. Ascertainment Bias within the Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Smith, C.D.M. Final Remediation Investigation/Feasibility Study Report for Ambler Piles. Proc. Water Environ. Fed. 1988. [Google Scholar] [CrossRef] [Green Version]
- USEPA. Superfund Record of Decision: Ambler Asbestos; USEPA: Washington, DC, USA, 1988. [Google Scholar]
- Wagner, J.C.; Sleggs, C.A.; Marchand, P. Diffuse Pleural Mesothelioma and Asbestos Exposure in the North Western Cape Province. Occup. Environ. Med. 1960, 17, 260–271. [Google Scholar] [CrossRef] [Green Version]
- Navot, D.; Laufer, N.; Kopolovic, J.; Rabinowitz, R.; Birkenfeld, A.; Lewin, A.; Granat, M.; Margalioth, E.J.; Schenker, J.G. Artificially Induced Endometrial Cycles and Establishment of Pregnancies in the Absence of Ovaries. N. Engl. J. Med. 1986, 314, 806–811. [Google Scholar] [CrossRef]
- Weill, H.; Ziskind, M.M.; Waggenspack, C.; Rossiter, C.E. Lung Function Consequences of Dust Exposure in Asbestos Cement Manufacturing Plants. Arch. Environ. Health Int. J. 1975, 30, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Berry, G.; Wilson, M.R.; Stone, V.; Cullen, R.T.; Searl, A.; Maynard, R.L.; Donaldson, K. Mortality from all cancers of asbestos factory workers in east London 1933–80. Occup. Environ. Med. 2000, 57, 782–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarver, D.; Moak, D. Cancer: Evaluation Community Fact Sheet: Ambler Area, Montgomery County. Pennsylvania Department of Health. 2011. Available online: http://www.boritcag.org/pdf/PADOH_Ambler_Cancer_Evaluation_Final_Ju1%2020%2011.pdf (accessed on 24 February 2021).
- Newhouse, M.L.; Berry, G.; Wagner, J.C.; Turok, M.E. A Study of the mortality of female asbestos workers. Occup. Environ. Med. 1972, 29, 134–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agudo, A.; Escolar, A.; González, C.A.; Bleda, M.J.; Ramírez, J.; Hernández, S.; López, F.; Calleja, A.; Panadès, R.; Turuguet, D.; et al. Occupation and risk of malignant pleural mesothelioma: A case-control study in Spain. Am. J. Ind. Med. 1999, 37, 159–168. [Google Scholar] [CrossRef]
- Pintos, J.; Parent, M.-E.; Case, B.W.; Rousseau, M.-C.; Siemiatycki, J. Risk of Mesothelioma and Occupational Exposure to Asbestos and Man-Made Vitreous Fibers: Evidence From Two Case-Control Studies in Montreal, Canada. J. Occup. Environ. Med. 2009, 51, 1177–1184. [Google Scholar] [CrossRef]
- Ulvestaf, B.; Kjœrheim, K.; Martinsen, J.I. Danish National Research Centre for the Working Environment Finnish Institute of Occupational Health Norwegian National Institute of Occupational Health Cancer incidence among workers in the asbes-tos-cement producing industry in Norway Author (s): Bente. Scand. J. Work Environ. Health 2021, 28, 411–417. [Google Scholar]
- Ribak, J.; Lilis, R.; Suzuki, Y.; Penner, L.; Selikoff, I.J. Malignant mesothelioma in a cohort of asbestos insulation workers: Clinical presentation, diagnosis, and causes of death. Occup. Environ. Med. 1988, 45, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Plant, D.D.; Christian, P.; County, H.; Services, H. Health Consultation BoRit Asbestos Site Ambler; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2012. [Google Scholar]
- Doll, R. Mortality from lung cancer in asbestos workers. Occup. Environ. Med. 1993, 50, 484. [Google Scholar] [CrossRef] [Green Version]
- Kurumatani, N.; Natori, Y.; Mizutani, R.; Kumagai, S.; Haruta, M.; Miura, H.; Yonemasu, K. A Historical Cohort Mortality Study of Workers Exposed to Asbestos in a Refitting Shipyard. Ind. Health 1999, 37, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, P.A. Vermiculite, Respiratory Disease, and Asbestos Exposure in Libby, Montana: Update of a Cohort Mortality Study. Environ. Health Perspect. 2007, 115, 579–585. [Google Scholar] [CrossRef] [Green Version]
- Anderson, H.A.; Lilis, R.; Daum, S.M.; Fischbein, A.S.; Selikoff, I.J. Household-contact asbestos neoplastic risk. Ann. N. Y. Acad. Sci. 1976, 271, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Magnani, C.; Ferrante, D.; Barone-Adesi, F.; Bertolotti, M.; Todesco, A.; Mirabelli, D.; Terracini, B. Cancer risk after cessation of asbestos exposure: A cohort study of Italian asbestos cement workers. Occup. Environ. Med. 2008, 65, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.-L.; Day, H.W.; Wang, W.; Beckett, L.A.; Schenker, M.B. Residential Proximity to Naturally Occurring Asbestos and Mesothelioma Risk in California. Am. J. Respir. Crit. Care Med. 2005, 172, 1019–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnani, C.; Dalmasso, P.; Biggeri, A.; Ivaldi, C.; Mirabelli, D.; Terracini, B. Increased Risk of Malignant Mesothelioma of the Pleura after Residential or Domestic Exposure to Asbestos: A Case-Control Study in Casale Monferrato, Italy. Environ. Health Perspect. 2001, 109, 915–919. [Google Scholar] [CrossRef] [PubMed]
- Erren, T.C.; Jacobsen, M.; Peikarski, C. Synergy between Asbestos and Smoking on Lung Cancer Risk. Epidemiology 1999, 10, 405–411. [Google Scholar] [CrossRef]
- Leigh, J.; Davidson, P.; Hendrie, L.; Berry, D. Malignant mesothelioma in Australia, 1945–2000. Am. J. Ind. Med. 2002, 41, 188–201. [Google Scholar] [CrossRef]
- Moore, A.J.; Parker, R.J.; Wiggins, J. Malignant mesothelioma. Orphanet J. Rare Dis. 2008, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- De Klerk, N.H.; Armstrong, B.K.; Musk, A.W.; Hobbs, M.S. Cancer mortality in relation to measures of occupational exposure to crocidolite at Wittenoom Gorge in Western Australia. Occup. Environ. Med. 1989, 46, 529–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goswami, E.; Craven, V.; Dahlstrom, D.L.; Alexander, D.; Mowat, F. Domestic Asbestos Exposure: A Review of Epidemiologic and Exposure Data. Int. J. Environ. Res. Public Health 2013, 10, 5629–5670. [Google Scholar] [CrossRef] [Green Version]
- Newhouse, M.L.; Thompson, H. Mesothelioma of pleura and peritoneum following exposure to asbestos in the London area. Occup. Environ. Med. 1965, 22, 261–269. [Google Scholar] [CrossRef]
- Noonan, C.W.; Conway, K.; Landguth, E.L.; McNew, T.; Linker, L.; Pfau, J.; Black, B.; Szeinuk, J.; Flores, R. Multiple pathway asbestos exposure assessment for a Superfund community. J. Expo. Sci. Environ. Epidemiol. 2014, 25, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Raffn, E.; Lynge, E.; Juel, K.; Korsgaard, B. Incidence of cancer and mortality among employees in the asbestos cement industry in Denmark. Occup. Environ. Med. 1989, 46, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selikoff, I.J.; Hammond, E.C.; Seidman, H. Mortality Experience of Insulation Workers in the United States and Canada, 1943–1976. Ann. N. Y. Acad. Sci. 1979, 330, 91–116. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.-V.; Chowdhury, N.; Kandl, C.; Hoover, C.; Robinson, A.; Hoover, L.; Ba, C.H.; And, A.R.; Facs, L.H. Genealogical databases as a tool for extending follow-up in clinical reviews. Int. Forum Allergy Rhinol. 2016, 6, 880–882. [Google Scholar] [CrossRef] [PubMed]
- Emmett, E.A.; Cakouros, B. Communities at High Risk in the Third Wave of Mesothelioma. Mol. Determ. Head Neck Cancer 2017, 2017, 103–130. [Google Scholar] [CrossRef]
- Reid, A.; Heyworth, J.; De Klerk, N.; Musk, A.W. The mortality of women exposed environmentally and domestically to blue asbestos at Wittenoom, Western Australia. Occup. Environ. Med. 2008, 65, 743–749. [Google Scholar] [CrossRef]
- Virta, R.L. Worldwide Asbestos Supply and Consumption Trends from 1900 through 2003; U.S. Geological Survey: Reston, VA, USA, 2006. [Google Scholar]
- York, A.M.; Tuccillo, J.; Boone, C.G.; Bolin, B.; Gentile, L.; Schoon, B.; Kane, K. Zoning and Land Use: A Tale of Incompatibility and Environmental Injustice in Early Phoenix. J. Urban Aff. 2014, 36, 833–853. [Google Scholar] [CrossRef]
- Clapp, J.T.; Roberts, J.A.; Dahlberg, B.; Berry, L.S.; Jacobs, L.M.; Emmett, E.A.; Barg, F.K. Realities of environmental toxicity and their ramifications for community engagement. Soc. Sci. Med. 2016, 170, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ESRI. ArcGIS Desktop: Release 10; ESRI: Redlands, CA, USA, 2011. [Google Scholar]
- Maule, M.M.; Magnani, C.; Dalmasso, P.; Mirabelli, D.; Merletti, F.; Biggeri, A. Modeling Mesothelioma Risk Associated with Environmental Asbestos Exposure. Environ. Heal. Perspect. 2007, 115, 1066–1071. [Google Scholar] [CrossRef]
- Mensi, C.; Riboldi, L.; De Matteis, S.; Bertazzi, P.A.; Consonni, D. Impact of an asbestos cement factory on mesothelioma incidence: Global assessment of effects of occupational, familial, and environmental exposure. Environ. Int. 2015, 74, 191–199. [Google Scholar] [CrossRef] [Green Version]
- Kurumatani, N.; Kumagai, S. Mapping the Risk of Mesothelioma Due to Neighborhood Asbestos Exposure. Am. J. Respir. Crit. Care Med. 2008, 178, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Sauder, R.A. The use of Sanborn maps in reconstructing “geographies of the past”; Boston’s waterfront from 1867 to 1972. J. Geogr. 1980, 79, 204–213. [Google Scholar] [CrossRef]
- Reid, A.; De Klerk, N.H.; Magnani, C.; Ferrante, D.; Berry, G.; Musk, A.W.; Merler, E. Mesothelioma risk after 40 years since first exposure to asbestos: A pooled analysis. Thorax 2014, 69, 843–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database Title | Location | Dates | Data | Source |
|---|---|---|---|---|
| PA, Death Certificates | PA | 1906–1963 Note: 1925 is missing from the archive |
| Pennsylvania Department of Health |
| U.S. Social Security Death Index | U.S. | 1935–2011 Note: Social Security number is not available for those who passed within the past 10 years. |
| Social Security Administration, Social Security Death Index, Master File, Social Security Administration |
| U.S. Find A Grave Index | U.S. | 1600s–Current |
| All data is uploaded by Find-A-Grave volunteers to http://www.findagrave.com |
| 2A | (n) | Entire Cohort (n = 4530) | (n) | Occupational Exp. (n = 474) | sig | (n) | Para-occupational Exp. (n = 1638) | sig | (n) | No Occupational or Paraoccupational Exp (n = 2619) | sig | (n) | Occupational & Paraoccupational Exp. (n = 201) | sig | |
| Avg Age in 1930 +/− sd | 4530 | 29.65 +/− 20.29 | 474 | 38.5 +/− 14.5 | ** | 1638 | 24.6 +/− 18.8 | ** | 2619 | 31.7 +/− 21.0 | ** | 201 | 35.5 +/− 14.9 | ** | |
| Avg Dist (ft) from Waste Piles +/− sd | 4530 | 1852.5 +/− 1159.7 | 474 | 1574 +/− 1124.6 | ** | 1638 | 1560 +/− 1124.6 | ** | 2619 | 2183.6 +/− 1067.6 | ** | 201 | 1490.0 +/− 1061.1 | ** | |
| Race | % black | 560 | 12.39 | 88 | 18.57 | ** | 321 | 19.6 | ** | 205 | 35.8 | ** | 42 | 20.9 | ** |
| % white | 3958 | 87.61 | 386 | 81.43 | 1317 | 80.4 | 2414 | 61 | 159 | 79.1 | |||||
| % other | |||||||||||||||
| total | 4518 | 100 | 474 | 100 | 1638 | 100 | 2619 | 100 | 201 | 100 | |||||
| Sex | % male | 2232 | 49.38 | 419 | 88.4 | ** | 768 | 46.89 | ** | 1268 | 55.4 | * | 167 | 83.1 | ** |
| % female | 2288 | 50.62 | 55 | 11.6 | 870 | 53.11 | 1341 | 60.1 | 34 | 16.92 | |||||
| total | 4520 | 100 | 419 | 100 | 1638 | 100 | 2609 | 100 | 201 | 100 | |||||
| Img. Stat. | % 1st Gen | 712 | 15.74 | 195 | 41.14 | ** | 314 | 19.17 | ** | 282 | 39.6 | ** | 79 | 39.3 | ** |
| % 2nd Gen | 857 | 18.94 | 37 | 7.81 | 446 | 27.23 | 393 | 45.9 | 19 | 9.45 | |||||
| % Non-Immigrant | 2955 | 65.32 | 242 | 51.05 | 878 | 53.6 | 1939 | 65.6 | 103 | 51.2 | |||||
| 2B | (n) | Proximity Exposure | sig | (n) | Wind Exposure (n = 2003) | sig | (n) | Proximity and Wind Exposure (n = 62) | sig | (n) | Flood Exposure (n = 231) | sig | |||
| (n = 1365) | |||||||||||||||
| Avg Age in 1930 +/− sd | 1365 | 30.0 +/− 20.8 | * | 2003 | 24.9 +/− 18.3 | ** | 62 | 29.8 +/− 18.8 | 231 | 25.3 +/− 18.5 | * | ||||
| Avg Dist (ft)from Waste Piles +/− sd | 1365 | 1232.4 +/− 619.6 | ** | 2003 | 534.3 +/− 563.3 | ** | 62 | 983.1 +/− 673 | ** | 231 | 1836.7 +/− 662.9 | ||||
| Race | % black | 68 | 4.9 | ** | 216 | 28.6 | ** | 8 | 5.41 | * | 17 | 7.4 | ** | ||
| % white | 1296 | 94.9 | 540 | 71.4 | 140 | 94.6 | 213 | 92.2 | |||||||
| % other | 1 | 0.073 | |||||||||||||
| total | 1365 | 99.873 | 756 | 100 | 61 | 100 | 230 | 99.6 | |||||||
| Sex | % male | 669 | 49 | 408 | 54 | * | 74 | 50 | 123 | 53.2 | |||||
| % female | 696 | 51 | 348 | 46 | 74 | 50 | 108 | 46.8 | |||||||
| total | 1365 | 100 | 756 | 100 | 62 | 100 | 231 | 100 | |||||||
| Img. Stat. | % 1st Gen | 241 | 17.7 | ** | 154 | 20.4 | ** | 24 | 16.2 | 64 | 27.7 | ** | |||
| % 2nd Gen | 291 | 21.3 | 213 | 28.2 | 37 | 25 | 82 | 35.5 | |||||||
| % Non-Immigrant | 833 | 61 | 389 | 51.5 | 87 | 58.8 | 85 | 36.8 | |||||||
| 2C | (n) | Occupational & Proximity Exp. (n = 38) | sig | (n) | Occupational & Wind Exposure (n = 119) | sig | (n) | Paraoccupational & Proximity Exposure (n = 132) | sig | (n) | Paraoccupational & Wind Exposure (n = 466) | sig | |||
| Avg Age +/− sd | 38 | 36.1 +/− 13.7 | * | 119 | 35.9 +/− 12.2 | ** | 132 | 28.7 +/− 18.2 | 466 | 20.9 +/− 16.8 | ** | ||||
| Avg Dist (ft)from Waste Piles +/− sd | 38 | 3675.628 +/− 285.4 | ** | 119 | 358.6 +/− 366.2 | ** | 132 | 3906.7 +/− 1081.5 | ** | 466 | 347.4 +/− 328.7 | ** | |||
| Race | % black | 24 | 63.2 | ** | 36 | 30.25 | ** | 86 | 65.2 | ** | 148 | 31.8 | ** | ||
| % white | 14 | 36.8 | 83 | 69.75 | 46 | 34.9 | 318 | 68.2 | |||||||
| % other | |||||||||||||||
| total | 38 | 100 | 119 | 100 | 132 | 100 | 466 | 100 | |||||||
| Sex | % male | 35 | 92.1 | ** | 108 | 90.8 | ** | 59 | 44.7 | 231 | 49.6 | ||||
| % female | 3 | 7.9 | 11 | 9.24 | 73 | 55.3 | 235 | 50.43 | |||||||
| total | 38 | 100 | 119 | 100 | 132 | 100 | 466 | 100 | |||||||
| Img. Stat. | % 1st Gen | 2 | 5.26 | * | 63 | 52.9 | ** | 6 | 4.55 | ** | 94 | 20.2 | ** | ||
| % 2nd Gen | 0 | 0 | 10 | 8.4 | 3 | 2.27 | 168 | 36.1 | |||||||
| % Non-Immigrant | 36 | 94.7 | 46 | 38.7 | 123 | 93.2 | 204 | 43.8 | |||||||
| Frequency (%) | ||
|---|---|---|
| Death Data Source | Death Certificate | 1014 (22.4) |
| Social Security Death Index | 1046 (23.1) | |
| US Find-a-Grave Index | 189 (4.2) | |
| Other | 132 (2.9) | |
| No data found * | 2139 (47.3) | |
| Death Certificate Source ** | Pennsylvania | 992 (97.8) |
| Philadelphia | 13 (1.3) | |
| North Carolina | 2 (0.2) | |
| Texas | 2 (0.2) | |
| Vermont | 1 (0.1) | |
| Ohio | 1 (0.1) | |
| Florida | 3 (0.3) | |
| Location of Death (if known) | Pennsylvania | 1005 (83.2) |
| Outside of Pennsylvania | 177 (16.8) | |
| Ambler ⍭ | 413 (41.1) | |
| Outside of Ambler ⍭ | 447 (44.5) | |
| Not Indicated ⍭ | 145 (14.4) |
| YOD Present (n = 2452) N (%) 1 | YOD Absent (n = 2078) N (%) 1 | OR (95% CI) 2 | p-Value | COD Present (n = 567) N (%) 1 | COD Absent (n = 3963) N (%) 1 | OR (95% CI) 2 | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Occupational Exposure | 260 (54.9) | 214 (45.2) | 1.02 (0.85, 1.24) | 0.78 | 65 (13.7) | 409 (86.3) | 1.12 (0.85, 1.48) | 0.42 |
| Para- occupational Exposure | 754 (46.0) | 884 (54.0) | 0.59 (0.53, 0.67) | <0.0001 ** | 115 (7.0) | 1523 (93.0) | 0.41 (0.33, 0.50) | <0.0001 ** |
| Proximity Exposed | 337 (58.7) | 237 (41.3) | 1.25 (1.04, 1.49) | 0.014 * | 122 (21.3) | 452 (78.8) | 2.37 (1.89, 2.97) | <0.0001 ** |
| Wind Exposed | 340 (45.0) | 416 (55.0) | 0.64 (0.55, 0.75) | <0.0001 ** | 25 (3.32) | 731 (96.7) | 0.20 (0.14, 0.31) | <0.0001 ** |
| Black | 250 (43.71) | 322 (56.29) | 0.62 (0.52, 0.74) | <0.0001 ** | 35 (6.12) | 537 (93.88) | 0.42 (0.29, 0.60) | <0.0001 ** |
| Female | 1035 (46.37) | 1197 (53.63) | 0.53 (0.47, 0.60) | <0.0001 ** | 262 (11.74) | 1970 (88.26) | 0.86 (0.72, 1.03) | 0.106 |
| 1st Gen Immigrant | 343 (48.17) | 369 (51.83) | 0.67 (0.57, 0.79) | 0.001 * | 76 (10.67) | 636 (89.33) | 0.71 (0.55, 0.92) | 0.009 * |
| 2nd Gen Immigrant | 388 (45.27) | 469 (54.73) | 0.59 (0.51, 0.69) | <0.0001 ** | 65 (7.58) | 792 (92.42) | 0.49 (0.37, 0.64) | <0.0001 ** |
| Young (≤19 y) | 679 (42.41) | 922 (57.59) | 0.31 (0.25, 0.39) | <0.0001 ** | 30 (1.87) | 1571 (98.13) | 0.028 (0.019, 0.042) | <0.0001 ** |
| Middle-Age (20–59 y) | 1445 (59.83) | 970 (40.17) | 0.63 (0.51, 0.79) | <0.0001 ** | 363 (15.03) | 2052 (84.97) | 0.26 (0.21, 0.32) | <0.0001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wortzel, J.D.; Wiebe, D.J.; Elahi, S.; Agawu, A.; Barg, F.K.; Emmett, E.A. Ascertainment Bias in a Historic Cohort Study of Residents in an Asbestos Manufacturing Community. Int. J. Environ. Res. Public Health 2021, 18, 2211. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052211
Wortzel JD, Wiebe DJ, Elahi S, Agawu A, Barg FK, Emmett EA. Ascertainment Bias in a Historic Cohort Study of Residents in an Asbestos Manufacturing Community. International Journal of Environmental Research and Public Health. 2021; 18(5):2211. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052211
Chicago/Turabian StyleWortzel, Jeremy D., Douglas J. Wiebe, Shabnam Elahi, Atu Agawu, Frances K. Barg, and Edward A. Emmett. 2021. "Ascertainment Bias in a Historic Cohort Study of Residents in an Asbestos Manufacturing Community" International Journal of Environmental Research and Public Health 18, no. 5: 2211. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052211