
Responsiveness and Minimal Clinically Important Difference of the Five Times Sit-to-Stand Test in Patients with Stroke

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
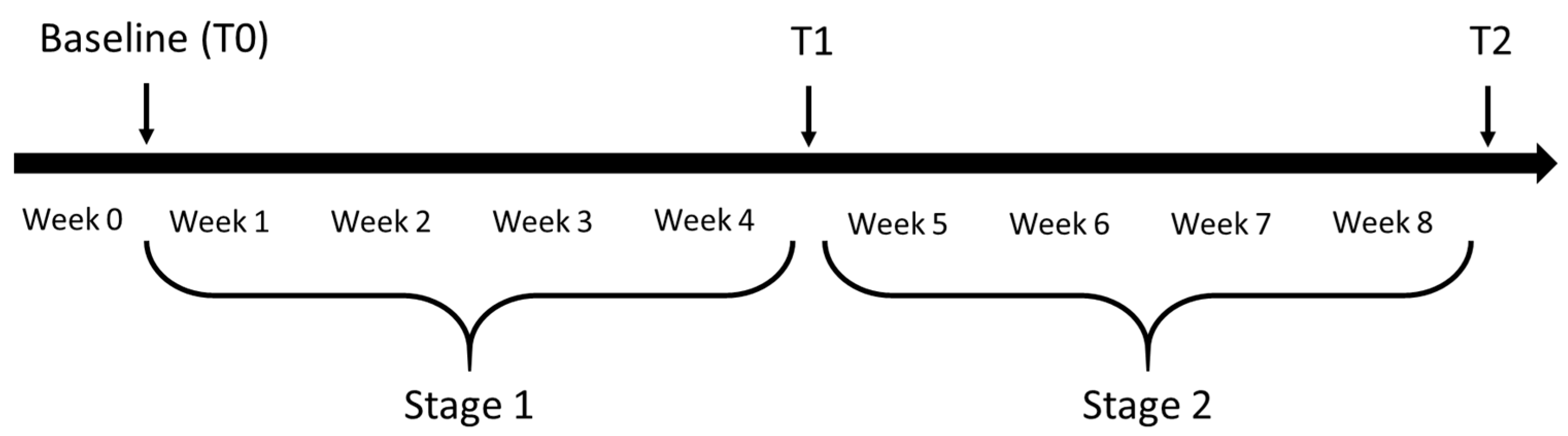
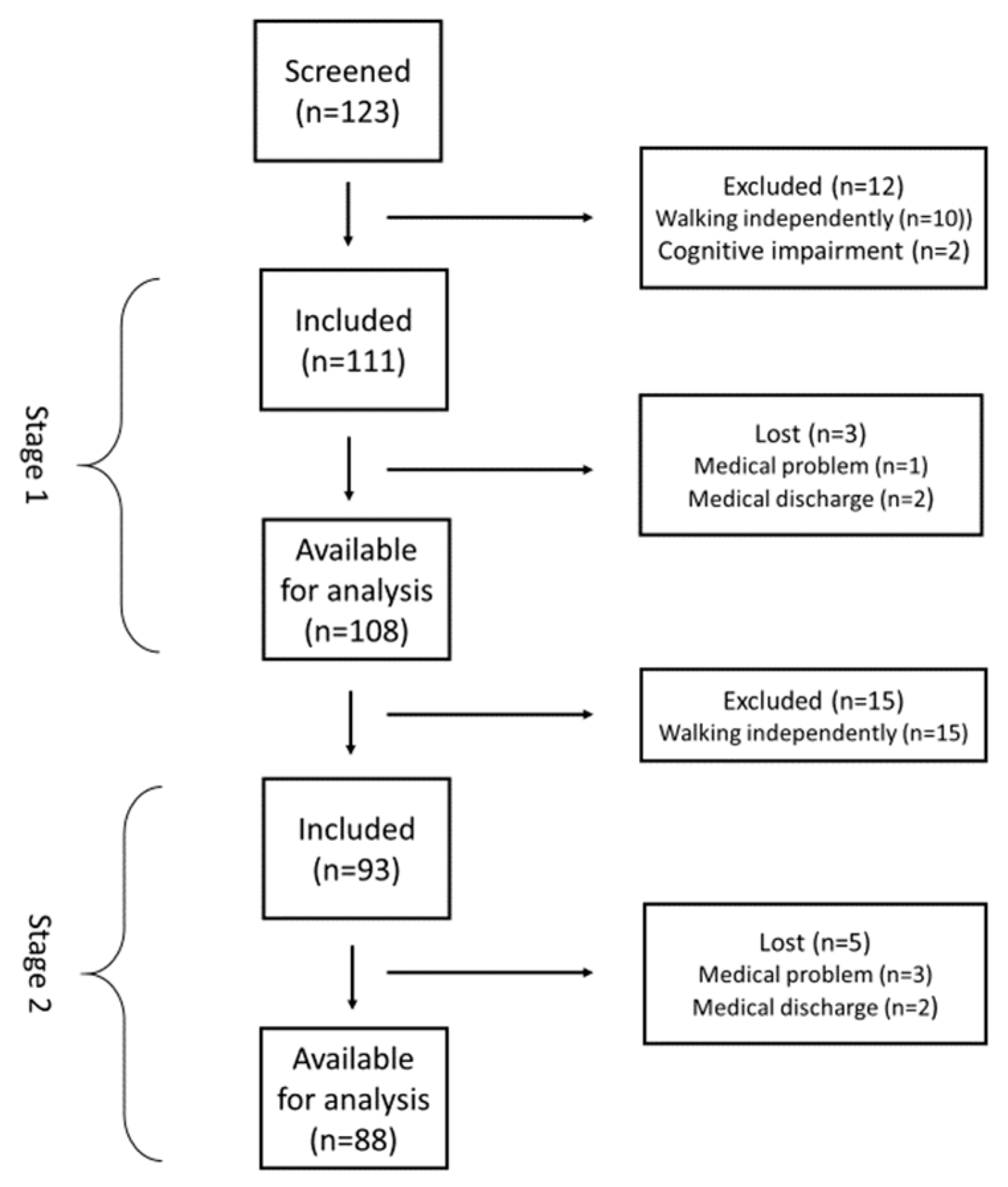
2.1. Study Design and Participants
2.2. Intervention
2.3. Measures
2.3.1. The 5STS and Gait Speed
2.3.2. Global Rating of Change
2.3.3. Comparator Instruments for Responsiveness
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Minimal Clinically Important Difference
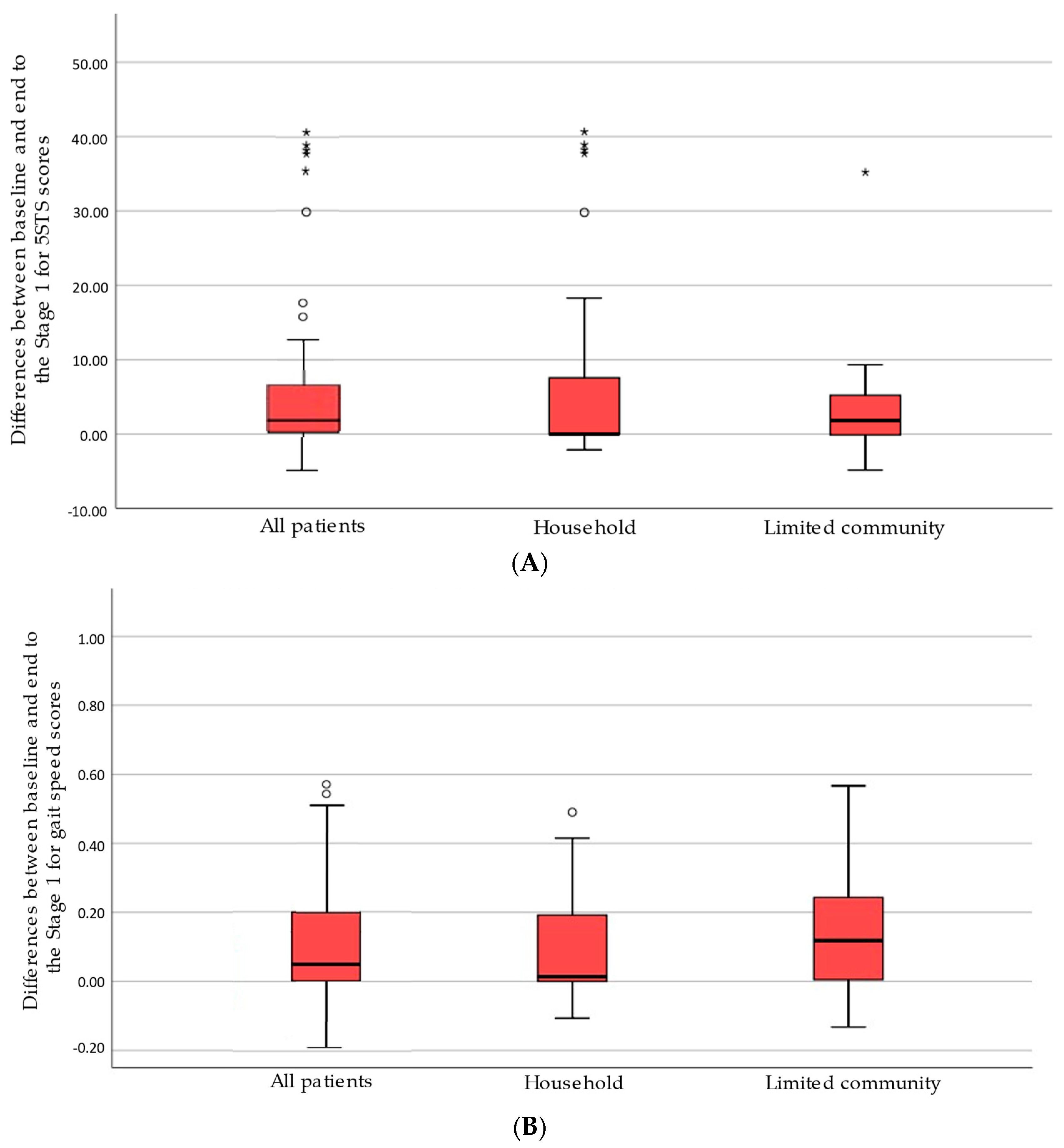
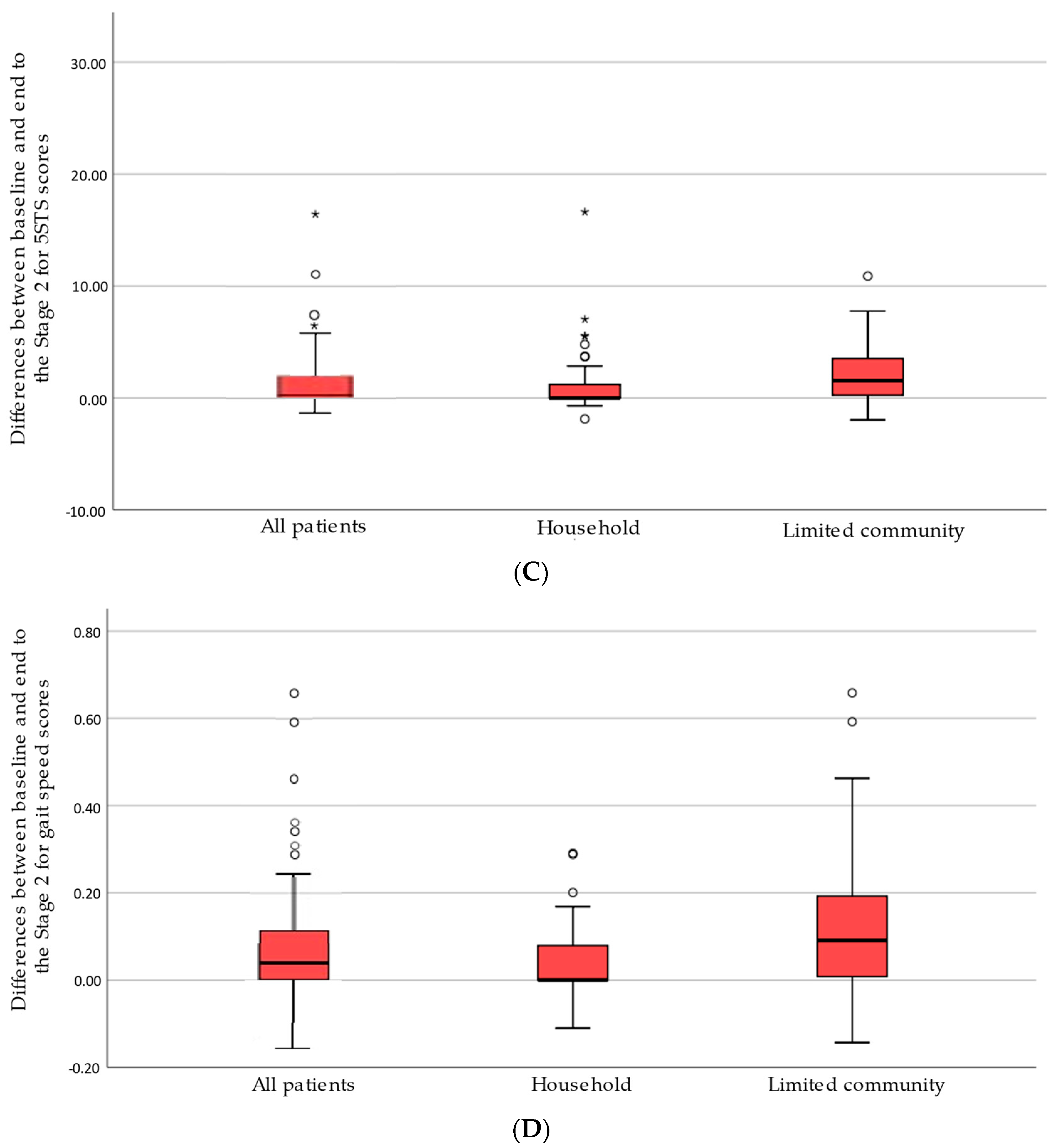
3.3. Responsiveness
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Silva, P.F.; Quintino, L.F.; Franco, J.; Faria, C.D. Measurement Properties and Feasibility of Clinical Tests to Assess Sit-to-Stand/Stand-to-Sit Tasks in Subjects with Neurological Disease: A Systematic Review. Braz. J. Phys. Ther. 2014, 18, 99–110. [Google Scholar] [CrossRef] [Green Version]
- Pua, Y.H.; Thumboo, J.; Clark, R.A. Correspondence: Time-Based versus Repetition-Based Sit-to-Stand Measures: Choice of Metrics Matters. J. Physiother. 2018, 64, 200–201. [Google Scholar] [CrossRef]
- Mentiplay, B.F.; Clark, R.A.; Bower, K.J.; Williams, G.; Pua, Y.H. Five Times Sit-to-Stand Following Stroke: Relationship with Strength and Balance. Gait Posture 2020, 78, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Tsang, Y.L.; Mak, M.K. Sit-and-Reach Test Can Predict Mobility of Patients Recovering from Acute Stroke. Arch. Phys. Med. Rehabil. 2004, 85, 94–98. [Google Scholar] [CrossRef]
- Mong, Y.; Teo, T.W.; Ng, S.S. 5-Repetition Sit-to-Stand Test in Subjects With Chronic Stroke: Reliability and Validity. Arch. Phys. Med. Rehabil. 2010, 91, 407–413. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Knol, D.L.; Stratford, P.W.; Alonso, J.; Patrick, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN Checklist for Evaluating the Methodological Quality of Studies on Measurement Properties: A Clarification of Its Content. BMC Med. Res. Methodol. 2010, 10, 22. [Google Scholar] [CrossRef] [Green Version]
- Stratford, P.W.; Binkley, J.M.; Riddle, D.L.; Guyatt, G.H. Sensitivity to Change of the Roland-Morris Back Pain Questionnaire: Part 1. Phys. Ther. 1998, 78, 1186–1196. [Google Scholar] [CrossRef]
- Revicki, D.; Hays, R.D.; Cella, D.; Sloan, J. Recommended Methods for Determining Responsiveness and Minimally Important Differences for Patient-Reported Outcomes. J. Clin. Epidemiol. 2008, 61, 102–109. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Andrews, A.W.; Glenney, S.S. Minimal Clinically Important Difference for Comfortable Speed as a Measure of Gait Performance in Patients Undergoing Inpatient Rehabilitation after Stroke. J. Phys. Ther. Sci. 2013, 25, 1223–1225. [Google Scholar] [CrossRef] [Green Version]
- Ostelo, R.W.; de Vet, H.C. Clinically Important Outcomes in Low Back Pain. Best Pract. Res. Clin. Rheumatol. 2005, 19, 593–607. [Google Scholar] [CrossRef] [PubMed]
- Copay, A.G.; Subach, B.R.; Glassman, S.D.; Polly, D.W.; Schuler, T.C. Understanding the Minimum Clinically Important Difference: A Review of Concepts and Methods. Spine J. 2007, 7, 541–546. [Google Scholar] [CrossRef]
- Tilson, J.K.; Sullivan, K.J.; Cen, S.Y.; Rose, D.K.; Koradia, C.H.; Azen, S.P.; Duncan, P.W. Locomotor Experience Applied Post Stroke (LEAPS) Investigative Team Meaningful Gait Speed Improvement during the First 60 Days Poststroke: Minimal Clinically Important Difference. Phys. Ther. 2010, 90, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.E.; Edwards, D.F.; Birkenmeier, R.L.; Dromerick, A.W. Estimating Minimal Clinically Important Differences of Upper-Extremity Measures Early after Stroke. Arch. Phys. Med. Rehabil. 2008, 89, 1693–1700. [Google Scholar] [CrossRef] [Green Version]
- Fulk, G.D.; Ludwig, M.; Dunning, K.; Golden, S.; Boyne, P.; West, T. Estimating Clinically Important Change in Gait Speed in People with Stroke Undergoing Outpatient Rehabilitation. J. Neurol. Phys. Ther. 2011, 35, 82–89. [Google Scholar] [CrossRef]
- Perry, J.; Garrett, M.; Gronley, J.K.; Mulroy, S.J. Classification of Walking Handicap in the Stroke Population. Stroke 1995, 26, 982–989. [Google Scholar] [CrossRef]
- Bernabeu-Mora, R.; Giménez-Giménez, L.M.; Montilla-Herrador, J.; García-Guillamón, G.; García-Vidal, J.A.; Medina-Mirapeix, F. Determinants of Each Domain of the Short Physical Performance Battery in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2539–2544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, S.E.; Kon, S.S.; Canavan, J.L.; Patel, M.S.; Clark, A.L.; Nolan, C.M.; Polkey, M.I.; Man, W.D. The Five-Repetition Sit-to-Stand Test as a Functional Outcome Measure in COPD. Thorax 2013, 68, 1015–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- van Bloemendaal, M.; van de Water, A.T.; van de Port, I.G. Walking Tests for Stroke Survivors: A Systematic Review of Their Measurement Properties. Disabil. Rehabil. 2012, 34, 2207–2221. [Google Scholar] [CrossRef]
- Scrivener, K.; Schurr, K.; Sherrington, C. Responsiveness of the Ten-Metre Walk Test, Step Test and Motor Assessment Scale in Inpatient Care after Stroke. BMC Neurol. 2014, 14, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehrholz, J.; Wagner, K.; Rutte, K.; Meissner, D.; Pohl, M. Predictive Validity and Responsiveness of the Functional Ambulation Category in Hemiparetic Patients after Stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1314–1319. [Google Scholar] [CrossRef]
- Ratner, B. The Correlation Coefficient: Its Values Range between +1/−1, or Do They? J. Target. Meas. Anal. Mark. 2009, 17, 139–142. [Google Scholar] [CrossRef] [Green Version]
- Husted, J.A.; Cook, R.J.; Farewell, V.T.; Gladman, D.D. Methods for Assessing Responsiveness: A Critical Review and Recommendations. J. Clin. Epidemiol. 2000, 53, 459–468. [Google Scholar] [CrossRef]
- Martín-San Agustín, R.; Medina-Mirapeix, F.; Casaña-Granell, J.; García-Vidal, J.A.; Lillo-Navarro, C.; Benítez-Martínez, J.C. Tensiomyographical Responsiveness to Peripheral Fatigue in Quadriceps Femoris. PeerJ 2020, 8, e8674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fini, N.A.; Bernhardt, J.; Holland, A.E. Low Gait Speed Is Associated with Low Physical Activity and High Sedentary Time Following Stroke. Disabil. Rehabil. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bijleveld-Uitman, M.; van de Port, I.; Kwakkel, G. Is Gait Speed or Walking Distance a Better Predictor for Community Walking after Stroke? J. Rehabil. Med. 2013, 45, 535–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meretta, B.M.; Whitney, S.L.; Marchetti, G.F.; Sparto, P.J.; Muirhead, R.J. The Five Times Sit to Stand Test: Responsiveness to Change and Concurrent Validity in Adults Undergoing Vestibular Rehabilitation. J. Vestib. Res. 2006, 16, 233–243. [Google Scholar] [PubMed]
- van de Port, I.G.; Kwakkel, G.; Lindeman, E. Community Ambulation in Patients with Chronic Stroke: How Is It Related to Gait Speed? J. Rehabil. Med. 2008, 40, 23–27. [Google Scholar] [CrossRef] [Green Version]
- Lewek, M.D.; Sykes, R. Minimal Detectable Change for Gait Speed Depends on Baseline Speed in Individuals with Chronic Stroke. J. Neurol. Phys. Ther 2019, 43, 122–127. [Google Scholar] [CrossRef]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful Change and Responsiveness in Common Physical Performance Measures in Older Adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 111) | Walking Category | |||
|---|---|---|---|---|
| Household (n = 76) | Limited Community (n = 31) | Subgroup Differences p Value | ||
| Age. years; mean (SD) | 68.3 (12.1) | 70.6 (11.1) | 63.9 (13.3) | 0.02 |
| Gender (male) | 60 (54%) | 39 (35%) | 18 (16%) | 0.61 |
| Side affected (right) | 59 (53%) | 37 (33%) | 19 (17%) | 0.29 |
| Type of stroke (ischemic) | 91 (82%) | 62 (56%) | 26 (23%) | 0.90 |
| Time from stroke to admission to outpatient PT. days; mean (SD) | 51.8 (31.5) | 53.8 (31.9) | 50.3 (31.2) | 0.87 |
| FAC. score 0–5; median (IQR) | 2 (2) | 1 (3) | 4 (1) | 0.01 |
| Patients unable to do 5STS/4MGS | 44/44 | 42/44 | 2/0 | - |
| 5STS. s; median (IQR) | 29.75 (43.80) | 60 (35.80) | 15.96 (6.39) | 0.01 |
| Gait speed. m/s; median (IQR) | 0.27 (0.43) | 0 (0.27) | 0.59 (0.26) | 0.01 |
| Baseline | ||
|---|---|---|
| At Stage 1 n1 = 108; n2 = 66; n3 = 42 | At Stage 2 n1 = 88; n2 = 62; n3 = 26 | |
| 5STS (s) | ||
| All patients (n1) | 29.97 (43.68) | 23.5 (44.53) |
| Household (n2) | 60 (34.1) | 60 (38.37) |
| Limited community (n3) | 15.96 (6.39) | 16.4 (8.87) |
| Gait speed (m/s) | ||
| All patients (n1) | 0.27 (0.45) | 0.37 (0.49) |
| Household (n2) | 0 (0.26) | 0.15 (0.27) |
| Limited community (n3) | 0.59 (0.26) | 0.52 (0.17) |
| Stage1 | Stage 2 | |||||
|---|---|---|---|---|---|---|
| ROC Method | Within Patients | ROC Method | Within Patients | |||
| AUC | MCIDs (Associated ORs a) | MCIDs (Associated ORs a) | AUC | MCIDs (Associated ORs a) | MCIDs (Associated ORs a) | |
| 5STS (s) | ||||||
| All patients | 0.71 | 1.18 † (2.44 *) | 2.81 (1.64 *) | 0.73 | 0.76 † (3.87 *) | 2.02 (3.31 *) |
| Household | 0.72 | 1.90 † (4.13 *) | 5.1 (2.46 *) | 0.76 | 0.72 † (6.67 *) | 1.94 (5.67 *) |
| Limited community | 0.70 | 2.92 † (0.70 *) | 1.61 (0.68 *) | 0.70 | 3.09 † (4.96 *) | 2.09 (1.07 *) |
| Gait speed (m/s) | ||||||
| All patients | 0.71 | 0.19 † (3.71 *) | 0.11 (2.67 *) | 0.71 | 0.09 † (2.88 *) | 0.09 (2.88 *) |
| Household | 0.74 | 0.19 † (6.19 *) | 0.10 (3.71 *) | 0.70 | 0.04 † (8.17 *) | 0.07 (2.76 *) |
| Limited community | 0.70 | 0.21 † (1.83 *) | 0.17 (1.43 *) | 0.73 | 0.11 † (3.71 *) | 0.12 (2.63 *) |
| Stage 1 | Stage 2 | |||
|---|---|---|---|---|
| Spearman’s Rho | AUC | Spearman’s Rho | AUC | |
| FAC | ||||
| All patients | 0.307 * | 0.68 | 0.357 * | 0.71 |
| Household | 0.332 * | 0.68 | 0.308 * | 0.66 |
| Limited community | 0.302 * | 0.67 | 0.448 * | 0.76 |
| Gait speed (m/s) | ||||
| All patients | 0.492 * | 0.73 | 0.376 * | 0.72 |
| Household | 0.566 * | 0.75 | 0.431 * | 0.74 |
| Limited community | 0.396 * | 0.71 | 0.301 * | 0.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agustín, R.M.-S.; Crisostomo, M.J.; Sánchez-Martínez, M.P.; Medina-Mirapeix, F. Responsiveness and Minimal Clinically Important Difference of the Five Times Sit-to-Stand Test in Patients with Stroke. Int. J. Environ. Res. Public Health 2021, 18, 2314. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052314
Agustín RM-S, Crisostomo MJ, Sánchez-Martínez MP, Medina-Mirapeix F. Responsiveness and Minimal Clinically Important Difference of the Five Times Sit-to-Stand Test in Patients with Stroke. International Journal of Environmental Research and Public Health. 2021; 18(5):2314. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052314
Chicago/Turabian StyleAgustín, Rodrigo Martín-San, Mª José Crisostomo, Mª Piedad Sánchez-Martínez, and Francesc Medina-Mirapeix. 2021. "Responsiveness and Minimal Clinically Important Difference of the Five Times Sit-to-Stand Test in Patients with Stroke" International Journal of Environmental Research and Public Health 18, no. 5: 2314. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052314