
Understanding the Effect of Electronic Prehospital Medical Records in Ambulances: A Qualitative Observational Study in a Prehospital Setting


 , and
, and 
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Data Collection
2.5. Analysis
3. Results
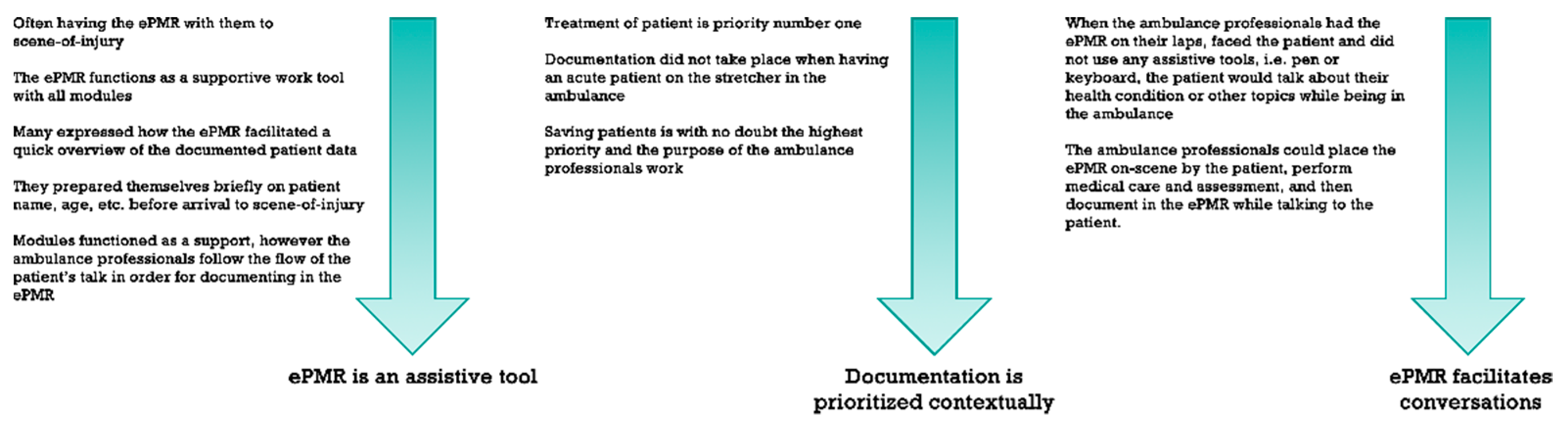
3.1. Ambulance Professionals’ Interaction with ePMR
“Whenever I have handed over a patient, I always go through the ePMR, like a checklist, to see if I forgot to type/document anything (in the ePMR)”.
“It is much easier to deliver an emergency patient than it was before we had the ePMR. It (ePMR) is a good tool as we now collaborate more actively”.
“Back in the days, we experienced that they (the doctors and nurses) threw out the paper records when we came to deliver the patient at the hospital… Now we collaborate—through the ePMR”.
“In specific situations, you want to communicate messages to the ED in a discrete way. For instance, if the patient is covered with feces”.
“It becomes very clear that when the ePMR is not working I use a lot of time documenting (in the paper medical record) and I actually realize that the ePMR is very helpful in my daily work… It is timesaving when it’s (ePMR) working”.
3.2. Documentation as Secondary Priority
“It is of great value to be able to call the ED when having a very acute patient—then you are assured that the professionals in the ED gathers the right team within the hospital before we arrive. It is a lot faster to tell the nurse the situation over the phone. The risks of just documenting in the ePMR with a very acute patient are many. It could be a matter of life or death. You have to treat and save the patient! That is your number one priority”.
“It is a part of our working culture (to verbally hand-over the patient). That is just what we do. This gives us the opportunity to be certain that we communicate the most important information regarding the patient”.
3.3. Mobility of the ePMR Invites to Conversation
“If you are having a conversation and the person you are talking to looks at their phone, you feel like they are not listening… In the same way we create a bigger distance between us and the patient whenever we start typing in the ePMR”.
“Well yes, it (when typing in the ePMR) can expand the distance between us and the patient, but when you gather information from the patient and concurrently register the data you can actually obtain a fine relation with the patient”.
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Greenhalgh, T.; Potts, H.W.W.; Wong, G.; Bark, P.; Swinglehurst, D. Tensions and Paradoxes in Electronic Patient Record Research: A Systematic Literature Review Using the Meta-narrative Method. Milbank Q. 2009, 87, 729–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, G.; Ellingsen, G. A Review of 25 Years of CSCW Research in Healthcare: Contributions, Challenges and Future Agendas. Comput. Support. Coop. Work 2013, 22, 609–665. Available online: http://0-link-springer-com.brum.beds.ac.uk/10.1007/s10606-012-9168-0 (accessed on 26 February 2021). [CrossRef]
- Houben, S.; Frost, M.; Bardram, J.E. Collaborative Affordances of Hybrid Patient Record Technologies in Medical Work. In Proceedings of the 18th ACM Conference on Computer Supported Cooperative Work & Social Computing—CSCW ’15; ACM Press: New York, NY, USA, 2015; pp. 785–797. Available online: http://0-dl-acm-org.brum.beds.ac.uk/citation.cfm?doid=2675133.2675164 (accessed on 26 February 2021).
- Tang, C.; Carpendale, S. Evaluating the deployment of a mobile technology in a hospital ward. In Proceedings of the ACM 2008 Conference on Computer Supported Cooperative work—CSCW ’08; ACM Press: New York, NY, USA, 2008; p. 205. Available online: http://0-portal-acm-org.brum.beds.ac.uk/citation.cfm?doid=1460563.1460596 (accessed on 26 February 2021).
- Peace, J.M.; Yuen, T.C.; Borak, M.H.; Edelson, D.P. Tablet-based cardiac arrest documentation: A pilot study. Resuscitation 2014, 85, 266–269. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC3624763/pdf/nihms412728.pdf (accessed on 26 February 2021). [CrossRef] [PubMed] [Green Version]
- Grundgeiger, T.; Albert, M.; Reinhardt, D.; Happel, O.; Steinisch, A.; Wurmb, T. Real-time tablet-based resuscitation documentation by the team leader: Evaluating documentation quality and clinical performance. Scand. J. Trauma. Resusc. Emerg. Med. 2016, 24, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, C.; Hemmings, L.; Brown, T. Lost in translation: Maximizing handover effectiveness between paramedics and receiving staff in the emergency department. Emerg. Med. Australas. 2009, 21, 102–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paramedic, E.M. eMR for Paramedics. Available online: http://www.emergencymedicalparamedic.com/emr-for-paramedics/ (accessed on 11 February 2021).
- Lindskou, T.A.; Mikkelsen, S.; Christensen, E.F.; Hansen, P.A.; Jørgensen, G.; Hendriksen, O.M.; Kirkegaard, H.; Berlac, P.A.; Søvsø, M.B. The Danish prehospital emergency healthcare system and research possibilities. Scand. J. Trauma. Resusc. Emerg. Med. 2019, 27, 100. Available online: https://0-sjtrem-biomedcentral-com.brum.beds.ac.uk/articles/10.1186/s13049-019-0676-5 (accessed on 26 February 2021). [CrossRef] [PubMed] [Green Version]
- Porter, A.; Badshah, A.; Black, S.; Fitzpatrick, D.; Harris-Mayes, R.; Islam, S.; Jones, M.; Kingston, M.; LaFlamme-Williams, Y.; Mason, S.; et al. Electronic health records in ambulances: The ERA multiple-methods study. Health Serv. Deliv. Res. 2020, 8, 1–140. Available online: https://www.journalslibrary.nihr.ac.uk/hsdr/hsdr08100 (accessed on 26 February 2021). [CrossRef] [PubMed] [Green Version]
- Frischknecht Christensen, E.; Berlac, P.A.; Nielsen, H.; Christiansen, C.F. The Danish quality database for prehospital emergency medical services. Clin. Epidemiol. 2016, 8, 667–671. Available online: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC5098515 (accessed on 26 February 2021). [CrossRef] [PubMed] [Green Version]
- The National State Auditors. Rigsrevisionens Notat om Beretning om Regionernes Præhospitale Indsats; National Audit Office: Copenhagen, Denmark, 2016; Available online: https://www.ft.dk/statsrevisorerne/dokumenter/samling/20131/beretning/sb7/bilag/4/1644776.pdf (accessed on 26 February 2021).
- Danish Regions, Danish Health Authority. De Danske Akutmodtagelser—Status 2016; The Danish Emergency Departments Status: Copenhagen, Denmark, 2016; p. 71. Available online: https://www.ft.dk/samling/20161/almdel/SUU/bilag/121/1706332.pdf (accessed on 26 February 2021).
- Neyland, D. Organizational Ethnography; SAGE Publications Ltd.: London, UK, 2008; Available online: https://0-methods-sagepub-com.brum.beds.ac.uk/book/organizational-ethnography (accessed on 26 February 2021).
- O’Reilly, K. Team Ethnography. In Key Concepts in Ethnography; SAGE Publications Ltd.: London, UK, 2009; pp. 202–208. ISBN 9781412928656. Available online: http://0-sk-sagepub-com.brum.beds.ac.uk/books/key-concepts-in-ethnography (accessed on 26 February 2021).
- Spradley, J.P. Participant Observation; Holt, Rinehart and Winston: New York, NY, USA, 1980. [Google Scholar]
- Bryant, A.; Charmaz, K. Grounded Theorizing Using Situational Analysis. In The SAGE Handbook of Grounded Theory; SAGE Publications Ltd.: London, UK, 2007; pp. 363–397. ISBN 9781412923460. Available online: http://0-methods-sagepub-com.brum.beds.ac.uk/book/the-sage-handbook-of-grounded-theory (accessed on 26 February 2021).
- Johnson, M.; Whyte, M.; Loveridge, R.; Yorke, R.; Naleem, S. A Unified Electronic Tool for CPR and Emergency Treatment Escalation Plans Improves Communication and Early Collaborative Decision Making for Acute Hospital Admissions. BMJ Qual. Improv. Rep. 2017, 6, u213254.w6626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groth, K.; Yngling, A.; Frykholm, O. Clinical journal: A collaborative shared medical workspace. Proc. ACM Conf. Comput. Support. Coop. Work. CSCW 2011, 633–636. [Google Scholar] [CrossRef]
- Poulymenopoulou, M.; Malamateniou, F.; Vassilacopoulos, G. E-EPR: A workflow-based electronic emergency patient record. Pers. Ubiquitous Comput. 2014, 18, 91–100. Available online: http://0-link-springer-com.brum.beds.ac.uk/10.1007/s00779-012-0620-4 (accessed on 26 February 2021). [CrossRef]
- Knutsen, G.O.; Fredriksen, K. Usage of documented pre-hospital observations in secondary care: A questionnaire study and retrospective comparison of records. Scand. J. Trauma. Resusc. Emerg. Med. 2013, 21, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, D.; McKenna, M.; Duncan, E.A.S.; Laird, C.; Lyon, R.; Corfield, A. Critcomms: A national cross-sectional questionnaire based study to investigate prehospital handover practices between ambulance clinicians and specialist prehospital teams in Scotland. Scand. J. Trauma. Resusc. Emerg. Med. 2018, 26, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sujan, M.A.; Chessum, P.; Rudd, M.; Fitton, L.; Inada-Kim, M.; Spurgeon, P.; Cooke, M.W. Emergency Care Handover (ECHO study) across care boundaries: The need for joint decision making and consideration of psychosocial history. Emerg. Med. J. 2015, 32, 112–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balla, J.; Heneghan, C.; Thompson, M.; Balla, M. Clinical decision making in a high-risk primary care environment: A qualitative study in the UK. BMJ Open 2012, 2, e000414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Dunne, R.; Yu, Z.; Shi, W. STREMS: A Smart Real-Time Solution toward Enhancing EMS Prehospital Quality. In Proceedings of the 2017 IEEE/ACM International Conference on Connected Ealth: Applications, Systems and Engineering Technologies (CHASE); IEEE: Piscataway, NJ, USA, 2017; pp. 365–372. Available online: http://0-ieeexplore-ieee-org.brum.beds.ac.uk/document/8010675/ (accessed on 26 February 2021).


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jensen, F.B.; Ladefoged, K.T.; Lindskou, T.A.; Søvsø, M.B.; Christensen, E.F.; Teli, M. Understanding the Effect of Electronic Prehospital Medical Records in Ambulances: A Qualitative Observational Study in a Prehospital Setting. Int. J. Environ. Res. Public Health 2021, 18, 2330. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052330
Jensen FB, Ladefoged KT, Lindskou TA, Søvsø MB, Christensen EF, Teli M. Understanding the Effect of Electronic Prehospital Medical Records in Ambulances: A Qualitative Observational Study in a Prehospital Setting. International Journal of Environmental Research and Public Health. 2021; 18(5):2330. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052330
Chicago/Turabian StyleJensen, Frederikke Bøgh, Kathrine Tornbjerg Ladefoged, Tim Alex Lindskou, Morten Breinholt Søvsø, Erika Frischknecht Christensen, and Maurizio Teli. 2021. "Understanding the Effect of Electronic Prehospital Medical Records in Ambulances: A Qualitative Observational Study in a Prehospital Setting" International Journal of Environmental Research and Public Health 18, no. 5: 2330. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052330