
Research Trends on Mobile Mental Health Application for General Population: A Scoping Review


Abstract
:1. Introduction
2. Methods
2.1. Identifying the Research Question
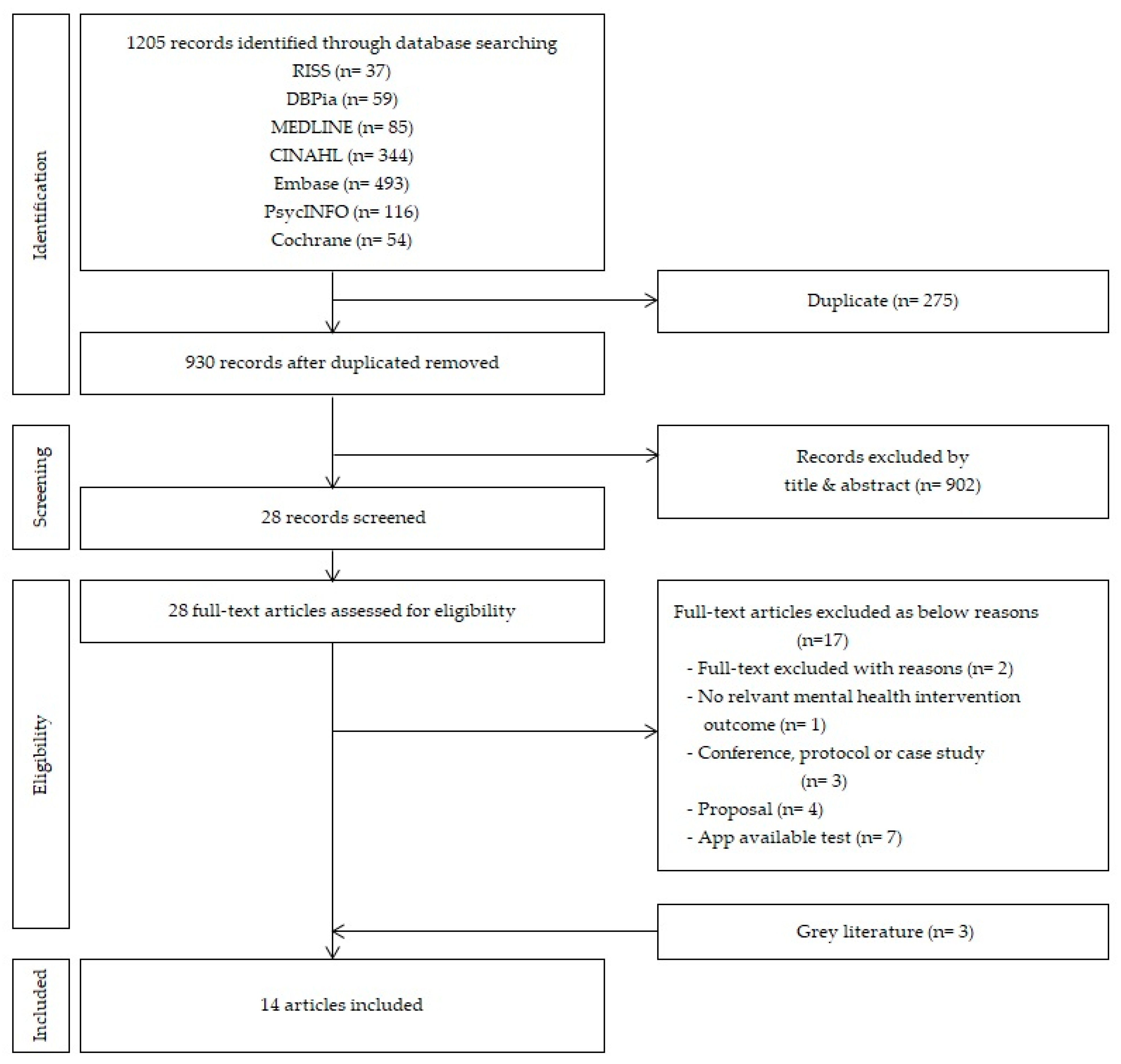
2.2. Identifying Relevant Studies
2.3. Study Selection
2.3.1. Study Population
2.3.2. Interventions
2.3.3. Comparisons
2.3.4. Outcomes
2.3.5. Study Design
2.4. Quality Evaluation of Selected Literature
2.5. Charting the Data
3. Results
3.1. General Characteristics of the Literature
3.2. Quality Evaluation of the Literature
3.3. Summary of the Literature
3.4. Experimental Research Using Mobile Apps
3.5. Mobile App Programs and Theoretical Evidence
- “It’s time to relax!” [16] is a stress management program developed by an Android smartphone app. Based on a mindfulness protocol, the app was designed so that users could follow instructions and practice meditation for free.
- “MoodPrism” [17] is an app developed to monitor and provide feedback on the user’s emotional state by converting the daily mood report to incorporate health aspects. The app also provides links on mental health information and resources.
- “ACT Daily” [18] is an EMI app designed to support the improvement and generalization of ACT (Acceptance and Commitment Therapy) technology, on which the users self-report emotions such as depression, anger, violent thoughts, and feelings of being trapped, and rate them on a Likert scale. Information is then provided on ways to alleviate such emotions.
- “Flowy” [19] is an app developed as a set of breathing-retraining exercises to manage anxiety, and uses simulations such as games to enable the user to subconsciously utilize breathing techniques.
- “IntelliCare” [21] is an app developed with the purpose of reducing depression or anxiety caused by sleep disorders, social isolation, or lack of physical activity, based on acceptance and commitment, conscious behavior, optimism, and problem-solving techniques.
- “iSMI (Internet-based stress management intervention)” [22] is an internet-based stress management program aimed to reduce stress, comprised of eight modules using problem-solving, relaxation, and acceptance tolerance therapy. Through adherence monitoring by an E-coach and presenting feedback pertaining to the user’s needs, an opportunity for the user to develop self-guided health promotion and behavioral change is provided.
- “Mhapp (MoodKit, MoodPrism, MoodMission)” [24] is a study involving the use of 3 apps—“MoodKit” and “MoodMission” are apps designed to manage depression, anxiety, and stress based on cognitive behavioral therapy. Upon analyzing mood, activity, values, and sentiment, it provides individualized goals that the user can choose and work towards.
- “Cognitive Control App” [25] is an app designed for the user to actively self-regulate behavior through choosing appropriate activities and refusing activities deemed inappropriate. It uses Cognitive Control Therapy (EVO), Problem-Solving Therapy App (iPST), Information Control (Health Tips) apps to facilitate both problem-solving abilities and provision of health information.
- “mHhealth” [26] is a mobile app with a combination approach involving wearables and cognitive behavioral therapy to reduce stress, depression, anxiety, and rage, developed to compensate for limitations observed in traditional approaches involving only cognitive behavioral therapy, such as dropout and loss, as well as the shortage of objective data between user experience and cognitive behavioral therapy sessions. Additionally, it provides objective data for the users and providers by identifying the user’s condition through cardiovascular and electrodermal input from wearable devices, enabling the detection of psychological stress.
- “DeStressify” [27] is a commercially available meditation app that provides guided meditation through audio, video, and text files. There are free and pro versions of the app, both of which are organized into visualization, gratitude, imagining one’s ideal life, and finding purpose. In the pro version, additional functions including the options “my friends,” “nutrition,” and “shop” are offered. Such functions are intended to manage symptoms of stress, anxiety, and depression.
- “Headspace & Smiling Mind” [28] is a preregistered meditation app with over 100,000 downloads on the Google play app with high-quality mobile ratings. ‘Headspace’ is designed for users to download the app and complete a basic 10-day training session on mindful breathing, body scan (systematically focusing on certain parts of the body), practice of nonjudgement of thoughts and emotions, and sitting meditation, then access other meditation tracks for the following 30 days using a prepaid voucher. “Smiling Mind” is a smartphone app developed by a psychologist and an educator that provides a variety of meditation programs for a diverse audience in different age groups. The adult program is designed for everyday use for 10 days, followed by continuous use for another 30 days to manage mental health using “Smiling Mind.” If the content is deemed insufficient, the user can select contents of their choice.
- “Mind Healer” [29] is an app developed for workers and the general adult population to manage stress and involves a psychological test and a PPG sensor that measures heart rate, enabling users to measure their mental health status, thus increasing workers’ self-awareness. Additionally, if stress, anxiety, or depression is detected, a short-term healing program is offered, providing breathing, meditation, music, and yoga practices for healing and management of mental health. By also providing materials for mental health education, the app enables users to promote mental health by themselves.
3.6. Effectiveness of Mental Health Interventions using Mobile Apps
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Pricewaterhouse Coopers. Emerging mHealth: Paths for Growth. 2014. Available online: pwc.com/gx/en/healthcare/mhealth/assets/pwc-emerging-mhealth-full.pdf (accessed on 1 March 2021).
- Commission, E. Green Paper on Mobile Health (‘m-Health’). 2014. Available online: ec.europa.eu/digital-single-market/en/node/69759 (accessed on 2 March 2020).
- East, M.L.; Havard, B.C. Mental Health Mobile Apps: From Infusion to Diffusion in the Mental Health Social System. JMIR Ment. Health 2015, 2, e10. [Google Scholar] [CrossRef] [PubMed]
- Marley, J.; Farooq, S. Mobile telephone apps in mental health practice: Uses, opportunities and challenges. BJPsych Bull. 2015, 39, 288–290. [Google Scholar] [CrossRef] [Green Version]
- Kay, M.; Santos, J.; Takane, M. mHealth: New horizons for health through mobile technologies. World Health Organ. 2011, 64, 66–71. [Google Scholar]
- Chandrashekar, P. Do mental health mobile apps work: Evidence and recommendations for designing high-efficacy mental health mobile apps. mHealth 2018, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Newman, M.G.; Szkodny, L.E.; Llera, S.J.; Przeworski, A. A review of technology-assisted self-help and minimal contact therapies for anxiety and depression: Is human contact necessary for therapeutic efficacy? Clin. Psychol. Rev. 2011, 31, 89–103. [Google Scholar] [CrossRef]
- Khalaf, S. Health and Fitness Apps Finally Take Off, Fueled by Fitness Fanatics. 2014. Available online: http://www.flurry.com/blog/health-and-fitness-apps-finally-take-off-fueled/ (accessed on 1 January 2021).
- Jang, J.S.; Cho, S.H. Mobile health (m-health) on mental health. Korean J. Stress Res. 2016, 24, 231–236. [Google Scholar] [CrossRef] [Green Version]
- Bakker, D.; Kazantzis, N.; Rickwood, D.; Rickard, N. Mental Health Smartphone Apps: Review and Evidence-Based Recommendations for Future Developments. JMIR Ment. Health 2016, 3, e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, H.J.; Kim, S.Y. What is scoping review? The Korean association for health technology assessment. J. Health Technol. Assess. 2018, 6, 16–21. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Scottish Intercollegiate Guidelines Network, S. SIGN 50: A Guideline Developer’s Handbook (Vol. SIGN Publication No. 50). Edinburgh: SIGN. Available online: http://www.sign.ac.uk (accessed on 1 December 2019).
- Kim, K.; Kim, J.H.; Lim, K.-C.; Lee, K.-S.; Jeong, J.-S.; Choe, M.; Chae, Y.R. Quality assessment tools and reporting standards in nursing research. J. Korean Biol. Nurs. Sci. 2012, 14, 221–230. [Google Scholar] [CrossRef]
- Donker, T.; Petrie, K.; Proudfoot, J.; Clarke, J.; Birch, M.R.; Christensen, H. Smartphones for Smarter Delivery of Mental Health Programs: A Systematic Review. J. Med. Internet Res. 2013, 15, e247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carissoli, C.; Villani, D.; Riva, G. Does a meditation protocol supported by a mobile application help people reduce stress? Suggestions from a controlled pragmatic trial. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Bakker, D.; Rickard, N. Engagement in mobile phone app for self-monitoring of emotional wellbeing predicts changes in mental health: MoodPrism. J. Affect. Disord. 2018, 227, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.E.; Haeger, J.; Pierce, B.; Cruz, R.A. Evaluating an Adjunctive Mobile App to Enhance Psychological Flexibility in Acceptance and Commitment Therapy. Behav. Modif. 2017, 41, 846–867. [Google Scholar] [CrossRef] [PubMed]
- Pham, Q.; Khatib, Y.; Stansfeld, S.; Fox, S.; Green, T. Feasibility and Efficacy of an mHealth Game for Managing Anxiety: “Flowy” Randomized Controlled Pilot Trial and Design Evaluation. Games Health J. 2016, 5, 50–67. [Google Scholar] [CrossRef] [PubMed]
- Yang, E.; Schamber, E.; Meyer, R.M.L.; Gold, J.I. Happier Healers: Randomized Controlled Trial of Mobile Mindfulness for Stress Management. J. Altern. Complement. Med. 2018, 24, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Mohr, D.C.; Tomasino, K.N.; Lattie, E.G.; Palac, H.L.; Kwasny, M.J.; Weingardt, K.; Schueller, S.M. IntelliCare: An Eclectic, Skills-Based App Suite for the Treatment of Depression and Anxiety. J. Med Internet Res. 2017, 19, e10. [Google Scholar] [CrossRef]
- Ebert, D.D.; Lehr, D.; Heber, E.; Riper, H.; Cuijpers, P.; Berking, M. Internet- and mobile-based stress management for employees with adherence-focused guidance: Efficacy and mechanism of change. Scand. J. Work Environ. Health 2016, 42, 382–394. [Google Scholar] [CrossRef] [Green Version]
- Morrison Wylde, C.; Mahrer, N.E.; Meyer, R.M.L.; Gold, J.I. Mindfulness for Novice Pediatric Nurses: Smartphone Application Versus Traditional Intervention. J Pediatr. Nurs. 2017, 36, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Bakker, D.; Kazantzis, N.; Rickwood, D.; Rickard, N. A randomized controlled trial of three smartphone apps for enhancing public mental health. Behav. Res. Ther. 2018, 109, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Arean, P.A.; Hallgren, K.A.; Jordan, J.T.; Gazzaley, A.; Atkins, D.C.; Heagerty, P.J.; Anguera, J.A. The use and effectiveness of mobile apps for depression: Results from a fully remote clinical trial. J. Med. Internet Res. 2016, 18, e330. [Google Scholar] [CrossRef] [Green Version]
- Winslow, B.D.; Chadderdon, G.L.; Dechmerowski, S.J.; Jones, D.L.; Kalkstein, S.; Greene, J.L.; Gehrman, P. Development and Clinical Evaluation of an mHealth Application for Stress Management. Front. Psychiatry 2016, 7, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, R.A.; Jung, M.E. Evaluation of an mHealth App (DeStressify) on university students’ mental health: Pilot trial. JMIR Ment. Health 2018, 5, e2. [Google Scholar] [CrossRef]
- Flett, J.A.; Hayne, H.; Riordan, B.C.; Thompson, L.M.; Conner, T.S. Mobile mindfulness meditation: A randomised controlled trial of the effect of two popular apps on mental health. Mindfulness 2019, 10, 863–876. [Google Scholar] [CrossRef]
- Hwang, W.J.; Jo, H.H. Evaluation of the Effectiveness of Mobile App-Based Stress-Management Program: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miralles, I.; Granell, C.; Díaz-Sanahuja, L.; Van Woensel, W.; Bretón-López, J.; Mira, A.; Casteleyn, S. Smartphone apps for the treatment of mental disorders: Systematic review. JMIR Mhealth Uhealth 2020, 8, e14897. [Google Scholar] [CrossRef] [PubMed]
- An, S.; Lee, H. Use of Mobile Mental Health Application for Mental Health Promotion: Based on the Information-Motivation-Behavioral Skills Model. Asian Commun. Res. 2018, 62, 167–194. [Google Scholar] [CrossRef]
- Kanthawala, S.; Joo, E.; Kononova, A.; Peng, W.; Cotten, S. Folk theorizing the quality and credibility of health apps. Mob. Media Commun. 2019, 7, 175–194. [Google Scholar] [CrossRef]
- Chung, B.Y.; Oh, E.H.; Song, S.J. Mobile Health for Breast Cancer Patients: A Systematic Review. Asian Oncol. Nurs. 2017, 17, 133–142. [Google Scholar] [CrossRef]
- Anderson, K.; Burford, O.; Emmerton, L. Mobile Health Apps to Facilitate Self-Care: A Qualitative Study of User Experiences. PLoS ONE 2016, 11, e0156164. [Google Scholar] [CrossRef] [Green Version]
- Fischer, E.H.; Farina, A. Attitudes toward seeking professional psychologial help: A shortened form and considerations for research. J. Coll. Stud. Dev. 1995, 36, 368–373. [Google Scholar]
- Fisher, W.A.; Fisher, J.D.; Harman, J. The information-motivation-behavioral skills model: A general social psychological approach to understanding and promoting health behavior. Soc. Psychol. Found. Health Illn. 2003, 22, 82–106. [Google Scholar]
- Linardon, J.; Cuijpers, P.; Carlbring, P.; Messer, M.; Fuller-Tyszkiewicz, M. The efficacy of app-supported smartphone interventions for mental health problems: A meta-analysis of randomized controlled trials. World Psychiatry 2019, 18, 325–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lecomte, T.; Potvin, S.; Corbière, M.; Guay, S.; Samson, C.; Cloutier, B.; Khazaal, Y. Mobile apps for mental health issues: Meta-review of meta-analyses. JMIR mHealth uHealth 2020, 8, e17458. [Google Scholar] [CrossRef] [PubMed]
- Weisel, K.K.; Fuhrmann, L.M.; Berking, M.; Baumeister, H.; Cuijpers, P.; Ebert, D.D. Standalone smartphone apps for mental health—a systematic review and meta-analysis. NPJ Digit. Med. 2019, 2, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Deady, M.; Choi, I.; Calvo, R.A.; Glozier, N.; Christensen, H.; Harvey, S.B. eHealth interventions for the prevention of depression and anxiety in the general population: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, E.; Lampit, A.; Choi, I.; Calvo, R.A.; Harvey, S.B.; Glozier, N. Effectiveness of eHealth interventions for reducing mental health conditions in employees: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesiraju, L. Health and Fitness Apps Finally Take Off, Fueled by Fitness Fanatics. 2017. Available online: https://www.flurry.com/blog/post/165079311062/health-fitness-app-users-are-going-the-distance (accessed on 13 June 2020).
- Martinez-Perez, B.; de la Torre-Diez, I.; Lopez-Coronado, M. Mobile Health Applications for the Most Prevalent Conditions by the World Health Organization: Review and Analysis. J. Med. Internet Res. 2013, 15, e120. [Google Scholar] [CrossRef] [PubMed]
- Yasini, M.; Beranger, J.; Desmarais, P.; Perez, L.; Marchand, G. mHealth Quality: A Process to Seal the Qualified Mobile Health Apps. Stud. Health Technol. Inform. 2016, 228, 205–209. [Google Scholar] [PubMed]
- Boulos, M.N.; Brewer, A.C.; Karimkhani, C.; Buller, D.B.; Dellavalle, R.P. Mobile medical and health apps: State of the art, concerns, regulatory control and certification. Online J. Public Health Inform. 2014, 5, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loo Gee, B.; Griffiths, K.M.; Gulliver, A. Effectiveness of mobile technologies delivering Ecological Momentary Interventions for stress and anxiety: A systematic review. J. Am. Med. Inform. Assoc. 2016, 23, 221–229. [Google Scholar] [CrossRef] [Green Version]
- Klasnja, P.; Pratt, W. Healthcare in the pocket: Mapping the space of mobile-phone health interventions. J. Biomed. Inform. 2012, 45, 184–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoaib, M.; Bosch, S.; Incel, O.D.; Scholten, H.; Havinga, P.J. Fusion of smartphone motion sensors for physical activity recognition. Sensor 2014, 14, 10146–10176. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-Y. Updates in management of occupational mental health problems in the clinical preactice. J. Korean Neuropsychiatr. Assoc. 2020, 59, 87. [Google Scholar] [CrossRef]
- Larsen, M.E.; Huckvale, K.; Nicholas, J.; Torous, J.; Birrell, L.; Li, E.; Reda, B. Using science to sell apps: Evaluation of mental health app store quality claims. NPJ Digit. Med. 2019, 2, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, M.E.; Nicholas, J.; Christensen, H. A systematic assessment of smartphone tools for suicide prevention. PLoS ONE 2016, 11, e0152285. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Torous, J.; Nicholas, J.; Carney, R.; Rosenbaum, S.; Sarris, J. Can smartphone mental health interventions reduce symptoms of anxiety? A meta-analysis of randomized controlled trials. J. Affect. Disord. 2017, 218, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Coulon, S.M.; Monroe, C.M.; West, D.S. A Systematic, Multi-domain Review of Mobile Smartphone Apps for Evidence-Based Stress Management. Am. J. Prev. Med. 2016, 51, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Ernsting, C.; Dombrowski, S.U.; Oedekoven, M.; LO, J.; Kanzler, M.; Kuhlmey, A.; Gellert, P. Using smartphones and health apps to change and manage health behaviors: A population-based survey. J. Med. Internet Res. 2017, 19, e101. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Categories | N (%) |
|---|---|---|
| Publication Year | 2013∼2015 2016∼2019 | 1 (7.1) 13(92.9) |
| Research Designs | Randomized controlled trials Nonrandomized controlled trials Survey | 10(71.4) 3(21.4) 1 (7.1) |
| Intervention Group | The general adult population Psychological clients Employees Students Nurses Soldiers | 3(21.4) 3(21.4) 2(14.3) 3(21.4) 2(14.3) 1 (7.1) |
| Intervention Duration | below 4 weeks 8 weeks 12 weeks 24 weeks | 9 (64.3) 3 (21.4) 1 (7.1) 1 (7.1) |
| Controlled Trial | Carissoli (2015) [16] | David (2018) [17] | Levin (2017) [18] | Pham (2016) [19] | Yang (2018) [20] | Mohr (2017) [21] | Ebert (2016) [22] | Wylde (2017) [23] | Bakker (2018) [24] | Arean (2016) [25] | Winslow (2016) [26] | Lee (2018) [27] | Flett (2019) [28] | Hwang (2019) [29] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1.1 The study addresses an appropriate and clearly focused question. | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | |
| 1.2 The assignment of subjects to treatment groups is randomized. | Y | NA | Y | Y | NA | Y | NA | Y | Y | Y | Y | Y | Y | |
| 1.3 An adequate concealment method is used. | CS | NA | Y | Y | NA | Y | NA | Y | Y | N | Y | Y | CS | |
| 1.4 The design keeps subjects and investigators ‘blind’ about treatment allocation. | CS | NA | N | Y | NA | Y | NA | Y | Y | N | Y | Y | CS | |
| 1.5 The treatment and control groups are similar at the start of the trial | Y | * | Y | Y | NA | Y | Y | Y | Y | Y | Y | Y | Y | |
| 1.6 The only difference between groups is the treatment under investigation. | Y | NA | Y | Y | NA | Y | Y | Y | Y | Y | Y | Y | Y | |
| 1.7 All relevant outcomes are measured in a standard, valid, and reliable way. | N | Y | Y | Y | Y | Y | Y | Y | CS | Y | Y | Y | Y | |
| 1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed? | 0.0% | 7.1% | 0.0% | 6.8% | 5.7% | 0.4% | 0.0% | 35.8% | 55.4% (4 weeks) 64.3% (8 weeks) 69.7% (12 weeks) | 0.0% | 20.9% | 1.0% | 6.7% | |
| 1.9 All the subjects are analyzed in the groups to which they were randomly allocated (often referred to as intention to treat analysis). | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | |
| 1.10 Where the study is carried out at more than one site, results are comparable for all sites. | CS | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | |
| Overall assessment of the study. | + | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ |
| Author (Year) | Name | Program/Evidence | Research Design | Intervention Group (N) | Period | Measure Tools | Results (Significant *) | |
|---|---|---|---|---|---|---|---|---|
| 1 | Carissoli et al. (2015) [16] | “it’s time to relax!’’ | Mindful apps, MindApps, both released from iTunes | Randomized Controlled Trial | Italian workers (56) | 3 weeks | MSP, HR | Meditation group: improvement in coping with stress, reduction in hyperactivity and accelerated behaviors and heartbeats* Listened to music: improvement in coping with stress. Reduction in pain and physical problems and heartbeats * |
| 2 | Bakker and Rickard (2018) [17] | MoodPrism | MoodPrism | Survey | General adults (234) | 30 days | PHQ-9, GAD-7, WEMWBS ESAS-R, MHLQ CSES, SDS | Reduction in depression * Reduction in anxiety * Increase in mental well-being * |
| 3 | Levin et al. (2017) [18] | ACT Daily | ecological momentary intervention, acceptance and commitment therapy(ACT) | Nonrandomized Controlled Trial | Depressed/ anxious clients (14) | 2 weeks | DASS, AAQ-Ⅱ CFQ, VQ PHLMS, SUS | Reduction in depression * Reduction in anxiety * Reduction in overall psychological inflexibility * Reduction in cognitive fusion * Reduction in obstacles * Reduction in acceptance * |
| 4 | Pham, Khatib, Stansfeld, Fox, and Green (2016) [19] | Flowy | breathing exercises Diaphragmatic breathing | Randomized Controlled Pilot Trial | Adults with Common Mental Health Disorders (63) | 4 weeks | eHEALS, GAD-7, OASIS, ASI-3, PDSS-SR, QLES-Q-SF Nijmegen Questionnaire | Reduction in anxiety, panic, hyperventilation Increase in quality of life * |
| 5 | Yang, Schamber, Meyer, and Gold (2018) [20] | Headspace | mindfulness | Randomized controlled trial | Medical students (88) | 60 days | PSS, FFMQ GWBS | Reduction in perceived stress * Increase in well-being and sustainment * |
| 6 | Mohr et al. (2017) [21] | IntelliCare | acceptance commitment therapy, cognitive-behavioral therapy, positive psychology | Nonrandomized Controlled Trial | Adults With depressive /anxiety symptoms (96) | 8 weeks | PHQ-9 GAD-7 | Reduction in depression * Reduction in anxiety * |
| 7 | Ebert et al. (2016) [22] | iSMI (internet- based stress management intervention) | Lazarus’ transactional model problem-solving therapy, emotion regulation | Randomized controlled trial | Employees with stress symptoms (264) | 6 months | PSS-10 | Reduction (7 weeks) in stress and sustainment * |
| 8 | Morrison Wylde, Mahrer, Meyer, and Gold (2017), [23] | SDM (smartphone delivered mindfulness) | Cognitive Behavior Therapy | Nonrandomized Controlled Trial | Novice pediatric Nurse (95) | 4 weeks | CFST LEC PCL-C FFMQ | Reduction in burnout Increase in compassion satisfaction Increase in “acting with awareness” and “nonreactivity to inner experience” * |
| 9 | Bakker, Kazantzis, Rickwood, and Rickard (2018) [24] | MHapp - MoodKit, - MoodPrism, - MoodMission | Cognitive Behavior Therapy | Randomized controlled trial | General adults (226) | 30 days | PHQ-9, GAD-7 WEMWBS, ESAS-R, CSES MHLQ | Increase in mental well-being Increase in coping self-efficacy Reduction in depression (MoodKit and MoodMission group) * Improvement in anxiety * |
| 10 | Arean et al. (2016) [25] | EVO iPST Health Tips | EVO: Cognitive Control Therapy iPST: Problem-Solving Therapy Health Tips: Information Control | Randomized controlled trial | General adults with depressive symptoms (626) | 12 weeks | PHQ-9, SDS GAD-7, IMPACT AUDIT-C | No difference at weeks 4 and 8 for the project EVO yielded higher rates of recovery at 4 weeks compared with the Health Tips group * Similar recovery between the iPST and Health Tips arms |
| 11 | Winslow et al. (2016) [26] | mHealth | Cognitive behavioral therapy | Randomized Controlled Trial | US military veterans (16) | 8 weeks | SUDS, DASS PROMIS, TSST | Reduction in stress * Reduction in anxiety * Reduction in stress and depression (between time points)* |
| 12 | Lee and Jung (2018) [27] | DeStressify | Mindfulness | Randomized controlled trial | University students (163) | 4 Weeks | PSS, STAI QIDS-SR, MDD PSQI, RAND WPAI | Reduction in trait anxiety * Improvement in general health, energy, emotional well-being * |
| 13 | Flett, Hayne, Riordan, Thompson, and Conner (2019) [28] | Headspace Smile Mind | Mindfulness | Randomized controlled trial | University students (208) | 30 Days | CES-D HADS-A PSS, BRS FS, CAT CAMS-R | Improvement in depressive symptoms and resilience * |
| 14 | Hwang and Jo (2019) [29] | Mind Healer | Meditation, sound, yoga, health information | Randomized controlled trial | nurses (56) | 4 Weeks | PSS-10, KOSS PHQ-9, GAD-10 | Reduction in perceived stress and occupational stress * Reduction in emotional labor * Increase in self-efficacy, well-being * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, W.J.; Ha, J.S.; Kim, M.J. Research Trends on Mobile Mental Health Application for General Population: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 2459. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052459
Hwang WJ, Ha JS, Kim MJ. Research Trends on Mobile Mental Health Application for General Population: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(5):2459. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052459
Chicago/Turabian StyleHwang, Won Ju, Ji Sun Ha, and Mi Jeong Kim. 2021. "Research Trends on Mobile Mental Health Application for General Population: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 5: 2459. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052459