
Impact and Effectiveness of Group Strategies for Supporting Breastfeeding after Birth: A Systematic Review

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment and Risk of Bias
3. Results
3.1. Literature Search Results: Study Selection
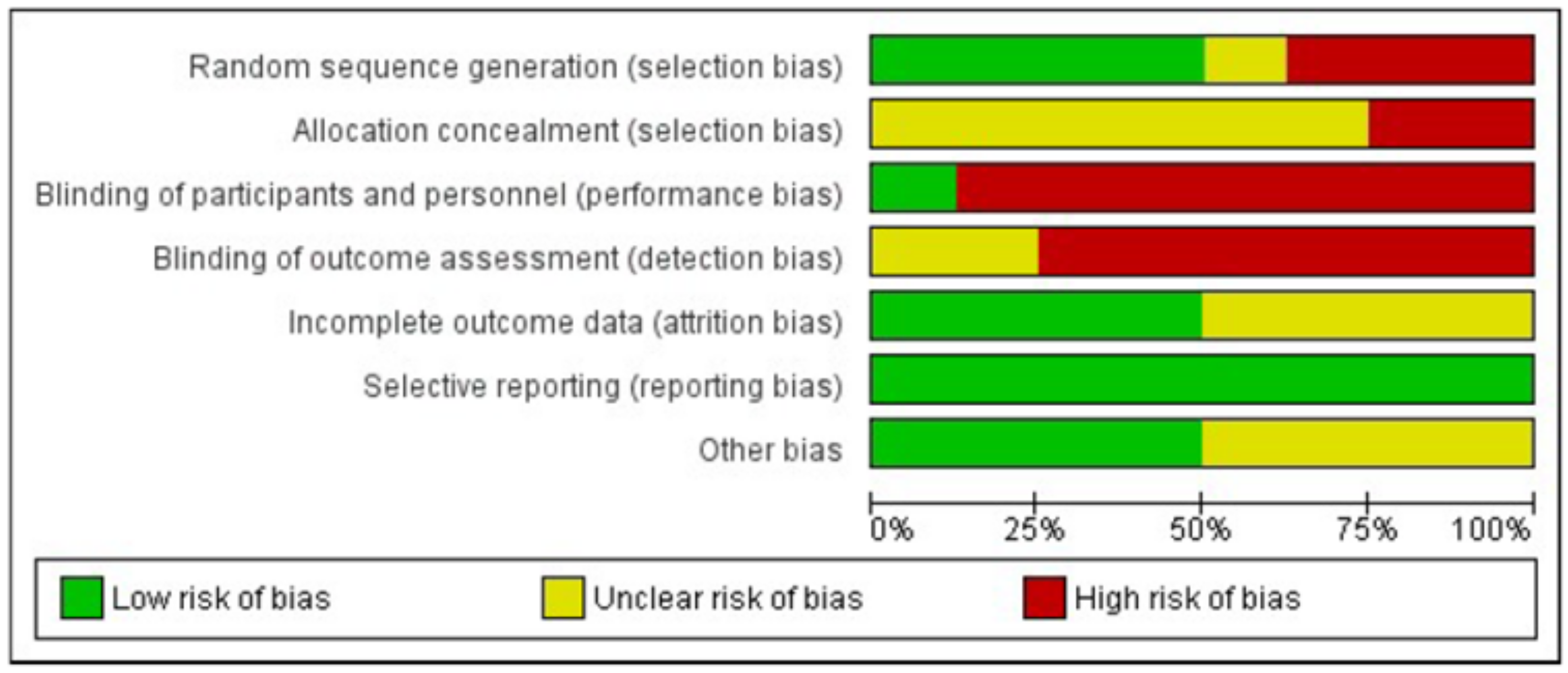
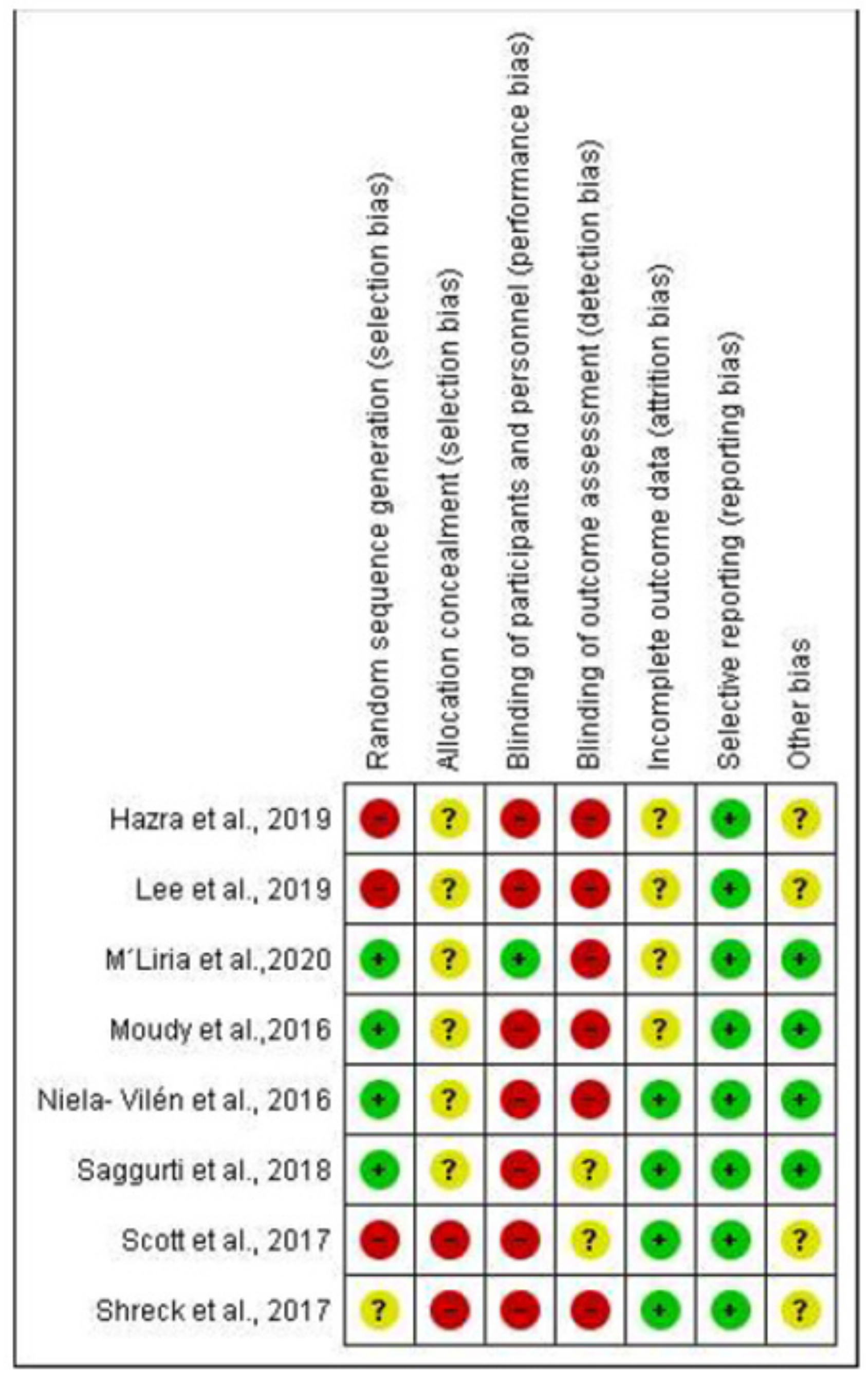
3.2. Risk of Bias
3.3. Characteristics of the Sample
3.4. Participants
3.5. Measuring Instruments and Interval
3.6. Characteristics of the Interventions
3.7. Impact of the Group Interventions on BF
3.7.1. Breastfeeding Initiation
3.7.2. Two Weeks Postpartum
3.7.3. Between One and Six Months Postpartum
3.7.4. Six Months Postpartum
4. Discussion
4.1. Summary of the Findings
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Exclusive Breastfeeding. Available online: https://www.who.int/nutrition/topics/exclusive_breastfeeding/es/ (accessed on 25 September 2020).
- World Health Organization; UNICEF. Global Strategy for Infants and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003; Available online: https://www.who.int/maternal_child_adolescent/documents/9243562215/es/ (accessed on 25 September 2020).
- Alzate-Meza, M.C.; Arango, C.; Castaño-Castrillón, J.J.; Henao-Hurtado, A.M.; Lozano-Acosta, M.M.; Muñoz-Salazar, G.; Ocampo-Muñoz, N.A.; Rengifo-Calderón, S.V.; Tovar-Orozco, L.M.; Vallejo-Chávez, S.H. Lactancia materna como factor protector para enfermedades prevalentes en niños hasta de 5 años de edad en algunas instituciones educativas de Colombia 2009. Estudio de corte transversal. Rev. Colomb. Obstet. Ginecol. 2011, 62, 57–63. [Google Scholar] [CrossRef]
- Woodward, L.J.; Liberty, K.A. Enciclopedia Sobre el Desarrollo de la Primera Infancia: Lactancia Materna y Desarrollo Psicosocial del niño. 2017. Available online: http://www.enciclopedia-infantes.com/sites/default/files/textes-experts/es/2271/lactancia-materna-y-desarrollo-psicosocial-del-nino.pdf (accessed on 28 September 2020).
- Kramer, M.S.; Chalmers, B.; Hodnett, E.D.; Shapiro, S.; Collet, J.P.; Shapiro, S.; Collet, J.; Vanilovich, I.; Mezen, I.; Ducruet, T.; et al. Promotion of Breastfeeding Intervention Trial (PROBIT): A randomized trial in the Republic of Belarus. JAMA 2001, 285, 413–420. [Google Scholar] [CrossRef]
- Comité de Lactancia Materna; Asociación Española de Pediatría. Tasas de Inicio y Duración de Lactancia Materna en España y Otros Países. AEP. 2016. Available online: https://www.aeped.es/sites/default/files/documentos/201602-lactancia-materna-cifras.pdf (accessed on 25 September 2020).
- Cabedo, R.; Manresa, M.; Cambredó, M.V.; Montero, L.; Reyes, A.; Gol, R.; Falguera, G. Tipos de lactancia materna y factores que influyen en su abandono hasta los 6 meses. Estudio LACTEM. Matronas Prof. 2019, 20, 54–61. [Google Scholar]
- United Nations Children’s Fund UNICEF. From the First Hour of Life: Making the Case for Improved Infant and Young Child Feeding Everywhere; UNICEF: New York, NY, USA, 2016; Available online: http://data.unicef.org/resources/first-hour-life-new-report-breastfeedingpractices/ (accessed on 25 September 2020).
- McAndrew, F.; Thompson, J.; Fellows, L.; Large, A.; Speed, M.; Renfrew, M.J. Infant Feeding Survey 2010; IFF Research; Health and Social Care Information Centre: London, UK, 2012; Available online: http://doc.ukdataservice.ac.uk/doc/7281/mrdoc/pdf/7281_ifs-uk-2010_report.pdf (accessed on 25 September 2020).
- Gianni, M.L.; Bettinelli, M.E.; Manfra, P.; Sorrentino, G.; Bezze, E.; Plevani, L.; Cavallaro, G.; Raffaeli, G.; Crippa, B.L.; Colombo, L.; et al. Breastfeeding Difficulties and Risk for Early Breastfeeding Cessation. Nutrients 2019, 11, 2266. [Google Scholar] [CrossRef] [Green Version]
- Hornsby, P.P.; Gurka, K.K.; Conaway, M.R.; Kellams, A.L. Reasons for Early Cessation of Breastfeeding among Women with Low Income. Breastfeed Med. 2019, 14, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Rúa, L.; Díaz-Grávalos, G.J. Early interruption of breastfeeding. A qualitative study. Enferm. Clin. 2019, 29, 207–215. [Google Scholar] [CrossRef]
- World Health Organization; UNICEF. Protecting, Promoting, and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services: The Revised Baby-Friendly Hospital Initiative; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/nutrition/publications/infantfeeding/bfhi-implementation/en/ (accessed on 28 September 2020).
- McFadden, A.; Gavine, A.; Renfrew, M.J.; Wade, A.; Buchanan, P.; Taylor, J.L.; Veitch, E.; Rennie, A.M.; Crowther, S.A.; Neiman, S.; et al. Support for healthy breastfeeding mothers with healthy term babies. Cochrane Database Syst. Rev. 2017, 28, CD001141. [Google Scholar] [CrossRef] [Green Version]
- Balaguer, J.V.; Valcarce, I.; Esquivel, J.N.; Hernández, A.; Martín, M.D.P.; Bernad, M. Apoyo telefónico de la lactancia materna desde Atención Primaria: Ensayo clínico aleatorizado y multicéntrico. An. Pediatr. 2018, 89, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L.; Kingston, D. A systematic review of telephone support for women during pregnancy and the early postpartum period. J. Obstet. Gynecol. Neonatal. Nurs. 2008, 37, 301–314. [Google Scholar] [CrossRef]
- Ferraz Dos Santos, L.; Borges, R.F.; De Azambuja, D.A. Telehealth and Breastfeeding: An Integrative Review. Telemed. J. E-Health 2020, 26, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Wolynn, T. Using social media to promote and support breastfeeding. Breastfeed Med. 2012, 7, 364–365. [Google Scholar] [CrossRef] [PubMed]
- Bridges, N.; Howell, G.; Schmied, V. Exploring breastfeeding support on social media. Int. Breastfeed J. 2018, 13, 22. [Google Scholar] [CrossRef] [PubMed]
- Skouteris, H.; Nagle, C.; Fowler, M.; Kent, B.; Sahota, P.; Morris, H. Interventions designed to promote exclusive breastfeeding in high-income countries: A systematic review. Breastfeed Med. 2014, 9, 113–127. [Google Scholar] [CrossRef] [Green Version]
- Sebastián-Vicente, M. Los grupos de apoyo a la lactancia materna como iniciativas de participación y promoción de la salud en la comunidad. Dilemata 2017, 25, 227–238. [Google Scholar]
- Chetwynd, E.M.; Wasser, H.M.; Poole, C. Breastfeeding Support Interventions by International Board Certified Lactation Consultants: A Systemic Review and Meta-Analysis. J. Hum. Lact. 2019, 35, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Equator Network. Enhancing the QUAlity and Transparency of health Research. Available online: https://www.equator-network.org/about-us/equator-network-what-we-do-and-how-we-are-organised/ (accessed on 30 October 2020).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 16, e296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 23, c332. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; updated March 2011; The Cochrane Collaboration: London, UK, 2011; Available online: https://training.cochrane.org/handbook/current (accessed on 1 October 2020).
- Moudi, S.; Tafazoli, M.; Boskabadi, H.; Ebrahimzadeh, S.; Salehiniya, H. Comparing the effect of breastfeeding promotion interventions on exclusive breastfeeding: An experimental study. Biomed. Res. Ther. 2016, 3, 910–927. [Google Scholar] [CrossRef] [Green Version]
- Niela-Vilén, H.; Axelin, A.; Melender, H.L.; Löyttyniemi, E.; Salanterä, S. Breastfeeding preterm infants—A randomized controlled trial of the effectiveness of an Internet-based peer-support group. J. Adv. Nurs. 2016, 72, 2495–2507. [Google Scholar] [CrossRef]
- Saggurti, N.; Atmavilas, Y.; Porwal, A.; Schooley, J.; Das, R.; Kande, N.; Irani, L.; Hay, K. Effect of health intervention integration within women’s self- help groups on collectivization and healthy practices around reproductive, maternal, neonatal and child health in rural India. PLoS ONE 2018, 13, e0202562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- M‘Liria, J.K.; Kimiywe, J.; Ochola, S. Impact of Mother-to-Mother Support Groups in Promoting Exclusive Breastfeeding in a Low-Resource Rural Community in Kenya: A Randomized Controlled Trial. Curr. Res. Nutr. Food Sci. J. 2020, 8, 609–621. [Google Scholar] [CrossRef]
- Scott, S.; Pritchard, C.; Szatkowski, L. The impact of breastfeeding peer support for mothers aged under 25: A time series analysis. Matern. Child Nutr. 2017, 13, e12241. [Google Scholar] [CrossRef] [Green Version]
- Hazra, A.; Atmavilas, Y.; Hay, K.; Saggurti, N.; Verma, R.K.; Ahmad, J.; Kumar, S.; Mohanan, P.; Mavalankar, D.; Irani, L. Effects of health behaviour change intervention through women’s self-help groups on maternal and newborn health practices and related inequalities in rural India: A quasi-experimental study. EClinicalMedicine 2019, 20, 100198. [Google Scholar] [CrossRef] [Green Version]
- Schreck, P.K.; Solem, K.; Wright, T.; Schulte, C.; Ronnisch, K.J.; Szpunar, S. Both Prenatal and Postnatal Interventions Are Needed to Improve Breastfeeding Outcomes in a Low-Income Population. Breastfeed Med. 2017, 12, 142–148. [Google Scholar] [CrossRef]
- Lee, Y.H.; Chang, G.L.; Chang, H.Y. Effects of education and support groups organized by IBCLCs in early postpartum on breastfeeding. Midwifery 2019, 75, 5–11. [Google Scholar] [CrossRef]
- Rayfield, S.; Oakley, L.; Quigley, M.A. Association between breastfeeding support and breastfeeding rates in the UK: A comparison of late preterm and term infants. BMJ Open 2015, 5, e009144. [Google Scholar] [CrossRef]
- Undlien, M.; Viervoll, H.-A.; Rostad, B. Effect of mother support groups on nutritional status in children under two years of age in Laisamis village, Kenya. Afr. Health Sci. 2016, 16, 904–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruducha, J.; Huang, X.; Potter, J.; Hariharan, D.; Ahmad, D.; Kumar, S.; Mohanan, P.S.; Hazra, A. Perceived Social Networks and Newborn Health: Evidence from Self-Help Group Communities in Northern India. Societies 2018, 8, 92. [Google Scholar] [CrossRef] [Green Version]
- Robinson, A.; Lauckner, C.; Davis, M.; Hall, J.; Anderson, A.K. Facebook support for breastfeeding mothers: A comparison to offline support and associations with breastfeeding outcomes. Digit Health 2019, 11. [Google Scholar] [CrossRef]
- Jenkins, L.A.; Barnes, K.; Latter, A.; Edwards, R.A. Examining the Baby Café Model and Mothers’ Breastfeeding Duration, Meeting of Goals, and Exclusivity. Breastfeed Med. 2020, 15, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Brahm, P.; Valdés, V. Benefits of breastfeeding and risks associated with not breastfeeding. Rev. Chil. Pediatr. 2017, 88, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Olufunlayo, T.F.; Roberts, A.A.; MacArthur, C.; Thomas, N.; Odeyemi, K.A.; Price, M.; Jolly, K. Improving exclusive breastfeeding in low and middle-income countries: A systematic review. Matern. Child Nutr. 2019, 15, e12788. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Park, S.; Oh, J.; Kim, J.; Ahn, S. Interventions promoting exclusive breastfeeding up to six months after birth: A systematic review and meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 2018, 50, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.V.; Phua, J.; Lee, K.M. Telling stories about breastfeeding through Facebook: The impact of user-generated content (UGC) on pro-breastfeeding attitudes. Comput. Hum. Behav. 2015, 46, 6–17. [Google Scholar] [CrossRef]
- Tang, K.; Gerling, K.; Chen, W.; Geurts, L. Information and Communication Systems to Tackle Barriers to Breastfeeding: Systematic Search and Review. J. Med. Internet Res. 2019, 21, e13947. [Google Scholar] [CrossRef] [Green Version]
- Coulson, N.S.; Greenwood, N. Families affected by childhood cancer: An analysis of the provision of social support within online support groups. Child Care Health Dev. 2012, 38, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Cox, K.; Binns, C.W.; Giglia, R. Predictors of breastfeeding duration for rural women in a high-income country: Evidence from a cohort study. Acta Paediatr. 2015, 104, e350–e359. [Google Scholar] [CrossRef]
- Shakya, P.; Kunieda, M.K.; Koyama, M.; Rai, S.S.; Miyaguchi, M.; Dhakal, S.; Sandy, S.; Sunguya, B.F.; Jimba, M. Effectiveness of community-based peer support for mothers to improve their breastfeeding practices: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0177434. [Google Scholar]
- Sinha, B.; Chowdhury, R.; Sankar, M.J.; Martines, J.; Taneja, S.; Mazumder, S.; Rollins, N.; Bahl, R.; Bhandari, N. Interventions to improve breastfeeding outcomes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 114–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoddinott, P.; Britten, J.; Prescott, G.J.; Tappin, D.; Ludbrook, A.; Godden, D.J. Effectiveness of policy to provide breastfeeding groups (BIG) for pregnant and breastfeeding mothers in primary care: Cluster randomised controlled trial. BMJ 2009, 30, a3026. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Database | Strategy | Filter | Results |
|---|---|---|---|
| MEDLINE | (breastfeeding OR “breast feeding” OR “milk secretion” OR lactation) AND (“support group” OR meeting OR “self-help group” OR “breastfeeding workshop” OR “Group Processes”) AND (impact OR effect OR influence) | 2015–2020, humans, language English, Spanish and Portuguese | 195 |
| SCOPUS | 2015–2020, language English, Spanish and Portuguese | 193 | |
| WOS | 2015–2020, language English, Spanish and Portuguese | 520 | |
| CINHAL | 2015–2020, language English, Spanish and Portuguese | 90 | |
| COCHRANE LIBRARY | 2015–2020 | 363 | |
| LILACS | 2015–2020, language English, Spanish and Portuguese | 3 |
| Author, Year and Country | Study Design | Objective | Study Characteristics | Intervention | Measuring Instrument | Main Results | Impact on Breastfeeding | Quality Assessment Outcome |
|---|---|---|---|---|---|---|---|---|
| Rayfield et al. [36] (2015) United Kingdom | Observational Descriptive Cross-sectional and Comparative study | To explore the association between breastfeeding support and breastfeeding among late preterm (34–36 gestational weeks) and term (≥37 gestational weeks) infants. | Participants = 15,104 singletons born with a gestational age over 34 weeks, of which 14,525 (95.9%) were full term and 579 (4.1%) were late preterm. | Prenatal and postnatal professional advice (midwives or midwife care assistants) + support group Face to face | Structured questionnaire Infant Feeding Survey (IFS) Self-report 6–10 weeks 4–6 months 8–10 months | The mothers who used support from community support groups had significantly higher BF rates than those who did not use this support (p = 0.043). The mothers who reported receiving contact details for breastfeeding support groups had a higher likelihood of breastfeeding late preterm (aOR = 3.14, 95% CI = 1.40 to 7.04) and term (aOR = 2.24, 95% CI = 1.86 to 2.68) infants at 10 days and term infants at 6 weeks (aOR = 1.83, 95% CI = 01.51 to 2.22). | Successful breastfeeding | High |
| Moudi et al. [28] (2016) Iran | Quasi-experimental study | To compare the effect of breastfeeding promotion interventions on exclusive BMF among primiparous women | Participants = 93 primigravidae mothers Age = 18–35 years old Three groups: peer support, education by health care providers, and control (routine prenatal and postpartum care). | The selected mothers in the centre assigned to the peer support were introduced to a volunteer peer with regard to cultural, social, and economical similarities. Face to face and telephone interventions were combined. The selected mothers in the centre assigned to the training health care providers received the first training at 36–38 gestational weeks, and three latter training sessions in 1-, 2- and 3-week intervals after birth by a health care provider. Face to face and telephone interventions were combined. | Structured questionnaire Exclusive breastfeeding rate Initiation–4 weeks–8 weeks | BMF initiation = No significant differences in the three groups (p = 0.879) The three groups had no significant difference in terms of duration of exclusive BMF at 4 weeks (p = 0.056) but did have a significant difference at 8 weeks (p = 0.014) Exclusive BMF at 4 weeks = Peer support group (90.3%), education by health care provider group (83.3%) and control group (65.6%). Significant differences in the three groups (p = 0.043). Exclusive BMF at 8 weeks = Peer support group (6.5%), education by health care provider group (6.7%) and control group (28.1%). Significant difference between the three groups (p = 0.023). | Successful breastfeeding | 1- |
| Undlien et al. [37] (2016) Kenya | Observational Descriptive Cross-sectional and Comparative study | To determine how the Mother Support Groups (MSGs) affect the nutrition status of children under 2 years of age. | Participants = 20 mothers in each group (41 children) IG: Children whose mothers participated in MSGs CG: Children whose mothers did not participate in MSGs. Both groups received standardized treatment (including supplementary feeding if defined as malnourished) and counselling. Age = Children aged 6 months old or less. | Groups of women either pregnant or with children under 5 years of age learn about the importance of breastfeeding and adequate nutrition by means of health education, demonstrations and discussions. Face to face | Structured questionnaire Every month (during 1 year) First week postpartum (T1) Five-six weeks postpartum (T2) | There was no significant difference between the two groups with respect to breastfeeding practices (p = 0.414). Every mother in both groups stated that they had breastfed their child exclusively for the first 6 months. | No significant difference | High |
| Niela-Vilén et al. [29] (2016) Finland | Randomized controlled trial | To examine whether an Internet-based peer support intervention has any effect on the duration of breastfeeding, breast milk expression or maternal breastfeeding attitude compared with routine care in the mothers of preterm infants. | Participants = 124 mothers (64 in the CG; 60 in the IG) Intervention: Peer-support group in social media (Facebook) Control: Routine breastfeeding support in the NICU | A closed breastfeeding peer-support group in social media (Facebook). Peer support was provided by three voluntary mothers who had previous experience on breastfeeding their own preterm infants. The participating mothers were also peer supporters of each other. | Structured questionnaire Exclusive/ Overall breastfeeding rate Iowa Infant Feeding Attitudes Scale (IFFAS) Breastfeeding Self-Efficacy—Short Form (BSES-SF) 1st week postpartum—Infant’s corrected age of 3/6/12 months | Duration of exclusive BMF; p = 0.10 Duration of overall BMF; p = 0.60 Duration of expressing milk; p = 0.80 | No significant difference | 1- |
| Scott et al. [32] (2017) UK | Pre-/Post-quasi-experimental | To evaluate the effectiveness of a Breastfeeding Peer Support Service (BPSS) in increasing breastfeeding initiation and duration in young mothers. | Participants = 5790 women Age < 25 year old | The supporters receive externally accredited BPS training prior to supporting women. Paid peer supporters offer intensive one-to-one support from 30–34 gestational weeks until 6 weeks post-partum, with the highest intensity of support provided during the 2 weeks following birth, offering ongoing and responsive support (face to face or by telephone) according to the women’s individual needs | Any and Exclusive breastfeeding rate Baseline-2 weeks postpartum-6 weeks postpartum | Prevalence at birth increased by 0.55 percentage points per month (95% CI = 0.10–1.00, p = 0.018) and, at 2 weeks, by 0.50 percentage points (95% CI = 0.15–0.86, p = 0.007). There was no change from an increasing trend in prevalence at 6 weeks. | Successful breastfeeding | 1- |
| Schreck et al. [34] (2017) USA | Pre-/Post- quasi- experimental | To measure the effect of hospital-based prenatal and postnatal breastfeeding interventions on breastfeeding initiation and continuation rates in a low-income population. | Participants: 650 women. Baseline group n = 330 Post-intervention group n = 320 Age ≥ 18 years old | The prenatal intervention consisted of a breastfeeding-focused prenatal education curriculum offered one-on-one by an IBCLC. The postnatal intervention consisted of a breastfeeding support group. | Structured questionnaire Baseline/Post-intervention | Breastfeeding initiation rates were higher in the post-intervention group (p < 0.0001). The mothers in the post-intervention group were significantly more likely to breastfeed (p = 0.027, OR = 1.7) compared with those in the baseline group. The breastfeeding continuation rate at or beyond 6 months did not differ between the baseline and post-intervention groups (p = 0.5), but was greater among women who also participated in the breastfeeding support group compared with those who participated in the prenatal intervention alone. Over 95% of the participating women reported that the support group was influential in their decision to continue breastfeeding. | Successful breastfeeding | 1- |
| Saggurti et al. [30] (2018) India | Pre-post quasi- experimental | To evaluate a behaviour-changing health intervention with women’s Self-Help Groups (SHGs) aimed at promoting healthy maternal and newborn practices among the more socially and economically marginalized groups. | Participants: 545 SHGs Age ≥ 18 years old Eight sessions | The SHGs included eight weekly cycles of participatory behaviour communication using different thematic modules on maternal, neonatal, child health and promoting collectivization processes facilitated by community health facilitators or sahelis. | Structured questionnaire Baseline-12 months | In the IG, a significant difference is observed in terms of EBF compared to the two measurements (p = 0.001); this difference is non-existent in the CG (p = 0.22). EBF showed a statistically significant increase over time for SHGs with health integration than without health integration (p < 0.05). | Successful breastfeeding | 1- |
| Ruducha et al. [38] (2018) India | Observational, Descriptive Cross-sectional and Comparative study | To expand the understanding of village dynamics in India and how first degree social and advice networks, as well as the cognitive perceptions of 185 women who had recently given birth in areas with and without women’s Self-Help Groups (SHGs), affect immediate breastfeeding. | Participants: 185 women Age = 18–43 years old | Social and advice networks, with important messages related to maternal and newborn health, in microfinance organizations of SHGs. The health workers include Accredited Social Health Activist, voluntary village health worker paid for specific tasks, Auxiliary Nurse Midwife | Structured questionnaire | The women in the SHG blocks had a significantly higher proportion of immediate breastfeeding than those in the non-SHG blocks (66.7% vs. 41.5%, p = 0.0010) | Successful breastfeeding | High |
| Lee et al. [35] (2019) Taiwan | Quasi-experimental | To examine the effectiveness of breastfeeding education and peer support groups organized by International Board Certified Lactation Consultants (IBCLCs) | Participants: 214 postpartum women. CG (n = 122): Standard care. IG (n = 92): Standard care and support group. | Peer support groups organized by IBCLCs, with weekly face-to-face meetings. Each group consisted of 8–10 mothers. | Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF) Exclusive breastfeeding rate T1: First week postpartum T2: Sixth week postpartum | Exclusive BMF rate at T1 was high and there was no significant proportion difference between groups (p = 0.11) Exclusive BMF rate at 6 weeks postpartum = CG: 39%, IG: 61% (p = 0.001) | Successful breastfeeding | 1- |
| Hazra et al. [33] (2019) India | Quasi-experimental study | To assess the effects of health behaviour changing interventions through women’s self-help groups (SHGs) on maternal and newborn health behaviours. | Participants: 8865 women. (120 geographic blocks, IG; n = 83 blocks, CG). Age = 15 to 49 years old. | The intervention included maternal and child health information dissemination in SHG meetings by trained peer educators, building community norms for behaviour change through a set of community outreach activities including home visits, community meetings, and community events. | Structured questionnaire Round 1: 2015 Round 2: 2017 | There are statistically significant differences in both groups at BF initiation (p = 0.047), but they were not observed in the duration of EBF (p = 0.697). Regarding socioeconomic differences, in the “Least marginalized” group, no differences were observed in both measurements: (p = 0.93) and (p = 0.19), respectively. However, in the “Most marginalized” group, a difference was observed in breastfeeding initiation (p = 0.001), but it was not observed in EBF (p = 0. 439). | No significant difference | 1- |
| Robinson et al. [39] (2019) USA | Observational, Descriptive, Cross-sectional and comparative study . | To identify the sources of breastfeeding support for mothers who participate in support groups on Facebook, and to explore a possible mechanism by which the support received on social network sites leads to behavioural outcomes among breastfeeding mothers. | Participants = 277 Afro-American mothers (from 6 breastfeeding online support groups) Age = 19 to 49 years old. | Support groups on Facebook | Structured questionnaire The Network Support for Breastfeeding (NSB) IOWA Infant Breastfeeding Scale (IFFAS) Breastfeeding Self-Efficacy Scale-Short Form (BFSE-SF) | Compared with other support sources, Facebook was valued with a mean score of 2.7 (± 0.38), compared to health care provider support, 2.3 (± 0.74) and spouse support, 2.0 (± 0.78), among others. There were statistically significant differences between the Facebook online support groups and non-Facebook support in terms of the intention of BF duration, perceived self-efficacy and BF attitudes (p < 0.05) | Successful breastfeeding | High |
| M’Liria et al. [31] (2020) Kenya | A cluster randomized controlled trial | To assess the impact of Mother-to-Mother Support Groups on the promotion of exclusive breastfeeding. | Participants = 249 women (Three study groups) IG1: Breastfeeding education and support during seven monthly meetings (MES) IG2: IG1 Intervention + Income generating activities (MESIGA) | Breastfeeding information and support. At each meeting, one topic on breastfeeding was discussed in a session moderated by a trained facilitator. Groups of at most 15 mothers each to facilitate easy sharing of breastfeeding information and mutual support. | Structured questionnaire (WHO/ UNICEF) Baseline- Monthly at 6 months postpartum | The women in the MES and MESIGA groups were twice as likely to exclusively breastfeed at 6 months compared to those in the control group [RR = 2.42; CI = 1.36–4.28; (p = 0.004)] and [RR = 1.89; CI = 1.02-3.49; (p = 0.033)], respectively. Cumulative EBF was significantly shorter at 0.7 (± 0.15) months in the CG compared to the mean duration of EBF for mothers in the MES (2.8 months) and MESIGA (3.4 months) groups (p = 0.001) | Successful breastfeeding | 1+ |
| Jenkins et al. [40] (2020) USA | Observational, Descriptive, Cross-sectional and comparative study | To evaluate the “Baby Café” program as a support instrument for breastfeeding. | Participants: 559 women. Melrose Baby Café San Antonio Baby Café | Peer support coupled with professional breastfeeding care (IBCLC) or oversight by an IBCLC when the cafe is staffed with alternative approved breastfeeding counsellors. Regular weekly sessions offering comfortable informal seating, breastfeeding positive messaging and snacks. | Structured questionnaire Baseline–6 months–12 months | Exclusive BMF assistant in Baby Café: 77% (Melrose)/ 52% (San Antonio) at 3 months, 71% (Melrose)/47% (San Antonio) at 6 months. Comparative: 47% at 3 months, 25% at 6 months. Any breastfeeding at 12 months: 67% (Melrose)/56% (San Antonio). Comparative: 36%. | Successful breastfeeding | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Gallego, I.; Leon-Larios, F.; Corrales-Gutierrez, I.; González-Sanz, J.D. Impact and Effectiveness of Group Strategies for Supporting Breastfeeding after Birth: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 2550. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052550
Rodríguez-Gallego I, Leon-Larios F, Corrales-Gutierrez I, González-Sanz JD. Impact and Effectiveness of Group Strategies for Supporting Breastfeeding after Birth: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(5):2550. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052550
Chicago/Turabian StyleRodríguez-Gallego, Isabel, Fatima Leon-Larios, Isabel Corrales-Gutierrez, and Juan Diego González-Sanz. 2021. "Impact and Effectiveness of Group Strategies for Supporting Breastfeeding after Birth: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 5: 2550. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052550