
A Mixed-Methods Evaluation of Parent-Assisted Children’s Friendship Training to Improve Social Skills and Friendship Quality in Children with Autism in Malaysia


 ,
, 

Abstract
:1. Introduction
Parent-Assisted Friendship Training for Friendship Quality and Social Skills of Children with ASD
- RQ1:
- What are the roles of parent-assisted CFT for friendship quality?
- RQ2:
- Does parents’ CFT affect the social skills of children with ASD?
2. Materials and Methods
2.1. Participants
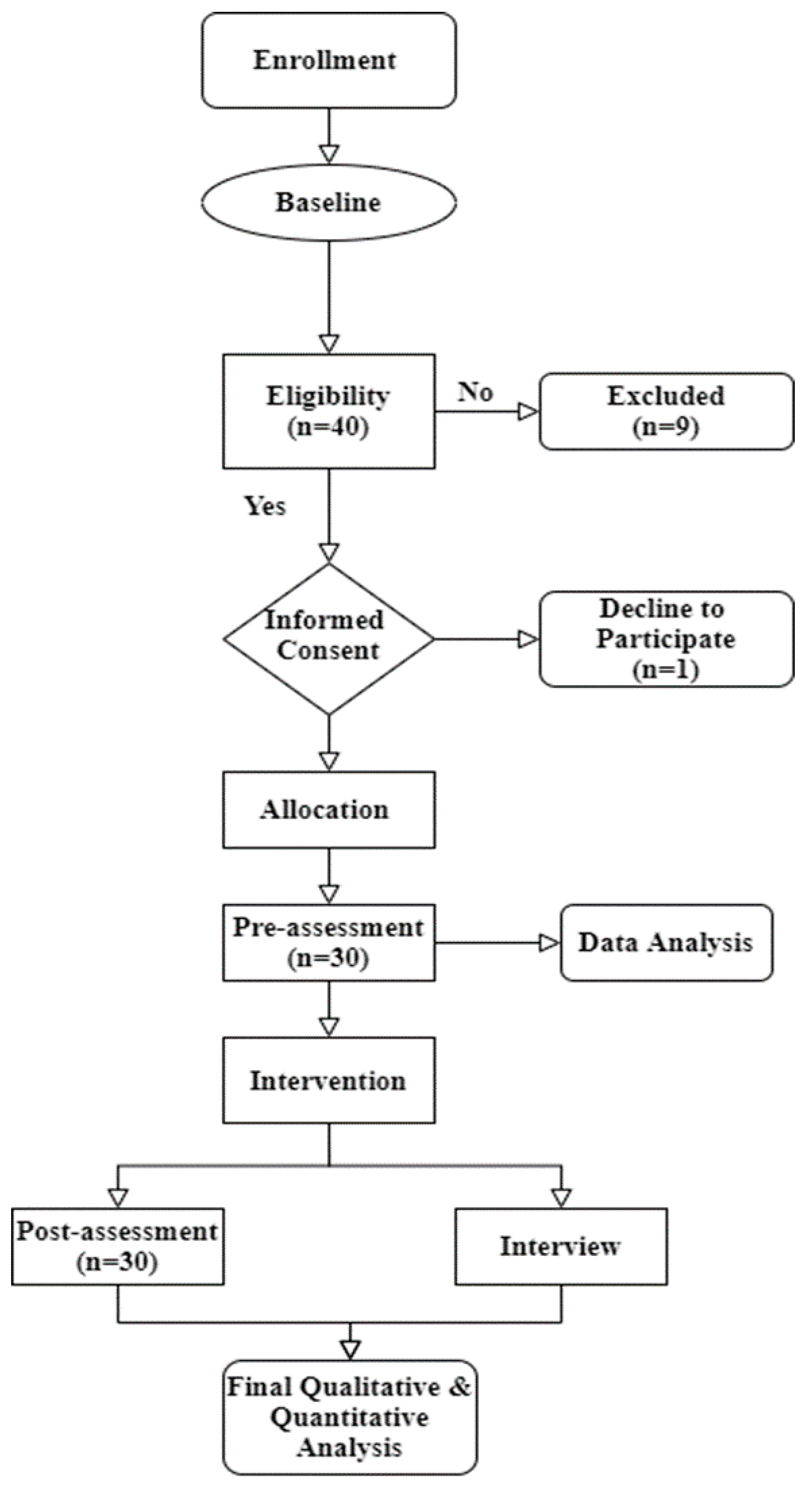
2.2. Study Design
2.3. Variables and Hypotheses
2.4. Intervention
2.5. Experimental Procedure
- (1)
- Parent room: The room should have a large table and enough space for all parents to be seated together at the same time.
- (2)
- Child room: The room should have whiteboards, tables, and chairs for children to sit in.
- (3)
- Play deck: The outside play area is used to teach skills for outdoor games and should resemble a schoolyard, as much as possible.
2.6. Measures
2.6.1. Socio-Demographic Information
2.6.2. Quantitative Evaluation of Program Perceptions
2.7. Qualitative Data
2.8. Ethical Aspect
2.9. Protection of Human Subjects
2.10. Data Collection
2.11. Data analysis
3. Results
3.1. Descriptive Analysis
3.2. Results of Quantitative Data
3.3. Results of Semi-Structured Interviews
4. Discussion
5. Conclusions
5.1. Implications of the Study
5.2. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hyman, S.L.; Levy, S.E.; Myers, S.M. Identification, Evaluation, and Management of Children with Autism Spectrum Disorder. Pediatrics 2020, 145, 1–45. [Google Scholar] [CrossRef] [Green Version]
- White, S.W.; Koenig, K.; Scahill, L. Group Social Skills Instruction for Adolescents with High-Functioning Autism Spectrum Disorders. Focus Autism Other Dev. Disabil. 2010, 25, 209–219. [Google Scholar] [CrossRef]
- Taresh, S.; Ahmad, N.A.; Roslan, S.; Ma’Rof, A.M.; Zaid, S. Pre-School Teachers’ Knowledge, Belief, Identification Skills, and Self-Efficacy in Identifying Autism Spectrum Disorder (ASD): A Conceptual Framework to Identify Children with ASD. Brain Sci. 2020, 10, 165. [Google Scholar] [CrossRef] [Green Version]
- Neik, T.T.X.; Lee, L.W.; Low, H.M.; Chia, N.K.H.; Chua, A.C.K. Prevalence, Diagnosis, Treatment and Research on Autism Spectrum Disorders (ASD) in Singapore and Malaysia. Int. J. Spec. Educ. 2014, 29, 82–92. [Google Scholar]
- McConnell, S.R. Interventions to Facilitate Social Interaction for Young Children with Autism: Review of Available Research and Recommendations for Educational Intervention and Future Research. J. Autism Dev. Disord. 2002, 32, 351–372. [Google Scholar] [CrossRef]
- Hayden, E.P.; Mash, E.J. Child Psychopathology: A Developmental-Systems Perspective. In Child Psychopathology; Mash, E.J., Barkley, R.A., Eds.; The Guilford Press: New York, NY, USA, 2014. [Google Scholar]
- Rumney, H.L.; MacMahon, K. Do Social Skills Interventions Positively Influence Mood in Children and Young People with Autism? A Systematic Review. Ment. Health Prev. 2017, 5, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Locke, J.; Ishijima, E.H.; Kasari, C.; London, N. Loneliness, Friendship Quality and the Social Networks of Adolescents with High-Functioning Autism in an Inclusive School Setting. J. Res. Spec. Educ. Needs 2010, 10, 74–81. [Google Scholar] [CrossRef]
- Schonfeld, A.M.; Mattson, S.N.; Riley, E.P. Moral Maturity and Delinquency after Prenatal Alcohol Exposure. J. Stud. Alcohol 2005, 66, 545–554. [Google Scholar] [CrossRef]
- Wolstencroft, J.; Robinson, L.; Srinivasan, R.; Kerry, E.; Mandy, W.; Skuse, D. A Systematic Review of Group Social Skills Interventions, and Meta-Analysis of Outcomes, for Children with High Functioning ASD. J. Autism Dev. Disord. 2018, 48, 2293–2307. [Google Scholar] [CrossRef] [Green Version]
- Goh, H.S.E.; Roslan, S.; Baguri, E.M.; Ong, S.Y.; Li, S.Y. The Effects of Children’s Friendship Training on Social Skills and Quality of Play among Children with Autism Spectrum Disorder. Int. J. Learn. Teach. Educ. Res. 2020, 19, 225–245. [Google Scholar]
- Sigman, M.; Ruskin, E.; Arbelle, S.; Corona, R.; Dissanayake, C.; Espinosa, M.; Kim, N.; López, A.; Zierhut, C.; Mervis, C.B. Continuity and Change in the Social Competence of Children with Autism, Down Syndrome, and Developmental Delays. Monogr. Soc. Res. Child Dev. 1999, 64, 115–130. [Google Scholar]
- Bellini, S.; Akullian, J. A Meta-Analysis of Video Modeling and Video Self-Modeling Interventions for Children and Adolescents with Autism Spectrum Disorders. Except. Child. 2007, 73, 264–287. [Google Scholar] [CrossRef]
- Healy, S.; Nacario, A.; Braithwaite, R.E.; Hopper, C. The Effect of Physical Activity Interventions on Youth with Autism Spectrum Disorder: A Meta-Analysis. Autism Res. 2018, 11, 818–833. [Google Scholar] [CrossRef] [PubMed]
- Silverman, L.B.; Eigsti, I.-M.; Bennetto, L. I Tawt i Taw a Puddy Tat: Gestures in Canary Row Narrations by High-Functioning Youth with Autism Spectrum Disorder. Autism Res. 2017, 10, 1353–1363. [Google Scholar] [CrossRef]
- Frankel, F.; Myatt, R. Children’s Friendship Training; Brunner-Routledge: New York, NY, USA, 2003. [Google Scholar]
- Ashman, R.; Banks, K.; Philip, R.C.; Walley, R.; Stanfield, A.C. A Pilot Randomised Controlled Trial of a Group Based Social Skills Intervention for Adults with Autism Spectrum Disorder. Res. Autism Spectr. Disord. 2017, 43, 67–75. [Google Scholar] [CrossRef]
- Oono, I.P.; Honey, E.J.; McConachie, H. Parent-Mediated Early Intervention for Young Children with Autism Spectrum Disorders (ASD). Evid. Based Child Health Cochrane Rev. J. 2013, 8, 2380–2479. [Google Scholar] [CrossRef]
- Ingersoll, B.R.; Wainer, A.L. Pilot Study of a School-Based Parent Training Program for Preschoolers with ASD. Autism 2013, 17, 434–448. [Google Scholar] [CrossRef]
- Kasari, C.; Gulsrud, A.; Paparella, T.; Hellemann, G.; Berry, K. Randomized Comparative Efficacy Study of Parent-Mediated Interventions for Toddlers with Autism. J. Consult. Clin. Psychol. 2015, 83, 554–563. [Google Scholar] [CrossRef]
- Wetherby, A.M.; Guthrie, W.; Woods, J.; Schatschneider, C.; Holland, R.D.; Morgan, L.; Lord, C. Parent-Implemented Social Intervention for Toddlers with Autism: An RCT. Pediatrics 2014, 134, 1084–1093. [Google Scholar] [CrossRef] [Green Version]
- Green, J.; Charman, T.; McConachie, H.; Aldred, C.; Slonims, V.; Howlin, P.; Le Couteur, A.; Leadbitter, K.; Hudry, K.; Byford, S. Parent-Mediated Communication-Focused Treatment in Children with Autism (PACT): A Randomised Controlled Trial. Lancet 2010, 375, 2152–2160. [Google Scholar] [CrossRef] [Green Version]
- Oosterling, I.; Visser, J.; Swinkels, S.; Rommelse, N.; Donders, R.; Woudenberg, T.; Roos, S.; van der Gaag, R.J.; Buitelaar, J. Randomized Controlled Trial of the Focus Parent Training for Toddlers with Autism: 1-Year Outcome. J. Autism Dev. Disord. 2010, 40, 1447–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karst, J.S.; van Hecke, A.V. Parent and Family Impact of Autism Spectrum Disorders: A Review and Proposed Model for Intervention Evaluation. Clin. Child Fam. Psychol. Rev. 2012, 15, 247–277. [Google Scholar] [CrossRef]
- Sofronoff, K.; Farbotko, M. The Effectiveness of Parent Management Training to Increase Self-Efficacy in Parents of Children with Asperger Syndrome. Autism 2002, 6, 271–286. [Google Scholar] [CrossRef] [PubMed]
- Tonge, B.; Brereton, A.; Kiomall, M.; Mackinnon, A.; King, N.; Rinehart, N. Effects on Parental Mental Health of an Education and Skills Training Program for Parents of Young Children with Autism: A Randomized Controlled Trial. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Barnett, J.H. Three Evidence-Based Strategies That Support Social Skills and Play among Young Children with Autism Spectrum Disorders. Early Child. Educ. J. 2018, 46, 665–672. [Google Scholar] [CrossRef]
- Moore-Dean, A.; Renwick, R.; Schormans, A.F. Friendship Characteristics of Children with Intellectual/Developmental Disabilities: Qualitative Evidence from Video Data. J. Dev. Disabil. 2016, 22, 39. [Google Scholar]
- APA DSM-IV-TR. Available online: www.google.com/search?sxsrf=ALeKk01_3oiSEvkaoM8lntWUfNlEHvpF5A%3A1612833197011&ei=reEhYNAJ-b_ctQ_T2KLoCA&q=dsm-iv-tr+%28apa+2000%29&oq=DSM-IV-TR+%28APA%2C+2000%29&gs_lcp=CgZwc3ktYWIQARgAMgYIABAWEB4yBggAEBYQHlCq3QNYqt0DYNf4A2gAcAJ4AIAB2gqIAdQNkgEHMy0xLjctMZgBAKABAqABAaoBB2d3cy13aXrAAQE&sclient=psy-ab (accessed on 9 February 2021).
- APA DSM-5. Available online: www.google.com/search?q=DSM-5+(APA%2C+2013)&oq=DSM-5+(APA%2C+2013)&aqs=chrome..69i57j46j0i22i30l4.1879j0j7&sourceid=chrome&ie=UTF-8 (accessed on 9 February 2021).
- Raven, J.C.; Court, J.H. Raven Matrices Progresivas. CPM-SPM-APM. Manual; TEA: Madrid, Spain, 1996.
- Mertens, D.M. Mixed Methods and the Politics of Human Research: The Transformative Emancipatory Perspective. In Handbook of Mixed Methods in Social and Behavioral Research; Tashakkor, A., Teddlie, C., Eds.; Sage: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Price, P.C.; Jhangiani, R.S.; Chiang, I.A.; Leighton, D.C.; Cuttler, C. Research Methods in Psychology, 3rd ed.; Washington State University: Pullman, WA, USA, 2017. [Google Scholar]
- Alzyoudi, M.; Sartawi, A.; Almuhiri, O. The Impact of Video Modelling on Improving Social Skills in Children with Autism. Br. J. Spec. Educ. 2015, 42, 53–68. [Google Scholar] [CrossRef]
- Nevin, J.A.; Grace, R.C. Behavioral Momentum and the Law of Effect. Behav. Brain Sci. 2000, 23, 73–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gresham, F.M.; Elliot, S.N. Manual for the Social Skills Rating System; American Guidance Service: Circle Pines, MN, USA, 1990. [Google Scholar]
- Frankel, F.; Mintz, J. Measuring the Quality of Play Dates; UCLA Parenting and Children’s Friendship Program, UCLA Jane & Terry Semel Institute for Neuroscience & Human Behavior: Los Angeles, CA, USA, 2008. [Google Scholar]
- Schmidt, C. The Analysis of Semi-Structured Interviews. In A Companion to Qualitative Research; Flick, U., von Kardorff, E., Steinke, I., Eds.; Sage: Thousand Oaks, CA, USA, 2004; pp. 253–258. [Google Scholar]
- First, M.B. Structured Clinical Interview for the DSM (SCID). In The Encyclopedia of Clinical Psychology; Wiley: Hoboken, NJ, USA, 2014; pp. 1–6. [Google Scholar]
- Lindseth, A.; Norberg, A. A Phenomenological Hermeneutical Method for Researching Lived Experience. Scand. J. Caring Sci. 2004, 18, 145–153. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Frankel, F.; Myatt, R.; Feinberg, D. Parent-Assisted Friendship Training for Children with Autism Spectrum Disorders: Effects of Psychotropic Medication. Child Psychiatry Hum. Dev. 2007, 37, 337–346. [Google Scholar] [CrossRef]
- Mandelberg, J.; Laugeson, E.A.; Cunningham, T.D.; Ellingsen, R.; Bates, S.; Frankel, F. Long-Term Treatment Outcomes for Parent-Assisted Social Skills Training for Adolescents with Autism Spectrum Disorders: The UCLA PEERS Program. J. Ment. Health Res. Intellect. Disabil. 2014, 7, 45–73. [Google Scholar] [CrossRef]
- Dekker, V.; Nauta, M.H.; Mulder, E.J.; Timmerman, M.E.; de Bildt, A. A Randomized Controlled Study of a Social Skills Training for Preadolescent Children with Autism Spectrum Disorders: Generalization of Skills by Training Parents and Teachers? BMC Psychiatry 2014, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Adams, R.E.; Santo, J.B.; Bukowski, W.M. The Presence of a Best Friend Buffers the Effects of Negative Experiences. Dev. Psychol. 2011, 47, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnall, C.A. Managing Change in Organizations, 6th ed.; Pearson Education: New York, NY, USA, 2014. [Google Scholar]
- Teo, J.X.; Lau, B.T. Parental Perceptions, Attitudes and Involvement in Interventions for Autism Spectrum Disorders in Sarawak, Malaysia. Disabil. CBR Incl. Dev. 2018, 29, 26–46. [Google Scholar] [CrossRef] [Green Version]
- Moroz, A. Exploring the Factors Related to Parent Involvement in the Interventions of Their Children with Autism. Master’s Thesis, California State University, Sacramento, CA, USA, 2015. [Google Scholar]
- Tully, L.A.; Piotrowska, P.J.; Collins, D.A.; Mairet, K.S.; Black, N.; Kimonis, E.R.; Hawes, D.J.; Moul, C.; Lenroot, R.K.; Frick, P.J. Optimising Child Outcomes from Parenting Interventions: Fathers’ Experiences, Preferences and Barriers to Participation. BMC Public Health 2017, 17, 1–14. [Google Scholar] [CrossRef]
- Piškur, B.; Beurskens, A.J.; Jongmans, M.J.; Ketelaar, M.; Norton, M.; Frings, C.A.; Hemmingsson, H.; Smeets, R.J. Parents’ Actions, Challenges, and Needs While Enabling Participation of Children with a Physical Disability: A Scoping Review. BMC Pediatrics 2012, 12, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keshavarz, S.; Baharudin, R. Perceived Parenting Style of Fathers and Adolescents’ Locus of Control in a Collectivist Culture of Malaysia: The Moderating Role of Fathers’ Education. J. Genet. Psychol. 2013, 174, 253–270. [Google Scholar] [CrossRef]
- Triandis, H.C. Collectivism: Cultural Concerns. In International Encyclopedia of the Social & Behavioral Sciences; Elsevier: Amsterdam, The Netherlands, 2001; pp. 2227–2232. [Google Scholar]
- Algood, C.L.; Harris, C.; Hong, J.S. Parenting Success and Challenges for Families of Children with Disabilities: An Ecological Systems Analysis. J. Hum. Behav. Soc. Environ. 2013, 23, 126–136. [Google Scholar] [CrossRef]
- Hall, H.R.; Graff, J.C. Parenting Challenges in Families of Children with Autism: A Pilot Study. Issues Compr. Pediatric Nurs. 2010, 33, 187–204. [Google Scholar] [CrossRef]


{kind=link}
| N (%) | N (%) | N (%) | N (%) | ||||
|---|---|---|---|---|---|---|---|
| Age | Diagnosis | Pragmatic Language IMPAIRMENT | Social Communication DISORDER 1 | ||||
| 7 | 8 (26.6) | ASD | 17 (56.66) | Receptive language disorder | Difficulties in Interpersonal communication 2 | ||
| 8 | 10 (33.33) | ASD, ADD | 1 (3.33) | Mild | 0 | Mild | 2 (6.6) |
| 9 | 5 (16.66) | ASD, ADHD | 1 (3.36) | Moderate | 18 (60) | Moderate | 27 (90) |
| 10 | 2 (6.66) | Asperger Syndrome | 1 (3.36) | Severe | 12 (40) | Severe | 1 (3.4) |
| 11 | 2 (6.66) | Asperger Syndrome, ADHD | 1 (3.36) | Expressive language disorder | Difficulties in social initiation and response | ||
| 12 | 3 (10) | GDD | 1 (3.36) | Mild | 2 (6.66) | Mild | 16 (53.34) |
| School Type | GDD, ADHD | 3 (10) | Moderate | 17 (56.66) | Moderate | 12 (40) | |
| Government School (Sekolah Harian) | 13 (43.4) | PDD- NOS | 5 (16.66) | Severe | 11 (36.66) | Severe | 2 (6.66) |
| Government School (PPKI) | 6 (20) | Degree of Autism | Written expression disorder | Social interaction skills deficits | |||
| Home School Center | 6 (20) | Mild | 1 (3.3) | Mild | 6 (20) | Mild | 2 (6.66) |
| International Primary School | 3 (10) | Moderate | 27 (90) | Moderate | 20 (66.6) | Moderate | 23 (76.66) |
| Private Primary School | 2 (6.6) | Severe | 2 (6.6) | Severe | 4 (13.4) | Severe | 5 (16.66) |
| N (%) | N (%) | ||
|---|---|---|---|
| Parents Race/Ethnicity | SPM | 3 (10.00) | |
| Malay | 7 (23.33) | Parent Occupation | |
| Chinese | 17 (56.67) | Professional | 16 (53.33) |
| Indian | 6 (20) | Business | 3 (10) |
| Parent Religion | Housemaker | 11 (36.67) | |
| Muslim | 7 (23.33) | Parents’ Marital Status | |
| Buddhism | 14 (46.67) | Married—living together | 28 (93.33) |
| Christian | 4 (13.33) | Single—divorced—separated | 2 (6.67) |
| Hindu | 5 (16.67) | Parents’ Income | |
| Parents’ Education Level | Low (less than RM4360) | 11 (36.67) | |
| Postgraduate | 7 (23.33) | Medium (RM 4360-RM9618) | 11 (36.67) |
| Degree | 16 (53.33) | High (More than RM 9618) | 8 (26.67) |
| Diploma | 4 (13.33) |
| Timepoint | Enrollment | Baseline | CFT Intervention | |||
|---|---|---|---|---|---|---|
| −1 | 0 | Within 12 Weeks Follow up | ||||
| Enrolment | ||||||
| Eligibility screen | ✖ | |||||
| Informed consent | ✖ | |||||
| Allocation | ||||||
| Interventions |  | |||||
| Assessment | ||||||
| Demographic | ✖ | ✖ | ||||
| SSiS-RS | ✖ | ✖ | ||||
| QPQ | ✖ | ✖ | ||||
| Interview | ✖ | |||||
| Construct | Pre-Intervention | Post-Intervention | t | df | p-Value | Cohen’s d | ||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||||
| Social Skill | 70.70 | 12.804 | 79.40 | 4.97 | −2.7 | 29 | 0.011 a | 1.000 |
| Quality Friendship | ||||||||
| Friendship—Engage | 5.53 | 2.776 | 5.60 | 2.238 | −0.138 | 29 | 0.891 | 0.98 |
| Friendship—Disengage | 5.33 | 2.279 | 2.97 | 2.810 | 4.974 | 29 | 0.000 b | 1.21 |
| Friendship—Conflict | 9.57 | 5.302 | 4.93 | 4.799 | 4.328 | 29 | 0.000 b | 0.99 |
| Theme | Sub-Theme |
|---|---|
| Fear and resistance |
|
| Awareness, learning, and adjustment |
|
| Change is not easy |
|
| Identifying support |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ong, S.Y.; Roslan, S.; Ahmad, N.A.; Ayub, A.F.M.; Ping, C.L.; Zaremohzzabieh, Z.; Ahrari, S. A Mixed-Methods Evaluation of Parent-Assisted Children’s Friendship Training to Improve Social Skills and Friendship Quality in Children with Autism in Malaysia. Int. J. Environ. Res. Public Health 2021, 18, 2566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052566
Ong SY, Roslan S, Ahmad NA, Ayub AFM, Ping CL, Zaremohzzabieh Z, Ahrari S. A Mixed-Methods Evaluation of Parent-Assisted Children’s Friendship Training to Improve Social Skills and Friendship Quality in Children with Autism in Malaysia. International Journal of Environmental Research and Public Health. 2021; 18(5):2566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052566
Chicago/Turabian StyleOng, Sing Yee, Samsilah Roslan, Nor Aniza Ahmad, Ahmad Fauzi Mohd Ayub, Chen Lee Ping, Zeinab Zaremohzzabieh, and Seyedali Ahrari. 2021. "A Mixed-Methods Evaluation of Parent-Assisted Children’s Friendship Training to Improve Social Skills and Friendship Quality in Children with Autism in Malaysia" International Journal of Environmental Research and Public Health 18, no. 5: 2566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052566