
Occupational Exposure in the Lombardy Region (Italy) to SARS-CoV-2 Infection: Results from the MUSTANG–OCCUPATION–COVID-19 Study


 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
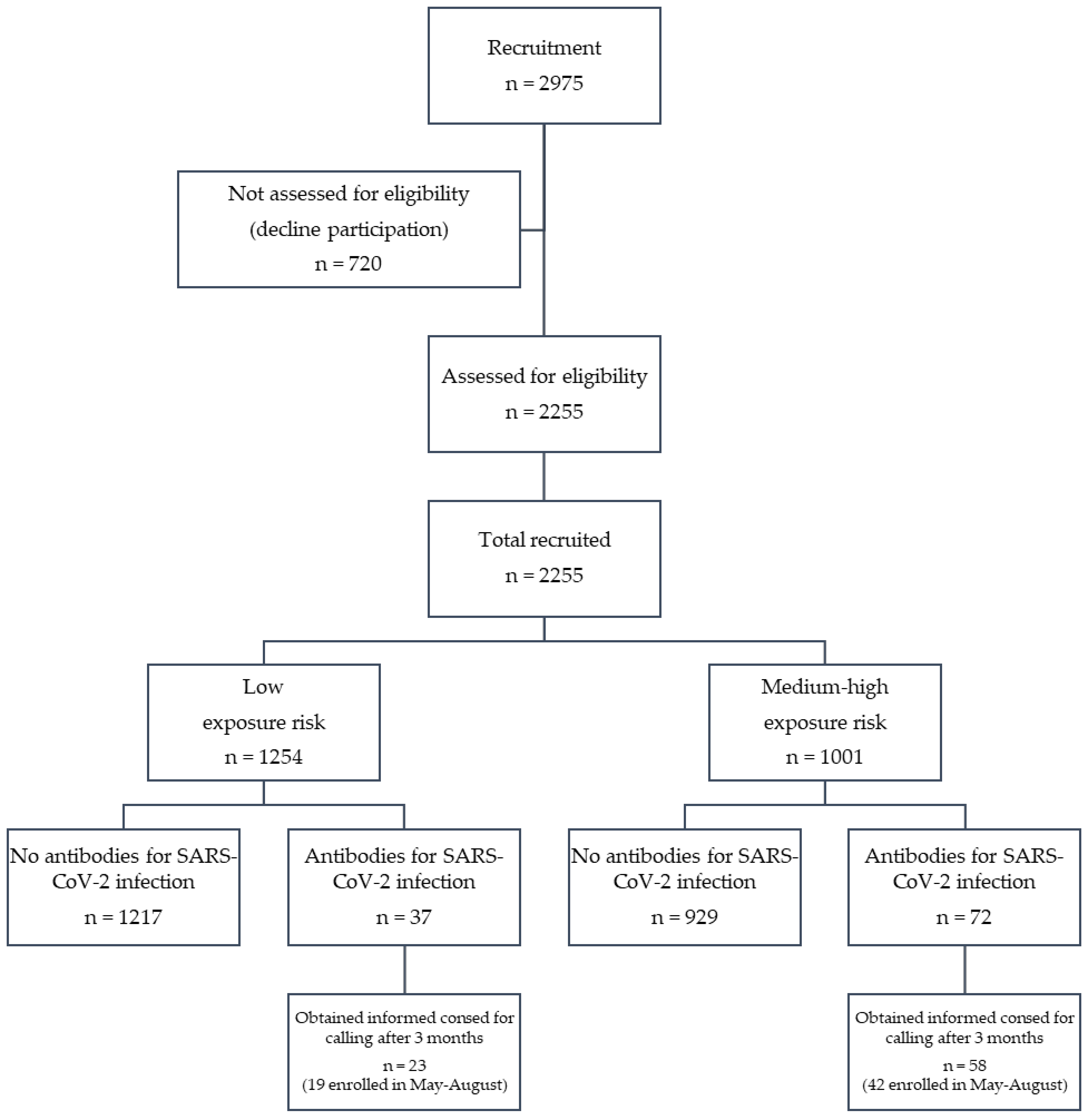
2.1. Study Design and Population
2.2. Endpoints
2.3. Data Definitions
2.4. Sample Size
2.5. Study Procedures
2.6. Statistical Analysis
2.7. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Study Population N = 2255 | |
|---|---|
| Age, n (%) | 0 (0.00) |
| Sex (male), n (%) | 0 (0.00) |
| Enrollment period, n (%) | 0 (0.00) |
| SARS-CoV-2 risk exposure, n (%) | 0 (0.00) |
| Municipality, n (%) | 12 (0.5) |
| Job description, n (%) | 0 (0.00) |
| Work type during lockdown period, n (%) | 8 (0.4) |
| Smoking habit, n (%) | 6 (0.3) |
| Chronic diseases, n (%) | 0 (0.00) |
| Chronic pharmacological therapies, n (%) | 0 (0.00) |
| Vaccinations | 0 (0.00) |
| Clinical parameters, n %) | |
| SpO2 (%) | 31 (1.4%) |
| Systolic blood pressure | 24 (1.1%) |
| Diastolic blood pressure | 22 (1.0%) |
| Heart rate | 12 (0.5%) |
| Body temperature | 16 (0.7%) |
| Symptoms COVID-19, n (%) | 0 (0.00) |
| Antibody test for SARS-CoV-2 infection, n (%) | |
| IgG | 0 (0.00) |
| IgM | 0 (0.00) |
References
- Dipartimento della Protezione Civile. COVID-19 Italia—Monitoraggio della situazione. Available online: www.opendatadpc.maps.arcgis.com/apps/opsdashboard/index.html#/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 26 January 2021).
- Ferrara, P.; Albano, L. COVID-19 and healthcare systems: What should we do next? Public Health 2020, 185, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Conti, S.; Ferrara, P.; Fornari, C.; Harari, S.; Madotto, F.; Silenzi, A.; Zucchi, A.; Manzoli, L.; Mantovani, L.G. Estimates of the initial impact of COVID-19 epidemic on overall mortality: Evidence from Italy. ERJ Open Res. 2020, 6, 00179–2020. [Google Scholar] [CrossRef] [PubMed]
- Balasco, N.; d’Alessandro, V.; Ferrara, P.; Smaldone, G.; Vitagliano, L. Analysis of the time evolution of COVID-19 lethality during the first epidemic wave in Italy. Acta Biomed 2021, 92. in press. [Google Scholar]
- Conti, S.; Ferrara, P.; Mazzaglia, G.; D’Orso, M.I.; Ciampichini, R.; Fornari, C.; Madotto, F.; Magoni, M.; Sampietro, G.; Silenzi, A.; et al. Magnitude and time-course of excess mortality during COVID-19 outbreak: Population-based empirical evidence from highly impacted provinces in northern Italy. ERJ Open Res. 2020, 6, 00458–2020. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; de Larrea, N.F.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, P535–P544. [Google Scholar] [CrossRef]
- Bertuzzo, E.; Mari, L.; Pasetto, D.; Miccoli, S.; Casagrandi, R.; Gatto, M.; Rinaldo, A. The geography of COVID-19 spread in Italy and implications for the relaxation of confinement measures. Nat. Commun. 2020, 11, 4264. [Google Scholar] [CrossRef]
- Sakurai, A.; Sasaki, T.; Kato, S.; Hayashi, M.; Tsuzuki, S.I.; Ishihara, T.; Iwata, M.; Morise, Z.; Doi, Y. Natural history of asymptomatic SARS-CoV-2 infection. N. Engl. J. Med. 2020, 383, 885–886. [Google Scholar] [CrossRef] [PubMed]
- Hung, I.F.N.; Cheng, V.C.C.; Li, X.; Tam, A.R.; Hung, D.L.L.; Chiu, K.H.Y.; Yip, C.C.Y.; Cai, J.P.; Ho, D.T.Y.; Wong, S.C.; et al. SARS-CoV-2 shedding and seroconversion among passengers quarantined after disembarking a cruise ship: A case series. Lancet Infect. Dis. 2020, 20, 1051–1060. [Google Scholar] [CrossRef]
- Hallal, P.C.; Hartwig, F.P.; Horta, B.L.; Silveira, M.F.; Struchiner, C.J.; Vidaletti, L.P.; Neumann, N.A.; Pellanda, L.C.; Dellagostin, O.A.; Burattini, M.N.; et al. SARS-CoV-2 antibody prevalence in Brazil: Results from two successive nationwide serological household surveys. Lancet Global Health 2020, 8, E1390–E1398. [Google Scholar] [CrossRef]
- Istituto Nazionale di Statistica (ISTAT). Primi risultati dell’indagine di sieroprevalenza SARS-CoV-2. Available online: https://www.istat.it/it/files/2020/08/ReportPrimiRisultatiIndagineSiero.pdf (accessed on 6 January 2021).
- Sim, M.R. The COVID-19 pandemic: Major risks to healthcare and other workers on the front line. Occup. Environ. Med. 2020, 77, 281–282. [Google Scholar] [CrossRef] [Green Version]
- Belingheri, M.; Paladino, M.E.; Riva, M.A. COVID-19: Health prevention and control in non-healthcare settings. Occup. Environ. Med. 2020, 70, 82–83. [Google Scholar] [CrossRef] [Green Version]
- Vena, A.; Berruti, M.; Adessi, A.; Blumetti, P.; Brignole, M.; Colognato, R.; Gaggioli, G.; Giacobbe, D.R.; Bracci-Laudiero, L.; Magnasco, L.; et al. Prevalence of Antibodies to SARS-CoV-2 in Italian Adults and Associated Risk Factors. J. Clin. Med. 2020, 9, 2780. [Google Scholar] [CrossRef] [PubMed]
- Plebani, M.; Padoan, A.; Fedeli, U.; Schievano, E.; Vecchiato, E.; Lippi, G.; Cascio, G.L.; Porru, S.; Palù, G. SARS-CoV-2 serosurvey in health care workers of the Veneto Region. Clin. Chem. Lab. Med. 2020, 58, 2107–2111. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Basteiro, A.L.; Moncunill, G.; Tortajada, M.; Vidal, M.; Guinovart, C.; Jimenez, A.; Santano, R.; Sanz, S.; Méndez, S.; Llupià, A.; et al. Seroprevalence of antibodies against SARS-CoV-2 among health care workers in a large Spanish reference hospital. Nat. Commun. 2020, 11, 3500. [Google Scholar] [CrossRef] [PubMed]
- Marinaccio, A.; Boccuni, F.; Rondinone, B.M.; Brusco, A.; D’Amario, S.; Iavicoli, S. Occupational factors in the COVID-19 pandemic in Italy: Compensation claims applications support establishing an occupational surveillance system. Occup. Environ. Med. 2020, 77, 818–821. [Google Scholar] [CrossRef]
- Cereda, D.; Tirani, M.; Rovida, F.; Demicheli, V.; Ajelli, M.; Poletti, P.; Trentini, F.; Guzzetta, G.; Marziano, V.; Barone, A.; et al. The early phase of the COVID-19 outbreak in Lombardy, Italy. arXiv 2020, arXiv:2003.09320. [Google Scholar]
- Technogenetics SRL. TGS COVID-19 IgG—Istruzioni per l’uso. REF CVCL100G. IFU105TGS—Versione: 03_IT—17 giugno 2020; Technogenetics SRL: Milano, Italy, 2020. [Google Scholar]
- Technogenetics SRL. TGS COVID-19 IgM—Istruzioni per l’uso. REF CVCL100M. IFU107TGS—Versione: 05_IT—23 settembre 2020; Technogenetics SRL: Milano, Italy, 2020. [Google Scholar]
- Technogenetics SRL. TGS COVID-19 Control Set—Istruzioni per l’uso. REF CVCLCSGM. IFU106TGS—Versione: 03A_IT—07 luglio 2020; Technogenetics SRL: Milano, Italy, 2020. [Google Scholar]
- Moderbacher, C.R.; Ramirez, S.I.; Dan, J.M.; Grifoni, A.; Hastie, K.M.; Weiskopf, D.; Belanger, S.; Abbott, R.K.; Kim, C.; Choi, J.; et al. Antigen-Specific Adaptive Immunity to SARS-CoV-2in Acute COVID-19 and Associationswith Age and Disease Severity. Cell 2020, 183, 996–1012. [Google Scholar] [CrossRef] [PubMed]
- Stock, A.D.; Bader, E.R.; Cezayirli, P.; Inocencio, J.; Chalmers, S.A.; Yassari, R.; Yanamadala, V.; Eskandar, E. COVID-19 Infection Among Healthcare Workers: Serological Findings Supporting Routine Testing. Front. Med. 2020, 7, 471. [Google Scholar] [CrossRef]
- Moscola, J.; Sembajwe, G.; Jarrett, M.; Farber, B.; Chang, T.; McGinn, T.; Davidson, K.W.; Northwell Health COVID-19 Research Consortium. Prevalence of SARS-CoV-2 Antibodies in Health Care Personnel in the New York City Area. JAMA 2020, 324, 893–895. [Google Scholar] [CrossRef]
- Iversen, K.; Bundgaard, H.; Hasselbalch, R.B.; Kristensen, J.H.; Nielsen, P.B.; Pries-Heje, M.; Knudsen, A.D.; Christensen, C.E.; Fogh, K.; Norsk, J.B.; et al. Risk of COVID-19 in health-care workers in Denmark: An observational cohort study. Lancet Inf. Dis. 2020, 20, P1401–P1408. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità. COVID-19 Integrated Surveillance Data in Italy. Available online: https://www.epicentro.iss.it/en/coronavirus/sars-cov-2-dashboard (accessed on 21 January 2021).
- Israel, A.; Feldhamer, I.; Lahad, A.; Levin-Zamir, D.; Lavie., G. Smoking and the risk of COVID-19 in a large observational population study. medRxiv 2020, 20118877. [Google Scholar]
- Farsalinos, K.; Barbouni, A.; Niaura, R. Systematic review of the prevalence of current smoking among hospitalized COVID-19 patients in China: Could nicotine be a therapeutic option? Reply. Int. Emerg. Med. 2020, 16, 235–236. [Google Scholar]
- Farsalinos, K.; Barbouni, A.; Niaura, R. Systematic review of the prevalence of current smoking among hospitalized COVID-19 patients in China: Could nicotine be a therapeutic option? Int. Emerg. Med. 2020, 15, 1601–1603. [Google Scholar]
- Farsalinos, K.; Barbouni, A.; Poulas, K.; Polosa, R.; Caponnetto, P.; Niaura, R. Current smoking, former smoking, and adverse outcome among hospitalized COVID-19 patients: A systematic review and meta-analysis. Ther. Adv. Chronic Dis. 2020, 11, 2040622320935765. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.; Rutherford, G.W. Facial Masking for Covid-19—Potential for “Variolation” as We Await a Vaccine. N. Engl. J. Med. 2020, 383, e101. [Google Scholar] [CrossRef] [PubMed]
- Isho, B.; Abe, K.T.; Zuo, M.; Jamal, A.J.; Rathod, B.; Wang, J.H.; Li, Z.; Chao, G.; Rojas, O.L.; Bang, Y.M.; et al. Persistence of serum and saliva antibody responses to SARS-CoV-2 spike antigens in COVID-19 patients. Sci. Immunol. 2020, 5, eabe5511. [Google Scholar]
- Iyer, A.S.; Jones, F.K.; Nodoushani, A.; Kelly, M.; Becker, M.; Slater, D.; Mills, R.; Teng, E.; Kamruzzaman, M.; Garcia-Beltran, W.F.; et al. Persistence and decay of human antibody responses to the receptor binding domain of SARS-CoV-2 spike protein in COVID-19 patients. Sci. Immunol. 2020, 5, eabe0367. [Google Scholar] [CrossRef]
- Ibarrondo, F.J.; Fulcher, J.A.; Goodman-Meza, D.; Elliott, J.; Hofmann, C.; Hausner, M.A.; Ferbas, K.G.; Tobin, N.H.; Aldrovandi, G.M.; Yang, O.O. Rapid Decay of Anti–SARS-CoV-2 Antibodies in Persons with Mild Covid-19. N. Engl. J. Med. 2020, 383, 1085–1087. [Google Scholar] [CrossRef]
- Gudbjartsson, D.F.; Norddahl, G.L.; Melsted, P.; Gunnarsdottir, K.; Holm, H.; Eythorsson, E.; Arnthorsson, A.O.; Helgason, D.; Bjarnadottir, K.; Ingvarsson, R.F.; et al. Humoral Immune Response to SARS-CoV-2 in Iceland. N. Engl. J. Med. 2020, 383, 1724–1734. [Google Scholar] [CrossRef]

| Total | Low Exposure Risk | Medium-High Exposure Risk | p-Value ^ | |
|---|---|---|---|---|
| N (%) | 2255 | 1254 (55.61) | 1001 (44.39) | - |
| Age, mean ± SD | 44.45 ± 9.71 | 45.65 ± 9.58 | 42.94 ± 9.67 | <0.0001 |
| Sex, n (%) | <0.0001 | |||
| Male | 1569 (69.58) | 758 (60.45) | 811 (81.02) | |
| Female | 686 (30.42) | 496 (39.55) | 190 (18.98) | |
| Enrollment period, n (%) | ||||
| May-June | 1263 (56.01) | 824 (65.71) | 439 (43.86) | <0.0001 |
| July-August | 665 (29.29) | 327 (26.08) | 338 (33.77) | <0.0001 |
| September-October | 327 (14.50) | 103 (8.21) | 224 (22.39) | <0.0001 |
| Municipality*, n (%) | ||||
| Province of Milan | 1523 (67.90) | 852 (68.16) | 671 (67.57) | 0.7674 |
| Province of Monza-Brianza | 277 (12.35) | 176 (14.08) | 101 (10.17) | 0.0052 |
| Other Lombardy provinces | 380 (16.94) | 191 (15.28) | 189 (19.03) | 0.0186 |
| Others | 63 (2.81) | 31 (2.48) | 32 (3.22) | 0.2904 |
| Job description, n (%) | ||||
| Healthcare worker | 49 (2.17) | 6 (0.48) | 43 (4.30) | <0.0001 |
| Office worker | 993 (44.04) | 808 (64.43) | 185 (18.48) | <0.0001 |
| Police | 1213 (53.79) | 440 (35.09) | 773 (77.22) | <0.0001 |
| Work type during lockdown period*, n (%) | ||||
| Usual workplace | 907 (40.36) | 151 (12.08) | 756 (75.83) | <0.0001 |
| Working from home | 845 (37.61) | 736 (58.88) | 109 (10.93) | <0.0001 |
| Both | 451 (20.07) | 329 (26.32) | 122 (12.24) | <0.0001 |
| Stop of working activity | 44 (1.96) | 34 (2.72) | 10 (1.00) | 0.0035 |
| Smoking habit*, n (%) | ||||
| Never | 1437 (63.90) | 805 (64.35) | 632 (63.33) | 0.6162 |
| Ex-smoker | 383 (17.03) | 237 (18.94) | 146 (14.63) | 0.0068 |
| Current smoker | 429 (19.08) | 209 (16.71) | 220 (22.04) | 0.0014 |
| Chronic diseases, n (%°) | ||||
| None | 584 (25.90) | 870 (69.38) | 801 (80.02) | <0.0001 |
| At least one of the following: | 1, 71 (74.10) | 384 (30.62) | 200 (19.98) | |
| Pulmonary disease, n (%°) | 79 (13.53) | 49 (12.76) | 30 (15.00) | 0.4527 |
| Cardiac heart disease, n (%°) | 55 (9.42) | 40 (10.42) | 15 (7.50) | 0.2521 |
| Hypertension, n (%°) | 260 (44.52) | 164 (42.71) | 96 (48.00) | 0.2221 |
| Renal diseases, n (%°) | 8 (1.37) | 7 (1.82) | 1 (0.50) | 0.2748 |
| Immunological disorder, n (%°) | 136 (23.29) | 99 (25.78) | 37 (18.50) | 0.0482 |
| Neoplasm, n (%°) | 48 (8.22) | 35 (9.11) | 13 (6.50) | 0.2750 |
| Metabolic disorder, n (%°) | 113 (19.35) | 74 (19.27) | 39 (19.50) | 0.947 |
| Liver disease, n (%°) | 13 (2.23) | 10 (2.60) | 3 (1.50) | 0.5577 |
| Depression/anxiety, n (%°) | 70 (11.99) | 53 (13.80) | 17 (8.50) | 0.0612 |
| Chronic pharmacological therapies, n (%°) | ||||
| None | 1642 (72.82) | 839 (66.91) | 803 (80.22) | <0.0001 |
| At least one | 613 (27.18) | 415 (33.09) | 198 (19.78) | |
| Aspirin, n (%°) | 38 (6.20) | 25 (6.02) | 13 (6.57) | 0.7948 |
| Oral anticoagulants, n (%°) | 11 (1.79) | 7 (1.69) | 4 (2.02) | 0.7529 |
| Antihypertensive, n (%°) | 246 (40.13) | 153 (36.87) | 93 (46.97) | 0.0170 |
| Statin, n (%°) | 63 (10.28) | 37 (8.92) | 26 (13.13) | 0.1080 |
| Antidiabetic, n (%°) | 24 (3.92) | 15 (3.61) | 9 (4.55) | 0.5784 |
| Anticancer, n (%°) | 10 (1.63) | 8 (1.93) | 2 (1.01) | 0.5128 |
| Cortisone, n (%°) | 55 (8.97) | 36 (8.67) | 19 (9.60) | 0.7090 |
| Antithyroid agent, n (%°) | 74 (12.07) | 51 (12.29) | 23 (11.62) | 0.811 |
| Anti-inflammatory agent, n (%°) | 34 (5.55) | 21 (5.06) | 13 (6.57) | 0.4464 |
| Anxiolytic, n (%°) | 36 (5.87) | 29 (6.99) | 7 (3.54) | 0.0891 |
| Anti-depressant, n (%°) | 25 (4.08) | 17 (4.10) | 8 (4.04) | 0.9739 |
| Food supplement, n (%°) | 167 (27.24) | 132 (31.81) | 35 (17.68) | 0.0002 |
| Immunosuppressive, n (%°) | 14 (2.28) | 13 (3.13) | 1 (0.51) | 0.0443 |
| Vaccinations | ||||
| Flu vaccine (Autumn 2019), n (%) | 234 (10.38) | 155 (12.36) | 79 (7.89) | 0.0005 |
| Pneumococcal vaccine (last 12 months), n (%) | 12 (0.53) | 9 (0.72) | 3 (0.30) | 0.1752 |
| Other vaccine (last 12 months), n (%) | 83 (3.68) | 53 (4.23) | 30 (3.00) | 0.1234 |
| No Antibodies | IgG or IgM Antibodies | p-Value ^ | |
|---|---|---|---|
| N (%) | 2146 (95.17) | 109 (4.83) | - |
| Age, mean ± SD | 44.37 ± 9.70 | 46.00 ± 9.80 | 0.0527 |
| Sex, n (%) | 0.8046 | ||
| Male | 1492 (69.52) | 77 (70.64) | |
| Female | 654 (30.48) | 32 (29.36) | |
| Enrollment period, n (%) | |||
| May-June | 1202 (56.01) | 61 (55.96) | 0.2647 |
| July-August | 638 (29.73) | 27 (24.77) | |
| September-October | 306 (14.26) | 21 (19.27) | |
| SARS-CoV-2 risk exposure | |||
| Low | 1217 (56.71) | 37 (33.94) | <0.0001 |
| Middle-high | 929 (43.29) | 72 (66.06) | |
| Enrollment period and exposure risk | |||
| May-June | |||
| Low exposure | 802 (66.72) | 22 (36.07) | <0.0001 |
| Middle-high exposure | 400 (33.28) | 39 (63.93) | |
| July-August | |||
| Low exposure | 316 (49.53) | 11 (40.74) | 0.3709 |
| Middle-high exposure | 322 (50.47) | 16 (59.26) | |
| September-October | |||
| Low exposure | 99 (32.35) | 4 (19.05) | 0.2042 |
| Middle-high exposure | 207 (67.65) | 17 (80.95) | |
| Municipality*, n (%) | |||
| Province of Milan | 1458 (68.26) | 65 (60.75) | 0.3395 |
| Province of Monza-Brianza | 262 (12.27) | 15 (14.02) | |
| Other Lombardy provinces | 358 (16.76) | 22 (20.56) | |
| Others | 58 (2.72) | 5 (4.67) | |
| Job description, n (%) | |||
| Healthcare worker | 43 (2.00) | 6 (5.50) | 0.0285 |
| Office worker | 957 (44.59) | 36 (33.03) | 0.0176 |
| Police | 1146 (53.40) | 67 (61.47) | 0.0994 |
| Work type during lockdown period*, n (%) | |||
| Usual workplace | 849 (39.71) | 58 (53.21) | 0.0051 |
| Working from home | 818 (38.26) | 27 (24.77) ‡ | 0.0046 |
| Both | 432 (20.21) | 19 (17.43) | 0.4805 |
| Stop of working activity | 39 (1.82) | 5 (4.59) ‡ | 0.0590 |
| Smoking habit*, n (%) | |||
| Never | 1360 (63.55) | 77 (70.64) | 0.1327 |
| Ex-smoker | 361 (16.87) | 22 (20.18) | 0.3692 |
| Current smoker | 419 (19.58) | 10 (9.17) | 0.0070 |
| Chronic diseases, n (%°) | |||
| None | 1597 (74.42) | 74 (67.89) | 0.1292 |
| At least one | 549 (25.58) | 35 (32.11) | |
| Pulmonary disease, n (%°) | 77 (14.03) | 2 (5.71) | 0.2072 |
| Cardiac heart disease, n (%°) | 52 (9.47) | 3 (8.57) | 1.0000 |
| Hypertension, n (%°) | 242 (44.08) | 18 (51.43) | 0.3964 |
| Renal disease, n (%°) | 8 (1.46) | 0 (0.00) | 1.0000 |
| Immunological disorder, n (%°) | 129 (23.50) | 7 (20.00) | 0.6351 |
| Neoplasm, n (%°) | 45 (8.20) | 3 (8.57) | 1.0000 |
| Metabolic disorder, n (%°) | 106 (19.31) | 7 (20.00) | 0.9199 |
| Liver disease, n (%°) | 13 (2.37) | 0 (0.00) | 1.0000 |
| Depression/anxiety, n (%°) | 66 (12.02) | 4 (11.43) | 1.0000 |
| Chronic pharmacological therapies, n (%) | |||
| None | 1567 (73.02) | 75 (68.81) | 0.3349 |
| At least one | 579 (26.98) | 34 (31.19) | |
| Aspirin, n (%°) | 38 (6.56) | 0 (0.00) | 0.2585 |
| Oral anticoagulants, n (%°) | 11 (1.90) | 0 (0.00) | 1.0000 |
| Antihypertensive, n (%°) | 231 (39.90) | 15 (44.12) | 0.6255 |
| Statin, n (%°) | 58 (10.02) | 5 (14.71) | 0.3799 |
| Antidiabetic, n (%°) | 24 (4.15) | 0 (0.00) | 0.6369 |
| Anticancer, n (%°) | 8 (1.38) | 2 (5.88) | 0.1016 |
| Cortisone, n (%°) | 54 (9.33) | 1 (2.94) | 0.3501 |
| Antithyroid agent, n (%°) | 70 (12.09) | 4 (11.76) | 1.0000 |
| Anti-inflammatory agent, n (%°) | 32 (5.53) | 2 (5.88) | 0.7123 |
| Anxiolytic, n (%°) | 33 (5.70) | 3 (8.82) | 0.4421 |
| Anti-depressant, n (%°) | 23 (3.97) | 2 (5.88) | 0.6429 |
| Flood supplement, n (%°) | 159 (27.46) | 8 (23.53) | 0.6168 |
| Immunosuppressive, n (%°) | 13 (2.25) | 1 (2.94) | 0.5541 |
| Vaccinations | |||
| Flu vaccine (Autumn 2019), n (%) | 228 (10.62) | 6 (5.50) | 0.0873 |
| Pneumococcal vaccine (last 12 months), n (%) | 12 (0.56) | 0 (0.00) | 1.0000 |
| Other vaccines (last 12 months), n (%) | 79 (3.68) | 4 (3.67) | 1.0000 |
| Clinical parameters | |||
| SpO2 (%), median [IQR] | 99 [98,99] | 99 [98,99] | 0.5823 |
| Systolic blood pressure (mmHg), mean ± SD | 120.04 ± 13.98 | 122.54 ± 15.19 | 0.1045 |
| Diastolic blood pressure (mmHg), mean ± SD | 77.62 ± 9.74 | 78.80 ± 10.60 | 0.5807 |
| Heart rate (bpm), mean ± SD | 76.75 ± 13.34 | 75.72 ± 11.93 | 0.4678 |
| Body temperature (°C), mean ± SD | 35.97 ± 0.57 | 36.02 ± 0.55 | 0.2177 |
| Symptoms COVID-19, n (%) | |||
| None | 1538 (71.67) | 35 (32.11) | <0.0001 |
| At least 1 | 608 (28.33) | 74 (67.89) | |
| Fever, n(%°) | 174 (28.62) | 53 (71.62) | <0.0001 |
| Cough, n(%°) | 196 (32.24) | 26 (35.14) | 0.6154 |
| Sore throat/cold, n(%°) | 280 (46.05) | 24 (32.43) | 0.0260 |
| Headache, n(%°) | 115 (18.91) | 16 (21.62) | 0.5767 |
| Muscles/bones/joints pain, n(%°) | 107 (17.60) | 25 (33.78) | 0.0009 |
| Anosmia/ageusia, n(%°) | 30 (4.93) | 30 (40.54) | <0.0001 |
| Respiratory distress, n (%°) | 41 (6.74) | 6 (8.11) | 0.6617 |
| Chest pain, n (%°) | 26 (4.28) | 4 (5.41) | 0.5559 |
| Tachycardia, n (%°) | 15 (2.47) | 3 (4.05) | 0.4320 |
| Gastrointestinal disorders, n (%°) | 100 (16.45) | 13 (17.57) | 0.8067 |
| Conjunctivitis, n (%°) | 48 (7.89) | 5 (6.76) | 0.7299 |
| Clinical diagnosis of pneumonia, n (%°) | 2 (0.33) | 5 (6.76) | 0.0002 |
| Total | Low Exposure Risk | Medium-High Exposure Risk | p-Value ^ | |
|---|---|---|---|---|
| N (%) | 2255 | 1254 (55.61) | 1001 (44.39) | - |
| Clinical parameters | ||||
| SpO2 (%), median [IQR] | 99 [98,99] | 99 [98,99] | 99 [98,99] | 0.0648 |
| Systolic blood pressure (mmHg), mean ± SD | 120.16 ± 14.05 | 119.44 ± 14.32 | 121.07 ± 13.66 | 0.0079 |
| Diastolic blood pressure (mmHg), mean ± SD | 77.68 ± 9.79 | 77.13 ± 10.27 | 78.37 ± 9.10 | 0.0025 |
| Heart rate (bpm), mean ± SD | 76.70 ± 13.28 | 77.63 ± 13.49 | 75.55 ± 12.93 | 0.0001 |
| Body temperature (°C), mean ± SD | 35.97 ± 0.57 | 35.91 ± 0.60 | 36.05 ± 0.52 | <0.0001 |
| Symptoms COVID-19, n (%) | ||||
| None | 1573 (69.76) | 855 (68.18) | 718 (71.73) | 0.0685 |
| At least one | 682 (30.24) | 399 (31.82) | 283 (28.27) | |
| Fever, n (%*) | 227 (33.28) | 103 (25.81) | 124 (43.82) | <0.0001 |
| Cough, n (%*) | 222 (32.55) | 116 (29.07) | 106 (37.46) | 0.0213 |
| Sore throat/cold, n (%*) | 304 (44.57) | 189 (47.37) | 115 (40.64) | 0.0814 |
| Headache, n (%*) | 131 (19.21) | 86 (21.55) | 45 (15.90) | 0.0648 |
| Muscles/bones/joints pain, n (%*) | 132 (19.35) | 65 (16.29) | 67 (23.67) | 0.0162 |
| Anosmia/ageusia, n (%*) | 60 (8.80) | 19 (4.76) | 41 (14.49) | <.0001 |
| Respiratory distress, n (%*) | 47 (6.89) | 25 (6.27) | 22 (7.77) | 0.4436 |
| Chest pain, n (%*) | 30 (4.40) | 11 (2.76) | 19 (6.71) | 0.0130 |
| Tachycardia, n (%*) | 18 (2.64) | 8 (2.01) | 10 (3.53) | 0.2198 |
| Gastrointestinal disorders, n (%*) | 113 (16.57) | 67 (16.79) | 46 (16.25) | 0.8524 |
| Conjunctivitis, n (%*) | 53 (7.77) | 33 (8.27) | 20 (7.07) | 0.5630 |
| Clinical diagnosis of Pneumonia, n (%*) | 7 (1.03) | 2 (0.50) | 5 (1.77) | 0.1332 |
| Antibody test for SARS-CoV-2 infection | ||||
| No antibodies | 2146 (95.17) | 1,217 (97.05) | 929 (92.81) | <0.0001 |
| IgG or IgM antibodies | 109 (4.83) | 37 (2.95) | 72 (7.19) | |
| Only IgG antibodies | 89 (81.65) | 31 (83.78) | 58 (80.56) | 0.8583 |
| Only IgM antibodies | 12 (11.01) | 3 (8.11) | 9 (12.50) | |
| IgG and IgM antibodies | 8 (7.34) | 3 (8.11) | 5 (6.94) |
| Adjusted OR (95% CI) | p-Value | |
|---|---|---|
| Multivariable model* on 2,255 subjects (100%) | ||
| Exposure risk (ref. low-risk group) | 3.088 (2.027−4.704) | <0.0001 |
| COVID-19 symptoms (ref. No) | 5.769 (3.799−8.763) | <0.0001 |
| Age (continuous, in year) | 1.026 (1.005−1.048) | 0.0132 |
| Total | Low Exposure Risk | Medium-High Exposure Risk | p-Value ^ | |
|---|---|---|---|---|
| Patients with serological test after 3 months | 48 | 16 | 32 | - |
| Antibody test for SARS-CoV-2 infection | 1.0000 | |||
| No antibodies | 9 (18.7) | 3 (18.7) | 6 (18.7) | |
| IgG or IgM antibodies | 39 (81.3) | 13 (81.3) | 26 (81.3) | |
| Only IgG antibodies | 36 (92.3) | 12 (92.3) | 24 (92.3) | |
| Only IgM antibodies | 1 (7.7) | 1 (7.7) | 0 (0.00) | 0.4073 |
| IgG and IgM antibodies | 2 (5.1) | 0 (0.0) | 2 (7.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Della Valle, P.; Fabbri, M.; Madotto, F.; Ferrara, P.; Cozzolino, P.; Calabretto, E.; D’Orso, M.I.; Longhi, E.; Polosa, R.; Riva, M.A.; et al. Occupational Exposure in the Lombardy Region (Italy) to SARS-CoV-2 Infection: Results from the MUSTANG–OCCUPATION–COVID-19 Study. Int. J. Environ. Res. Public Health 2021, 18, 2567. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052567
Della Valle P, Fabbri M, Madotto F, Ferrara P, Cozzolino P, Calabretto E, D’Orso MI, Longhi E, Polosa R, Riva MA, et al. Occupational Exposure in the Lombardy Region (Italy) to SARS-CoV-2 Infection: Results from the MUSTANG–OCCUPATION–COVID-19 Study. International Journal of Environmental Research and Public Health. 2021; 18(5):2567. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052567
Chicago/Turabian StyleDella Valle, Paola, Marco Fabbri, Fabiana Madotto, Pietro Ferrara, Paolo Cozzolino, Elisabetta Calabretto, Marco Italo D’Orso, Ermanno Longhi, Riccardo Polosa, Michele Augusto Riva, and et al. 2021. "Occupational Exposure in the Lombardy Region (Italy) to SARS-CoV-2 Infection: Results from the MUSTANG–OCCUPATION–COVID-19 Study" International Journal of Environmental Research and Public Health 18, no. 5: 2567. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052567