
Digital Health Transition in Rheumatology: A Qualitative Study

 , , , , , , ,
, , , , , , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
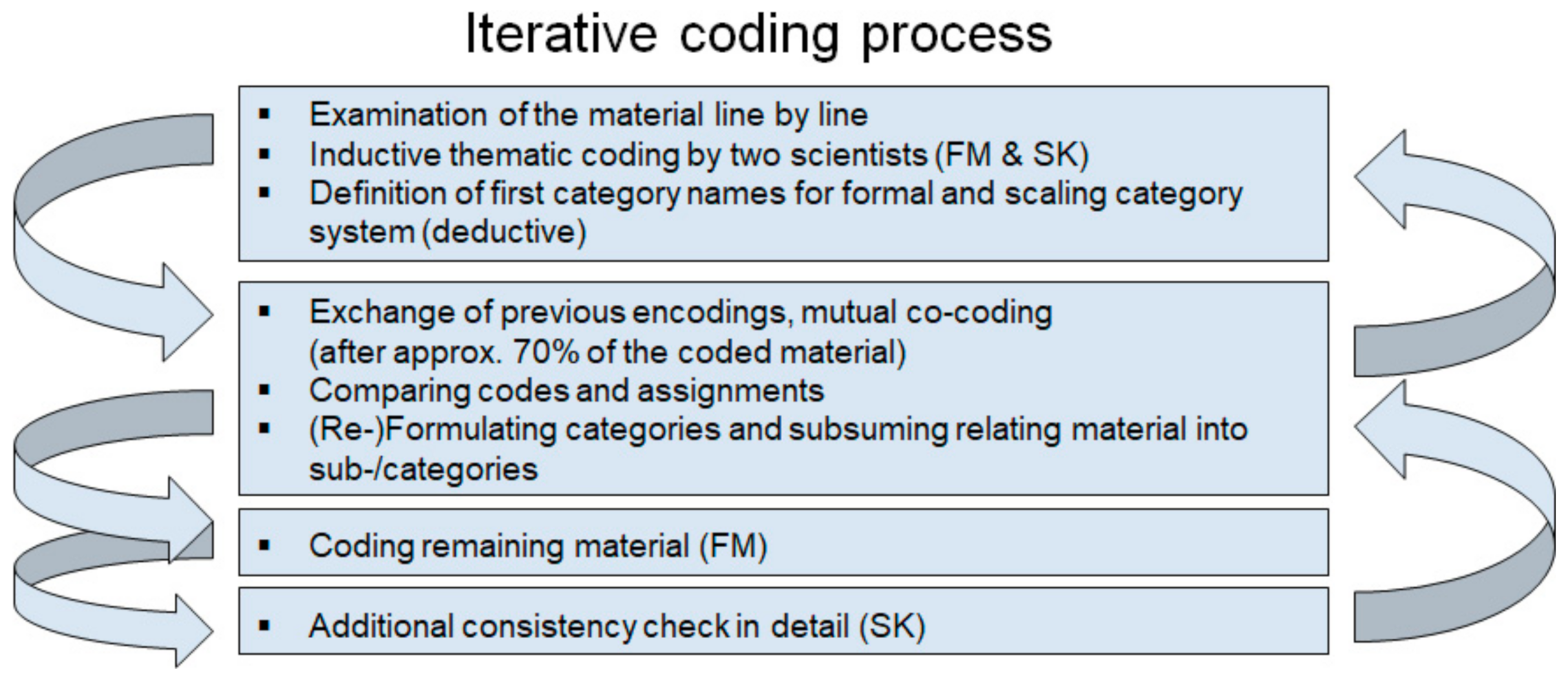
2. Materials and Methods
3. Results
3.1. Digital Rheumatology Use Cases
“Electronic patient records—the next big thing. I see this as an extremely great opportunity to strengthen the doctor–patient relationship and this precious therapy time of five minutes and so on.”(Patient representative I)
“I consider the concept as a chance to provide sensible content to patients, to people, in a centralized way.”(Rheumatologist I)
“I think this extension and supplementation of care through digital health apps, DiGAs, will be a nice, good, viable addition.”(Digital product developer I)
“On the one hand sensitivity and specificity [of diagnosis apps] is very poor at 50 percent. But on the other hand it’s still 20 percent higher than the referral of the non-experienced general practitioner, with a specificity of about 30 percent. That means there’s a clear potential for improvement without any physical examination, as you said, with the methods of [name of a certain digital health application] or [name of another application] or other diagnostic apps. But the power has already been demonstrated.”(Rheumatologist II)
“But that’s what you read now in magazines again and again in a striking way: A patient has foam in her urine, feels somehow bad, weary, and so on, goes to the convenience store, somehow hands in her sample and then receives her results digitally, oh, she knows it’s lupus? That is, I think, not exactly the good start to a chronic patient’s career and good care that we actually want.”(Patient representative I)
3.2. User Descriptions
“And, for a well-cared for or well-adjusted patient like me, a doctor’s contact is really necessary only once a year for therapy monitoring reasons, and if there is something beyond that, like maybe checking whether my blood pressure needs to be adjusted, talking to the doctor once in a while, that would of course be ideal to cover the perhaps necessary two to three doctor’s contacts a year once briefly via a secure telemedicine platform.”(Patient representative I)
“Particularly in the area of rare diseases or unusual symptoms, patients also do research on the internet if they do their research well, find good sources or do research at organizations or patient self-help organizations. Patients who use swarm intelligence can also arrive more quickly at more or less target-oriented diagnostic suggestions. That is a knowledge gain overall.”(Patient representative I)
“My rheumatologist is like that; she tells me that she won’t invest in any digital infrastructure here and I know five, six, seven rheumatologists who are of the same age.”(Patient representative I)
3.3. Adaptation to Different Environments of Rheumatology Care
“Initial diagnosis is only possible by the rheumatologist in direct physical contact and after detailed clinical examination. And then later on, you can talk about how the patient can be followed up by the internet or video consultation or anything else. That’s my opinion at least.”(Rheumatologist III)
“Hey, a qualified initial diagnosis should please, please, please be made by a qualified rheumatologist. I think that is the consensus here in the panel.”(Patient representative I)
“Many patients have no idea what kind of medication they are taking, what kind of therapy they actually want, and I often spend most of my time gathering all this information. Electronic patient records could be a huge relief and I think that it is the key to speed up digitization.”(Rheumatologist II)
“Yes, I am well-adjusted and my CRP is fine. But with new digital tools, for example the app that [name of a digital health application] is going to launch in the area of disease monitoring or something like [name of another application] … new solutions for disease monitoring are entering the market, which will contribute to maintaining the ability to work.”(Patient representative I)
3.4. Potentials of Digital Rheumatology Implementation
“It has been passed and eight months later the first products are about to be approved. I think that is the speed of light for the health system and shows again how the legislator wants to support this transition.”(Digital product developer I)
“It can only be done with education and information campaigns. How should patients and practitioners receive the information, that there is the possibility of prescribing apps … and which ones are available … and how good they are?”(Digital product developer II)
“Digitization is not positive in itself, but it might be positive in its effect and this effect still has to be proven, in other words, evaluated. And in the digitization law and specifically also for the introduction of apps, there is still a necessity to prove the benefit.”(Rheumatologist I)
“How do the individual specialist areas position themselves in regard to digitalization and apps? I think that the rheumatologists—to praise them once again—are pretty much at the forefront here, as is the group of Young Rheumatologists and the Digital Commission. Ultimately, I consider it very state of the art to deal with the topic in this way.”(Digital product developer II)
“I think this is precisely where digital aids could offer a very exciting aspect and expansion: To the extent that the job description of a rheumatologist becomes much more interesting and attractive when one knows that one can deal with digital, innovative tools in the treatment of patients.”(Digital product developer I)
“Because I also think it might be quite pleasant for patients to do without one or two unneeded doctor’s appointments.”(Rheumatologist III)
“As long as things are fine, I don’t need to travel through the city to a non-accessible doctor’s office, anyways.”(Patient representative I)
“Digitization allows us to have more time to talk. That is the quality of care, which is also increasing, because if I have already answered all the questions asked beforehand, then I have maybe five more minutes in the conversation with the patient, and that is an essential five minutes of conversation to improve the perceived care.”(Rheumatologist I)
3.5. Barriers to Digital Rheumatology Implementation
“In many parts of society, that not only include special circumstances, but also students and the general population, from patients to doctors, who simply do not have the technical equipment. And I don’t even want to mention the 5G network, which is also not available in Germany.”(Rheumatologist IV)
“… also the remuneration of digital services. And I think this is the challenge right now, especially in rheumatology … set it up digitally and get away from ‘well, I only want to see the patients who also bring me the money, but I try to care for the patients according to their needs with digital support’.”(Digital product developer I)
“We also have to consider that digitalization creates a wealth gap: people who cannot afford large contracts, good mobile phones, good tablets, do not have good access. And this is also evident in telemedicine and applications, where these systems are not being used. Thus, I believe that we also have to consider the social aspect.”(Rheumatologist I)
“These apps that we are supposed to recommend—to pick up on this—I personally have a very, very hard time with them in my day-to-day practice. Surprisingly, not a single patient has asked me for an app so far. So, all this information is not yet there and then I once again ask you: Why has no patient asked for it yet?”(Rheumatologist V)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dejaco, C.; Alunno, A.; Bijlsma, J.W.; Boonen, A.; Combe, B.; Finckh, A.; Machado, P.M.; Padjen, I.; Sivera, F.; Stamm, T.A.; et al. Influence of COVID-19 pandemic on decisions for the management of people with inflammatory rheumatic and musculoskeletal diseases: A survey among EULAR countries. Ann. Rheum. Dis. 2020. [Google Scholar] [CrossRef]
- Schulze-Koops, H.; Specker, C.; Krueger, K. Telemedicine holds many promises but needs to be developed to be accepted by patients as an alternative to a visit to the doctor. Response to: ‘Patient acceptance of using telemedicine for follow-up of lupus nephritis in the COVID-19 outbreak’ by So et al. Ann. Rheum. Dis. 2020. [Google Scholar] [CrossRef]
- Aries, P.; Welcker, M.; Callhoff, J.; Chehab, G.; Krusche, M.; Schneider, M.; Specker, C.; Richter, J.G. Stellungnahme der Deutschen Gesellschaft für Rheumatologie e. V. (DGRh) zur Anwendung der Videosprechstunde in der Rheumatologie [Statement of the German Society for Rheumatology (DGRh) on the use of video consultations in rheumatology]. Z. Rheumatol. 2020, 79, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Kernder, A.; Morf, H.; Klemm, P.; Vossen, D.; Haase, I.; Mucke, J.; Meyer, M.; Kleyer, A.; Sewerin, P.; Bendzuck, G.; et al. Digital rheumatology in the era of COVID-19: Results of a national patient and physician survey. RMD Open 2021, 7, e001548. [Google Scholar] [CrossRef] [PubMed]
- Gesetz für Eine Bessere Versorgung durch Digitalisierung und Innovation [Digital Health Act]. 2019. Available online: https://dip21.bundestag.de/dip21/btd/19/134/1913438.pdf (accessed on 11 January 2021).
- Krusche, M.; Sewerin, P.; Kleyer, A.; Mucke, J.; Vossen, D.; Morf, H. Facharztweiterbildung quo vadis? [Specialist training quo vadis?]. Z. Rheumatol. 2019, 78, 692–697. [Google Scholar] [CrossRef]
- Combe, B.; Landewe, R.; Daien, C.I.; Hua, C.; Aletaha, D.; Álvaro-Gracia, J.M.; Bakkers, M.; Brodin, N.; Burmester, G.R.; Codreanu, C.; et al. 2016 update of the EULAR recommendations for the management of early arthritis. Ann. Rheum. Dis. 2016, 76, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Aletaha, D.; Bijlsma, J.W.; Breedveld, F.C.; Boumpas, D.; Burmester, G.; Combe, B.; Cutolo, M.; de Wit, M.; Dougados, M.; et al. Treating rheumatoid arthritis to target: Recommendations of an international task force. Ann. Rheum. Dis. 2010, 69, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Knitza, J.; Knevel, R.; Raza, K.; Bruce, T.; Eimer, E.; Gehring, I.; Mathsson-Alm, L.; Poorafshar, M.; Hueber, A.J.; Schett, G.; et al. Toward Earlier Diagnosis Using Combined eHealth Tools in Rheumatology: The Joint Pain Assessment Scoring Tool (JPAST) Project. JMIR Mhealth Uhealth 2020, 8, e17507. [Google Scholar] [CrossRef] [PubMed]
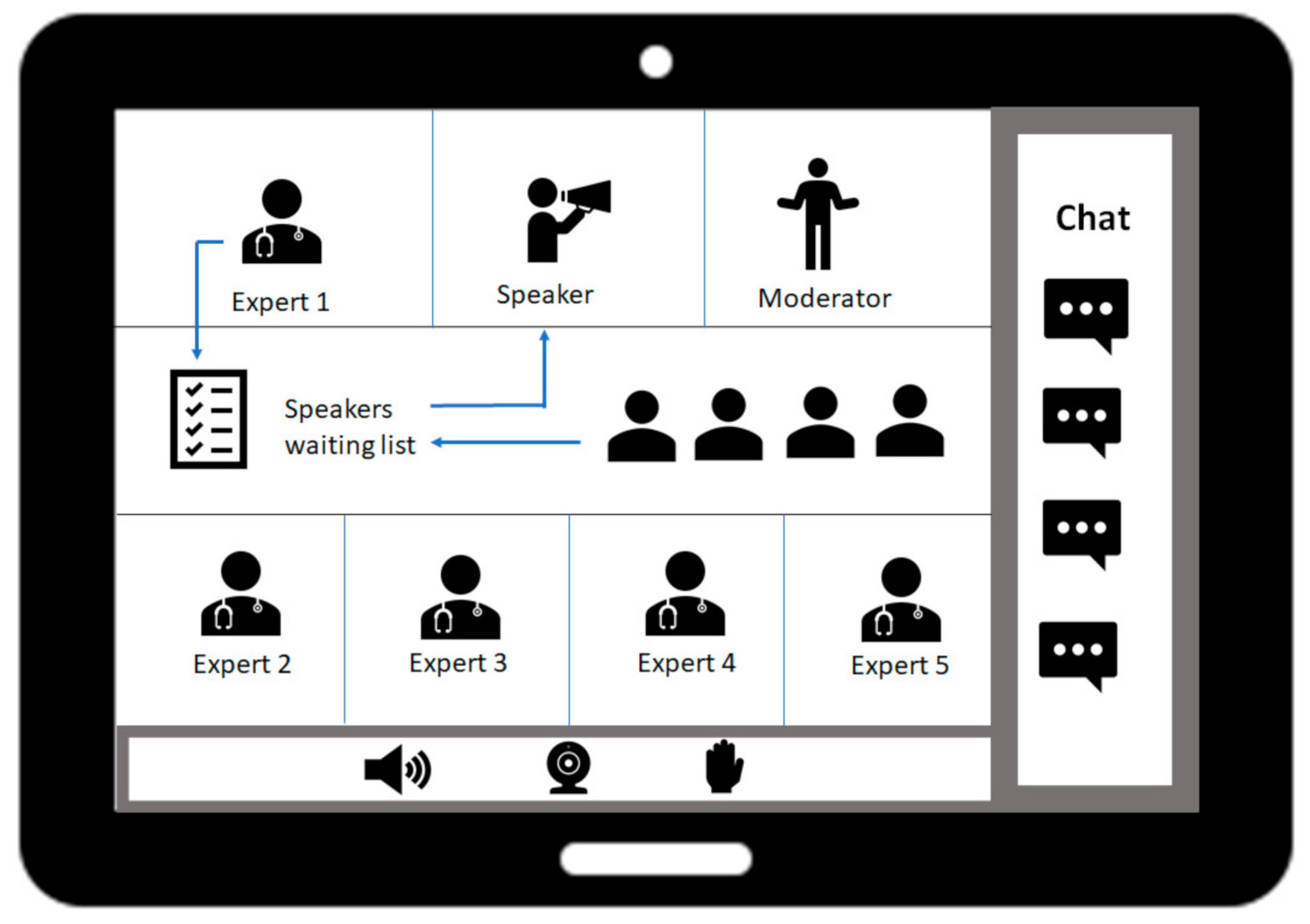
- Muehlensiepen, F.; Mucke, J.; Krusche, M.; Kurkowski, S.; Bendzuck, G.; Koetter, I.; Lemarié, V.; Grahammer, M.; Heinze, M.; Schulze-Koops, H.; et al. The virtual fishbowl: Bringing back dynamic debates to medical conferences. Ann. Rheum. Dis. 2020. [Google Scholar] [CrossRef]
- Mayring, P. Qualitative Inhaltsanalyse. Forum Qual. Soc. Res. 2000, 1, 20. Available online: https://www.qualitative-research.net/index.php/fqs/article/view/1089/2383 (accessed on 11 January 2021).
- Mucke, J.; Anders, H.J.; Aringer, M.; Chehab, G.; Fischer-Betz, R.; Heipe, F.; Lorenz, H.-M.; Schwarting, A.; Specker, C.; Voll, R.E.; et al. Swimming against the stream: The fishbowl discussion method as an interactive tool for medical conferences: Experiences from the 11th European lupus meeting. Ann. Rheum. Dis. 2019, 78, 713–714. [Google Scholar] [CrossRef]
- Dutt, K.M. The Fishbowl Motivates students to participate. Coll. Teach. 1997, 45, 143. [Google Scholar] [CrossRef]
- Zoom Video Communications, Inc. ZOOM Cloud Meetings. Available online: https://zoom.us/ (accessed on 11 January 2021).
- MAXQDA. Software für qualitative Datenanalyse. Available online: https://www.maxqda.de/ (accessed on 11 January 2021).
- Kurkowski, S.; Radon, J.; Vogt, A.R.; Weber, M.; Stiel, S.; Ostgathe, C.; Heckel, M. Hospital end-of-life care: Families’ free-text notes. BMJ Support Palliat Care 2020. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Kulcsar, Z.; Albert, D.; Ercolano, E.; Mecchella, J.N. Telerheumatology: A technology appropriate for virtually all. Semin. Arthritis Rheum. 2016, 46, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Krusche, M.; Burmester, G.R.; Knitza, J. Digital crowdsourcing: Unleashing its power in rheumatology. Ann. Rheum. Dis. 2020, 79, 1139–1140. [Google Scholar] [CrossRef]
- Ruffer, N.; Knitza, J.; Krusche, M. #Covid4Rheum: An analytical twitter study in the time of the COVID-19 pandemic. Rheumatol. Int. 2020, 40, 2031–2037. [Google Scholar] [CrossRef] [PubMed]
- Knitza, J.; Simon, D.; Lambrecht, A.; Raab, C.; Tascilar, K.; Hagen, M.; Kleyer, A.; Bayat, S.; Derungs, A.; Amft, O.; et al. Mobile Health Usage, Preferences, Barriers, and eHealth Literacy in Rheumatology: Patient Survey Study. JMIR Mhealth Uhealth 2020, 8, e19661. [Google Scholar] [CrossRef] [PubMed]
- Krusche, M.; Klemm, P.; Grahammer, M.; Mucke, J.; Vossen, D.; Kleyer, A.; Sewerin, P.; Knitza, J. Acceptance, Usage, and Barriers of Electronic Patient-Reported Outcomes Among German Rheumatologists: Survey Study. JMIR Mhealth Uhealth 2020, 8, e18117. [Google Scholar] [CrossRef] [PubMed]
- Muehlensiepen, F.; Knitza, J.; Marquardt, W.; Engler, J.; Hueber, A.; Welcker, M. Acceptance of Telerheumatology: Results of a nationwide Survey of Rheumatologists and General Practitioners. J. Intern. Med. under review. [CrossRef]
- Mangin, D.; Parascandalo, J.; Khudoyarova, O.; Agarwal, G.; Bismah, V.; Orr, S. Multimorbidity, eHealth and implications for equity: A cross-sectional survey of patient perspectives on eHealth. BMJ Open 2019, 9, e023731. [Google Scholar] [CrossRef] [PubMed]
- de Thurah, A.; Stengaard-Pedersen, K.; Axelsen, M.; Fredberg, U.; Schougaard, L.M.V.; Hjollund, N.H.I.; Pfeiffer-Jensen, M.; Laurberg, T.B.; Tarp, U.; Lomborg, K.; et al. Tele-Health Followup Strategy for Tight Control of Disease Activity in Rheumatoid Arthritis: Results of a Randomized Controlled Trial. Arthritis Care Res. 2018, 70, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knitza, J.; Kleyer, A.; Klüppel, M.; Krasuer, M.; Wacker, J.; Schett, G.; Simon, D. Online-Ultraschalllernmodule in der Rheumatologie [Online ultrasound learning modules in rheumatology]. Z. Rheumatol. 2020, 79, 276–279. [Google Scholar] [CrossRef] [Green Version]
- Melchiorre, M.G.; Lamura, G.; Barbabella, F. eHealth for people with multimorbidity: Results from the ICARE4EU project and insights from the “10 e’s” by Gunther Eysenbach. PLoS ONE 2018, 13, e0207292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granström, E.; Wannheden, C.; Brommels, M.; Hvitfeldt, H.; Nyström, M.E. Digital tools as promoters for person-centered care practices in chronic care? Healthcare professionals’ experiences from rheumatology care. BMC Health Serv Res. 2020, 20, 1108. [Google Scholar] [CrossRef]
- Mehta, B.; Jannat-Khah, D.; Fontana, M.A.; Moezinia, C.J.; Mancuso, C.A.; Bass, A.R.; Antao, V.C.; Gibofsky, A.; Goodman, S.M.; Ibrahim, S. Impact of COVID-19 on vulnerable patients with rheumatic disease: Results of a worldwide survey. RMD Open 2020, 6, e001378. [Google Scholar] [CrossRef] [PubMed]
- Kataria, S.; Ravindran, V. Digital health: A new dimension in rheumatology patient care. Rheumatol. Int. 2018, 38, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Kavadichanda, C.; Shah, S.; Daber, A.; Bairwa, D.; Mathew, A.; Dunga, S.; Das, A.C.; Gopal, A.; Ravi, K.; Kar, S.S.; et al. Tele-rheumatology for overcoming socioeconomic barriers to healthcare in resource constrained settings: Lessons from COVID-19 pandemic. Rheumatology (Oxford) 2020. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mühlensiepen, F.; Kurkowski, S.; Krusche, M.; Mucke, J.; Prill, R.; Heinze, M.; Welcker, M.; Schulze-Koops, H.; Vuillerme, N.; Schett, G.; et al. Digital Health Transition in Rheumatology: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 2636. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052636
Mühlensiepen F, Kurkowski S, Krusche M, Mucke J, Prill R, Heinze M, Welcker M, Schulze-Koops H, Vuillerme N, Schett G, et al. Digital Health Transition in Rheumatology: A Qualitative Study. International Journal of Environmental Research and Public Health. 2021; 18(5):2636. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052636
Chicago/Turabian StyleMühlensiepen, Felix, Sandra Kurkowski, Martin Krusche, Johanna Mucke, Robert Prill, Martin Heinze, Martin Welcker, Hendrik Schulze-Koops, Nicolas Vuillerme, Georg Schett, and et al. 2021. "Digital Health Transition in Rheumatology: A Qualitative Study" International Journal of Environmental Research and Public Health 18, no. 5: 2636. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052636