
Intranasal Insulin Administration to Prevent Delayed Neurocognitive Recovery and Postoperative Neurocognitive Disorder: A Narrative Review

 ,
,
Abstract
:1. Introduction
2. Preclinical Evidence
3. Clinical Evidence
4. Discussion
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Evered, L.; Silbert, B.; Knopman, D.S.; Scott, D.A.; DeKosky, S.T.; Rasmussen, L.S.; Oh, E.S.; Crosby, G.; Berger, M.; Eckenhoff, R.G.; et al. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018. Anesthesiology 2018, 129, 872–879. [Google Scholar] [CrossRef]
- Evered, L.; Silbert, B.; Scott, D.A.; Eckenhoff, R.G. Recommendations for a new perioperative cognitive impairment nomenclature. Alzheimers Dement. 2019, 15, 1115–1116. [Google Scholar] [CrossRef] [PubMed]
- Bilotta, F.; Qeva, E.; Matot, I. Anesthesia and cognitive disorders: A systematic review of the clinical evidence. Expert. Rev. Neurother. 2016, 16, 1311–1320. [Google Scholar] [CrossRef] [PubMed]
- Needham, M.J.; Webb, C.E.; Bryden, D.C. Postoperative cognitive dysfunction and dementia: What we need to know and do. Br. J. Anaesth. 2017, 119, i115–i125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evered, L.A.; Silbert, B.S. Postoperative cognitive dysfunction and noncardiac surgery. Anesth. Analg. 2018, 127, 496–505. [Google Scholar] [CrossRef]
- Van Harten, A.E.; Scheeren, T.W.; Absalom, A.R. A review of postoperative cognitive dysfunction and neuroinflammation associated with cardiac surgery and anaesthesia. Anaesthesia 2012, 67, 280–293. [Google Scholar] [CrossRef]
- Steinmetz, J.; Christensen, K.B.; Lund, T.; Lohse, N.; Rasmussen, L.S. ISPOCD Group: Long-term consequences of postoperative cognitive dysfunction. Anesthesiology 2009, 110, 548–555. [Google Scholar] [CrossRef] [Green Version]
- Borozdina, A.; Qeva, E.; Cinicola, M.; Bilotta, F. Perioperative cognitive evaluation. Curr. Opin. Anaesthesiol. 2018, 31, 756–761. [Google Scholar] [CrossRef]
- Hermanides, J.; Qeva, E.; Preckel, B.; Bilotta, F. Perioperative hyperglycemia and neurocognitive outcome after surgery: A systematic review. Minerva Anestesiol. 2018, 84, 1178–1188. [Google Scholar] [CrossRef]
- Ballard, C.; Jones, E.; Gauge, N.; Aarsland, D.; Nilsen, O.B.; Saxby, B.K.; Lowery, D.; Corbett, A.; Wesnes, K.; Katsaiti, E.; et al. Optimised anaesthesia to reduce post operative cognitive decline (POCD) in older patients undergoing elective surgery, a randomised controlled trial. PLoS ONE 2012, 7, e37410. [Google Scholar] [CrossRef]
- Shoair, O.A.; Grasso, M.P., II; Lahaye, L.A.; Daniel, R.; Biddle, C.J.; Slattum, P.W. Incidence and risk factors for postoperative cognitive dysfunction in older adults undergoing major noncardiac surgery: A prospective study. J. Anaesthesiol. Clin. Pharmacol. 2015, 31, 30–36. [Google Scholar] [CrossRef]
- Mason, S.E.; Noel-Storr, A.; Ritchie, C.W. The impact of general and regional anesthesia on the incidence of post-operative cognitive dysfunction and post-operative delirium: A systematic review with meta-analysis. J. Alzheimers Dis. 2010, 22, S67–S79. [Google Scholar] [CrossRef]
- Bilotta, F.; Lauretta, M.P.; Tewari, A.; Haque, M.; Hara, N.; Uchino, H.; Rosa, G. Insulin and the brain: A sweet relationship with intensive care. J. Intensive Care Med. 2017, 32, 48–58. [Google Scholar] [CrossRef]
- Kleinridders, A.; Ferris, H.A.; Cai, W.; Kahn, C.R. Insulin action in brain regulates systemic metabolism and brain function. Diabetes 2014, 63, 2232–2243. [Google Scholar] [CrossRef] [Green Version]
- Erol, A. An integrated and unifying hypothesis for the metabolic basis of sporadic Alzheimer’s Disease. J. Alzheimers Dis. 2008, 13, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Stoeckel, L.E.; Arvanitakis, Z.; Gandy, S.; Small, D.; Kahn, C.R.; Pascual-Leone, A.; Pawlyk, A.; Sherwin, R.; Smith, P. Complex mechanisms linking neurocognitive dysfunction to insulin resistance and other metabolic dysfunction. F1000Research 2016, 5, 353. [Google Scholar] [CrossRef]
- Frölich, L.; Blum-Degen, D.; Riederer, P.; Hoyer, S. A disturbance in the neuronal insulin receptor signal transduction in sporadic Alzheimer’s disease. Ann. N. Y. Acad. Sci. 1999, 893, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Craft, S.; Baker, L.D.; Montine, T.J.; Minoshima, S.; Watson, G.S.; Claxton, A.; Arbuckle, M.; Callaghan, M.; Tsai, E.; Plymate, S.R.; et al. Intranasal insulin therapy for Alzheimer disease and amnestic mild cognitive impairment: A pilot clinical trial. Arch. Neurol. 2012, 69, 29–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craft, S.; Raman, R.; Chow, T.W.; Rafii, M.S.; Sun, C.K.; Rissman, R.A.; Donohue, M.C.; Brewer, J.B.; Jenkins, C.; Harless, K.; et al. Safety, efficacy, and feasibility of intranasal insulin for the treatment of mild cognitive impairment and Alzheimer disease dementia: A randomized clinical trial. JAMA Neurol. 2020, 77, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Run, X.; Liang, Z.; Zhao, Y.; Dai, C.L.; Iqbal, K.; Liu, F.; Gong, C.X. Intranasal insulin prevents anesthesia-induced hyperphosphorylation of tau in 3xTg-AD mice. Front. Aging Neurosci. 2014, 6, 100. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Dai, C.L.; Chen, Y.; Iqbal, K.; Liu, F.; Gong, C.X. Intranasal insulin prevents anesthesia-induced spatial learning and memory deficit in mice. Sci. Rep. 2016, 6, 21186. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Dai, C.L.; Wu, Z.; Iqbal, K.; Liu, F.; Zhang, B.; Gong, C.X. Intranasal insulin prevents anesthesia-induced cognitive impairment and chronic neurobehavioral changes. Front. Aging Neurosci. 2017, 9, 136. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Dai, C.L.; Gu, J.H.; Peng, S.; Li, J.; Yu, Q.; Iqbal, K.; Liu, F.; Gong, C.X. Intranasal administration of insulin reduces chronic behavioral abnormality and neuronal apoptosis induced by general anesthesia in neonatal mice. Front. Neurosci. 2019, 13, 706. [Google Scholar] [CrossRef] [Green Version]
- Dai, C.L.; Li, H.; Hu, X.; Zhang, J.; Liu, F.; Iqbal, K.; Gong, C.X. Neonatal exposure to anesthesia leads to cognitive deficits in old age: Prevention with intranasal administration of insulin in mice. Neurotox. Res. 2020, 38, 299–311. [Google Scholar] [CrossRef]
- Yu, Q.; Dai, C.L.; Zhang, Y.; Chen, Y.; Wu, Z.; Iqbal, K.; Liu, F.; Gong, C.X. Intranasal insulin increases synaptic protein expression and prevents anesthesia-induced cognitive deficits through mTOR-eEF2 pathway. J. Alzheimers Dis. 2019, 70, 925–936. [Google Scholar] [CrossRef]
- Li, X.; Run, X.; Wei, Z.; Zeng, K.; Liang, Z.; Huang, F.; Ke, D.; Wang, Q.; Wang, J.Z.; Liu, R.; et al. Intranasal insulin prevents anesthesia-induced cognitive impairments in aged mice. Curr. Alzheimer Res. 2019, 16, 8–18. [Google Scholar] [CrossRef]
- Banting, F.G.; Best, C.H.; Collip, J.B.; Campbell, W.R.; Fletcher, A.A. Pancreatic extracts in the treatment of diabetes mellitus. Can. Med. Assoc. J. 1922, 12, 141–146. [Google Scholar] [PubMed]
- Sakel, M. The origin and nature of the hypoglycemic therapy of the psychoses. Bull. N. Y. Acad. Med. 1937, 13, 97–109. [Google Scholar] [PubMed]
- Mack, C.W.; Burch, B.O. Insulin shock therapy in dementia praecox: A report of a series of cases. Calif. West. Med. 1939, 50, 339–344. [Google Scholar]
- Fink, M.; Shaw, R.; Gross, G.E.; Coleman, F.S. Comparative study of chlorpromazine and insulin coma in therapy of psychosis. J. Am. Med. Assoc. 1958, 166, 1846–1850. [Google Scholar] [CrossRef]
- Begg, D.P. Insulin transport into the brain and cerebrospinal fluid. Vitam. Horm. 2015, 98, 229–248. [Google Scholar]
- Dorn, A.; Bernstein, H.G.; Rinne, A.; Ziegler, M.; Hahn, H.J.; Ansorge, S. Insulin—and glucagonlike peptides in the brain. Anat. Rec. 1983, 207, 69–77. [Google Scholar] [CrossRef]
- Lioutas, V.A.; Alfaro-Martinez, F.; Bedoya, F.; Chung, C.C.; Pimentel, D.A.; Novak, V. Intranasal insulin and Insulin-Like Growth Factor 1 as neuroprotectants in acute ischemic stroke. Transl. Stroke Res. 2015, 6, 264–275. [Google Scholar] [CrossRef]
- Lioutas, V.A.; Novak, V. Intranasal insulin neuroprotection in ischemic stroke. Neural. Regen. Res. 2016, 11, 400–401. [Google Scholar] [CrossRef] [PubMed]
- Benedict, C.; Hallschmid, M.; Schultes, B.; Born, J.; Kern, W. Intranasal insulin to improve memory function in humans. Neuroendocrinology 2007, 86, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Shemesh, E.; Rudich, A.; Harman-Boehm, I.; Cukierman-Yaffe, T. Effect of intranasal insulin on cognitive function: A systematic review. J. Clin. Endocrinol. Metab. 2012, 97, 366–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reger, M.A.; Watson, G.S.; Frey, W.H., 2nd; Baker, L.D.; Cholerton, B.; Keeling, M.L.; Belongia, D.A.; Fishel, M.A.; Plymate, S.R.; Schellenberg, G.D.; et al. Effects of intranasal insulin on cognition in memory-impaired older adults: Modulation by APOE genotype. Neurobiol. Aging 2006, 27, 451–458. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Kalaitzidis, G.; Malli, A.; Kalaitzoglou, D.; Myserlis, P.G.; Lioutas, V.A. Intranasal insulin in Alzheimer’s dementia or mild cognitive impairment: A systematic review. J. Neurol. 2018, 265, 1497–1510. [Google Scholar] [CrossRef] [PubMed]
- Benedict, C.; Frey, W.H., 2nd; Schiöth, H.B.; Schultes, B.; Born, J.; Hallschmid, M. Intranasal insulin as a therapeutic option in the treatment of cognitive impairments. Exp. Gerontol. 2011, 46, 112–115. [Google Scholar] [CrossRef]
- Chapman, C.D.; Schiöth, H.B.; Grillo, C.A.; Benedict, C. Intranasal insulin in Alzheimer’s disease: Food for thought. Neuropharmacology 2018, 136, 196–201. [Google Scholar] [CrossRef]
- Claxton, A.; Baker, L.D.; Hanson, A.; Trittschuh, E.H.; Cholerton, B.; Morgan, A.; Callaghan, M.; Arbuckle, M.; Behl, C.; Craft, S. Long-acting intranasal insulin detemir improves cognition for adults with mild cognitive impairment or early-stage Alzheimer’s disease dementia. J. Alzheimers Dis. 2015, 44, 897–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, P.; Pimentel Maldonado, D.A.; Novak, V. Safety and preliminary efficacy of intranasal insulin for cognitive impairment in Parkinson disease and multiple system atrophy: A double-blinded placebo-controlled pilot study. PLoS ONE 2019, 14, e0214364. [Google Scholar] [CrossRef] [Green Version]
- Bilotta, F.; Gelb, A.W.; Stazi, E.; Titi, L.; Paoloni, F.P.; Rosa, G. Pharmacological perioperative brain neuroprotection: A qualitative review of randomized clinical trials. Br. J. Anaesth. 2013, 110, i113–i120. [Google Scholar] [CrossRef] [Green Version]
- Eckenhoff, R.G.; Maze, M.; Xie, Z.; Culley, D.J.; Goodlin, S.J.; Zuo, Z.; Wei, H.; Whittington, R.A.; Terrando, N.; Orser, B.A.; et al. Perioperative neurocognitive disorder: State of the preclinical science. Anesthesiology 2020, 132, 55–68. [Google Scholar] [CrossRef]
- Mitchell, S.J.; Pellett, O.; Gorman, D.F. Cerebral protection by lidocaine during cardiac operations. Ann. Thorac. Surg. 1999, 67, 1117–1124. [Google Scholar] [CrossRef]
- Mathew, J.P.; Mackensen, G.B.; Phillips-Bute, B.; Grocott, H.P.; Glower, D.D.; Laskowitz, D.T.; Blumenthal, J.A.; Newman, M.F.; Neurologic Outcome Research Group (NORG) of the Duke Heart Center. Randomized, double-blinded, placebo controlled study of neuroprotection with lidocaine in cardiac surgery. Stroke 2009, 40, 880–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mack, W.J.; Kellner, C.P.; Sahlein, D.H.; Ducruet, A.F.; Kim, G.H.; Mocco, J.; Zurica, J.; Komotar, R.J.; Haque, R.; Sciacca, R.; et al. Intraoperative magnesium infusion during carotid endarterectomy: A double-blind placebo-controlled trial. J. Neurosurg. 2009, 110, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Hudetz, J.A.; Iqbal, Z.; Gandhi, S.D.; Patterson, K.M.; Byrne, A.J.; Hudetz, A.G.; Pagel, P.S.; Warltier, D.C. Ketamine attenuates post-operative cognitive dysfunction after cardiac surgery. Acta Anaesthesiol. Scand. 2009, 53, 864–872. [Google Scholar] [CrossRef]
- Thorne, R.G.; Pronk, G.J.; Padmanabhan, V.; Frey, W.H., 2nd. Delivery of insulin-like growth factor-I to the rat brain and spinal cord along olfactory and trigeminal pathways following intranasal administration. Neuroscience 2004, 127, 481–496. [Google Scholar] [CrossRef] [PubMed]
- Brown, C., IV; Deiner, S. Perioperative cognitive protection. Br. J. Anaesth. 2016, 117, iii52–iii61. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Reference | Results |
|---|---|
| Chen, Y., et al. [20] | Intranasal insulin administered before anesthesia exposure in AD mice was associated with lower phosphorylation levels of tau protein. |
| Zhang, Y., et al. [21] | Intranasal insulin administered before anesthesia exposure in wild-type mice was shown to reduce hyperphosphorylation of tau proteins and to prevent spatial learning impairment. |
| Chen, Y., et al. [22] | Intranasal insulin administration in AD mice before anesthesia exposure was shown to prevent anesthesia-induced spatial learning and memory deficit and long-term neurobehavioral changes. |
| Li, H., et al. [23] | Intranasal insulin administered in neonatal mice before anesthesia exposure was reported to prevent long-term behavioral abnormalities, changes in synaptic proteins, and neuronal apoptosis. |
| Dai, C.L., et al. [24] | Intranasal insulin administration before anesthesia exposure in neonatal mice was shown to prevent anesthesia-related behavioral and cognitive impairment associated with specific brain areas such as the amygdala, hippocampus, frontal cortex, and cingulate cortex. |
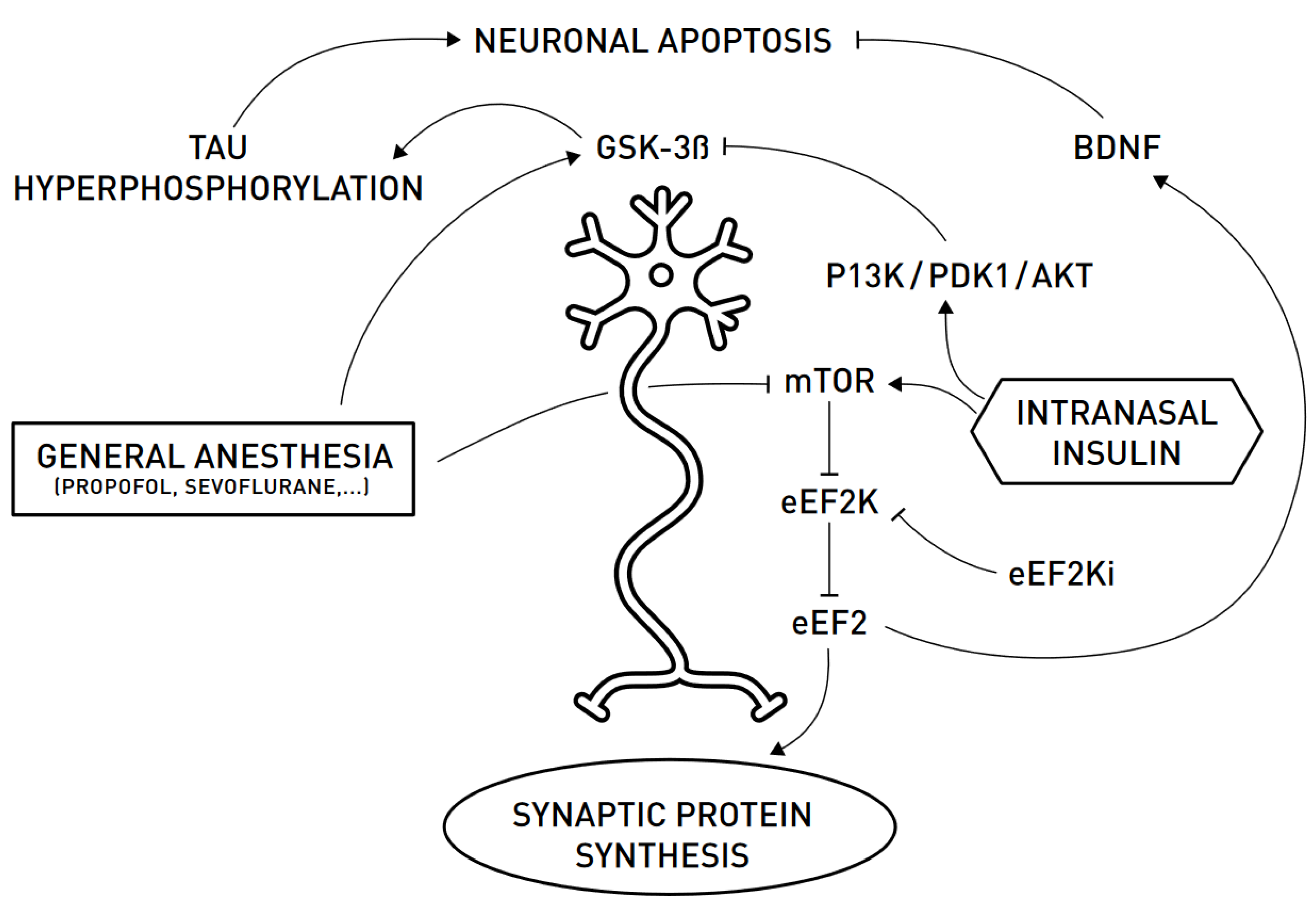
| Yu, Q., et al. [25] | Intranasal insulin administered before anesthesia exposure in wild-type aged mice was demonstrated to promote mTOR-eEF2 signaling pathway and prevent anesthesia-induced reduction in brain synaptic proteins and the BDNF and cognitive decline. |
| Li, X., et al. [26] | Intranasal insulin administration in aged mice exposed to anesthesia was shown to prevent hyperphosphorylation of tau proteins, loss of specific synaptic proteins, and cognitive defects. |
| Reference | Type of Study | Other Information | Results |
|---|---|---|---|
| Banting, F.G., et al. [27] | Case control | 14-year-old boy with glycosuria, weight loss, increased frequency of day and night micturition | Extracts of insular tissue of the pancreas injected subcutaneously or intravenously led to reduction in the blood glucose concentration, abolishment of glycosuria, disappearance of acetone bodies from the urine, and increase in the of carbohydrates. |
| Sakel, M. [28] | Case series | Psychiatric patients under insulin-induced hypoglycemia/coma | Patients with morphine addiction and schizophrenia had a reduction in or the disappearance of hallucinations during insulin-induced hypoglycemia and a protraction of the lucid phase. |
| Mack, C.W., et al. [29] | Case series | 19 dementia praecox patients undergoing insulin-induced hypoglycemic shock | Hypoglycemia shock induced by insulin has shown clinical improvement in dementia praecox patients. |
| Fink, M., et al. [30] | Randomized control trial | 60 psychiatric patients: 30 patients received chlorpromazine by mouth with a median of 800 mg daily for at least 3 months; insulin coma induced in each of the other 30 patients | Chlorpromazine was safer, easier to administer, and suited to long-term management than an insulin coma in schizophrenic patients. |
| Begg, D.P. [31]; Dorn, A., et al. [32] | Chapter; observational study | Insulin transport into the brain/CSF; brain insulin production | Plasma insulin is transported through endothelial BBB cells by an IR-mediated transcytosis mechanism, while the hypothalamus, hippocampus, and brain stem produce insulin independently. |
| Lioutas, V.A. [33] | Review | Intranasal insulin administration in healthy, MCI, and AD participants | Intranasal insulin reaches the CNS through olfactory and trigeminal neurons without causing systemic hypoglycemia or hepatic first-pass metabolism; it increased the feeling of well-being and self-confidence and decreased anger in healthy participants, while in MCI/AD patients, it improved functional status and in AD patients general cognition performance. |
| Lioutas, V.A., et al. [34] | Perspective article | Role of intranasal insulin as a neuroprotective agent in ischemic stroke patients | Effects of intranasal insulin as a neuroprotective agent: suppression of pro-inflammatory transcription response, vasodilatory effects, induction of thrombolysis, reduction in infarct volume, anti-apoptotic effects, promotion of neurite regeneration, neurotransmission, and functional connectivity. |
| Benedict, C., et al. [35] | Randomized controlled trial | 38 healthy participants; each group n = 19; intranasal insulin administration (4X40 UI/d) vs. placebo | Intranasal insulin administration in individuals without memory impairment was shown to improve recall ability and self-confidence in cognitive tasks after 8-week treatment. |
| Shemesh, E., et al. [36] | Systematic review | 8 studies: healthy participants, MCI, or AD patients | High doses of intranasal insulin (160 IU/die) compared to low doses (≥60 IU/die) in healthy individuals were shown to induce beneficial effects; in MCI/AD patients, long-term intranasal insulin administration of 20 UI showed a beneficial effect on cognitive functions. |
| Reger, M.A., et al. [37] | Randomized controlled trial | 35 healthy adults and 26 MCI/AD patients receiving saline, 20 IU, or 40 IU intranasal insulin administration | Intranasal insulin administration in APOE4- MCI/AD patients was shown to facilitate recall of verbal memory, with stronger effects compared to APOE4+ MCI/AD patients and healthy adults. |
| Avgerinos, K.I., et al. [38] | Systematic review | 7 studies of 293 MCI/AD patients receiving intranasal insulin administration | Improved story recall performance in APOE4- MCI/AD patients. |
| Benedict, C., et al. [39] | Review | Intranasal insulin administration in healthy individuals or AD patients | Memory-improving effect of the CNS in both healthy and AD individuals. |
| Chapman, C.D., et al. [40] | Review | Cognitively healthy or MCI/AD individuals treated with intranasal insulin | Cognitive and functional status improvement and preservation of brain volume. |
| Claxton, A., et al. [41] | Randomized controlled trial | 60 MCI/AD patients receiving intranasal placebo, 20 IU, or 40 IU of insulin detemir for 21 days | 40 IU intranasal detemir improved verbal memory in MCI/AD APOE-4 allele carrier patients and visuospatial and verbal working memory for all participants. |
| Novak, P., et al. [42] | Randomized controlled trial | 16 PD/MSA patients receiving placebo or 40 IU insulin intranasally | Intranasal insulin administration improved cognitive and functional performance in PD patients, while in MSA patients, it induced a lack of disease progression. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badenes, R.; Qeva, E.; Giordano, G.; Romero-García, N.; Bilotta, F. Intranasal Insulin Administration to Prevent Delayed Neurocognitive Recovery and Postoperative Neurocognitive Disorder: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 2681. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052681
Badenes R, Qeva E, Giordano G, Romero-García N, Bilotta F. Intranasal Insulin Administration to Prevent Delayed Neurocognitive Recovery and Postoperative Neurocognitive Disorder: A Narrative Review. International Journal of Environmental Research and Public Health. 2021; 18(5):2681. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052681
Chicago/Turabian StyleBadenes, Rafael, Ega Qeva, Giovanni Giordano, Nekane Romero-García, and Federico Bilotta. 2021. "Intranasal Insulin Administration to Prevent Delayed Neurocognitive Recovery and Postoperative Neurocognitive Disorder: A Narrative Review" International Journal of Environmental Research and Public Health 18, no. 5: 2681. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052681