
A Real-Time Artificial Intelligence-Assisted System to Predict Weaning from Ventilator Immediately after Lung Resection Surgery

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Period and Case Number
3.1.1. Patient Grouping According to Outcome
3.1.2. Detailed Baseline Characteristics
3.2. AI Intervention
3.2.1. AI Algorithms
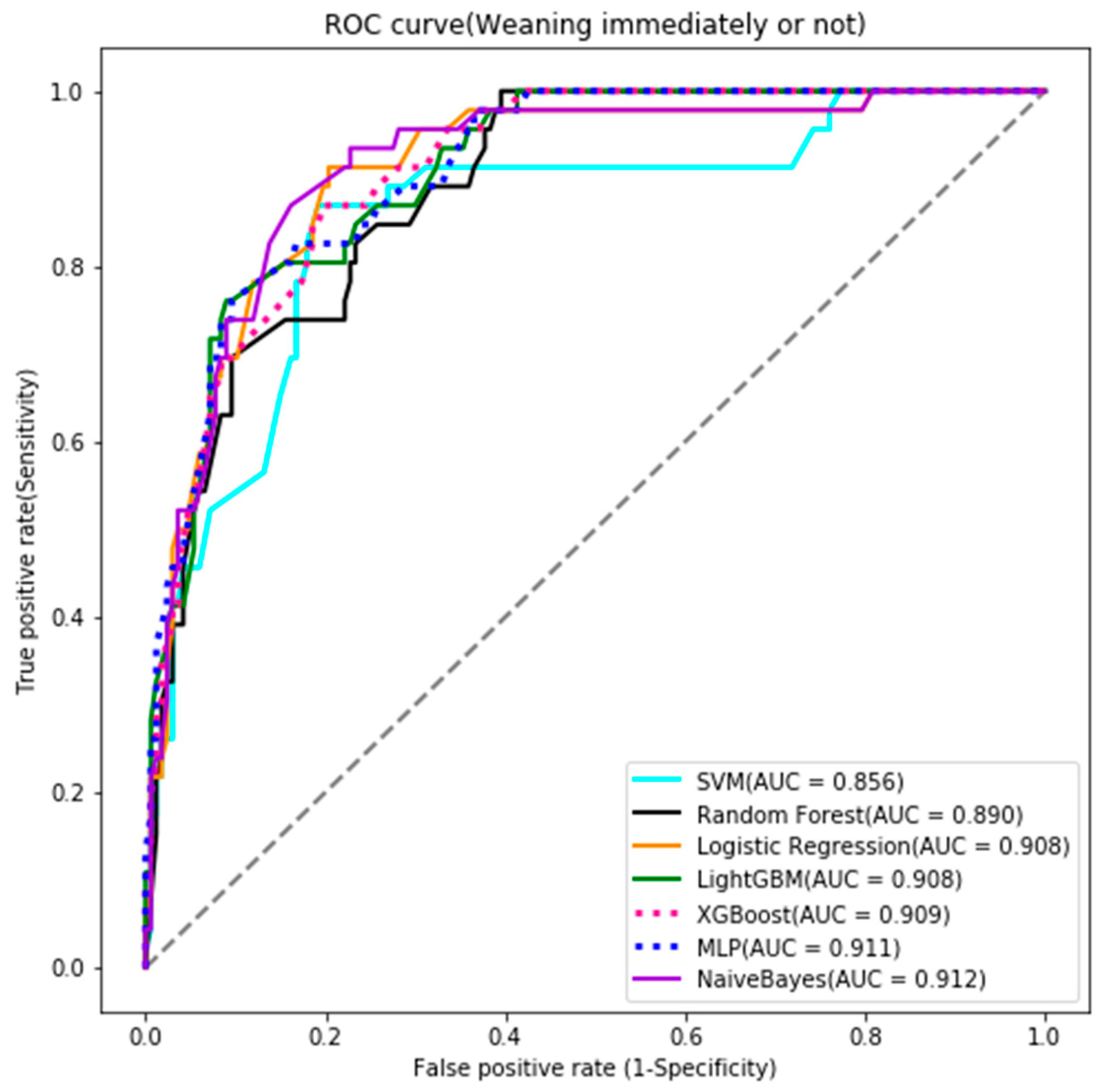
3.2.2. Testing Results of Prediction Models
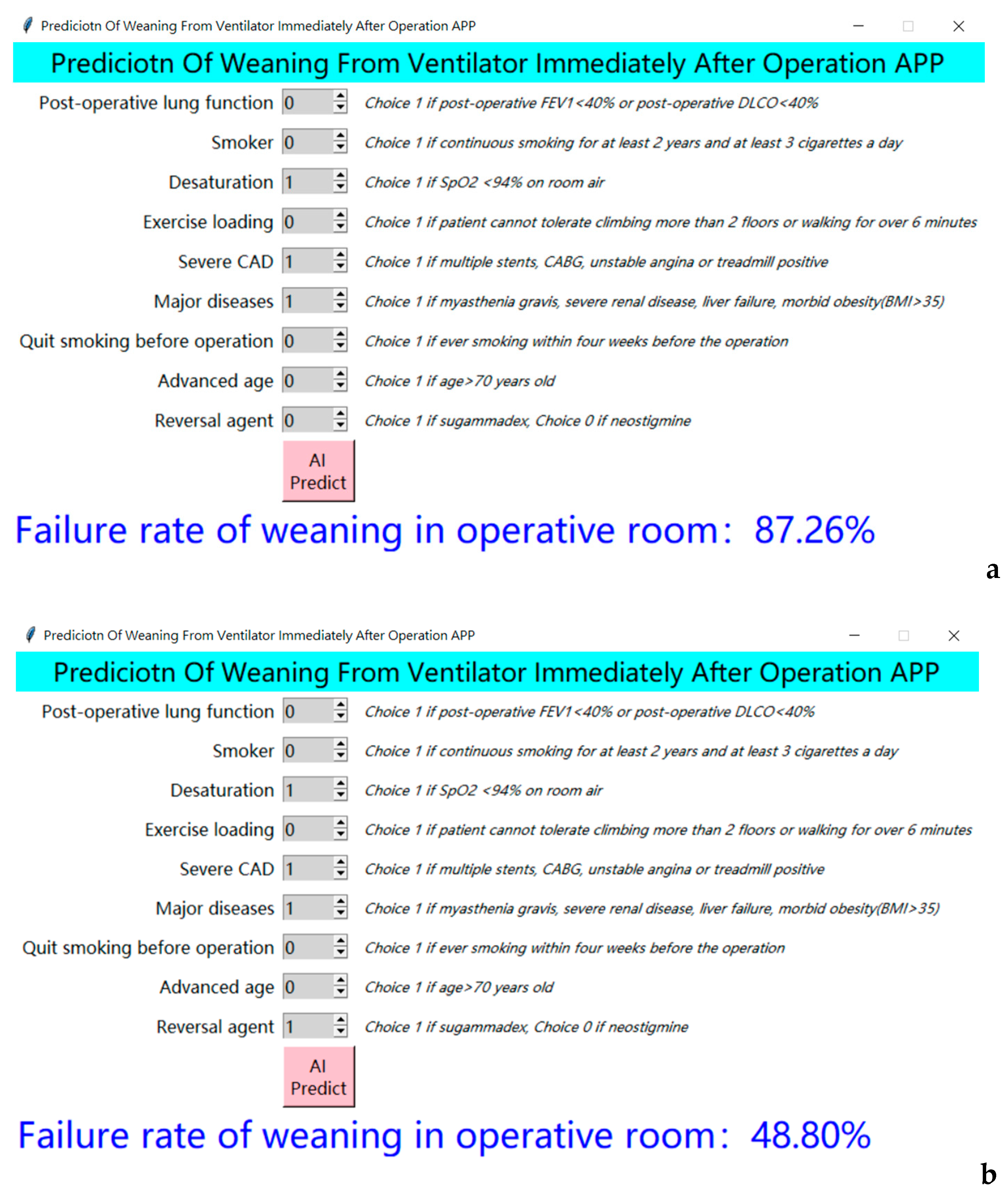
3.3. Clinical Application
Embedment of the above AI Prediction Model in the Pre-Anesthetic Clinic
3.4. Satisfaction Score, before and after AI Application
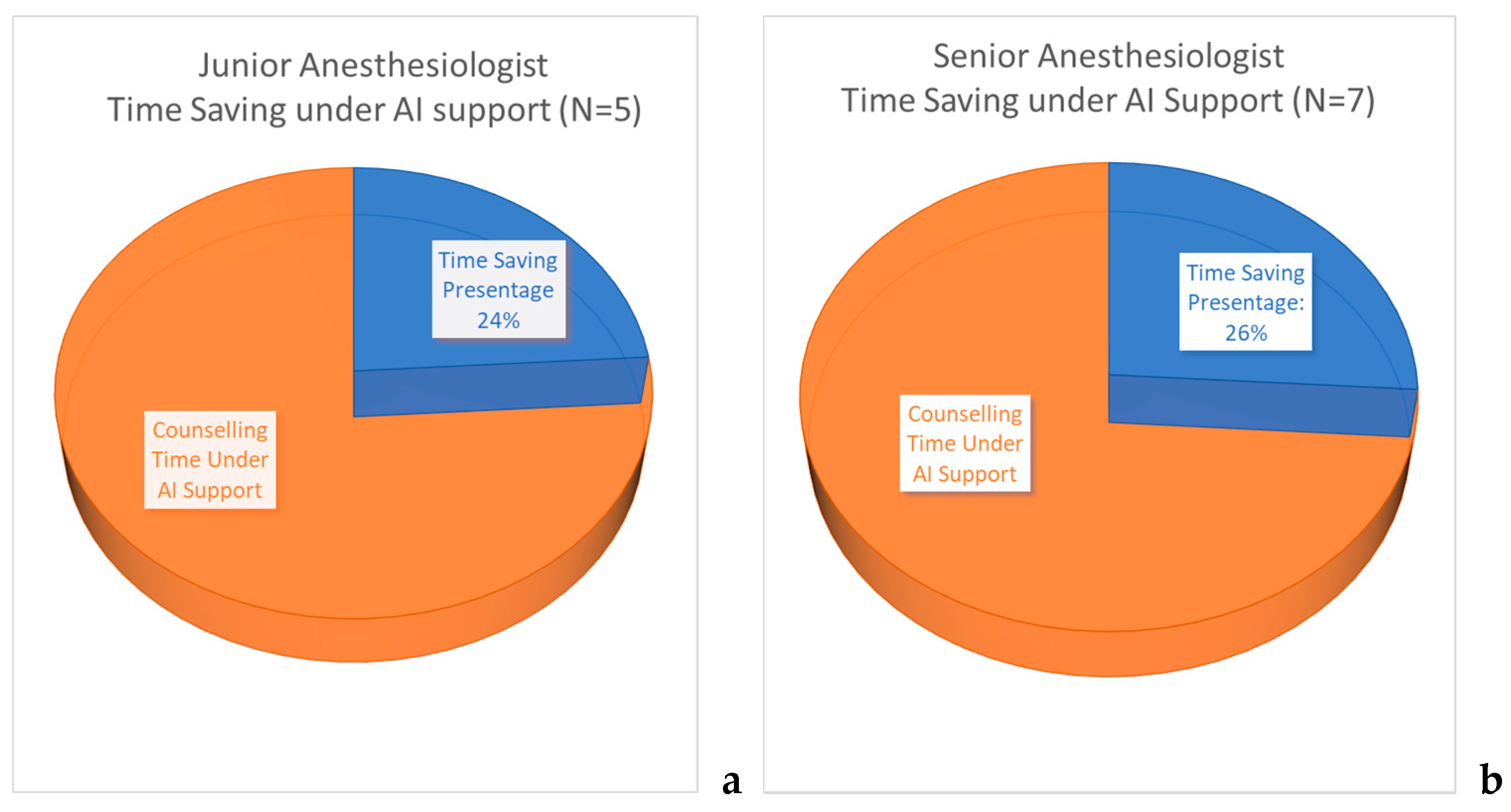
- Junior anesthesiologists (with less than 10 years of experience)
- Senior anesthesiologists (who had more than 10 years of clinical experience)
3.4.1. The Subjective Benefit Scores
3.4.2. Subjective Perception of Time-Saving Percentage
3.4.3. Patient Satisfaction Scores
4. Discussion
5. Limitations
Future Research Directions
6. Conclusions
Practice Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | artificial intelligence |
| AUC | area under receiver operating characteristic curve |
| CAD | coronary artery disease |
| CT | computed tomography |
| FEV1 | forced expiratory volume in one second |
| ICU | intensive care unit |
| Light GBM | Light Gradient Boosting Machine |
| MLP | Multilayer Perceptron |
| ppoDLCO | postoperative diffusing capacity for carbon monoxide |
| ppoFEV1 | postoperative forced expiratory volume in one second |
| ROC curve | receiver operating characteristic curve |
| SVM | Support Vector Machine |
| XGBoost | Extreme Gradient Boosting |
References
- Tseng, C.-H.; Tsuang, B.-J.; Chiang, C.-J.; Ku, K.-C.; Tseng, J.-S.; Yang, T.-Y.; Hsu, K.-H.; Chen, K.-C.; Yu, S.-L.; Lee, W.-C.; et al. The Relationship between Air Pollution and Lung Cancer in Nonsmokers in Taiwan. J. Thorac. Oncol. 2019, 14, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Popper, H.H. Progression and metastasis of lung cancer. Cancer Metastasis Rev. 2016, 35, 75–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Cabo, C.M.; Alarza, F.H.; Rodriguez, A.C.; Delgado, M.M. Perioperative management in thoracic surgery. Med. Intensiv. (Engl. Ed.) 2020, 44, 185–191. [Google Scholar] [CrossRef]
- Alía, I.; Esteban, A. Weaning from mechanical ventilation. Crit. Care 2000, 4, 72–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruartmoner, G.; Mesquida, J.; Masip, J.; Martínez, M.L.; Villagra, A.; Baigorri, F.; Pinsky, M.R.; Artigas, A. Thenar oxygen saturation during weaning from mechanical ventilation: An observational study. Eur. Respir. J. 2013, 43, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, R.D. Miller’s Anesthesia, 8th ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2015; pp. 1945–1953. [Google Scholar]
- Royse, C. Principles and Practice of Anesthesia for Thoracic Surgery, 2nd ed.; Springer Science & Business Media: Berlin, Germany, 2019; Volume 129. [Google Scholar]
- Vaporciyan, A.A.; Merriman, K.W.; Ece, F.; Roth, J.A.; Smythe, W.; Swisher, S.G.; Walsh, G.L.; Nesbitt, J.C.; Putnam, J.B. Incidence of major pulmonary morbidity after pneumonectomy: Association with timing of smoking cessation. Ann. Thorac. Surg. 2002, 73, 420–426. [Google Scholar] [CrossRef]
- Jaklitsch, M.; Billmeier, S. Preoperative Evaluation and Risk Assessment for Elderly Thoracic Surgery Patients. Thorac. Surg. Clin. 2009, 19, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.; Khanna, S.; Argalious, M. Sugammadex for Reversal of Neuromuscular Blockade: Uses and Limitations. Curr. Pharm. Des. 2019, 25, 2140–2148. [Google Scholar] [CrossRef] [PubMed]
- Carron, M.; Ieppariello, G. Benefit of sugammadex in a morbidly obese patient with multiple sclerosis and severe res-piratory dysfunction. J. Clin. Anesth. 2019, 52, 119–120. [Google Scholar] [CrossRef]
- Cho, H.C.; Lee, J.H.; Lee, S.C.; Park, S.Y.; Rim, J.C.; Choi, S.R. Use of sugammadex in lung cancer patients undergoing video-assisted thoracoscopic lobectomy. Korean J. Anesthesiol. 2017, 70, 420–425. [Google Scholar] [CrossRef] [Green Version]
- Cappellini, I.; Ostento, D.; Loriga, B.; Tofani, L.; De Gaudio, A.R.; Adembri, C. Comparison of neostigmine vs. sugam-madex for recovery of muscle function after neuromuscular block by means of diaphragm ultrasonography in micro-laryngeal surgery: A randomised controlled trial. Eur. J. Anaesthesiol. 2020, 37, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Zein, H.; Baratloo, A.; Negida, A.; Safari, S. Ventilator Weaning and Spontaneous Breathing Trials; an Educational Review. Emergency 2016, 4, 65–71. [Google Scholar] [PubMed]
- Harada, T.; Shimizu, T.; Kaji, Y.; Suyama, Y.; Matsumoto, T.; Kosaka, C.; Shimizu, H.; Nei, T.; Watanuki, S. A Perspective from a Case Conference on Comparing the Diagnostic Process: Human Diagnostic Thinking vs. Artificial Intelligence (AI) Decision Support Tools. Int. J. Environ. Res. Public Health 2020, 17, 6110. [Google Scholar] [CrossRef] [PubMed]
- Hargraves, I.G.; Montori, V.M.; Brito, J.P.; Kunneman, M.; Shaw, K.; Lavecchia, C.; Wilson, M.; Walker, L.; Thorsteinsdottir, B. Purposeful SDM: A problem-based approach to caring for patients with shared decision making. Patient Educ. Couns. 2019, 102, 1786–1792. [Google Scholar] [CrossRef]
- Mathijssen, E.G.; Bemt, B.J.V.D.; Hoogen, F.H.V.D.; Popa, C.D.; Vriezekolk, J.E. Interventions to support shared decision making for medication therapy in long term conditions: A systematic review. Patient Educ. Couns. 2020, 103, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Ousseine, Y.M.; Durand, M.-A.; Bouhnik, A.-D.; Smith, A.; Mancini, J. Multiple health literacy dimensions are associated with physicians’ efforts to achieve shared decision-making. Patient Educ. Couns. 2019, 102, 1949–1956. [Google Scholar] [CrossRef] [PubMed]
- Hur, C.; Wi, J.; Kim, Y. Facilitating the Development of Deep Learning Models with Visual Analytics for Electronic Health Records. Int. J. Environ. Res. Public Health 2020, 17, 8303. [Google Scholar] [CrossRef]
- Blagus, R.; Lusa, L. SMOTE for high-dimensional class-imbalanced data. BMC Bioinform. 2013, 14, 106. [Google Scholar] [CrossRef] [Green Version]
- Karabulut, E.M.; Ibrikci, T. Effective Automated Prediction of Vertebral Column Pathologies Based on Logistic Model Tree with SMOTE Preprocessing. J. Med. Syst. 2014, 38, 50. [Google Scholar] [CrossRef] [PubMed]
- Pandey, S.K.; Janghel, R.R. Automatic detection of arrhythmia from imbalanced ECG database using CNN model with SMOTE. Australas. Phys. Eng. Sci. Med. 2019, 42, 1129–1139. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.-H.; Kim, Y.-H. Machine-Learning Approach to Optimize SMOTE Ratio in Class Imbalance Dataset for Intrusion Detection. Comput. Intell. Neurosci. 2018, 2018, 9704672. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, D.; Li, J.; Huang, T.; Cai, Y.-D. Identification and analysis of the cleavage site in a signal peptide using SMOTE, dagging, and feature selection methods. Mol. Omics 2017, 14, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Simon, M.; Bonde, P.; Harris, B.U.; Teuteberg, J.J.; Kormos, R.L.; Antaki, J.F. Prognosis of Right Ventricular Failure in Patients with Left Ventricular Assist Device Based on Decision Tree with SMOTE. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 383–390. [Google Scholar] [CrossRef]
- Wang, Y.; Wu, X.; Chen, Z.; Ren, F.; Feng, L.; Du, Q. Optimizing the Predictive Ability of Machine Learning Methods for Landslide Susceptibility Mapping Using SMOTE for Lishui City in Zhejiang Province, China. Int. J. Environ. Res. Public Health 2019, 16, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, M.; Kajiwara, Y.; Otsuka, A.; Kimura, H. LVQ-SMOTE—Learning Vector Quantization based Synthetic Minority Over–sampling Technique for biomedical data. BioData Min. 2013, 6, 16. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, M.H.; Chen, C.-M.; Hsieh, C.-C.; Chao, C.-M.; Lai, C.-C. Comparison of machine learning models for the prediction of mortality of patients with unplanned extubation in intensive care units. Sci. Rep. 2018, 8, 1–7. [Google Scholar] [CrossRef]
- Jan, S.U.; Lee, Y.-D.; Shin, J.; Koo, I. Sensor Fault Classification Based on Support Vector Machine and Statistical Time-Domain Features. IEEE Access 2017, 5, 8682–8690. [Google Scholar] [CrossRef]
- Zhang, J.; Mucs, D.; Norinder, U.; Svensson, F. LightGBM: An Effective and Scalable Algorithm for Prediction of Chemical Toxicity–Application to the Tox21 and Mutagenicity Data Sets. J. Chem. Inf. Model. 2019, 59, 4150–4158. [Google Scholar] [CrossRef] [PubMed]
- Géron, A.; O’Reilly, M. Hands-On Machine Learning with Scikit-Learn, Keras, and Tensor Flow: Concepts, Tools, and Techniques to Build Intelligent Systems, 6th ed.; O’Reilly: Heidelberg, Germany, 2020. [Google Scholar]
- Lou, W.; Wang, X.; Chen, F.; Chen, Y.; Jiang, B.; Zhang, H. Sequence Based Prediction of DNA-Binding Proteins Based on Hybrid Feature Selection Using Random Forest and Gaussian Naïve Bayes. PLoS ONE 2014, 9, e86703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behnoush, B.; Bazmi, E.; Nazari, S.; Khodakarim, S.; Looha, M.; Soori, H. Machine learning algorithms to predict seizure due to acute tramadol poisoning. Hum. Exp. Toxicol. 2021, 960327121991910. [Google Scholar] [CrossRef]
- Liu, Y.; Bai, F.; Tang, Z.; Liu, N.; Liu, Q. Integrative transcriptomic, proteomic, and machine learning approach to iden-tifying feature genes of atrial fibrillation using atrial samples from patients with valvular heart disease. BMC Cardiovasc. Disord. 2021, 21, 52. [Google Scholar] [CrossRef] [PubMed]
- Golpour, P.; Ghayour-Mobarhan, M.; Saki, A.; Esmaily, H.; Taghipour, A.; Tajfard, M.; Ghazizadeh, H.; Moohebati, M.; Ferns, G.A. Comparison of Support Vector Machine, Naïve Bayes and Logistic Regression for Assessing the Necessity for Coronary Angiography. Int. J. Environ. Res. Public Health 2020, 17, 6449. [Google Scholar] [CrossRef]
- Saeed, U.; Jan, S.U.; Lee, Y.-D.; Koo, I. Fault diagnosis based on extremely randomized trees in wireless sensor networks. Reliab. Eng. Syst. Saf. 2021, 205, 107284. [Google Scholar] [CrossRef]
- Lee, H.-C.; Yoon, H.-K.; Nam, K.; Cho, Y.J.; Kim, T.K.; Kim, W.H.; Bahk, J.-H. Derivation and Validation of Machine Learning Approaches to Predict Acute Kidney Injury after Cardiac Surgery. J. Clin. Med. 2018, 7, 322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, L.; Lam, C.; Mataraso, S.; Allen, A.; Green-Saxena, A.; Pellegrini, E.; Hoffman, J.; Barton, C.; McCoy, A.; Das, R. Mortality prediction model for the triage of COVID-19, pneumonia, and mechanically ventilated ICU patients: A retro-spective study. Ann. Med. Surg. (Lond.) 2020, 59, 207–216. [Google Scholar] [CrossRef]
- Nhu, V.-H.; Shirzadi, A.; Shahabi, H.; Singh, S.K.; Al-Ansari, N.; Clague, J.J.; Jaafari, A.; Chen, W.; Miraki, S.; Dou, J.; et al. Shallow Landslide Susceptibility Mapping: A Comparison between Logistic Model Tree, Logistic Regression, Naïve Bayes Tree, Artificial Neural Network, and Support Vector Machine Algorithms. Int. J. Environ. Res. Public Health 2020, 17, 2749. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, M.; Al-Mallah, M.; Keteyian, S.; Brawner, C.; Ehrman, J.; Sakr, S. Predicting diabetes mellitus using SMOTE and ensemble machine learning approach: The Henry Ford ExercIse Testing (FIT) project. PLoS ONE 2017, 12, e0179805. [Google Scholar] [CrossRef] [PubMed]
- Azarkhish, I.; Raoufy, M.R.; Gharibzadeh, S. Artificial Intelligence Models for Predicting Iron Deficiency Anemia and Iron Serum Level Based on Accessible Laboratory Data. J. Med. Syst. 2012, 36, 2057–2061. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Guo, S.; Ding, B. Technical Blossom in Medical Care: The Influence of Big Data Platform on Medical Innovation. Int. J. Environ. Res. Public Health 2020, 17, 516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J. Big Data-Driven Determinants of Length of Stay for Patients with Hip Fracture. Int. J. Environ. Res. Public Health 2020, 17, 4949. [Google Scholar] [CrossRef] [PubMed]
- Kunneman, M.; Gionfriddo, M.R.; Toloza, F.J.; Gärtner, F.R.; Spencer-Bonilla, G.; Hargraves, I.G.; Erwin, P.J.; Montori, V.M. Humanistic communication in the evaluation of shared decision making: A systematic review. Patient Educ. Couns. 2019, 102, 452–466. [Google Scholar] [CrossRef]
- Cheng, W.-J.; Hung, K.-C.; Ho, C.-H.; Yu, C.-H.; Chen, Y.-C.; Wu, M.-P.; Chu, C.-C.; Chang, Y.-J. Satisfaction in parturients receiving epidural analgesia after prenatal shared decision-making intervention: A prospective, before-and-after cohort study. BMC Pregnancy Child. 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.-H.; Chen, C.-M.; Hsieh, C.-C.; Chao, C.-M.; Lai, C.-C.; Hsieh, M.-J. An Artificial Neural Network Model for Predicting Successful Extubation in Intensive Care Units. J. Clin. Med. 2018, 7, 240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, J.M.; Kim, K.H.; Jeon, K.H.; Lee, S.E.; Lee, H.Y.; Cho, H.J.; Choi, J.O.; Jeon, E.S.; Kim, M.S.; Kim, J.J.; et al. Artificial in-telligence algorithm for predicting mortality of patients with acute heart failure. PLoS ONE 2019, 14, e0219302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syed, L.; Jabeen, S.; S., M.; Alsaeedi, A. Smart healthcare framework for ambient assisted living using IoMT and big data analytics techniques. Futur. Gener. Comput. Syst. 2019, 101, 136–151. [Google Scholar] [CrossRef]
- Rau, C.-S.; Wu, S.-C.; Chuang, J.-F.; Liu, H.-T.; Chien, P.-C.; Hsieh, C.-H. Machine Learning Models of Survival Prediction in Trauma Patients. J. Clin. Med. 2019, 8, 799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, D.S.; Krutzinna, J.; Bruce, I.N.; Griffiths, C.E.; McInnes, I.B.; Barnes, M.R.; Floridi, L. Clinical applications of machine learning algorithms: Beyond the black box. BMJ 2019, 364, l886. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Overall (n = 709) | Wean from Ventilator Immediately (n = 555) | Cannot Wean Immediately (n = 154) | p-Value |
|---|---|---|---|---|
| Postoperative lung function, n (%) | ||||
| ppoDLCO > 40 and ppoFEV1 > 40 | 603 (85.05) | 523 (94.23) | 80 (51.95) | <0.001 |
| ppoDLCO ≤ 40 or ppoFEV1 ≤ 40 | 106 (14.95) | 32 (5.77) | 74 (48.05) | |
| Smoker *, n (%) | ||||
| Never smoke | 468 (66.01) | 388 (69.91) | 80 (51.95) | <0.001 |
| Had history of smoking | 241 (33.99) | 167 (30.09) | 74 (48.05) | |
| Desaturation, n (%) | ||||
| Resting oxygen saturation > 94% | 608 (85.75) | 505 (90.99) | 103 (66.88) | <0.001 |
| Resting oxygen saturation ≤ 94% | 101 (14.25) | 50 (9.01) | 51 (33.12) | |
| Exercise loading, n (%) | ||||
| Patient can climb more than 2 floors without resting in between, or can walk for over 6 min | 627 (88.43) | 526 (94.77) | 101 (65.58) | <0.001 |
| Patient can nether climb more than 2 floors without resting in between nor walk for over 6 min | 82 (11.57) | 29 (5.23) | 53 (34.42) | |
| Severe CAD #, n (%) | ||||
| No history | 623 (87.87) | 511 (92.07) | 112 (72.73) | <0.001 |
| History of severe CAD | 86 (12.13) | 44 (7.93) | 42 (27.27) | |
| Major diseases ^, n (%) | ||||
| No | 620 (87.45) | 511 (92.07) | 109 (70.78) | <0.001 |
| Yes | 89 (12.55) | 44 (7.93) | 45 (29.22) | |
| Quit smoking before operation, n (%) | ||||
| Still smoking | 573 (80.82) | 468 (84.32) | 105 (68.18) | <0.001 |
| Quit smoking (cease smoking for more than 4 weeks before lung resection surgery) | 136 (19.18) | 87 (15.68) | 49 (31.82) | |
| Advanced age, n (%) | ||||
| <70 years | 581 (81.95) | 470 (84.68) | 111 (72.08) | 0.001 |
| ≥70 years | 128 (18.05) | 85 (15.32) | 43 (27.92) | |
| Reversal agent, n (%) | ||||
| neostigmine | 471 (66.43) | 341 (61.44) | 130 (84.42) | <0.001 |
| sugammadex | 238 (33.57) | 214 (38.56) | 24 (15.58) |
| Outcomes and Predictive Models | Accuracy | Sensitivity | Specificity | PPV | NPV | AUC |
|---|---|---|---|---|---|---|
| Wean immediately or not * | ||||||
| Logistic regression | 0.822 | 0.848 | 0.814 | 0.557 | 0.951 | 0.908 |
| Random forest | 0.779 | 0.804 | 0.772 | 0.493 | 0.935 | 0.890 |
| SVM | 0.822 | 0.848 | 0.814 | 0.557 | 0.951 | 0.856 |
| LightGBM | 0.822 | 0.804 | 0.826 | 0.561 | 0.939 | 0.908 |
| XGBoost | 0.817 | 0.826 | 0.814 | 0.551 | 0.944 | 0.909 |
| MLPClassifier | 0.831 | 0.826 | 0.832 | 0.576 | 0.946 | 0.911 |
| Naive Bayes Classifier | 0.845 | 0.870 | 0.838 | 0.597 | 0.959 | 0.912 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.-J.; Hung, K.-C.; Wang, L.-K.; Yu, C.-H.; Chen, C.-K.; Tay, H.-T.; Wang, J.-J.; Liu, C.-F. A Real-Time Artificial Intelligence-Assisted System to Predict Weaning from Ventilator Immediately after Lung Resection Surgery. Int. J. Environ. Res. Public Health 2021, 18, 2713. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052713
Chang Y-J, Hung K-C, Wang L-K, Yu C-H, Chen C-K, Tay H-T, Wang J-J, Liu C-F. A Real-Time Artificial Intelligence-Assisted System to Predict Weaning from Ventilator Immediately after Lung Resection Surgery. International Journal of Environmental Research and Public Health. 2021; 18(5):2713. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052713
Chicago/Turabian StyleChang, Ying-Jen, Kuo-Chuan Hung, Li-Kai Wang, Chia-Hung Yu, Chao-Kun Chen, Hung-Tze Tay, Jhi-Joung Wang, and Chung-Feng Liu. 2021. "A Real-Time Artificial Intelligence-Assisted System to Predict Weaning from Ventilator Immediately after Lung Resection Surgery" International Journal of Environmental Research and Public Health 18, no. 5: 2713. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052713