
SARS-CoV-2 Infection, Risk Perception, Behaviour and Preventive Measures at Schools in Berlin, Germany, during the Early Post-Lockdown Phase: A Cross-Sectional Study

 , , , , , , , , , , , add
Show full author list
, , , , , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Participants
2.2. Data Collection
2.3. Data Processing and Statistical Analysis
3. Results
3.1. Participants
3.2. Prevalence of SARS-CoV-2 Infection and IgG Antibodies
3.3. Signs and Symptoms, and Chronic Conditions
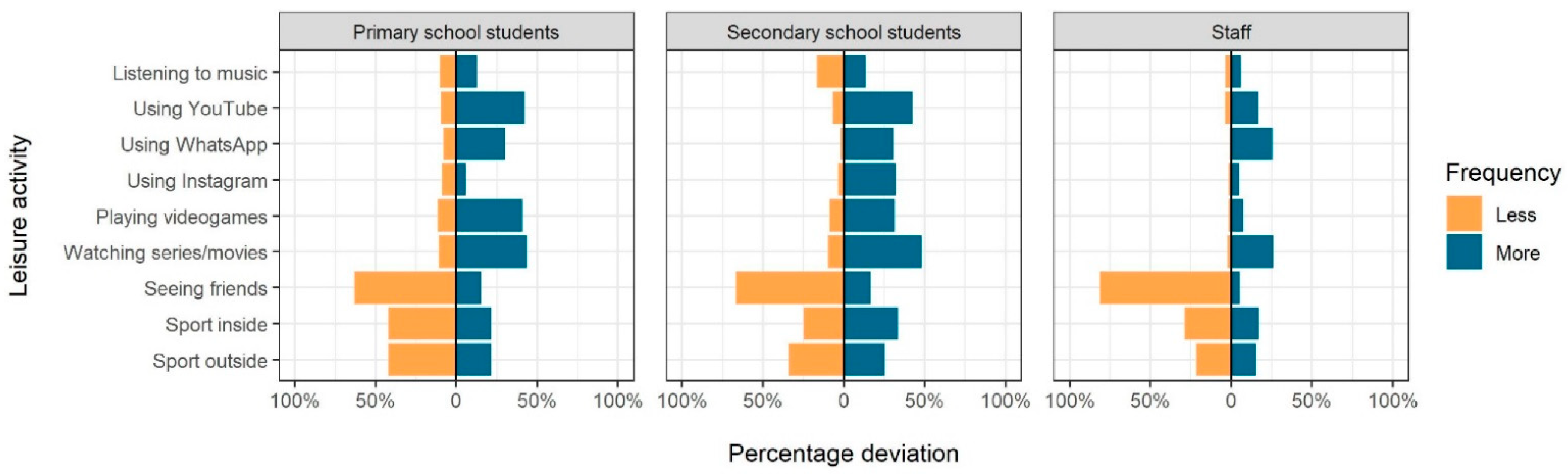
3.4. Household Characteristics and Leisure Activities
3.5. Fear of Infection and Risk Perception
3.6. Individual-Level Health Behaviours
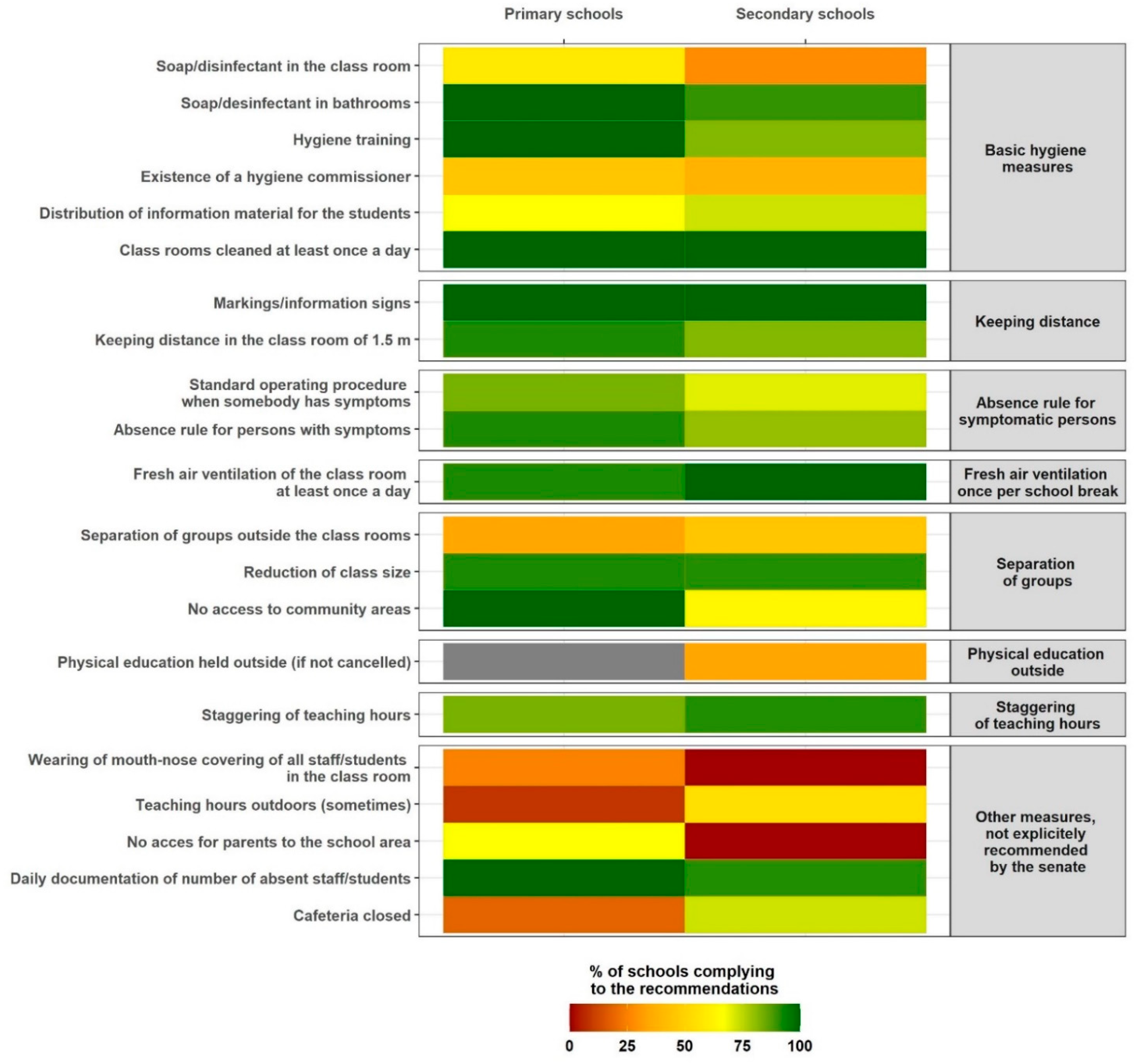
3.7. School-Level Infection Prevention Measures
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Masonbrink, A.R.; Hurley, E. Advocating for Children during the COVID-19 School Closures. Pediatrics 2020, 146. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R.; Nellums, L.B. Considering inequalities in the school closure response to COVID-19. Lancet Glob. Health 2020, 8, e644. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Margaritis, I.; Houdart, S.; El Ouadrhiri, Y.; Bigard, X.; Vuillemin, A.; Duché, P. How to deal with COVID-19 epidemic-related lockdown physical inactivity and sedentary increase in youth? Adaptation of Anses’ benchmarks. Arch. Public Health 2020, 78, 52. [Google Scholar] [CrossRef]
- Bayham, J.; Fenichel, E.P. Impact of school closures for COVID-19 on the US health-care workforce and net mortality: A modelling study. Lancet Public Health 2020, 5, e271–e278. [Google Scholar] [CrossRef]
- Nagata, J.M.; Abdel Magid, H.S.; Pettee Gabriel, K. Screen Time for Children and Adolescents during the Coronavirus Disease 2019 Pandemic. Obesity 2020, 28, 1582–1583. [Google Scholar] [CrossRef]
- Snape, M.D.; Viner, R.M. COVID-19 in children and young people. Science 2020, 370, 286–288. [Google Scholar] [CrossRef]
- Regional Office for Health and Social Affairs Berlin (LAGeSo). COVID-19 in Berlin, Distribution in the Districts-Complete Overview. Available online: https://daten.berlin.de/datensaetze/covid-19-berlin-verteilung-den-bezirken-gesamt%C3%BCbersicht (accessed on 24 October 2020). (In German).
- Merckx, J.; Labrecque, J.A.; Kaufman, J.S. Transmission of SARS-CoV-2 by Children. Dtsch. Arztebl. Int. 2020, 117, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, E.; Lipsitch, M.; Cevik, M. On the effect of age on the transmission of SARS-CoV-2 in households, schools and the community. J. Infect. Dis. 2021, 223, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Ehrhardt, J.; Ekinci, A.; Krehl, H.; Meincke, M.; Finci, I.; Klein, J.; Geisel, B.; Wagner-Wiening, C.; Eichner, M.; Brockmann, S.O. Transmission of SARS-CoV-2 in children aged 0 to 19 years in childcare facilities and schools after their reopening in May 2020, Baden-Württemberg, Germany. Eurosurveillance 2020, 25, 2001587. [Google Scholar] [CrossRef]
- Im Kampe, E.O.; Lehfeld, A.S.; Buda, S.; Buchholz, U.; Haas, W. Surveillance of COVID-19 school outbreaks, Germany, March to August 2020. Eurosurveillance 2020, 25, 2001645. [Google Scholar] [CrossRef]
- Isphording, I.E.; Lipfert, M.; Pestel, N. School Re-Openings after Summer Breaks in Germany Did Not Increase SARS-CoV-2 Cases; Discussion Paper No. 13790; Institute of Labor Economics: Bonn, Germany, 2020. [Google Scholar]
- Ludvigsson, J.F. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020, 109, 1088–1095. [Google Scholar] [CrossRef]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hippich, M.; Holthaus, L.; Assfalg, R.; Zapardiel Gonzalo, J.M.; Kapfelsperger, H.; Heigermoser, M.; Haupt, F.; Ewald, D.A.; Welzhofer, T.C.; Marcus, B.A.; et al. A Public health antibody screening indicates a six-fold higher SARS-CoV-2 exposure rate than reported cases in children. Med 2021, 2, 149–163.e4. [Google Scholar] [CrossRef]
- Macartney, K.; Quinn, H.E.; Pillsbury, A.J.; Koirala, A.; Deng, L.; Winkler, N.; Katelaris, A.L.; O’Sullivan, M.V.; Dalton, C.; Wood, N.; et al. Transmission of SARS-CoV-2 in Australian educational settings: A prospective cohort study. Lancet Child Adolesc. Health 2020, 4, 807–816. [Google Scholar] [CrossRef]
- Heavey, L.; Casey, G.; Kelly, C.; Kelly, D.; McDarby, G. No evidence of secondary transmission of COVID-19 from children attending school in Ireland. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Schwarzer, R. Modeling Health Behavior Change: How to Predict and Modify the Adoption and Maintenance of Health Behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Wittmann, N.; Sallmon, S.; Meinlschmidt, G. Gesundheits- und Sozialstrukturatlas für die Bundesrepublik Deutschland [Publication in German]. 2015. Available online: https://www.berlin.de/sen/gesundheit/service/gesundheitsberichterstattung/veroeffentlichungen/spezialberichte/ (accessed on 15 December 2020).
- Berlin Senate Administration for Education, Youth and Family. Musterhygieneplan Corona für die Berliner Schulen [Publication in German]. 2020. Available online: https://www.berlin.de/sen/bjf/coronavirus/aktuelles/schrittweise-schuloeffnung/20200623_musterhygieneplan-corona-fuer-die-berliner-schulen.pdf (accessed on 15 December 2020).
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Castagnoli, R.; Votto, M.; Licari, A.; Brambilla, I.; Bruno, R.; Perlini, S.; Rovida, F.; Baldanti, F.; Marseglia, G.L. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr. 2020, 174, 882–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OECD. Bildung auf Einen Blick 2020: OECD-Indikatoren. 2020. Available online: https://0-www-oecd--ilibrary-org.brum.beds.ac.uk/education/bildung-auf-einen-blick-2020-oecd-indikatoren_6001821nw;jsessionid=IuMPVy18f62Xhu7lTSzxz-Qj.ip-10-240-5-151 (accessed on 15 December 2020).
- Scheuch, K.; Haufe, E.; Seibt, R. Teachers’ Health. Dtsch. Arztebl. Int. 2015, 112, 347–356. [Google Scholar] [CrossRef] [Green Version]
- Xiang, M.; Zhang, Z.; Kuwahara, K. Impact of COVID-19 pandemic on children and adolescents’ lifestyle behavior larger than expected. Prog. Cardiovasc. Dis. 2020, 63, 531–532. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- López-Bueno, R.; López-Sánchez, G.F.; Casajús, J.A.; Calatayud, J.; Tully, M.A.; Smith, L. Potential health-related behaviors for pre-school and school-aged children during COVID-19 lockdown: A narrative review. Prev. Med. 2020, 106349. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Primary School Students (N = 193) | Secondary School Students (N = 192) | Staff (N = 150) | ||||
|---|---|---|---|---|---|---|
| % | n/N | % | n/N | % | n/N | |
| On examination day: | ||||||
| Any of the defined symptoms | 18.8 | 36/192 | 16.3 | 31/190 | 12.2 | 18/148 |
| Headache | 6.8 | 13/192 | 6.8 | 13/192 | 7.4 | 11/148 |
| Rhinorrhoea | 7.8 | 15/192 | 7.8 | 15/192 | 2.0 | 3/148 |
| Cough | 5.7 | 11/192 | 2.6 | 5/192 | 3.4 | 5/148 |
| Sore throat | 3.1 | 6/192 | 3.6 | 7/192 | 0.7 | 1/148 |
| Diarrhoea | 2.1 | 4/192 | 0 | 0/192 | 1.4 | 2/148 |
| Limb pain | 1.0 | 2/192 | 0 | 0/192 | 0 | 0/148 |
| Loss of smell and taste | 0.5 | 1/190 | 0.5 | 1/190 | 0 | 0/148 |
| Self-reported fever | 1.6 | 3/192 | 0 | 0/192 | 2.0 | 3/148 |
| Fever ≥ 37.5 °C; measured | 2.1 | 4/192 | 3.1 | 6/192 | 1.3 | 2/149 |
| During preceding 14 days: | ||||||
| Any of the defined symptoms | 40.6 | 76/187 | 54.9 | 101/184 | 48.0 | 71/148 |
| Headache | 21.5 | 41/191 | 35.4 | 67/189 | 32.9 | 49/149 |
| Rhinorrhoea | 11.1 | 21/190 | 20.2 | 38/188 | 7.5 | 11/146 |
| Cough | 5.3 | 10/190 | 11.6 | 22/189 | 4.7 | 7/149 |
| Sore throat | 7.0 | 13/187 | 14.4 | 27/187 | 6.9 | 10/145 |
| Diarrhoea | 7.0 | 13/186 | 4.9 | 9/184 | 7.6 | 11/145 |
| Limb pain | 3.7 | 7/189 | 5.4 | 10/186 | 3.5 | 5/144 |
| Loss of smell and taste | 0 | 0/191 | 1.6 | 3/185 | 0 | 0/147 |
| Breathlessness | 4.7 | 9/192 | 11.1 | 21/189 | 6.1 | 9/148 |
| Tiredness | 4.8 | 9/188 | 8.0 | 15/188 | 18.8 | 28/149 |
| Chills | 0 | 0/187 | 1.6 | 3/187 | 2.1 | 3/146 |
| Chest pain | 1.6 | 3/188 | 4.3 | 8/187 | 3.4 | 5/146 |
| Self-reported fever | 0.5 | 1/190 | 0.5 | 1/189 | 2.0 | 3/149 |
| Self-reported chronic diseases | ||||||
| Any | 13.0 | 25/192 | 18.1 | 34/188 | 44.2 | 65/147 |
| High blood pressure | 0 | 0/193 | 0 | 0/192 | 14.0 | 21/150 |
| Chronic heart disease | 0 | 0/193 | 2.1 | 4/192 | 4.7 | 7/150 |
| Obesity | 1.0 | 2/193 | 0 | 0/192 | 6.7 | 10/150 |
| Diabetes mellitus | 0 | 0/193 | 0 | 0/192 | 0.7 | 1/150 |
| Chronic lung disease | 4.1 | 8/193 | 4.2 | 8/192 | 4.0 | 6/150 |
| Immunodeficiency | 0.5 | 1/193 | 0.5 | 1/192 | 1.3 | 2/150 |
| Cancer | 0 | 0/193 | 0 | 0/192 | 2.0 | 3/150 |
| Other | 8.8 | 17/193 | 10.4 | 20/192 | 21.3 | 32/150 |
| Regular medication | 7.8 | 15/192 | 12.2 | 23/188 | 39.3 | 57/145 |
| Allergies | 29.4 | 55/187 | 26.5 | 48/181 | 40.7 | 57/140 |
| Smoking | - | - | 5.3 | 10/188 | 23.8 | 35/147 |
| Primary School Students (N = 193) | Secondary School Students (N = 192) | Staff (N = 150) | ||||
|---|---|---|---|---|---|---|
| % | n/N | % | n/N | % | n/N | |
| Fear of infection | ||||||
| Not at all to a bit | 72.9 | 137/188 | 70.0 | 133/190 | 51.7 | 77/149 |
| Medium to very strong | 27.1 | 51/188 | 30.0 | 57/190 | 48.3 | 72/149 |
| Risk perception | ||||||
| Very low to rather low | 72.9 | 137/188 | 60.5 | 115/190 | 40.9 | 61/149 |
| Moderate to very high | 27.1 | 51/188 | 39.5 | 75/190 | 59.1 | 88/149 |
| Hand washing/using handrub per day | ||||||
| 0–1 time | 1.0 | 2/192 | 4.7 | 9/191 | 0 | 0/149 |
| 2–4 times | 34.4 | 66/192 | 39.3 | 75/191 | 12.1 | 18/149 |
| ≥5 times | 64.6 | 124/192 | 56.0 | 107/191 | 87.9 | 131/149 |
| Physical distancing at school | ||||||
| Never to rarely | 2.6 | 5/189 | 15.8 | 30/190 | 3.4 | 5/147 |
| Sometimes | 16.4 | 31/189 | 29.5 | 56/190 | 19.7 | 29/147 |
| Frequently to always | 81.0 | 153/189 | 54.7 | 104/190 | 76.9 | 113/147 |
| Facemask wearing at school | ||||||
| Never to rarely | 38.9 | 74/190 | 53.7 | 102/190 | 38.5 | 57/148 |
| Sometimes | 11.1 | 21/190 | 11.1 | 21/190 | 21.6 | 32/148 |
| Frequently to always | 50.0 | 95/190 | 35.3 | 67/190 | 39.9 | 59/148 |
| Situations of facemask wearing in the school (multiple response scale) | ||||||
| Never | 32.9 | 55/167 | 29.4 | 55/187 | 25.5 | 36/141 |
| In class | 38.3 | 64/167 | 9.6 | 18/187 | 54.6 | 77/141 |
| In schoolyard | 32.9 | 55/167 | 35.8 | 67/187 | 22.7 | 32/141 |
| On way to school | 24.0 | 40/167 | 48.1 | 90/187 | 24.8 | 35/141 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hommes, F.; van Loon, W.; Thielecke, M.; Abramovich, I.; Lieber, S.; Hammerich, R.; Gehrke-Beck, S.; Linzbach, E.; Schuster, A.; von dem Busche, K.; et al. SARS-CoV-2 Infection, Risk Perception, Behaviour and Preventive Measures at Schools in Berlin, Germany, during the Early Post-Lockdown Phase: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 2739. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052739
Hommes F, van Loon W, Thielecke M, Abramovich I, Lieber S, Hammerich R, Gehrke-Beck S, Linzbach E, Schuster A, von dem Busche K, et al. SARS-CoV-2 Infection, Risk Perception, Behaviour and Preventive Measures at Schools in Berlin, Germany, during the Early Post-Lockdown Phase: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(5):2739. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052739
Chicago/Turabian StyleHommes, Franziska, Welmoed van Loon, Marlene Thielecke, Igor Abramovich, Sascha Lieber, Ralf Hammerich, Sabine Gehrke-Beck, Elisabeth Linzbach, Angela Schuster, Katja von dem Busche, and et al. 2021. "SARS-CoV-2 Infection, Risk Perception, Behaviour and Preventive Measures at Schools in Berlin, Germany, during the Early Post-Lockdown Phase: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 5: 2739. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052739