
The Effects of Abdominal Hypopressive Training on Postural Control and Deep Trunk Muscle Activation: A Randomized Controlled Trial


 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
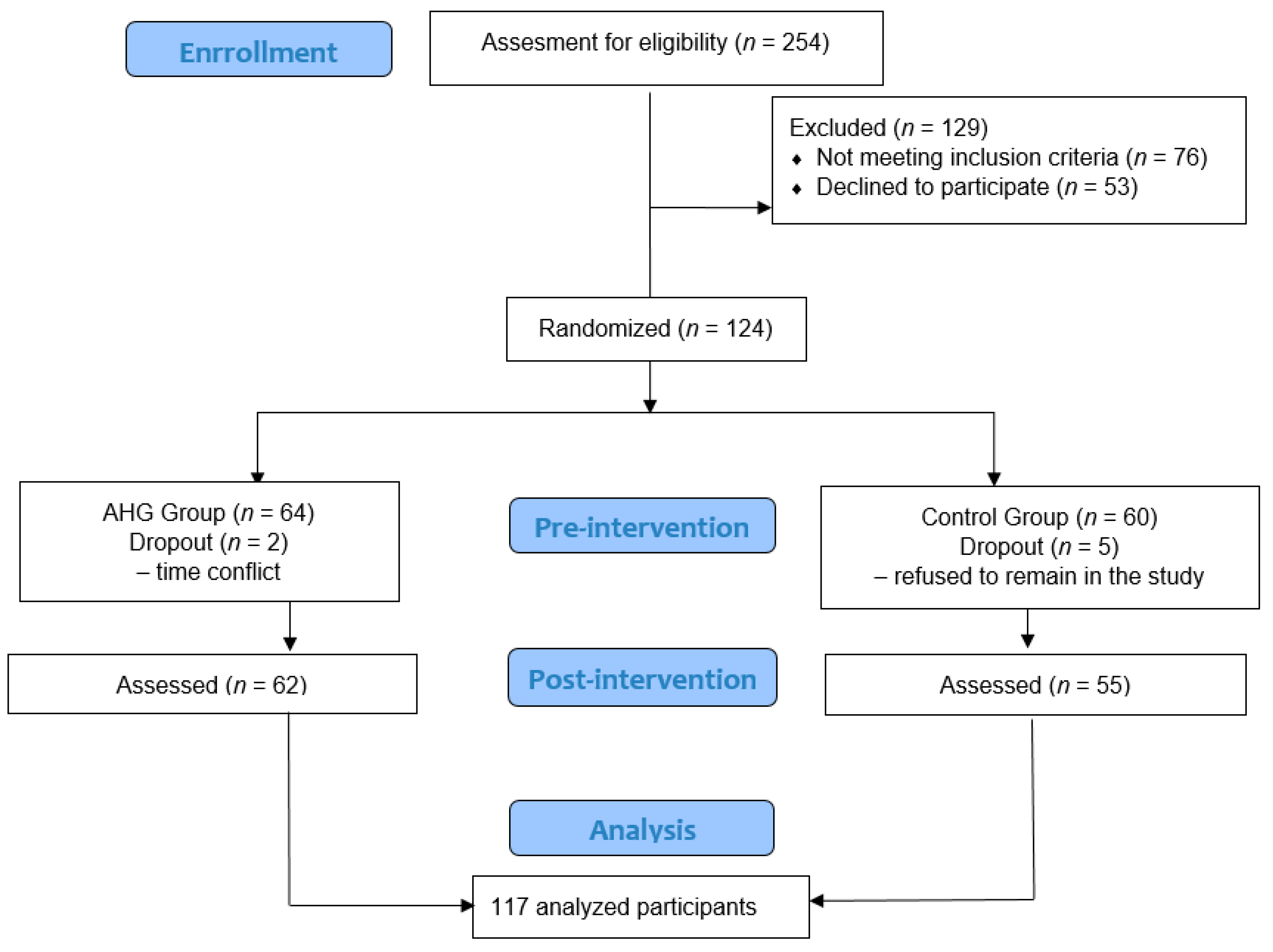
2.1. Study Design and Subjects
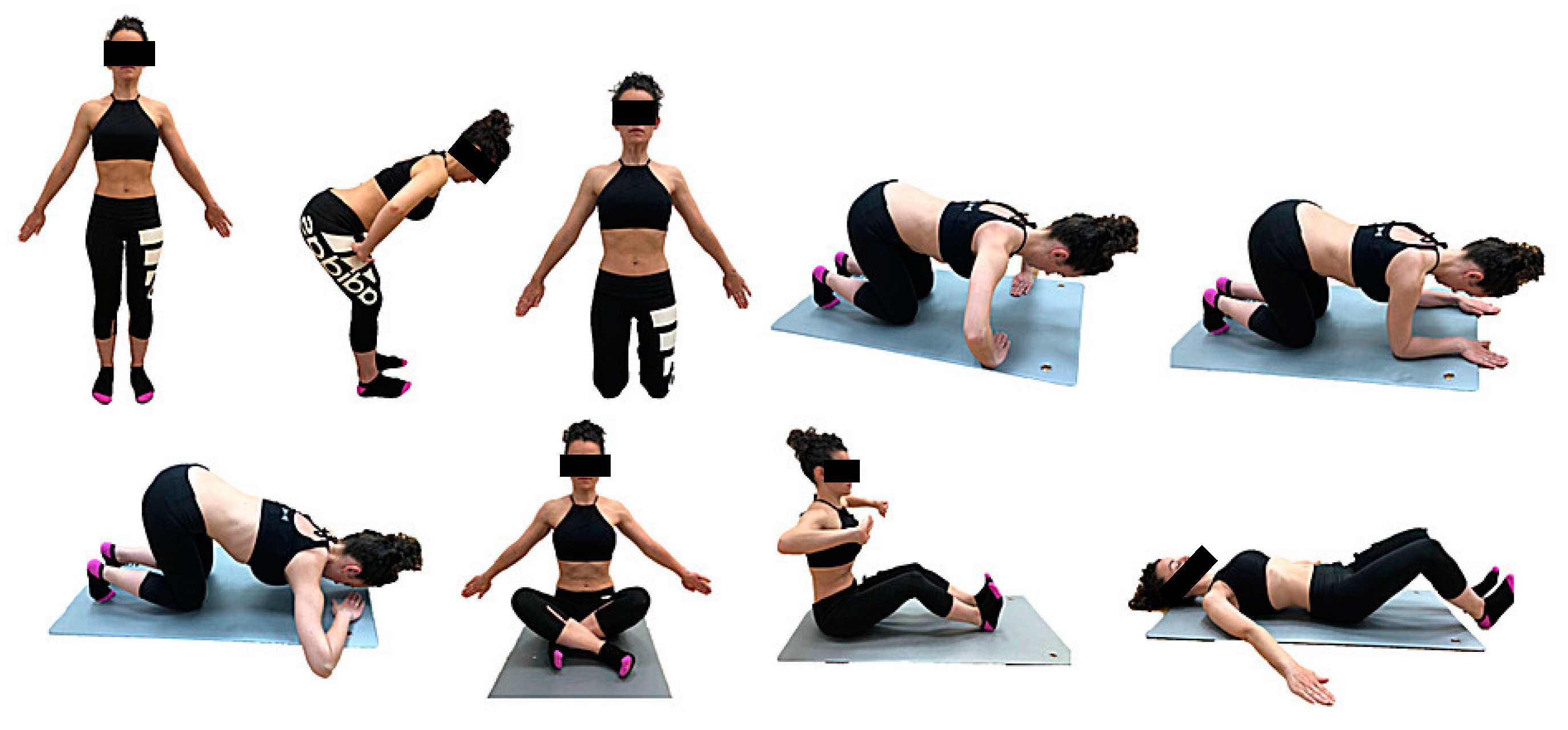
2.2. Procedure
2.3. Outcome Measures, Variables, and Instruments
2.4. Primary Outcome
2.5. Secondary Outcome
2.6. Statistical Analysis
3. Results
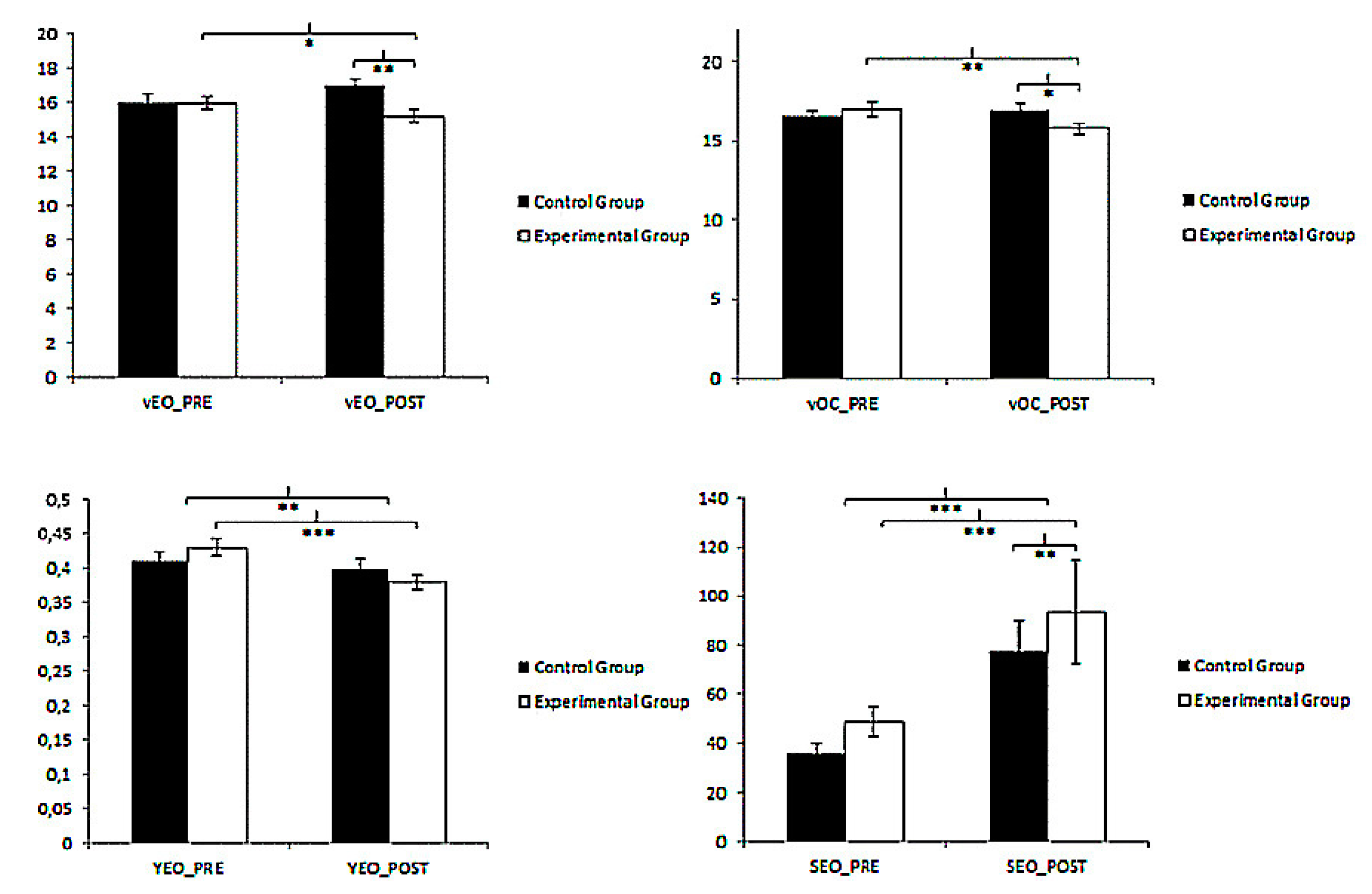
3.1. Postural Control
3.2. TrA Activation
4. Discussion
4.1. Postural Control
4.2. Deep Trunk Muscles
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Casonatto, J.; Yamacita, C.M. Pilates exercise and postural balance in older adults: A systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2019, 48, 102232. [Google Scholar] [CrossRef]
- Szafraniec, R.; Barańska, J.; Kuczyński, M. Acute effects of core stability exercises on balance control. Acta Bioeng. Biomech. 2018, 20. [Google Scholar] [CrossRef]
- Rosker, J.; Markovic, G.; Sarabon, N. Effects of vertical center of mass redistribution on body sway parameters during quiet standing. Gait Posture 2011, 33, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Chmielewska, D.; Stania, M.; Słomka, K.; Błaszczak, E.; Taradaj, J.; Dolibog, P.; Juras, G. Static postural stability in women with stress urinary incontinence: Effects of vision and bladder filling. Neurourol. Urodyn. 2017, 36, 2019–2027. [Google Scholar] [CrossRef] [PubMed]
- Nagar, V.R.; Sawyer, S.F.; James, C.R.; Brismée, J.; Hooper, T.L.; Sizer, P.S. The effects of volitional preemptive abdominal contraction on postural control responses in healthy subjects. PM&R 2015, 7, 1142–1151. [Google Scholar]
- Ehsani, F.; Sahebi, N.; Shanbehzadeh, S.; Arab, A.M.; ShahAli, S. Stabilization exercise affects function of transverse abdominis and pelvic floor muscles in women with postpartum lumbo-pelvic pain: A double-blinded randomized clinical trial study. Int. Urogynecol. J. 2020, 31, 197–204. [Google Scholar] [CrossRef]
- Kibler, W.B.; Press, J.; Sciascia, A. The role of core stability in athletic function. Sports Med. 2006, 36, 189–198. [Google Scholar] [CrossRef]
- Weber, T.; Salomoni, S.E.; Debuse, D.; Hug, F.; Caplan, N.; De Martino, E.; Scott, J.; Hides, J.; Hodges, P. Functional behaviour of spinal muscles after training with an exercise device developed to recruit and train postural muscles. Gait Posture 2018, 66, 189–193. [Google Scholar] [CrossRef] [Green Version]
- Emami, F.; Yoosefinejad, A.K.; Razeghi, M. Correlations between core muscle geometry, pain intensity, functional disability and postural balance in patients with nonspecific mechanical low back pain. Med. Eng. Phys. 2018, 60, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Larson, D.J.; Brown, S.H. The effects of trunk extensor and abdominal muscle fatigue on postural control and trunk proprioception in young, healthy individuals. Hum. Mov. Sci. 2018, 57, 13–20. [Google Scholar] [CrossRef]
- Caufriez, M.; Fernández, J.; Guignel, G.; Heimann, A. Comparación de las variaciones de presión abdominal en medio acuático y aéreo durante la realización de cuatro ejercicios abdominales hipopresivos. Rev. Iberoam. Fisioter. Kinesiol. 2007, 10, 12–23. [Google Scholar] [CrossRef]
- Bellido-Fernández, L.; Jiménez-Rejano, J.; Chillón-Martínez, R.; Gómez-Benítez, M.; De-La-Casa-Almeida, M.; Rebollo-Salas, M. Effectiveness of massage therapy and abdominal hypopressive gymnastics in nonspecific chronic low back pain: A randomized controlled pilot study. Evid. Based Complement. Altern. Med. 2018, 2018, 3684194. [Google Scholar]
- Juez, L.; Núñez-Córdoba, J.M.; Couso, N.; Aubá, M.; Alcázar, J.L.; Mínguez, J.Á. Hypopressive technique versus pelvic floor muscle training for postpartum pelvic floor rehabilitation: A prospective cohort study. Neurourol. Urodyn. 2019, 38, 1924–1931. [Google Scholar] [CrossRef]
- Sáez, M.M.Á.; Rebullido, T.R.; Medrano, I.C.; Soidán, J.L.G.; Tormo, J.M.C. ¿Puede un programa de ocho semanas basado en la técnica hipopresiva producir cambios en la función del suelo pélvico y composición corporal de jugadoras de rugby? RETOS Nuevas Tend. Educ. Fís. Deporte Recreación 2016, 30, 26–29. [Google Scholar]
- Navarro Brazález, B.; Sánchez Sánchez, B.; Prieto Gómez, V.; De La Villa Polo Pedro McLean, L.; Torres Lacomba, M. Pelvic floor and abdominal muscle responses during hypopressive exercises in women with pelvic floor dysfunction. Neurourol. Urodyn. 2020, 39, 793–803. [Google Scholar] [CrossRef]
- Stüpp, L.; Resende, A.P.M.; Petricelli, C.D.; Nakamura, M.U.; Alexandre, S.M.; Zanetti, M.R.D. Pelvic floor muscle and transversus abdominis activation in abdominal hypopressive technique through surface electromyography. Neurourol. Urodyn. 2011, 30, 1518–1521. [Google Scholar] [CrossRef] [PubMed]
- Caufriez, M.; Fernández, J.; Fanzel, R.; Snoeck, T. Efectos de un programa de entrenamiento estructurado de Gimnasia Abdominal Hipopresiva sobre la estática vertebral cervical y dorsolumbar. Fisioterapia 2006, 28, 205–216. [Google Scholar] [CrossRef]
- Rial, T.; Negreira, N.; Álvarez-Sáez, M.; García-Soidán, J. ¿Puede un programa de ejercicio hipopresivo influir sobre la extensibilidad isquiosural y movilidad lumbar de jugadoras de fútbol? Rev. Prep. Fís. Fútbol 2007, 1889, 5050. [Google Scholar]
- Guillaumes, S.; O’Callaghan, C.A. Versión en español del software gratuito OxMaR para minimización y aleatorización de estudios clínicos. Gac. Sanit. 2019, 33, 395–397. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.; Heinemann, A.W.; Roberts, J. Elevating the quality of disability and rehabilitation research: Mandatory use of the reporting guidelines. Ann. Phys. Rehabil. Med. 2014, 57, 558–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rial, T.; Pinsach, P. Practical Manual Low Pressure Fitness Level 1; International Hypopressive & Physical Therapy Institute: Vigo, Spain, 2017. [Google Scholar]
- Strzecha, M.; Knapik, H.; Baranowski, P.; Pękala, A.; Pasiak, J. Clinical significance of measurement reliability of diagnostic tools used for evaluation of body posture. Gabinet Fizjoterapeuty Rehabil. 2014, 1, 28–32. [Google Scholar]
- Hita-Contreras, F.; Zagalaz-Anula, N.; Martínez-Amat, A.; Cruz-Díaz, D.; Sánchez-Montesinos, I.; Aibar-Almazán, A.; Rafael, L.-V. Sleep quality and its association with postural stability and fear of falling among Spanish postmenopausal women. Menopause 2018, 25, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Norré, M.E. Posture in otoneurology. Acta Otorhinolaryngol. Belg. 1990, 44, 363. [Google Scholar]
- Hita-Contreras, F.; Martínez-Amat, A.; Lomas-Vega, R.; Álvarez, P.; Mendoza, N.; Romero-Franco, N.; Aránega, A.; Martínez-López, E. Predictive value of stabilometry and fear of falling on falls in postmenopausal women. Climacteric 2013, 16, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Baydal-Bertomeu, J.; Guillem, R.B.I.; Soler-Gracia, C.; De Moya, M.P.; Prat, J.; De Guzmán, R.B. Determinación de los patrones de comportamiento postural en población sana española. Acta Otorrinolaringol. Esp. 2004, 55, 260–269. [Google Scholar] [CrossRef]
- Aibar-Almazán, A.; Martínez-Amat, A.; Cruz-Díaz, D.; De la Torre-Cruz Manuel, J.; Jiménez-García, J.D.; Zagalaz-Anula, N.; Pérez-Herrezuelo, I.; Hita-Contreras, F. Effects of Pilates on fall risk factors in community-dwelling elderly women: A randomized, controlled trial. Eur. J. Sport Sci. 2019, 19, 1386–1394. [Google Scholar] [CrossRef]
- Cho, S.; Kim, K.H.; Baek, I.; Goo, B. Comparison of contraction rates of abdominal muscles of chronic low back pain patients in different postures. J. Phys. Ther. Sci. 2013, 25, 907–909. [Google Scholar] [CrossRef] [Green Version]
- Taghipour, M.; Mohseni-Bandpei, M.A.; Behtash, H.; Abdollahi, I.; Rajabzadeh, F.; Pourahmadi, M.R.; Emami, M. Reliability of Real-time Ultrasound Imaging for the Assessment of Trunk Stabilizer Muscles: A Systematic Review of the Literature. J. Ultrasound Med. 2019, 38, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Morán, M.T.C. Estudio comparativo de programas para cálculo del tamaño muestral. Metodol. Encuestas 2009, 11, 121–129. [Google Scholar]
- Garrido-Castells, X.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C.; Losa-Iglesias, M.E.; Palomo-López, P.; Navarro-Flores, E.; López-López, D. Effectiveness of Leukocyte and Platelet-Rich Fibrin versus Nitrofurazone on Nail Post-Surgery Bleeding and Wound Cicatrization Period Reductions: A Randomized Single Blinded Clinical Trial. J. Clin. Med. 2019, 8, 1552. [Google Scholar] [CrossRef] [Green Version]
- Mesquita, L.S.; de Carvalho, F.T.; Freire, L.S.; Neto, O.P.; Zângaro, R.A. Effects of two exercise protocols on postural balance of elderly women: A randomized controlled trial. BMC Geriatr. 2015, 15, 61. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Hillsdale, NJ: Lawrence Erlbaum, 1988. [Google Scholar] [CrossRef]
- Ferraro, R.; Garman, S.; Taylor, R.; Parrott, J.S.; Kadlowec, J. The effectiveness of transverse abdominis training on balance, postural sway and core muscle recruitment patterns: A pilot study comparison across age groups. J. Phys. Ther. Sci. 2019, 31, 729–737. [Google Scholar] [CrossRef]
- Cohen, R.G.; Baer, J.L.; Ravichandra, R.; Kral, D.; McGowan, C.; Cacciatore, T.W. Lighten Up! Postural Instructions Affect Static and Dynamic Balance in Healthy Older Adults. Innov. Aging 2020, 4, igz056. [Google Scholar] [CrossRef] [Green Version]
- Kocjan, J.; Adamek, M.; Gzik-Zroska, B.; Czyżewski, D.; Rydel, M. Network of breathing. Multifunctional role of the diaphragm: A review. Adv. Respir. Med. 2017, 85, 224–232. [Google Scholar] [CrossRef] [Green Version]
- Kaji, A.; Sasagawa, S.; Kubo, T.; Kanehisa, H. Transient effect of core stability exercises on postural sway during quiet standing. J. Strength Cond. Res. 2010, 24, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Nepocatych, S.; Ketcham, C.J.; Vallabhajosula, S.; Balilionis, G. The effects of unstable surface balance training on postural sway, stability, functional ability and flexibility in women. J. Sports Med. Phys. Fitness 2018, 58, 27–34. [Google Scholar] [PubMed]
- De Moya, M.P.; Bertomeu, J.B.; Broseta, M.V. Evaluación y rehabilitación del equilibrio mediante posturografía. Rehabilitación 2005, 39, 315–323. [Google Scholar] [CrossRef]
- Ithamar, L.; de Moura Filho, A.G.; Rodrigues, M.A.B.; Cortez, K.C.D.; Machado, V.G.; de Paiva Lima, C.R.O.; Moretti, E.; Lemosa, A. Abdominal and pelvic floor electromyographic analysis during abdominal hypopressive gymnastics. J. Bodywork Movement Ther. 2018, 22, 159–165. [Google Scholar] [CrossRef]
- Shamsi, M.; Sarrafzadeh, J.; Jamshidi, A.; Zarabi, V.; Pourahmadi, M.R. The effect of core stability and general exercise on abdominal muscle thickness in non-specific chronic low back pain using ultrasound imaging. Physiother. Theory Pract. 2016, 32, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Pinsach, P.; Rial, T.; Caufriez, M.; Fernandez, J.C.; Devroux, I.; Ruiz, K. Hipopresivos, un cambio de paradigma. Arch. Med. Deporte 2010, 16, 639–645. [Google Scholar]
- Cruz-Díaz, D.; Bergamin, M.; Gobbo, S.; Martínez-Amat, A.; Hita-Contreras, F. Comparative effects of 12 weeks of equipment based and mat Pilates in patients with Chronic Low Back Pain on pain, function and transversus abdominis activation. A randomized controlled trial. Complement. Ther. Med. 2017, 33, 72–77. [Google Scholar] [CrossRef]
- Smith, M.D.; Coppieters, M.W.; Hodges, P.W. Postural response of the pelvic floor and abdominal muscles in women with and without incontinence. Neurourol. Urodyn. 2007, 26, 377–385. [Google Scholar] [CrossRef]
- Gorbet, N.; Selkow, N.M.; Hart, J.M.; Saliba, S. No difference in transverse abdominis activation ratio between healthy and asymptomatic low back pain patients during therapeutic exercise. Rehabil. Res. Pract. 2010, 2010, 459738. [Google Scholar] [CrossRef] [PubMed]
- Koppenhaver, S.L.; Hebert, J.J.; Parent, E.C.; Fritz, J.M. Rehabilitative ultrasound imaging is a valid measure of trunk muscle size and activation during most isometric sub-maximal contractions: A systematic review. Aust. J. Physiother. 2009, 55, 153–169. [Google Scholar] [CrossRef] [Green Version]
- Bø, K.; Mørkved, S.; Frawley, H.; Sherburn, M. Evidence for benefit of transversus abdominis training alone or in combination with pelvic floor muscle training to treat female urinary incontinence: A systematic review. Neurourol. Urodyn. Off. J. Int. Cont. Soc. 2009, 28, 368–373. [Google Scholar] [CrossRef]
- Cruz-Díaz, D.; Romeu, M.; Velasco-González, C.; Martínez-Amat, A.; Hita-Contreras, F. The effectiveness of 12 weeks of Pilates intervention on disability, pain and kinesiophobia in patients with chronic low back pain: A randomized controlled trial. Clin. Rehabil. 2018, 32, 1249–1257. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technical Foundations | Definition |
|---|---|
| Autoelongation | Axial stretching of the spine, tensioning of deep spine and back extensors |
| Double chin | Pulling the crown to the ceiling |
| Decoaptation of the glenohumeral joint | Scapula abduction and serratus activation |
| Neutral pelvis | Equal distance between anterior and posterior superior iliac spines |
| Dorsal ankle flexion | Parallel lower extremities with hip-width, slight knee flexion, and dorsal ankle flexion |
| Gravity shaft overrun | Imbalance of the anteroposterior axis involving variation of the center of gravity |
| Diaphragmatic breathing | Nasal inspiration with rib opening Braked mouth breathing |
| Expiratory apnea | Total exhalation Apnea maintained with a costal opening: closure of the glottis, voluntary contraction of the serratus majors and muscles of the upper airway, intercostals, scalenes, and sternocleidomastoid Diaphragm relaxation and cavity pressure reduction |
| Demographic Characteristics | All Participants (n = 117) | CG (n = 56) | EG (n = 63) | p-Value | |
|---|---|---|---|---|---|
| Age: mean ± SD (years) | 45.65 ± 8.86 | 46.89 ± 6.59 | 44.54 ± 10.40 | 0.149 | |
| Weight: mean ± SD (Kg) | 63.59 ± 10.59 | 64.62 ± 10.04 | 62.67 ± 11.05 | 0.318 | |
| Height: mean ± SD (cm) | 162.56 ± 5.95 | 163.45 ± 5.83 | 161.78 ± 5.99 | 0.128 | |
| BMI: mean ± SD (kg/m2) | 24.03 ± 3,63 | 24.15 ± 3.31 | 23.93 ± 3.92 | 0.742 | |
| Nº pregnant: mean ± SD | 1.54 ± 1.07 | 1.71 ± 1.06 | 1.38 ± 1.07 | 0.090 | |
| Nº delivery: mean ± SD | 1.47 ± 1.05 | 1.63 ± 1.04 | 1.33 ± 1.05 | 0.130 | |
| Delivery type: n (%) | None | 28 (23.5) | 10 (35.7) | 18 (64.3) | 0.533 ** |
| Vaginal | 68 (57.1) | 34 (50) | 34 (50) | ||
| Caesarean | 12 (10.1) | 7 (58.3) | 5 (41.7) | ||
| Both | 10 (8.4) | 5 (45.5) | 6 (54.5) | ||
| Smoking: n (%) | No | 100 (84) | 49 (49) | 51 (51) | 0.33 |
| Yes | 19 (16) | 7 (36.8) | 12 (63.2) | ||
| Exercise: n (%) | No | 56 (47.1) | 27 (48.2) | 29 (51.8) | 0.812 |
| yes | 63 (52.9) | 29 (46) | 34 (54) | ||
| RMSX-OE: mean ± SD (mm) | 0.59 ± 0.11 | 0.58 ± 0.12 | 0.59 ± 0.10 | 0.833 | |
| RMSX-CE: mean ± SD(mm) | 0.64 ± 0.12 | 0.64 ± 0.11 | 0.64 ± 0.13 | 0.962 | |
| RMSY-OE: mean ± SD (mm) | 0.42 ± 0.99 | 0.41 ± 0.10 | 0.43 ± 0.09 | 0.354 | |
| RMSY-CE: mean ± SD (mm) | 0.50 ± 0.15 | 0.49 ± 0.14 | 0.50 ± 0.16 | 0.796 | |
| V-OE: mean ± SD (mm/s) | 15.97 ± 3.57 | 15.95 ± 4.31 | 15.98 ± 2.80 | 0.964 | |
| V-EC: mean ± SD (mm/s) | 16.78 ± 3.20 | 16.56 ± 2.79 | 16.98 ± 3.53 | 0.476 | |
| S-O: mean ± SD (mm2) | 42.56 ± 41.34 | 35.69 ± 31.22 | 48.67 ± 48.03 | 0.087 | |
| S-CE: mean ± SD (mm2) | 85.76 ± 137.31 | 77.32 ± 94.72 | 93.25 ± 166.74 | 0.530 | |
| TrA relaxation: mean ± SD | 0.40 ± 0.08 | 0.40 ± 0.09 | 0.39 ± 0.08 | 0.921 | |
| TrA contraction: mean ± SD | 0.70 ± 0.14 | 0.74 ± 0.14 | 0.67 ± 0.13 | 0.239 |
| Control Group (n = 56) | Experimental Group (n = 63) | Group | Time | Group × Time | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | F (1.117) | p-Value | η2 | F (1.117) | p-Value | η2 | F (1.117) | p-Value | η2 | |
| RMSX-OE (mm) | 0.58 ± 0.12 | 0.59 ± 0.11 | 0.59 ± 0.10 | 0.58 ± 0.10 | 0.086 | 0.770 | 0.001 | 0.025 | 0.875 | 0.001 | 0.411 | 0.52 | 0.003 |
| RMSX-CE (mm) | 0.64 ± 0.11 | 0.67 ± 0.14 | 0.64 ± 0.13 | 0.63 ± 0.10 | 1.088 | 0.299 | 0.009 | 1.153 | 0.285 | 0.010 | 2.714 | 0.102 | 0.023 |
| RMSY-OE (mm) | 0.41 ± 0.10 | 0.40 ± 0.10 | 0.43 ± 0.09 | 0.38 ± 0.09 | 0.032 | 0.859 | 0.001 | 12.585 | 0.001* | 0.097 | 5.095 | 0.026* | 0.042 |
| RMSY-CE (mm) | 0.49 ± 0.14 | 0.45 ± 0.12 | 0.50 ± 0.16 | 0.42 ± 0.10 | 0.292 | 0.590 | 0.002 | 17.049 | 0.001* | 0.127 | 1.315 | 0.254 | 0.011 |
| V-OE (mm/s) | 15.95 ± 4.31 | 17.00 ± 2.66 | 15.98 ± 2.80 | 15.21 ± 2.99 | 3.217 | 0.075 | 0.027 | 0.182 | 0.670 | 0.002 | 7.401 | 0.008** | 0.059 |
| V-CE (mm/s) | 16.56 ± 2.79 | 16.97 ± 2.66 | 16.98 ± 3.53 | 15.75 ± 2.78 | 0.761 | 0.385 | 0.006 | 1.861 | 0.175 | 0.016 | 7.648 | 0.007* | 0.061 |
| S-OE (mm2) | 35.69 ± 31.22 | 23.14 ± 18.59 | 48.67 ± 48.03 | 15.16 ± 2.55 | 0.369 | 0.545 | 0.003 | 37.168 | 0.001* | 0.241 | 7.705 | 0.006** | 0.062 |
| S-CE (mm2) | 77.32 ± 94.72 | 53.71 ± 52.75 | 93.25 ± 166.74 | 50.19 ± 50.62 | 0.158 | 0.691 | 0.001 | 9.151 | 0.003* | 0.073 | 0.779 | 0.379 | 0.007 |
| TrA relaxation | 0.40 ± 0.09 | 0.41 ± 0.09 | 0.39 ± 0.08 | 0.40 ± 0.08 | 0.013 | 0.911 | 0.001 | 0.904 | 0.344 | 0.008 | 0.001 | 0.989 | 0.001 |
| Tra contraction | 0.74 ± 0.14 | 0.74 ± 0.17 | 0.67 ± 0.13 | 0.75 ± 0.17 | 1.835 | 0.178 | 0.015 | 15.44 | 0.001* | 0.117 | 13.057 | 0.001** | 0.100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno-Muñoz, M.d.M.; Hita-Contreras, F.; Estudillo-Martínez, M.D.; Aibar-Almazán, A.; Castellote-Caballero, Y.; Bergamin, M.; Gobbo, S.; Cruz-Díaz, D. The Effects of Abdominal Hypopressive Training on Postural Control and Deep Trunk Muscle Activation: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 2741. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052741
Moreno-Muñoz MdM, Hita-Contreras F, Estudillo-Martínez MD, Aibar-Almazán A, Castellote-Caballero Y, Bergamin M, Gobbo S, Cruz-Díaz D. The Effects of Abdominal Hypopressive Training on Postural Control and Deep Trunk Muscle Activation: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(5):2741. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052741
Chicago/Turabian StyleMoreno-Muñoz, María del Mar, Fidel Hita-Contreras, María Dolores Estudillo-Martínez, Agustín Aibar-Almazán, Yolanda Castellote-Caballero, Marco Bergamin, Stefano Gobbo, and David Cruz-Díaz. 2021. "The Effects of Abdominal Hypopressive Training on Postural Control and Deep Trunk Muscle Activation: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 5: 2741. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052741