
Structure and Distribution of Health Care Costs across Age Groups of Patients with Multimorbidity in Lithuania

 , ,
, , 
Abstract
:1. Background
2. Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Study Sample and Health Care Service Cost
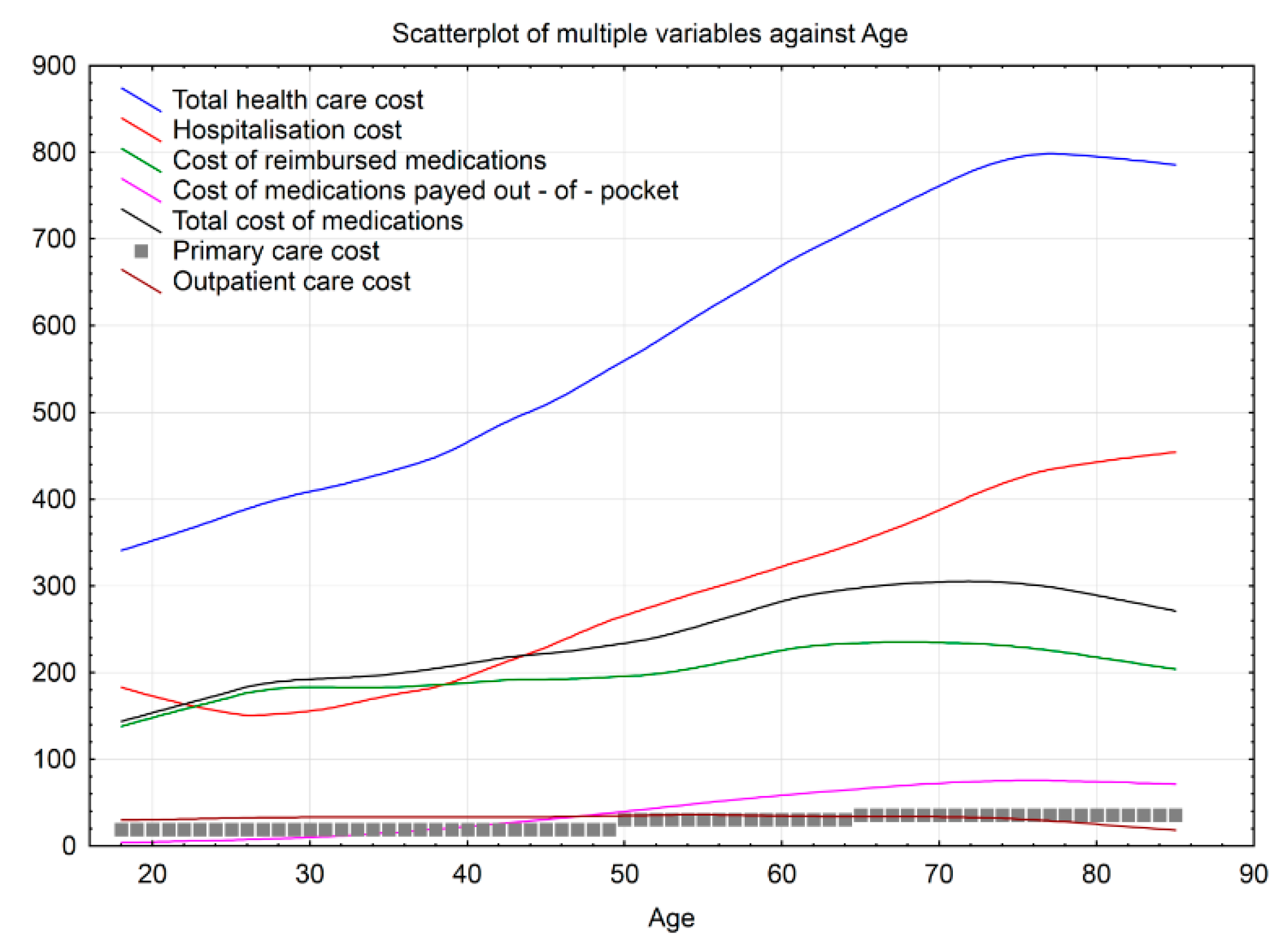
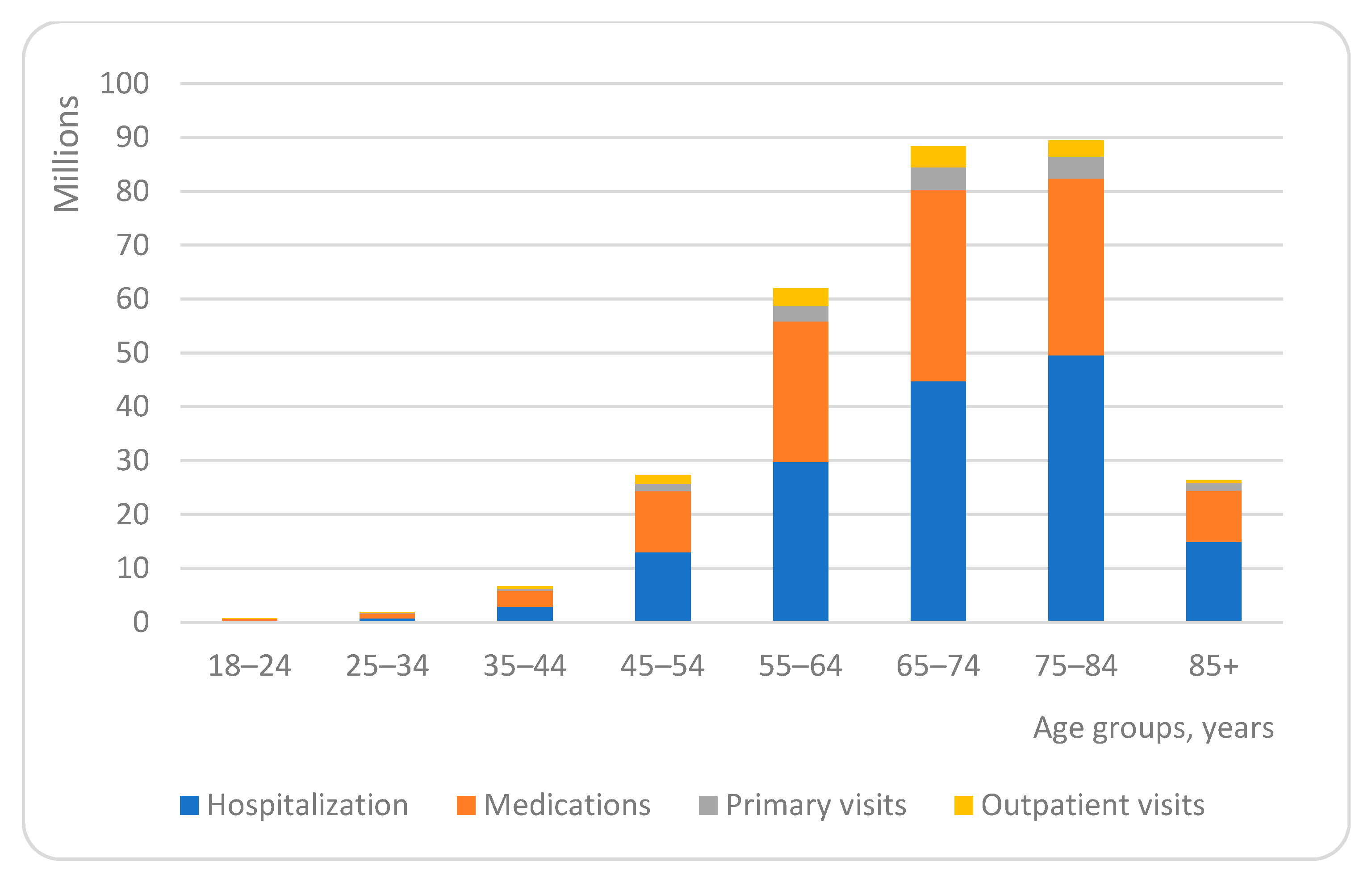
3.2. Health Care Cost and Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Violan, C.; Foguet-Boreu, Q.; Flores-Mateo, G.; Salisbury, C.; Blom, J.W.; Freitag, M.; Glynn, L.G.; Muth, C.; Valderas, J.M. Prevalence, Determinants and Patterns of Multimorbidity in Primary Care: A Systematic Review of Observational Studies. PLoS ONE 2014, 9, e102149. [Google Scholar] [CrossRef]
- van den Bussche, H.; Koller, D.; Kolonko, T.; Hansen, H.; Wegscheider, K.; Glaeske, G.; von Leitner, E.C.; Schäfer, I.; Schön, G. Which chronic diseases and disease combinations are specific to multimorbidity in the elderly? Results of a claims data based cross-sectional study in Germany. BMC Public Health 2011, 11, 101. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.M.; Valderas, J.M.; Yen, L.; Dawda, P.; Jowsey, T.; McRae, I.S. Multimorbidity and Comorbidity of Chronic Diseases among the Senior Australians: Prevalence and Patterns. PLoS ONE 2014, 9, e83783. [Google Scholar] [CrossRef]
- Schoen, C.; Osborn, R.; Doty, M.M.; Squires, D.; Peugh, J.; Applebaum, S. A Survey of Primary Care Physicians in Eleven Countries, 2009: Perspectives on Care, Costs, and Experiences. Health Aff. 2009, 28, w1171–w1183. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, J.; Abernethy, A.P.; Miller, C.; Currow, D.C. Managing comorbidities in patients at the end of life. BMJ 2004, 329, 909–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marengoni, A.; Winblad, B.; Karp, A.; Fratiglioni, L. Prevalence of chronic diseases and multimorbidity among the elderly popu-lation in Sweden. Am. J. Public Health 2008, 98, 1198–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehnert, T.; Heider, D.; Leicht, H.; Heinrich, S.; Corrieri, S.; Luppa, M.; Riedel-Heller, S.; König, H.-H. Review: Health Care Utilization and Costs of Elderly Persons with Multiple Chronic Conditions. Med. Care Res. Rev. 2011, 68, 387–420. [Google Scholar] [CrossRef] [PubMed]
- Polsky, D.; Bonafede, M.; Suaya, J.A. Comorbidities as a driver of the excess costs of community-acquired pneumonia in U.S. commercially-insured working age adults. BMC Health Serv. Res. 2012, 12, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogeli, C.; Shields, A.E.; Lee, T.A.; Gibson, T.B.; Marder, W.D.; Weiss, K.B.; Blumenthal, D. Multiple Chronic Conditions: Prevalence, Health Consequences, and Implications for Quality, Care Management, and Costs. J. Gen. Intern. Med. 2007, 22, 391–395. [Google Scholar] [CrossRef] [Green Version]
- Nagl, A.; Witte, J.; Hodek, J.; Greiner, W. Relationship between multimorbidity and direct healthcare costs in an advanced elderly population. Results of the PRISCUS trial. Z. Gerontol. Geriatr. 2012, 45, 146–154. [Google Scholar] [CrossRef]
- Bähler, C.; Huber, C.A.; Brüngger, B.; Reich, O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: A claims data based observational study. BMC Health Serv. Res. 2015, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kuo, R.N.; Lai, M.-S. The influence of socio-economic status and multimorbidity patterns on healthcare costs: A six-year follow-up under a universal healthcare system. Int. J. Equity Health 2013, 12, 69. [Google Scholar] [CrossRef] [Green Version]
- Yoon, J.; Zulman, D.; Scott, J.Y.; Maciejewski, M.L. Costs Associated with Multimorbidity among VA Patients. Med. Care 2014, 52, S31–S36. [Google Scholar] [CrossRef]
- Zulman, D.M.; Pal Chee, C.; Wagner, T.H.; Yoon, J.; Cohen, D.M.; Holmes, T.H.; Ritchie, C.; Asch, S.M. Multimorbidity and healthcare utilisation among high-cost patients in the US Veterans Affairs Health Care System. BMJ Open 2015, 5, e007771. [Google Scholar] [CrossRef] [Green Version]
- Navickas, R.; Visockienė, Ž.; Puronaitė, R.; Rukšėnienė, M.; Kasiulevičius, V.; Jurevičienė, E. Prevalence and structure of multiple chronic conditions in Lithuanian population and the distribution of the associated healthcare resources. Eur. J. Intern. Med. 2015, 26, 160–168. [Google Scholar] [CrossRef]
- Jureviciene, E.; Onder, G.; Visockiene, Z.; Puronaitė, R.; Petrikonytė, D.; Gargalskaitė, U.; Kasiulevicius, V.; Navickas, R. Does multimorbidity still remain a matter of the elderly: Lithuanian national data analysis. Health Policy 2018, 122, 681–686. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017; Available online: https://www.R-project.org (accessed on 10 May 2018).
- Vito, M.; Muggeo, R. Segmented: An R Package to Fit Regression Models with Broken-Line Relationships. R News 2008, 8, 20–25. [Google Scholar]
- Rijken, M.; Struckmann, V.; Dyakova, M.; Melchiorre, G.M.; Rissanen, S.; van Ginneken, E. ICARE4EU: Improving care for people with multiple chronic conditions in Europe. Eurohealth 2013, 19, 29–31. [Google Scholar]
- Schneider, K.M.; O’Donnell, B.E.; Dean, D. Prevalence of multiple chronic conditions in the United States’ Medicare population. Health Qual. Life Outcomes 2009, 7, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glynn, L.G.; Valderas, J.M.; Healy, P.; Burke, E.; Newell, J.; Gillespie, P.; Murphy, A.W. The prevalence of multimorbidity in primary care and its effect on health care utilization and cost. Fam. Pract. 2011, 28, 516–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picco, L.; Achilla, E.; Abdin, E.; Chong, S.A.; Vaingankar, J.A.; McCrone, P.; Chua, H.C.; Heng, D.; Magadi, H.; Ng, L.L.; et al. Economic burden of multimorbidity among older adults: Impact on healthcare and societal costs. BMC Health Serv. Res. 2016, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Thavorn, K.; Maxwell, C.J.; Gruneir, A.; Bronskill, S.E.; Bai, Y.; Koné Pefoyo, A.J.; Petrosyan, Y.; Wodchis, W.P. Effect of so-cio-demographic factors on the association between multimorbidity and healthcare costs: A population-based, retrospective cohort study. BMJ Open 2017, 7, e017264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahlman, C.; Lynn, J.; Doberman, D.; Gabel, J.; Finch, M. Prescription drug spending for beneficiaries in the last Medicare plus Choice year of life. J. Palliat. Med. 2006, 9, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Moxey, E.D.; O’Connor, J.P.; Novielli, K.D.; Teutsch, S.; Nash, D.B. Prescriptiondrug use in the elderly: A descriptive analysis. Health Care Financ. R 2003, 24, 127–141. [Google Scholar]
- Sambamoorthi, U.; Shea, D.; Crystal, S. Total and out-of-pocket expenditures for prescription drugs among older persons. Gerontologist 2003, 43, 345–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orueta, J.F.; García-Alvarez, A.; Garcia-Goñi, M.; Paolucci, F.; Nuño-Solinis, R. Prevalence and Costs of Multimorbidity by Deprivation Levels in the Basque Country: A Population Based Study Using Health Administrative Databases. PLoS ONE 2014, 9, e89787. [Google Scholar] [CrossRef] [PubMed]
- Statistics Lithuania. Available online: https://www.stat.gov.lt/en (accessed on 10 May 2018).
- Corrieri, S.; Heider, D.; Matschinger, H.; Lehnert, T.; Raum, E.; König, H.-H. Income-, education- and gender-related inequalities in out-of-pocket health-care payments for 65+ patients—A systematic review. Int. J. Equity Health 2010, 9, 20. [Google Scholar] [CrossRef] [Green Version]
- Wittenberg, R. The challenge of measuring multi-morbidity and its costs. Isr. J. Health Policy Res. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Chronic Diseases with ICD-10-AM Diagnostic Codes | |
|---|---|
| 1 | Cancer C00–C96 |
| 2 | Anaemia D50 |
| 3 | Hypothyroidism E02; E03; E89.0 |
| 4 | Diabetes E10.0–E10.9; E11.0–E11.9 |
| 5 | Obesity E66 |
| 6 | Dyslipidaemia E78 |
| 7 | Dementia F00.0–F00.9; G30.0–G30.9; F01.0–F01.9; F02.0–F02.8; F03 |
| 8 | Mental disorders F20.0–F20.9; F30.0–F39; F40.00–F40.9; F41.0–F41.9; F42.0–F42.9; F43.0–F43.9 |
| 9 | Parkinson disease G20 |
| 10 | Multiple sclerosis G35 |
| 11 | Epilepsy G40.00–G40.91 |
| 12 | Sleep apnoea G47.3 |
| 13 | Back Pain G54.1; G54.4; G55.1; M51 |
| 14 | Glaucoma H40–H42 |
| 15 | Blindness H53–H54 |
| 16 | Hearing loss H90.0–H90.8; H91.0–H91.9 |
| 17 | Hypertension I10–I15 |
| 18 | Ischemic heart disease I20–I25 |
| 19 | Arrhythmias I44–I49 |
| 20 | Heart failure I50.0–I50.9 |
| 21 | Intracranial bleeding I61–I62 |
| 22 | Stroke I63-I64; I69 |
| 23 | Chronic obstructive pulmonary disease J44.0–J44.9; J96 |
| 24 | Asthma J45.0–J45.9 |
| 25 | Inflammatory bowel disease K50; K51 |
| 26 | Psoriasis L40.0–L40.9 |
| 27 | Rheumatoid arthritis M05–M06 |
| 28 | Gout M10.0–M10.99 |
| 29 | Osteoarthritis M15–M19 |
| 30 | Systemic lupus erythematosus M32 |
| 31 | Osteoporosis M80–M82 |
| 32 | Renal failure N18–N19 |
| Age, Years | N | Mean of Total Amount | Mean Cost of Medication | Mean Cost of Hospitalization | Mean Cost of Primary Care | Mean Cost of Outpatient Care |
|---|---|---|---|---|---|---|
| 18–24 | 2000 | 378.70 | 154.64 | 173.83 | 19.26 | 30.97 |
| 25–34 | 4861 | 401.72 | 190.17 | 159.29 | 19.26 | 33.00 |
| 35–44 | 14,305 | 455.38 | 206.85 | 195.45 | 19.26 | 33.82 |
| 45–54 | 48,357 | 554.47 | 231.46 | 263.14 | 25.11 | 34.76 |
| 55–64 | 92,777 | 665.05 | 279.58 | 319.79 | 30.96 | 34.71 |
| 65–74 | 116,423 | 757.05 | 304.64 | 382.54 | 36.12 | 33.75 |
| 75–84 | 111,953 | 797.59 | 292.40 | 443.00 | 36.12 | 26.07 |
| 85+ | 37,754 | 697.17 | 252.78 | 395.24 | 36.12 | 13.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nedzinskienė, L.; Jurevičienė, E.; Visockienė, Ž.; Ulytė, A.; Puronaitė, R.; Kasiulevičius, V.; Kazėnaitė, E.; Burneikaitė, G.; Navickas, R. Structure and Distribution of Health Care Costs across Age Groups of Patients with Multimorbidity in Lithuania. Int. J. Environ. Res. Public Health 2021, 18, 2767. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052767
Nedzinskienė L, Jurevičienė E, Visockienė Ž, Ulytė A, Puronaitė R, Kasiulevičius V, Kazėnaitė E, Burneikaitė G, Navickas R. Structure and Distribution of Health Care Costs across Age Groups of Patients with Multimorbidity in Lithuania. International Journal of Environmental Research and Public Health. 2021; 18(5):2767. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052767
Chicago/Turabian StyleNedzinskienė, Laura, Elena Jurevičienė, Žydrūnė Visockienė, Agnė Ulytė, Roma Puronaitė, Vytautas Kasiulevičius, Edita Kazėnaitė, Greta Burneikaitė, and Rokas Navickas. 2021. "Structure and Distribution of Health Care Costs across Age Groups of Patients with Multimorbidity in Lithuania" International Journal of Environmental Research and Public Health 18, no. 5: 2767. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052767