
Exploring Factors That Could Potentially Have Affected the First 1000 Days of Absent Learners in South Africa: A Qualitative Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Approach and Design
2.2. Research Setting and Sampling
2.3. Procedure
2.4. Data Collection
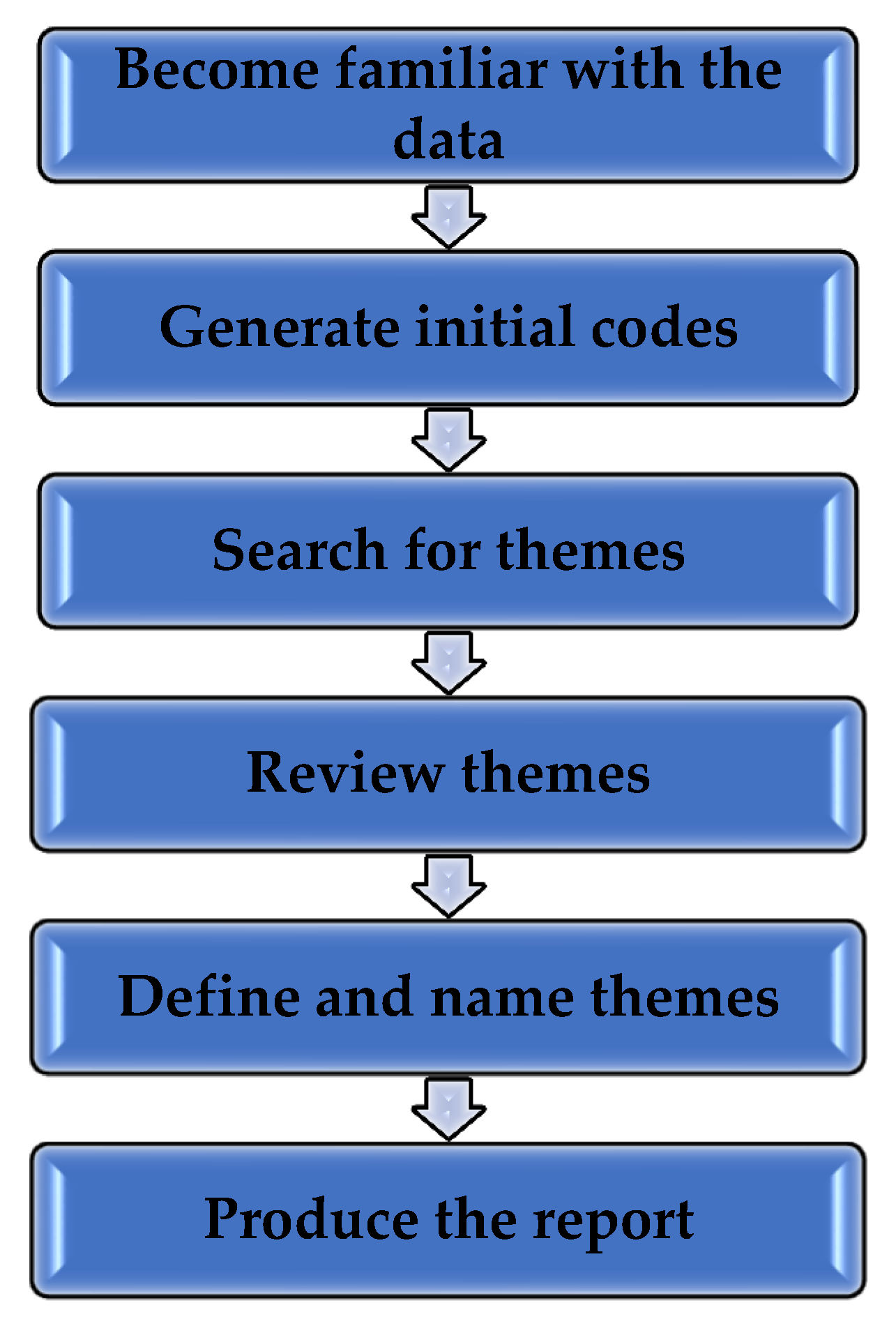
2.5. Data Analysis
3. Results
3.1. Theme 1: Health of the Mothers during the First 1000 Days of Their Children’s Lives
3.1.1. Sub-Theme 1.1: Physical Health of the Mothers
3.1.2. Sub-Theme 1.2: Mental Health and Emotional Well-Being of Mothers
3.1.3. Sub-Theme 1.3: Nutrition of Mothers
3.1.4. Sub-Theme 1.4: Substance Use/Abuse of Mothers during Pregnancy
3.2. Theme 2: The Health of Children during the First 1000 Days of Life
3.2.1. Sub-Theme 2.1: Physical Health of the Children
3.2.2. Sub-Theme 2.2: Nutrition of Children
3.3. Theme 3: Availability of Support to the Mothers and Their Children during the First 1000 Days of the Children’s Lives
3.3.1. Sub-Theme 3.1: The Mothers’ Experience Regarding Support
3.3.2. Sub-Theme 3.2: Support from the Children’s Biological Fathers
3.3.3. Sub-Theme 3.3: Support from Family Members and Others
3.4. Theme 4: Circumstances of the Mothers and Their Children during the First 1000 Days of Their Children’s Lives
3.4.1. Sub-Theme 4.1: Living Circumstances
3.4.2. Sub-Theme 4.2: Financial Circumstances
3.5. Theme 5: Attachment and Relationship between the Mothers and Their Children during the First 1000 Days of Their Children’s Lives
3.5.1. Sub-Theme 5.1: Attachment and Relationship between the Mothers and Their Children during Pregnancy
3.5.2. Sub-Theme 5.2: Attachment and Relationship between the Mothers and Their Children from Birth to Two Years
3.6. Theme 6: Development and Care of the Children during the First 1000 Days of Their Lives
3.6.1. Sub-Theme 6.1: The Children’s Development
3.6.2. Sub-Theme 6.2: The Mothers’ Care and Protection of the Children
3.6.3. Sub-Theme 6.3: Stimulation and Play
4. Discussion
4.1. Discussion of Findings
4.2. Limitations
4.3. Implications for Future Research
4.4. Contributions to Communities and Professionals Working in the Field of Early Child Development
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNICEF: Office of Research-Innocenti. The First 1000 Days of Life: The Brain’s Window of Opportunity. Available online: https://www.unicef-irc.org/article/958-the-first-1000-days-of-life-the-brains-window-of-opportunity.html (accessed on 8 April 2018).
- Pem, D. Factors affecting early childhood growth and development: Golden 1000 days. Adv. Pract. Nurs. 2015, 1. [Google Scholar] [CrossRef]
- Bornstein, M.H.; Arterberry, M.E.; Lamb, M.E. Development in Infancy: A Contemporary Introduction, 5th ed.; Psychology Press: Sussex, UK, 2013. [Google Scholar]
- Donald, K.; Wilmhurst, J.M. Research Newsletter: Advances in Neuroscience—The First 1000 Days. Research Newsletter. Western Cape Government, Western Cape. 2016. Available online: https://www.westerncape.gov.za/assets/departments/health/research_newsletter_30-11-2016.pdf (accessed on 10 June 2018).
- Center on the Developing Child of Harvard University. From Best Practices to Breakthrough Impacts a Science-Based Approach to Building a More Promising Future for Young Children and Families; Harvard University: Cambridge, MA, USA, 2016; Available online: https://developingchild.harvard.edu/wp-content/uploads/2016/05/From_Best_Practices_to_Breakthrough_Impacts-3.pdf (accessed on 3 October 2019).
- Mezmur, B.D. Foreword. In South African Child Gauge; Jamieson, L., Berry, L., Lake, L., Eds.; Available online: http://www.ci.uct.ac.za/sites/default/files/image_tool/images/367/Child_Gauge/South_Afrcan_Child_Gauge_2017/Child_Gauge_2017_lowres.pdf (accessed on 10 June 2018).
- Bhardwaj, S.; Sambu, W.; Jamieson, L. Setting an Ambitious Agenda for Children: The Sustainable Development Goals; The Children’s Institute, University of Cape Town: Cape Town, South Africa, 2017; Available online: http://www.ci.uct.ac.za/sites/default/files/image_tool/images/367/Child_Gauge/South African_Child_ Gauge_2017/Child_Gauge_2017_lowres. pdf (accessed on 10 June 2018).
- Mputle, L.D.P. Nurturing Care during the First 1000 Days of Life: A Systematic Review; Masters of Social Work in Child Protection; North-West University: Potchefstroom, South Africa, 2019. [Google Scholar]
- Moore, T.; Arefadib, N.; Deery, A.; Keyes, M.; West, S. The First Thousand Days: An Evidence Paper; Melbourne: Murdoch Children’s Research Institute: Parkville, Australia, 2017. [Google Scholar]
- Thanjan, S. Report on the First Round of the First 1000 Days Roadshows Conducted in the Cape Town Metro between April–September 2016. 2017. Available online: http://www.knowledgeco-op.uct.ac.za/sites/default/files/image_tool/images/155/356_First%201000%20Days%20roadshow_DOHreport.pdf (accessed on 12 September 2019).
- Western Cape Government. First 1000 Days Campaign. 2017. Available online: https://www.westerncape.gov.za/general-publication/first-1-000-days-campaign. (accessed on 2 March 2018).
- Western Cape Government. First 1000 Days: Grow, Love and Play. 2019. Available online: https://www.westerncape.gov.za/first-1000-days/ (accessed on 2 March 2019).
- Department of Basic Education. Policy on Learner Attendance (General Notice 361 of 2010). 2010. Available online: https://www.education.gov.za/Portals/0/Documents/Policies/Policy%20on%20Learner%20Attendance%202010.pdf?ver=2010-07-20-012020-000 (accessed on 2 March 2018).
- Attendance Works. Reducing Chronic Absence Starting in the Early Grades: An Essential Ingredient for Promoting Success in School. 2011. Available online: https://sites.ed.gov/underservedyouth/files/2017/01/MS3-Absences-Add-Up-Toolkit-for-City-Leaders.pdf (accessed on 6 September 2018).
- Henderson, T.; Hill, C.; Norton, K. The Connection between Missing School and Health: A review of Chronic Absenteeism and Student Health in Oregon. 2014. Available online: https://www.attendanceworks.org/wp-content/uploads/2017/08/Chronic-Absence-and-Health-Review-10.8.14-FINAL-REVISED.pdf (accessed on 16 October 2019).
- Sahin, S.; Arseven, Z.; Kiliç, A. Causes of Student Absenteeism and School Dropouts. Int. J. Instr. 2016, 9, 195–210. [Google Scholar] [CrossRef]
- Community Agency for Social Enquiry (CASE) & Joint Education Trust (JET). Learner Absenteeism in the South African Schooling System. 2007. Available online: http://us-cdn.creamermedia.co.za/assets/articles/attachments/12552_learner_absenteeism_report,_2008.pdf (accessed on 2 March 2018).
- Ogburn, J. Study Finds New Program Reduces Absenteeism. 2017. Available online: https://sanford.duke.edu/articles/study-finds-new-program-reduces-absenteeism-primary-schools (accessed on 3 April 2018).
- South Africa Department of Basic Education. Notice 2433: Age Requirements for Admission to an Ordinary Public School; South Africa Department of Basic Education: Pretoria, South Africa, 1998. [Google Scholar]
- Embury Institute for Higher Education. Available online: https://www.embury.ac.za/foundation-phase-teacher/ (accessed on 26 July 2018).
- Hoadley, U. Building strong foundations: Improving the quality of early education. S. Afr. Child Gauge 2013, 2, 72–77. [Google Scholar]
- UNICEF. School Readiness: A Conceptual Framework. 2012. Available online: https://www.unicef.org/earlychildhood/files/Child2Child_ConceptualFramework_FINAL(1).pdf (accessed on 17 October 2019).
- Pretorius, E.; Jackson, M.; McKay, V.; Murray, S.; Spaull, N. Teaching Reading (and Writing) in the Foundation Phase: A Concept Note; ReSEP Projects; Research on Socio-Economic Policy: Stellenbosch, South Africa, 2016. [Google Scholar]
- Van Zyl, E. The Relationship between School Readiness and School Performance in Grade 1 and Grade 4. S. Afr. J. Child. Educ. 2011, 1, 82–94. [Google Scholar]
- Maalouf-Manasseh, Z.; Oot, L.; Sethuraman, K. Giving Children the Best Start in Life: Integrating Nutrition and Early Childhood Development Programming within the First 1000 Days. Technical Brief; Food and Nutrition Technical Assistance III Project. 2016. Available online: https://pdfs.semanticscholar.org/7f33/01507c5f7f34d9ad89f3a5486983a86ea41a.pdf (accessed on 2 July 2018).
- Finnegan, L. Licit and Illicit Drug Use during Pregnancy: Maternal, Neonatal and Early Childhood Consequences; Canadian Centre on Substance Abuse: Ottawa, ON, Canada, 2013; Available online: https://csuch-cemusc.ccsa.ca/sites/default/files/2019-04/CCSA-Drug-Use-during-Pregnancy-Report-2013-en.pdf (accessed on 26 July 2018).
- Addiction Centre. Pregnant Women and Alcohol: Drinking While Pregnant. 2019. Available online: https://www.addictioncenter.com/addiction/pregnant-women-alcohol/ (accessed on 28 September 2019).
- Berk, L.E. Child Development, 9th ed.; Pearson Education: Boston, MA, USA, 2013. [Google Scholar]
- Adnams, C. Research Newsletter: Alcohol in Pregnancy and the Developing Child: What Can Be Done? Research Newsletter; Western Cape Government: Western Cape, South Africa, 2016. Available online: https://www.westerncape.gov.za/assets/departments/health/research_newsletter_30-11-2016.pdf (accessed on 10 June 2018).
- Kellerman, T. Secondary Disabilities in FASD. Available online: http://www.come-over.to/FAS/fasconf.htm (accessed on 10 April 2018).
- Center on the Developing Child of Harvard University. Brain Architecture. Available online: https://developingchild.harvard.edu/science/key-concepts/brain-architecture/ (accessed on 25 February 2018).
- Thompson, R.A. Stress and child development. Future Child. 2014, 24, 41–59. [Google Scholar] [CrossRef]
- Berg, A. Research Newsletter: Parent-Infant Attachment; Research Newsletter; Western Cape Government: Western Cape, South Africa, 2016. Available online: https://www.westerncape.gov.za/assets/departments/health/research_newsletter_30-11-2016.pdf (accessed on 10 June 2018).
- Newman, L.; Sivaratnam, C.; Komiti, A. Attachment and early brain development–neuroprotective interventions in infant–caregiver therapy. Transl. Dev. Psychiatry 2015, 3, 28647. [Google Scholar] [CrossRef]
- Jamieson, L.; Richter, L.; Cavoukian, R. Striving for the sustainable development goals: What do children need to thrive? Child Gauge 2017, 2, 201733. [Google Scholar]
- Ebrahim, H.; Seleti, J.; Dawes, A. Learning begins at birth: Improving access to early learning. Early Child. Res. Q. 2013, 21, 153–157. [Google Scholar]
- Hesse-Biber, S.N. The Practice of Qualitative Research, 3rd ed.; Sage Publications Ltd.: Thousand Oaks, CA, USA, 2017; p. 38. [Google Scholar]
- Brynard, D.J.; Hanekom, S.X.; Brynard, P.A. Introduction to Research, 3rd ed.; Van Schaik Publishers: Pretoria, South Africa, 2014. [Google Scholar]
- Ivankova, N.V.; Creswell, J.W.; Clark, V.L.P. Foundations and approaches to mixed methods research. In First Steps in Research, 2nd ed.; Maree, K., Ed.; Van Schaik: Pretoria, South Africa, 2016; pp. 305–336. [Google Scholar]
- Lambert, V.A.; Lambert, C.E. Qualitative descriptive research: An acceptable design. Pac. Rim Int. J. Nurs. Res. 2012, 16, 255–256. [Google Scholar]
- Marshall, C.; Rossman, G.B. Designing Qualitative Research, 6th ed.; Sage Publications Ltd.: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice, 4th ed.; Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Khula Development Group. Available online: http://www.khuladg.co.za/index.php/programs (accessed on 21 July 2018).
- South Africa Western Cape Government Community Safety. Policing Needs and Priorities (PNP) 2017/2018 Report for the Paarl-East Police Precinct. 2017. Available online: https://www.westerncape.gov.za/assets/paarl_east_pnp_report_final.pdf (accessed on 24 September 2019).
- Violence Prevention through Urban Upgrading (VPUU). Safe Node Area: Paarl-East. 2016. Available online: http://vpuu.org.za/safe-node-area/paarl-east/ (accessed on 6 February 2021).
- Wagner, C.; Kawulich, B.; Garner, M. Doing Social Research: A Global Context; McGraw-Hill Education Ltd.: Berkshire, UK, 2012. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Clarke, V.; Braun, V. Teaching thematic analysis: Overcoming challenges and developing strategies for effective learning. Psychologist 2013, 26, 120–123. [Google Scholar]
- Babbie, E.R.; Mouton, J. The Practice of Social Research; Oxford University Press Southern Africa: Cape Town, South Africa, 2001. [Google Scholar]
- Biswas, C.; Amato, P.; Dorling Kindersley, I. The Pregnancy Encyclopaedia: All Your Questions Answered; DK Publishing: New York, NY, USA, 2016. [Google Scholar]
- The Royal Australian and New Zealand College of Obstetricians and Gynaecologist. Pre-Eclampsia and High Blood Pressure during Pregnancy. 2017. Available online: https://ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27s%20Health/Patient%20information/Pre-eclampsia-and-High-Blood-Pressure-During-Pregnancy.pdf?ext=.pdf (accessed on 24 August 2019).
- World Health Organization. WHO Recommendation on Tuberculosis Testing in Pregnancy. 2016. Available online: https://extranet.who.int/rhl/topics/preconception-pregnancy-childbirth-and-postpartum-care/antenatal-care/who-recommendation-tuberculosis-testing-pregnancy (accessed on 1 September 2019).
- Statistics South Africa. Demographic and Health Survey. 2017. Available online: https://www.statssa.gov.za/publications/Report%2003-00-09/Report%2003-00-092016.pdf (accessed on 22 September 2019).
- Ankin Law. Even Mild Oxygen Deprivation at Birth Can Have Lasting Effects. Available online: https://ankinlaw.com/oxygen-deprivation-at-birth/#:~:text=According%20to%20research%20studies%2C%20even,learning%20disabilities%2C%20and%20behavioral%20problems (accessed on 29 August 2019).
- Birth Injury Guide. Oxygen Deprivation. Available online: https://www.birthinjuryguide.org/infant-brain-damage/causes/lack-of-oxygen-at-birth-causes-long-term-effects-for-babies/ (accessed on 29 August 2019).
- Murkoff, H. What to Expect When You’re Expecting; Workman Publishing: New York, NY, USA, 2016. [Google Scholar]
- Perinatal Mental Health Project. About Us. Available online: https://pmhp.za.org/about-us/ (accessed on 30 August 2019).
- American Pregnancy Association. Depression during Pregnancy. Available online: https://americanpregnancy.org/pregnancy-health/depression-during-pregnancy/ (accessed on 30 September 2019).
- Marroun, H.; Zou, R.; Muetzel, R.L.; Jaddoe, V.W.; Verhulst, F.C.; White, T.; Tiemeier, H. Prenatal exposure to maternal and paternal depressive symptoms and white matter microstructure in children. Depress. Anxiety 2018, 35, 321–329. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynaecologists. Postpartum Depression. 2013. Available online: https://www.acog.org/en/Patients/FAQs/Postpartum-Depression (accessed on 24 September 2019).
- American Psychiatric Association. What Is Postpartum Depression? Available online: https://www.psychiatry.org/patients-families/postpartum-depression/what-is-postpartum-depression (accessed on 24 September 2019).
- Mayo Clinic. Postpartum Depression. 2018. Available online: https://www.mayoclinic.org/diseases-conditions/postpartum-depression/symptoms-causes/syc-20376617 (accessed on 27 September 2019).
- Prado, E.L.; Dewey, K.G. Nutrition and brain development in early life. Nutr. Rev. 2014, 72, 267–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNICEF. Nutrition’s Lifelong Impact. Available online: https://www.unicef.org/nutrition/index_lifelong-impact.html (accessed on 1 September 2019).
- World Health Organization. Management of Substance Abuse. Available online: https://www.who.int/substance_abuse/activities/pregnancy_substance_use/en/ (accessed on 7 September 2019).
- Irner, T.B. Substance exposure in utero and developmental consequences in adolescence: A systematic review. Child Neuropsychol. 2012, 18, 521–549. [Google Scholar] [CrossRef] [PubMed]
- Olivier, L.; Viljoen, D.; Curfs, L. Fetal alcohol spectrum disorders: Prevalence rates in South Africa: The new millennium. S. Afr. Med. J. 2016, 106, 103–106. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. First 1000 Days the Critical Window to Ensure that Children Survive and Thrive. 2017. Available online: https://www.unicef.org/southafrica/sites/unicef.org.southafrica/files/2019-03/ZAF-First-1000-days-brief-2017.pdf (accessed on 8 April 2018).
- McEvoy, C.T.; Spindel, E.R. Pulmonary effects of maternal smoking on the fetus and child: Effects on lung development, respiratory morbidities, and lifelong lung health. Paediatr. Respir. Rev. 2017, 21, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- South Africa Department of Health. Improving Antenatal Care. Available online: https://www.google.com/search?client=firefox-b-d&q=www.health.gov.za%252Findex.php%252Fshortcodes%252F2015-03-29-10-42-47%252F2015-04-30-08-18-10%252F2015-04-30-08-24-27%253Fdownload%253D2002%253Aleaflet-improving-antenatal-care-in-south-africa%26usg%3DAOvVaw3yiYekpR8afbHRZKmHi+Linda%2C+1bm1y (accessed on 19 September 2019).
- World Health Organization. Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Department of Health. Nutrition Guidelines for Early Childhood Development Centres. Available online: https://ilifalabantwana.co.za/wp-content/uploads/2016/12/Nutrition-guidelines-for-ECD-centres_Draft-2_30-September-2016.pdf (accessed on 29 September 2019).
- Australian Government. Infant Feeding Guidelines. 2013. Available online: https://www.eatforhealth.gov.au/sites/default/files/files/the_guidelines/n56b_infant_feeding_summary_130808.pdf (accessed on 14 September 2019).
- UNICEF; WHO; World Bank. Levels and Trends in Child Malnutrition, 2018. Joint Child Malnutrition Estimates: Key Findings of the 2018 Edition. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=5&ved=2ahUKEwiVyb_7yvXkAhWnThUIHbRGDgwQFjAEegQIBRAC&url=https%3A%2F%2Fdata.unicef.org%2Fwp-content%2Fuploads%2F2018%2F05%2FJME-2018-brochure-.pdf&usg=AOvVaw3QEb_l6x53enmewSTXg8eu (accessed on 19 September 2019).
- Nurullah, A.S. Received and provided social support: A review of current evidence and future directions. Am. Health Stud. 2012, 27, 173–188. [Google Scholar]
- C. S. Mott Children’s Hospital. Partner Support During Pregnancy. Available online: https://www.mottchildren.org/health-library/abp7352 (accessed on 15 September 2019).
- Allen, S.M.; Daly, K.J. The Effects of Father Involvement: An Updated Research Summary of the Evidence; University of Guelph’s Centre for Families, Work & Well-Being: Guelph, ON, Canada, 2007; Available online: http://www.ecdip.org/docs/pdf/IF%20Father%20Res%20Summary%20(KD).pdf (accessed on 16 September 2019).
- Scorgie, F.; Blaauw, D.; Dooms, T.; Coovadia, A.; Black, V.; Chersich, M. “I get hungry all the time”: Experiences of poverty and pregnancy in an urban healthcare setting in South Africa. Glob. Health 2015, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- Higgens, S. The Psychology of Dealing with an Unplanned Pregnancy, 2018. PsychCentral. Available online: https://psychcentral.com/blog/the-psychology-of-dealing-with-an-unplanned-pregnancy/ (accessed on 22 September 2019).
- Faisal-Cury, A.; Menezes, P.R.; Quayle, J.; Matijasevich, A. Unplanned pregnancy and risk of maternal depression: Secondary data analysis from a prospective pregnancy cohort. Psychol. Health Med. 2017, 22, 65–74. [Google Scholar] [CrossRef] [PubMed]
- National Health Service. Attachment and Bonding during Pregnancy. 2019. Available online: https://www.nhsinform.scot/ready-steady-baby/pregnancy/relationships-and-wellbeing-in-pregnancy/attachment-and-bonding-during-pregnancy (accessed on 23 September 2019).
- Wheatley, S. Why Bonding During Pregnancy Matters. 2018. PsychReg. Available online: https://www.nhsinform.scot/ready-steady-baby/pregnancy/relationships-and-well-being-in-pregnancy/attachment-and-bonding-during-pregnancy (accessed on 8 September 2019).
- Van der Walt, M.M.; Coetzee, H.; Lubbe, W.; Moss, S.J. Effect of prenatal stimulation programmes for enhancing postnatal bonding in primigravida mothers from the Western Cape. Afr. J. Nurs. Midwifery 2016, 18, 27–46. [Google Scholar] [CrossRef]
- Stoppard, M. Bonding with Your Bump: The First Book on How to Begin Parenting in Pregnancy; Dorling Kindersley Ltd.: London, UK, 2008. [Google Scholar]
- Center on the Developing Child of Harvard University. Serve and Return. Available online: https://developingchild.harvard.edu/science/key-concepts/serve-and-return/ (accessed on 1 October 2019).
- Louw, D.A.; Louw, A.E. Child and Adolescent Development, 2nd ed.; Psychology Publications: Bloemfontein, South Africa, 2014. [Google Scholar]
- Zastrow, C.; Kirst-Ashman, K. Understanding Human Behavior and the Social Environment, 9th ed.; Cengage Learning: Boston, MA, USA, 2013. [Google Scholar]
- Rosa, E.M.; Tudge, J. Urie Bronfenbrenner’s theory of human development: Its evolution from ecology to bioecology. J. Fam. Theory Rev. 2013, 5, 243–258. [Google Scholar] [CrossRef]
- Beckley, P. The New Early Years Foundation Stage: Changes, Challenges and Reflections, 1st ed.; McGraw-Hill Education: London, UK, 2013. [Google Scholar]



{kind=link}
{kind=link}
| Participant | Current Age during the Study | Current Relational Status during the Study | Total Number of Children | Position of Absent Learner in Relation to Other Siblings |
|---|---|---|---|---|
| Participant 1 | 31 years | Single | 3 | Eldest |
| Participant 2 | 28 years | Married | 3 | Eldest |
| Participant 3 | 40 years | Married | 6 | Fourth child |
| Participant 4 | 31 years | Single | 2 | Youngest |
| Participant 5 | 26 years | Single | 3 | Eldest |
| Participant 6 | 37 years | Long-term relationship | 7 | Fifth child |
| Participant 7 | 42 years | Married | 5 | Youngest |
| Participant 8 | 39 years | Married | 7 | Fourth child |
| Participant 9 | 31 years | Married | 3 | Eldest |
| Participant 10 | 44 years | Long-term relationship | 5 | Youngest |
| Participant 11 | 37 years | Divorced | 4 | Third child |
| Participant 12 | 29 years | Single | 2 | Youngest |
| Participant 13 | 48 years | Single | 4 | Youngest |
| Participant 14 | 33 years | Married | 2 | Youngest |
| Participant 15 | 28 years | Long-term relationship | 2 | Eldest |
| Participant 16 | 29 years | Long-term relationship | 2 | Eldest |
| Participant 17 | 32 years | Long-term relationship | 2 | Youngest |
| Participant 18 | 34 years | Long-term relationship | 3 | Middle child |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Zyl, C.; van Wyk, C. Exploring Factors That Could Potentially Have Affected the First 1000 Days of Absent Learners in South Africa: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 2768. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052768
van Zyl C, van Wyk C. Exploring Factors That Could Potentially Have Affected the First 1000 Days of Absent Learners in South Africa: A Qualitative Study. International Journal of Environmental Research and Public Health. 2021; 18(5):2768. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052768
Chicago/Turabian Stylevan Zyl, Carien, and Carlien van Wyk. 2021. "Exploring Factors That Could Potentially Have Affected the First 1000 Days of Absent Learners in South Africa: A Qualitative Study" International Journal of Environmental Research and Public Health 18, no. 5: 2768. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052768