
Development of a Patient-Oriented Intervention to Support Patient-Provider Conversations about Unnecessary Lower Back Pain Imaging

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patient-Oriented Framework
2.2. Data Collection and Analysis
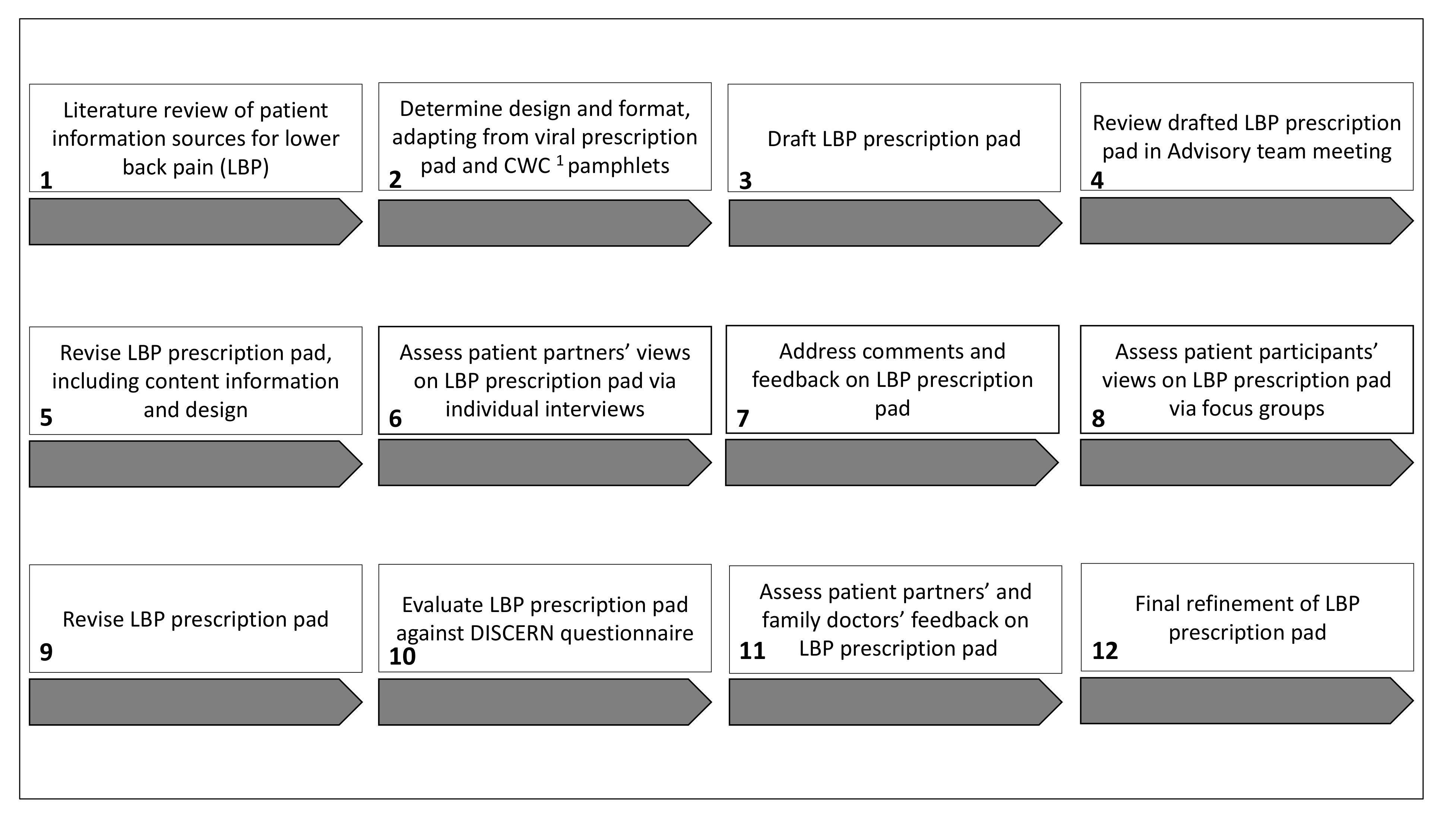
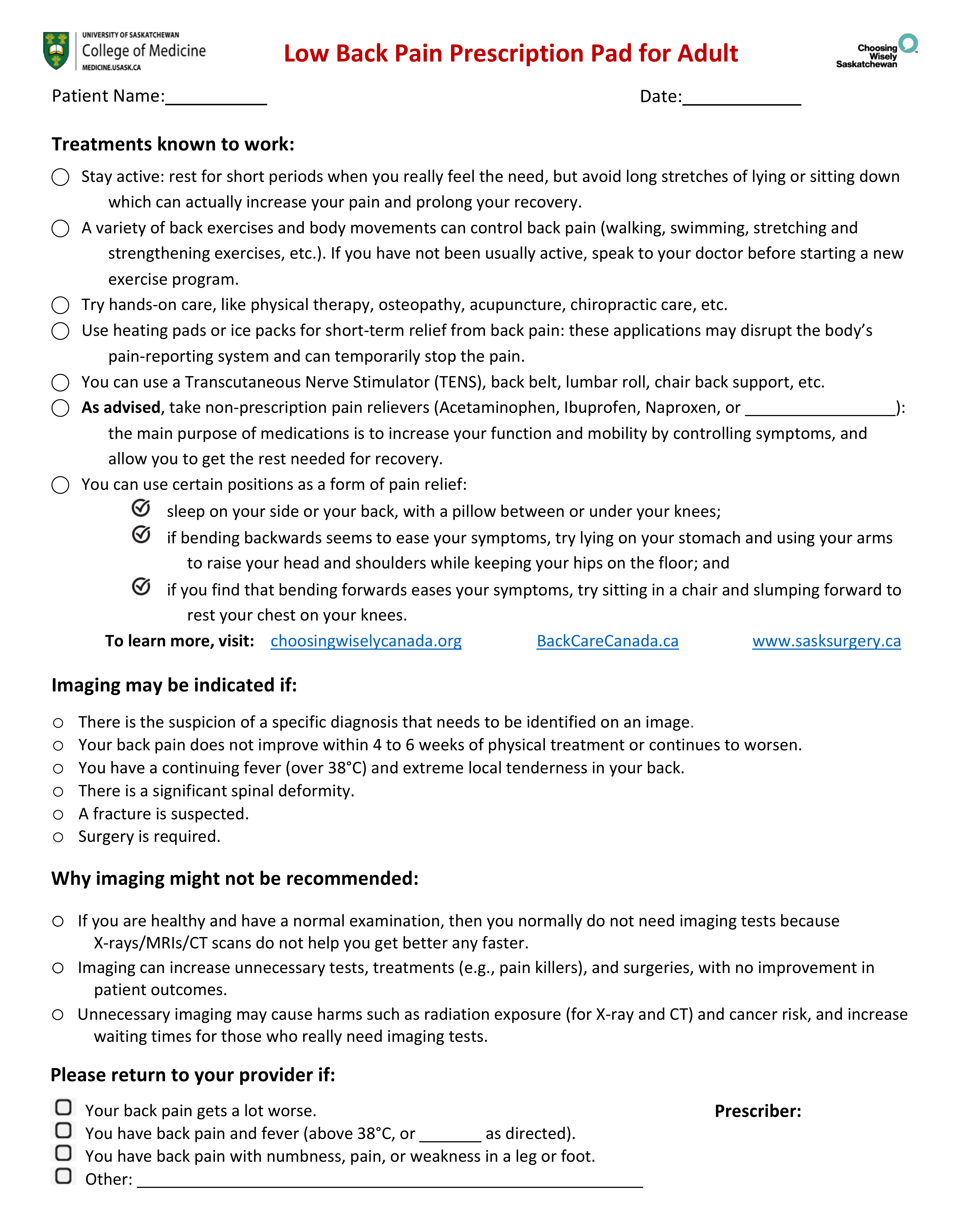
2.3. Intervention
3. Results
3.1. Patient-Identified Content and Format for LBP Prescription Pad
“My doctor didn’t necessarily give me that information, so that’s super handy to have that on the prescription pad so that it’s a talking-point for the doctor to check about that stuff. So, that was super helpful.”(Participant 7)
3.2. Three Key Themes
3.2.1. The Role of Imaging in the LBP Diagnosis
“Imaging was important to see if there were any breaks or anything. I was quite athletic and in a lot of sports, so they wanted just to make sure I hadn’t injured myself.”(Participant 2)
“I went for an X-ray, where this time, I asked my doctor to give it to me because […] I wanted to see what was going on because it seemed to have gotten worse with the nerve pain down my leg.”(Participant 4)
“I thought it was just obviously necessary because I had been in a car accident and then I was having back pain. But I think the second time that I had [imaging] done, it just kept coming back and getting worse, and depending on what I was doing, I felt I should have another [imaging test] just to make sure there wasn’t something wrong. But I haven’t had another [imaging test] since then.”(Participant 7)
3.2.2. The Impact of the Patient-Physician Relationship on the LBP Diagnosis and Treatment
“We don’t let financial advisors mess with our finances, our mechanics mess with our cars, our veterinarians mess with our pets, unless we know exactly what’s going on. We have to be that vigilant with our own healthcare.”(Patient partner 1)
“Even though [patients] all have lower back pain and have been through similar journeys as far as testing, treatments, etc., the experience for those who have trusting open relationships with their physicians is much more positive.”(Patient partner 1)
“[I]t is about having conversations between physicians and patients and respecting the lived-experience voice that we bring of living with our condition and all we bring, it has to be respected. And this happens when you have great relationships […] and I know my family doctor does the same thing.”(Patient partner 2)
3.2.3. Lack of Patient Awareness of CWC
“That’s the challenge, Choosing Wisely, is to move the initiative and get it rolling so that more people know about it. That’s our challenge. There are more and more physicians practicing wisely, so it’s coming, but it’s slow. So, [patients] can be a great help. All of [us].”(Participant 6)
“If I went to the walk-in clinic, which a lot of people don’t have family doctors unfortunately, and a walk-in doctor said: we’re not going to do anything and handed this to me, I think I would feel kind of like he was writing me off.”(Participant 6)
4. Discussion
4.1. Future Research
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canadian Institute for Health Information. Emergency Department Visits in 2014–2015: Information Sheet. Available online: https://secure.cihi.ca/free_products/NACRS_ED_QuickStats_Infosheet_2014-15_ENweb.pdf (accessed on 26 November 2020).
- Edwards, J.; Hayden, J.; Asbridge, M.; Magee, K. The prevalence of low back pain in the emergency department: A descriptive study set in the Charles, V. Keating Emergency and Trauma Centre, Halifax, Nova Scotia, Canada. BMC Musculoskelet. Disord. 2018, 19, 306. [Google Scholar] [CrossRef]
- Busse, J.; Alexander, P.E.; Abdul-Razzak, A.; Riva, J.J.; John Dufton, D.; Zhang, M.; Faulhaber, M.; Couban, C.R.; Guyatt, M.G.; Rampersaud, Y.R.; et al. Appropriateness of Spinal Imaging Use in Canada. 2013. Available online: http://nationalpaincentre.mcmaster.ca/documents/AppropriatenessofSpinalImagingFinalReportApril252013.pdf (accessed on 5 November 2020).
- De González, A.B. Projected Cancer Risks from Computed Tomographic Scans Performed in the United States in 2007. Arch. Intern. Med. 2009, 169, 2071–2077. [Google Scholar] [CrossRef]
- Lurie, J.D.; Birkmeyer, N.J.; Weinstein, J.N. Rates of Advanced Spinal Imaging and Spine Surgery. Spine 2003, 28, 616–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendrick, D.; Fielding, K.; Bentley, E.; Kerslake, R.; Miller, P.; Pringle, M. Radiography of the lumbar spine in primary care patients with low back pain: Randomised controlled trial. BMJ 2001, 322, 400–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flynn, T.W.; Smith, B.; Chou, R. Appropriate Use of Diagnostic Imaging in Low Back Pain: A Reminder That Unnecessary Imaging May Do as Much Harm as Good. J. Orthop. Sports Phys. Ther. 2011, 41, 838–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deyo, R.A. Imaging Idolatry. Arch. Intern. Med. 2009, 169, 921–923. [Google Scholar] [CrossRef] [PubMed]
- About Choosing Wisely Canada. Available online: http://choosingwiselycanada.org/about/ (accessed on 8 October 2020).
- Hall, A.M.; Aubrey-Bassler, K.; Thorne, B.; Maher, C.G. Do not routinely offer imaging for uncomplicated low back pain. BMJ 2021, 372, 291. [Google Scholar] [CrossRef]
- Wáng, Y.X.J.; Wu, A.-M.; Santiago, F.R.; Nogueira-Barbosa, M.H. Informed appropriate imaging for low back pain management: A narrative review. J. Orthop. Transl. 2018, 15, 21–34. [Google Scholar] [CrossRef]
- Canadian Institutes for Health Information. Unnecessary Care in Canada. Available online: https://www.cihi.ca/sites/default/files/document/choosing-wisely-baseline-report-en-web.pdf (accessed on 30 April 2017).
- Chou, R.; Deyo, R.A.; Jarvik, J.G. Appropriate Use of Lumbar Imaging for Evaluation of Low Back Pain. Radiol. Clin. N. Am. 2012, 50, 569–585. [Google Scholar] [CrossRef]
- Levinson, W.; Kallewaard, M.; Bhatia, R.S.; Wolfson, D.; Shortt, S.; Kerr, E.A. ‘Choosing Wisely’: A growing international campaign. BMJ Qual. Saf. 2015, 24, 167–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleifer, D.; Rothman, D.J. “The Ultimate Decision Is Yours”: Exploring Patients’ Attitudes about the Overuse of Medical Interventions. PLoS ONE 2012, 7, e52552. [Google Scholar] [CrossRef]
- Espeland, A.; Baerheim, A.; Albrektsen, G.; Korsbrekke, K.; Larsen, J.L. Patients’ Views on Importance and Usefulness of Plain Radiography for Low Back Pain. Spine 2001, 26, 1356–1363. [Google Scholar] [CrossRef]
- Werner, E.L.; Ihlebaek, C.; Laerum, E.; Wormgoor, M.E.; Indahl, A. Low back pain media campaign: No effect on sickness behaviour. Patient Educ. Couns. 2008, 71, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Moffett, J.A.K.; Newbronner, E.; Waddell, G.; Croucher, K.; Spear, S. Public perceptions about low back pain and its man-agement: A gap between expectations and reality? Health Expect. 2000, 3, 161–168. [Google Scholar] [CrossRef]
- Deyo, R.A.; Diehl, A.K.; Rosenthal, M. Reducing Roentgenography Use. Arch. Intern. Med. 1987, 147, 141–145. [Google Scholar] [CrossRef]
- Stacey, D.; Légaré, F.; Lewis, K.; Barry, M.J.; Bennett, C.L.; Eden, K.B.; Holmes-Rovner, M.; Llewellyn-Thomas, H.; Lyddiatt, A.; Thomson, R.; et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 2017, 4, cd001431. [Google Scholar] [CrossRef] [Green Version]
- Tapp, H.; McWilliams, A.; Dulin, M. Patient engagement and informed decision making regarding medical imaging. North Carol. Med. J. 2014, 75, 114–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slade, S.C.; Kent, P.; Bucknall, T.; Molloy, E.; Patel, S.; Buchbinder, R. Barriers to primary care clinician adherence to clinical guidelines for the management of low back pain: Protocol of a systematic review and meta-synthesis of qualitative studies. BMJ Open 2015, 5, e007265. [Google Scholar] [CrossRef] [PubMed]
- Davies, P.; Walker, E.A.; Grimshaw, J.M. A systematic review of the use of theory in the design of guideline dissemination and implementation strategies and interpretation of the results of rigorous evaluations. Implement. Sci. 2010, 5, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimshaw, J.; Thomas, R.; MacLennan, G.; Fraser, C.; Ramsay, C.R.; Vale, L.; Whitty, P.; Eccles, M.P.; Matowe, L.; Shirran, L.; et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol. Assess. 2004, 8, 1–72. [Google Scholar] [CrossRef] [PubMed]
- Madani Larijani, M.; Azizian, A.; Carr, T.; Badea, A.; Groot, G.; UK Insight Medical Publishing Group. Reducing Inappropriate Imaging Orders for Lower Back Pain Using MRI and CT Checklists: A Quality Improvement Study in Saskatchewan, Canada. Qual. Prim. Care 2020, 28, 24–31. [Google Scholar]
- Buist, D.S.M. Primary Care Clinicians’ Perspectives on Reducing Low-Value Care in an Integrated Delivery System. Perm. J. 2015, 20, 41–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zikmund-Fisher, B.J.; Kullgren, J.T.; Fagerlin, A.; Klamerus, M.L.; Bernstein, S.J.; Kerr, E.A. Perceived Barriers to Implementing Individual Choosing Wisely® Recommendations in Two National Surveys of Primary Care Providers. J. Gen. Intern. Med. 2017, 32, 210–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brownlee, S.; Berman, A. Defining Value in Health Care Resource Utilization: Articulating the Role of the Patient. 2016. Available online: https://academyhealth.org/sites/default/files/Brownlee-Berman%20Paper%20FINAL.pdf (accessed on 8 March 2021).
- Macfarlane, J.; Holmes, W.; Gard, P.; Thornhill, D.; Macfarlane, R.; Hubbard, R.C.; Van Weel, J.M.C. Reducing antibiotic use for acute bronchitis in primary care: Blinded, randomised controlled trial of patient information leaflet. Commentary: More self reliance in patients and fewer antibiotics: Still room for improvement. BMJ 2002, 324, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tannenbaum, C.; Martin, P.; Tamblyn, R.; Benedetti, A.; Ahmed, S. Reduction of Inappropriate Benzodiazepine Prescriptions Among Older Adults Through Direct Patient Education. JAMA Intern. Med. 2014, 174, 890–898. [Google Scholar] [CrossRef] [Green Version]
- Wheeler, J.G.; Fair, M.; Simpson, P.M.; Rowlands, L.A.; Aitken, M.E.; Jacobs, R.F. Impact of a waiting room videotape message on parent attitudes toward pediatric antibiotic use. Pediatrics 2001, 108, 591–596. [Google Scholar] [CrossRef]
- Gonzales, R.; Corbett, K.K.; Leeman-Castillo, B.A.; Glazner, J.; Erbacher, K.; Darr, C.A.; Wong, S.; Maselli, J.H.; Sauaia, A.; Kafadar, K. The “Minimizing Antibiotic Resistance in Colorado” Project: Impact of Patient Education in Improving Antibiotic Use in Private Office Practices. Heal. Serv. Res. 2005, 40, 101–116. [Google Scholar] [CrossRef] [Green Version]
- Ashe, D.; Patrick, P.A.; Stempel, M.M.; Shi, Q.; Brand, N.A. Educational Posters to Reduce Antibiotic Use. J. Pediatr. Heal. Care 2006, 20, 192–197. [Google Scholar] [CrossRef]
- Morgan, J.D.; Wright, D.J.; Chrystyn, H. Pharmacoeconomic evaluation of a patient education letter aimed at reducing long-term prescribing of benzodiazepines. Pharm. World Sci. 2002, 24, 231–235. [Google Scholar] [CrossRef]
- Born, K.B.; Coulter, A.; Han, A.; Ellen, M.; Peul, W.; Myres, P.; Lindner, R.; Wolfson, D.; Bhatia, R.S.; Levinson, W. Engaging patients and the public in Choosing Wisely. BMJ Qual. Saf. 2017, 26, 687–691. [Google Scholar] [CrossRef]
- Bernard, H.R. Research Methods in Anthropology: Qualitative and Quantitative Approaches; Rowman & Littlefield: Lanham, MD, USA, 2017. [Google Scholar]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis. Int. J. Qual. Methods 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research; Sage Publications: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Denzin, N.K.; Lincoln, Y.S. The SAGE Handbook of Qualitative Research; Sage: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Lee, C.; Jafari, M.; Brownbridge, R.; Phillips, C.; Vanstone, J.R. The viral prescription pad—A mixed methods study to determine the need for and utility of an educational tool for antimicrobial stewardship in primary health care. BMC Fam. Pr. 2020, 21, 42. [Google Scholar] [CrossRef] [PubMed]
- Choosing Wisely Canada. Imaging Tests for Lower Back Pain: When You Need Them and When You Don’t. Available online: https://choosingwiselycanada.org/imaging-tests-low-back-pain/ (accessed on 20 November 2020).
- Charnock, D.; Shepperd, S.; Needham, G.; Gann, R. DISCERN: An instrument for judging the quality of written consumer health information on treatment choices. J. Epidemiol. Community Heal. 1999, 53, 105–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassel, C.K. Choosing Wisely. JAMA 2012, 307, 1801–1802. [Google Scholar] [CrossRef]
- Chou, R.; Deyo, R.; Friedly, J.; Skelly, A.; Weimer, M.; Fu, R.; Dana, T.; Kraegel, P.; Griffin, J.; Grusing, S. Systemic Pharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann. Intern. Med. 2017, 166, 480–492. [Google Scholar] [CrossRef] [PubMed]
- Bansback, N.; Chiu, J.; Kerr, S.; McCracken, R.; Forster, B. Reducing imaging tests for low back pain: Can patients choose wisely? [abstract]. Arthritis Rheumatol. 2016, 68 (Suppl. 10), 1146. [Google Scholar]
- Jenkins, H.J.; Moloney, N.A.; French, S.D.; Maher, C.G.; Dear, B.F.; Magnussen, J.S.; Hancock, M.J. Using behaviour change theory and preliminary testing to develop an implementation intervention to reduce imaging for low back pain. BMC Heal. Serv. Res. 2018, 18, 734. [Google Scholar] [CrossRef] [PubMed]
- Rutten, G.; Van Eijk, J.; Beek, M.; Van Der Velden, H. Patient education about cough: Effect on the consulting behaviour of general practice patients. Br. J. Gen. Practice 1991, 41, 289–292. [Google Scholar]
- Johnson, A.; Sandford, J. Written and verbal information versus verbal information only for patients being discharged from acute hospital settings to home: Systematic review. Health Educ. Res. 2004, 20, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessels, R.P.C. Patients’ Memory for Medical Information. J. R. Soc. Med. 2003, 96, 219–222. [Google Scholar] [CrossRef] [Green Version]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M.; et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; King, R.; Goergen, S.K.; Melder, A.; Neeman, N.; Hadley, A.; Hutchinson, A.M. Semistructured interviews regarding patients’ perceptions of Choosing Wisely and shared decision-making: An Australian study. BMJ Open 2019, 9, e031831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catho, G.; Centemero, N.S.; Catho, H.; Ranzani, A.; Balmelli, C.; Landelle, C.; Zanichelli, V.; Huttner, B.D. Factors determining the adherence to antimicrobial guidelines and the adoption of computerised decision support systems by physicians: A qualitative study in three European hospitals. Int. J. Med. Inform. 2020, 141, 104233. [Google Scholar] [CrossRef] [PubMed]
- Moffatt-Bruce, S.D.; Hilligoss, B.; Gonsenhauser, I. ERAS: Safety checklists, antibiotics, and VTE prophylaxis. J. Surg. Oncol. 2017, 116, 601–607. [Google Scholar] [CrossRef]
- Levinson, W.; Kao, A.; Kuby, A.; Thisted, R.A. Not all patients want to participate in decision making. J. Gen. Intern. Med. 2005, 20, 531–535. [Google Scholar] [CrossRef] [Green Version]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Level of Engagement | Description | This Study |
|---|---|---|
| Partner | Establish partnership with patients | We partnered with two patient partners with LBP 1. |
| Engage | Engage patients in key role of planning, steering, and implementing. | The two patient partners were engaged in each step of the process, proposing the research questions, designing participant recruitment materials, data collection, analysis and interpretation of results, and refining the LBP prescription pad. |
| Inform | Inform patients of benefits, harms and uncertainties about tests, treatments and other procedures. | Exploring views and perspectives of patient partners and participants, we developed a LBP prescription pad as a knowledge translation intervention about treatment options, reasons for imaging, risks of unnecessary imaging, and follow-up to manage LBP. |
| Empower | Empower patients for shared decision making with healthcare providers. | The LBP prescription pad is intended to promote better patient-clinician conversations about unnecessary imaging. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madani Larijani, M.; Dumba, C.; Thiessen, H.; Palen, A.; Carr, T.; Vanstone, J.R.; Fourney, D.R.; Hartness, C.; Parker, R.; Groot, G. Development of a Patient-Oriented Intervention to Support Patient-Provider Conversations about Unnecessary Lower Back Pain Imaging. Int. J. Environ. Res. Public Health 2021, 18, 2786. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052786
Madani Larijani M, Dumba C, Thiessen H, Palen A, Carr T, Vanstone JR, Fourney DR, Hartness C, Parker R, Groot G. Development of a Patient-Oriented Intervention to Support Patient-Provider Conversations about Unnecessary Lower Back Pain Imaging. International Journal of Environmental Research and Public Health. 2021; 18(5):2786. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052786
Chicago/Turabian StyleMadani Larijani, Maryam, Cindy Dumba, Heather Thiessen, Angie Palen, Tracey Carr, Jason R. Vanstone, Daryl R. Fourney, Collin Hartness, Robert Parker, and Gary Groot. 2021. "Development of a Patient-Oriented Intervention to Support Patient-Provider Conversations about Unnecessary Lower Back Pain Imaging" International Journal of Environmental Research and Public Health 18, no. 5: 2786. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052786