
Characteristics of Physical Exercise Programs for Older Adults in Latin America: A Systematic Review of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy for the Identification of Studies
- (a)
- PubMed: Type of article: randomized controlled trial, Date of publication: 5 years, Language: English, Spanish and Portuguese, Age: aged (65+ years) and 80 and over (80+ years).
- (b)
- Scopus: Exclusion: Medline, Year of publication: 2015 to 2020, Status of publication: final, Type of document: article, Country: Latin American countries, Language: English, Spanish and Portuguese, Keyword: words that are related to the subject under study.
- (c)
- SciELO: Country: Brazil, Colombia and Chile, Year of publication: 2015 to 2020, Type of literature: article.
2.2. Selection of Studies and Inclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment Tool and Consensus on Exercise Reporting Template (CERT) Assessment Form
2.5. Strategy for Data Synthesis
3. Results
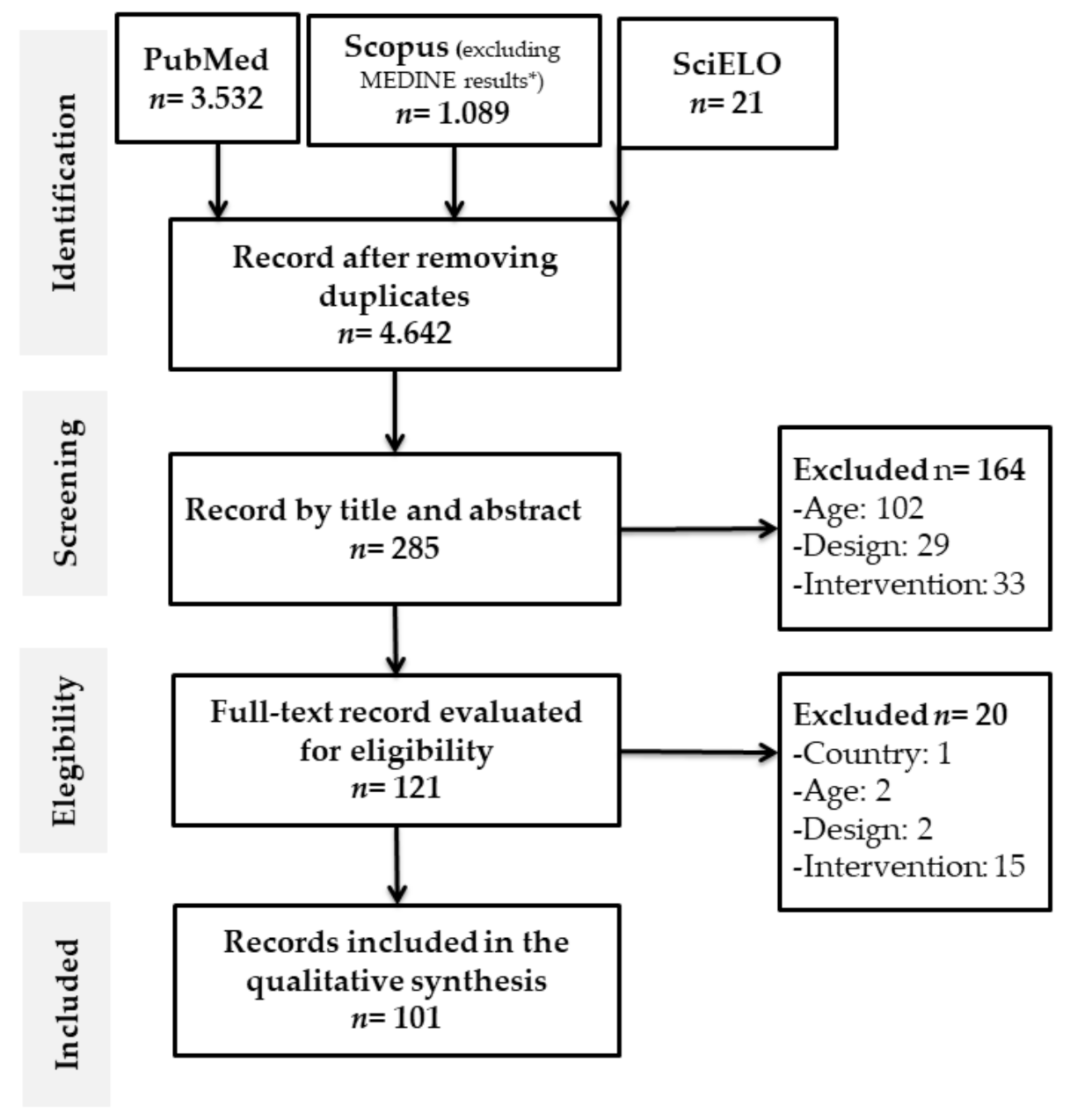
3.1. Literature Search
3.2. General Characteristics of the Studies
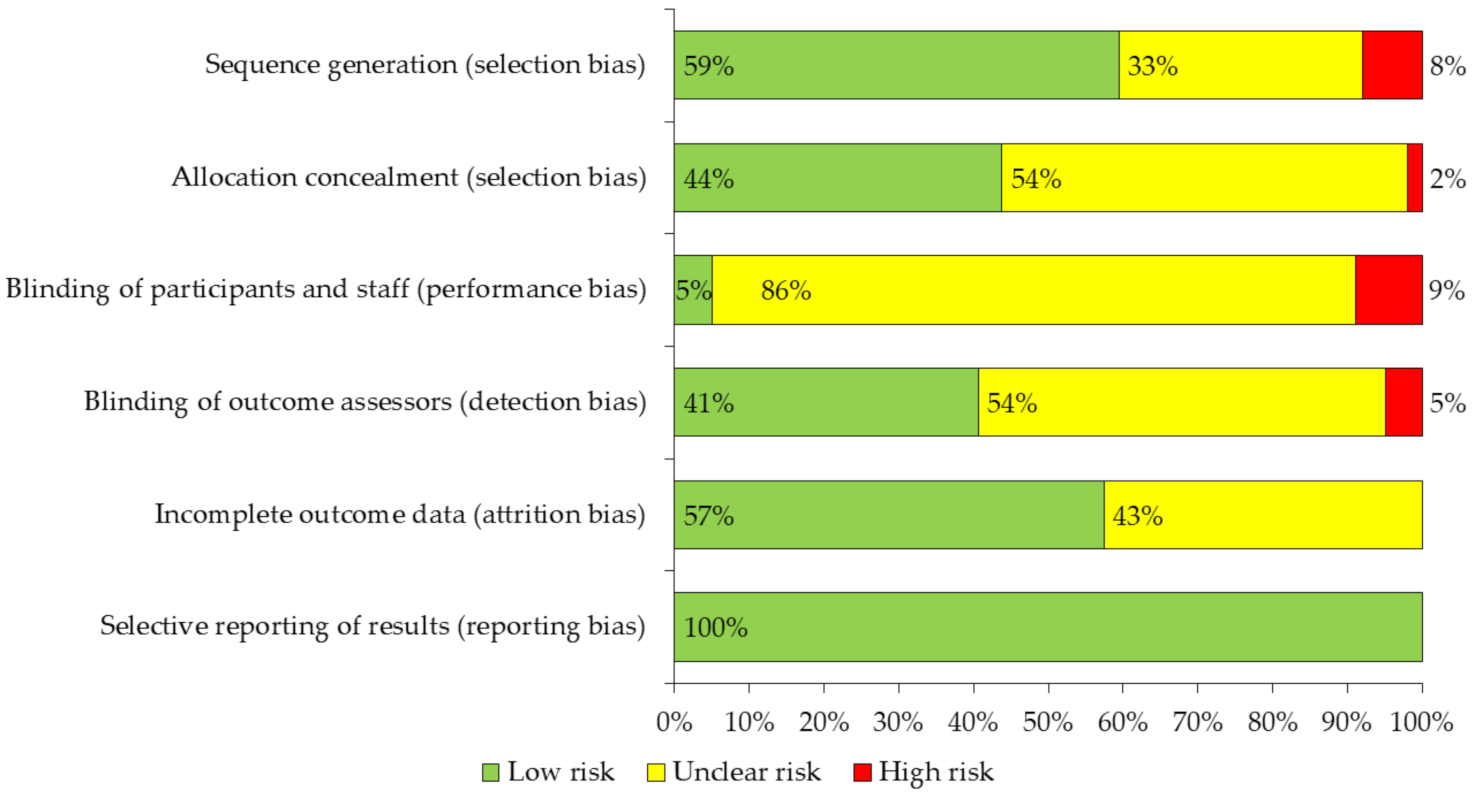
3.3. Assessment of Risk of Bias and CERT Compliance Level
3.4. Main Characteristics of the Interventions
3.5. Outcome Variables Analyzed
- (a)
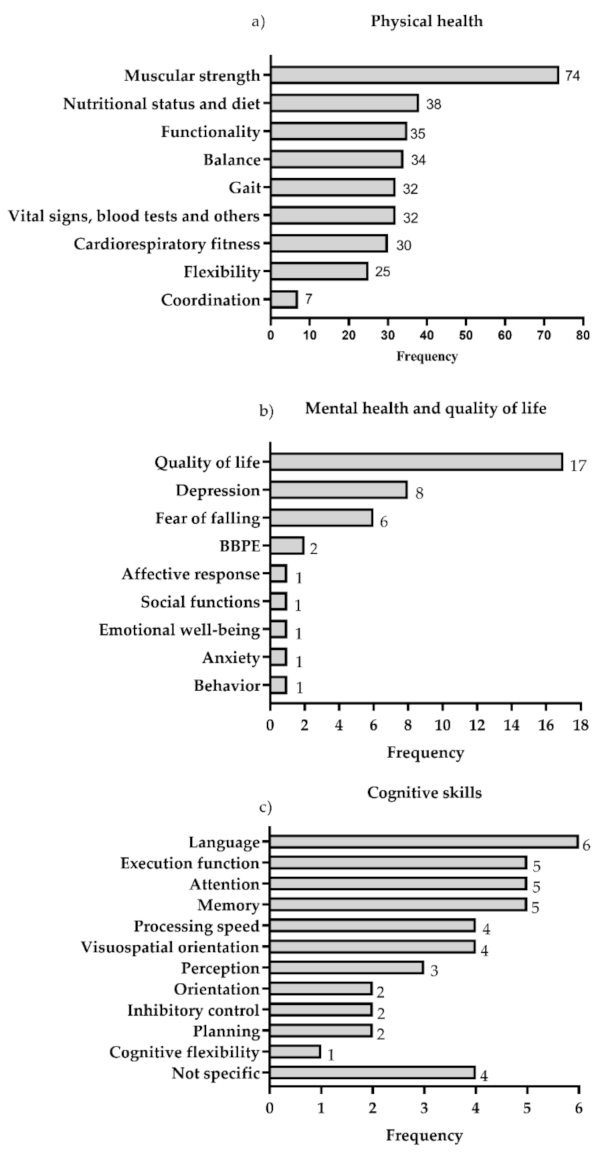
- Physical health: This category was considered in 100% of the studies and was divided into 10 outcome variables. Of these, the most evaluated was muscle strength (74 of the studies). The following most frequent were: nutritional status and diet, functionality, balance, gait and vital signs, blood tests and others (blood pressure, pain, dyspnea, heart rate variability and blood tests). The least evaluated was coordination (7 studies) (Figure 3a).
- (b)
- Mental health and quality of life: The mental health and quality of life categories were considered only in 28% of the studies, and was grouped into nine outcome variables related to emotional, psychological and social well-being. The most evaluated was quality of life, included in 17 studies, followed by depression and fear of falling, evaluated in eight and six studies, respectively (Figure 3b).
- (c)
- Cognitive Skills: the category of cognitive skills was considered only in 11% of the studies and 12 outcome variables were grouped. The most evaluated was language, included in six of the studies, followed by memory, attention and executive function, evaluated in five studies (Figure 3c).
3.6. Assessment Instruments Used
- (a)
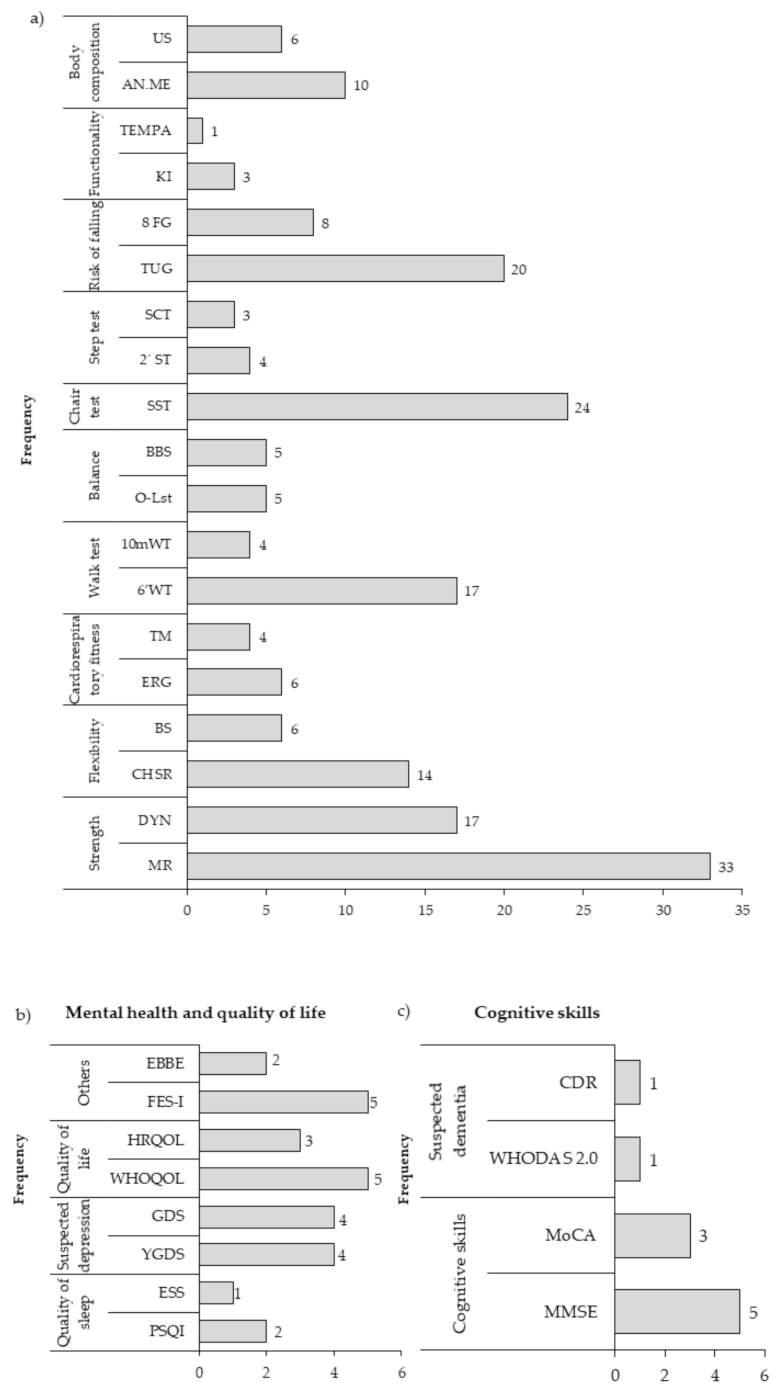
- Physical health instruments: 63 instruments were used, which were grouped into ten categories (strength, flexibility, cardiorespiratory fitness, walk test, balance, chair test, step test, risk of falls, functionality and body composition), being the most used instruments the maximum repetition to measure muscle strength (33 studies), the sit-to-stand test in tests that use a chair (24 studies), the timed up and go in tests of risk of falling (20 studies) and the test of 6-min walk in walking tests (17 studies) (Figure 4a).
- (b)
- Mental health and quality of life instruments: 18 instruments were used, which were grouped into four categories (quality of sleep, suspected depression, quality of life and others, which included instruments that evaluated affectivity, efficacy, mood, feelings, entertainment and perception barriers). The most widely used instruments were the Falls Efficacy Scale International (FES-I), the World Health Organization Quality of Life (WHOQoL), the Geriatric Depression Scale (GDS) and the Yesavage Geriatric Depression (YGDS) (Figure 4b).
- (c)
- Cognitive skills instruments: 22 instruments were used that were grouped into two categories (cognitive skills and suspected dementia). Of all the instruments, the most used were the Mini Mental State Examination (MMSE) in five studies and the Montreal Cognitive Assessment (MoCA) (Figure 4c).
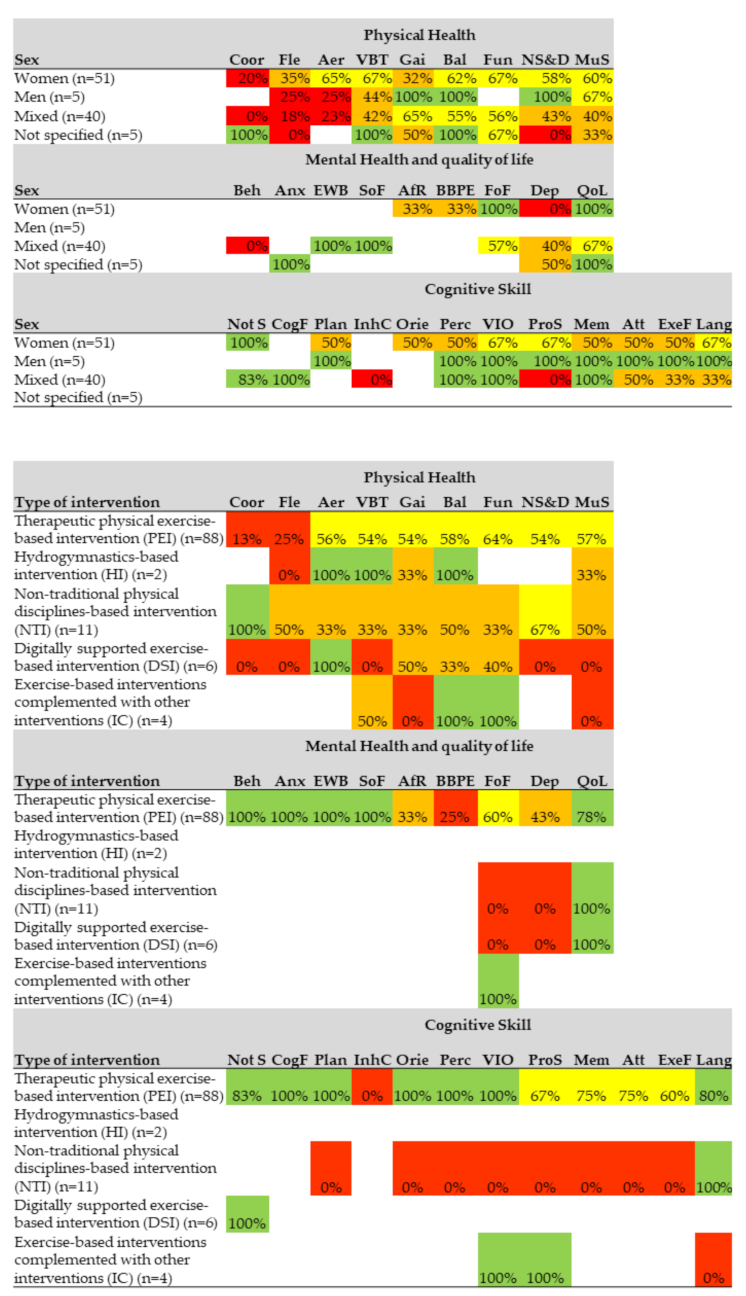
3.7. Effects by Sex and Type of Intervention
4. Discussion
4.1. General Characteristics of the Articles Reviewed
4.2. Evaluation of the Methodological Quality of the Studies and CERT Compliance
4.3. Main Characteristics of the Interventions
4.4. Outcome Variables Studied in the Articles and Instruments Used in Evaluations
4.5. Effects by Sex and by Type of Intervention
4.6. Limitations
4.7. How Does this Literature Review Contribute to the Existing One?
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Aging. WHO: Washington, DC, USA, 2015. Available online: http://www.who.int/topics/ageing/es/ (accessed on 24 July 2020).
- World Population Prospects 2019: 2019 Revision|Multimedia Library—United Nations Department of Economics and Social Affairs Un.org. 2020. Available online: https://www.un.org/development/desa/publications/world-population-prospects-2019-highlights.html (accessed on 24 July 2020).
- World Population Ageing 2019: 2019 Revision|Multimedia Library—United Nations Department of Economics and Social Affairs Un.org. 2020. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 24 July 2020).
- Machado-Cuétara, R.L.; Bazán-Machado, M.A.; Izaguirre-Bordelois, M. Principales Factores de Riesgo Asociados a las Caídas en Ancianos del área de Salud Guanabo. MEDISAN 2014, 18, 158–164. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S102930192014000200003&lng=es (accessed on 21 July 2020).
- Sun, F.; Norman, I.J.; While, A.E. Physical activity in older people: A systematic review. BMC Public Health 2013, 13, 449. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Farías, N.; Martino-Fuentealba, P.; Infante-Grandon, G.; Cortinez-O’Ryan, A. Physical inactivity in Chile: we must answer to global call. Rev. Méd. Chile 2017, 145, 12. [Google Scholar]
- World Health Organization. Diet and Physical Activity Factsheet. Secondary Diet and Physical Activity Factsheet. 2013. Available online: http://www.who.int/dietphysicalactivity/factsheet_inactivity/en/index.html (accessed on 21 July 2020).
- Guthold, R.; Stevens, G.; Riley, L.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, 1077–1086. [Google Scholar] [CrossRef] [Green Version]
- Roca, R. Actividad Física y Salud en el adulto mayor de 6 países latinoamericanos: Review. Rev. Cienc. Act. Física UCM 2016, 17, 77–86. [Google Scholar]
- Salinas, J.; Bello, M.; Flores, A.; Carbullanca, L.; Torres, M. Actividad física con adultos y adultos mayores en Chile: Resultados de un programa piloto. Rev. Chil. Nutr. 2005, 32, 215–224. [Google Scholar] [CrossRef]
- Kruger-Gonçalves, A.; Ribeiro-Teixeira, A.; Cristina-Valentini, N.; Rodriguez de Varga, A.; Dias-Possamai, V.; Feijó-Martins, V. Multicomponent physical activity program: Study with faller and non-faller older adults. J. Phys. Educ 2019, 30. [Google Scholar] [CrossRef]
- Ogawa, E.F.; You, T.; Leveille, S.G. Potential Benefits of Exergaming for Cognition and Dual-Task Function in Older Adults: A Systematic Review. J. Aging. Phys. Act. 2016, 24, 332–336. [Google Scholar] [CrossRef]
- Costantino, S.; Paneni, F.; Cosentino, F. Ageing, metabolism and cardiovascular disease. J. Physiol. 2016, 594, 2061–2073. [Google Scholar] [CrossRef] [PubMed]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of different exercise interventions on risk of falls, gait agilily, and balance in physical frail older adults: A sistematic review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Izquierdo, M.; Häkkinen, K.; Ibañez, J.; Garrues, M.; Antón, A.; Zúñiga, A.; Larrión, J.L.; Gorostiaga, E.M. Effects of strength training on muscle power and serum hormones in middle-aged and older men. J. Appl. Physiol. 2001, 90, 1497–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izquierdo, M.; Ibañez, J.; Hakkinen, K.; Kraemer, W.J.; Larrión, J.L.; Gorostiaga, E.M. Once weekly combined resistance and cardiovascular training in healthy older men. Med. Sci. Sports Exerc. 2004, 36, 435–443. [Google Scholar] [CrossRef] [Green Version]
- Cordero, A.; Solano, R. Impacto de la actividad física en salud mental de la persona mayor. Rev. Médica Costa Rica Cent. 2010, 593, 305310. [Google Scholar]
- OMS. Lucha contra las ENT: «Mejores Inversiones» y Otras Intervenciones Recomendadas Para la Prevención y el Control de las Enfermedades no Transmisibles; Ginebra, Organización Mundial de la Salud: Geneva, Switzerland, 2017. [Google Scholar]
- WHO Guidelines on Physical Activity and Sedentary Behaviour. World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 30 December 2020).
- ACTIVE: Paquete de Intervenciones Técnicas Para Acrecentar la Actividad Física [ACTIVE: A Technical Package for Increasing Physical Activity]; Ginebra, Organización Mundial de la Salud: Geneva, Switzerland, 2019.
- Fundación interamericana del corazón Argentina. La Actividad Física en Personas Mayores: Guía Para Promover un Envejecimiento Activo, 1st ed.; Fundación Navarro Viola: Buenos Aires, Argentina, 2018; pp. 17–26. [Google Scholar]
- Ministerio de Salud, Secretaria Nacional del Deporte. Uruguay. 2004. Available online: http://www.codajic.org/ (accessed on 26 July 2020).
- Rejas, N.; Ministerio de Salud. Documento Técnico: Gestión Para la Promoción de la Actividad Física Para la salud. Perú. 2015. Available online: http://docs.bvsalud.org/ (accessed on 26 July 2020).
- Costa Rica. In Ministerio de Salud y Ministerio del Deporte y Recreación. Plan Nacional de Actividad Física y Salud 2011–2021, 1st ed.; El ministerio: San José, CA, USA, 2011; Available online: https://www.ministeriodesalud.org.cr (accessed on 27 July 2020).
- Bukele, N. Deporte, Plan Cuscatlán. Un nuevo Gobierno Para el Salvador. El Salvador. 2019. Available online: https://www.plancuscatlan.com/ (accessed on 27 July 2020).
- Guía para Actividad Física Para Adultos Mayores. Panamá. 2018. Available online: https://www.hospitalsantafepanama.com/ (accessed on 27 July 2020).
- Paraguay; Ministerio de Salud Pública y Bienestar Social; Dirección General de Vigilancia de la Salud. Dirección de Vigilancia de Enfermedades No Transmisibles; Manual de Promoción de Actividad Física; MSP y BS: Asunción, Paraguay, 2014. [Google Scholar]
- Comisión de Alimentación y Nutrición de Puerto Rico. Guía de Alimentación y Actividad Física Para Puerto Rico. Puerto Rico. 2015. Available online: http://www.salud.gov.pr/ (accessed on 27 July 2020).
- Gobierno de Chile. Recomendaciones Para la Práctica de Actividad Física Según Curso de la Vida, 1st ed.; Gobierno de Chile: Santiago, Chile, 2017; pp. 48–51. [Google Scholar]
- Honduras, Secretaria de Salud. Guía de Actividad Física Para Facilitadores de Salud/Honduras, 1st ed.; Línea Creative: Tegucigalpa, Honduras, 2016. [Google Scholar]
- ACEMI. Se Activo Físicamente y Siéntete Bien. Colombia. 2011 [3 de agosto de 2020]. Available online: https://minsalud.gov.co/ (accessed on 27 July 2020).
- Ministerio de Salud Pública del Ecuador Coordinación Nacional de Nutrición. Guía de Actividad Física Dirigida al Personal de Salud II. Ecuador. 2011. Available online: https://bibliotecapromocion.msp.gob.ec/ (accessed on 27 July 2020).
- CONACYT, Consejo Nacional de Ciencia y Tecnología. Guías Alimentarias y de Actividad Física, en Contexto de Sobrepeso y Obesidad en la Población Mexicana. México. 2015. Available online: https://www.anmm.org.mx/ (accessed on 27 July 2020).
- Matsudo, S.M.; Matsudo, V.R.; Araujo, T.L.; Andrade, D.R.; Andrade, E.L.; Oliveira, L.C.; Braggion, G.F. The agita São Paulo Program as a model for using physical activity to promote health. Rev. Panam. Salud Publica 2003, 14, 265–272. [Google Scholar] [CrossRef] [Green Version]
- Matsudo, M.S.; Matsudo, R.V.; Araujo, T.L.; Andrade, D.R.; Oliveira, M.L. From diagnosis to action: The experience of Agita São Paulo program in promoting and active lifeestyle. Rev. Bras. Ativ. Fís. Saúde 2008, 13, 178–184. Available online: https://www.researchgate.net/publication/238744260_do_diagnostico_a_acao_a_experiencia_do_programa_agita_sao_paulo_na_promocao_do_estilo_de_vida_ativo (accessed on 24 July 2020).
- Liberati, A.; Altman, D.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.; Ioannidis, J.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGowan, J.; Sampson, M.; Salzwedel, D.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [Green Version]
- The Cochrane Collaboration; Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. 2011. Available online: www.cochrane-handbook.org (accessed on 20 February 2021).
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R.; Beck, B.; Bennell, K. Consensus on Exercise Reporting Template (CERT): Modified Delphi Study. Phys. Ther. 2016, 96, 1514–1524. [Google Scholar] [CrossRef]
- de Queiroz, J.L.; Sales, M.M.; Sousa, C.V.; Silva, S.; Asano, R.; Vila Nova-de Moraes, J.F. 12 weeks of Brazilian jiu-jitsu training improves functional fitness in elderly men. Sport Sci. Health 2016, 12, 291–295. [Google Scholar] [CrossRef]
- Antunes, H.K.; De Mello, M.T.; de Aquino-Lemos, V.; Santos-Galduroz, R.F.; Camargo-Galdieri, L.; Amodeo-Bueno, O.F.; Tufik, S.; D’Almeida, V. Aerobic physical exercise improved the cognitive function of elderly males but did not modify their blood homocysteine levels. Dement. Geriatr. Cogn. Dis. Extra 2015, 5, 13–24. [Google Scholar] [CrossRef]
- Santos, S.M.; da Silva, R.A.; Terra, M.B.; Almeida, I.A.; De Melo, L.B.; Ferraz, H.B. Balance versus resistance training on postural control in patients with Parkinson’s disease: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2017, 53, 173–183. [Google Scholar] [PubMed]
- de Oliveira, R.T.; Felippe, L.A.; Bucken-Gobbi, L.T.; Barbieri, F.A.; Christofoletti, G. Benefits of Exercise on the Executive Functions in People with Parkinson Disease: A Controlled Clinical Trial. Am. J. Phys. Med. Rehabil. 2017, 96, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.C.; Oliveira, R.G.; Pires-Oliveira, D.A. Comparison between static stretching and the Pilates method on the flexibility of older women. J. Bodyw. Mov. Ther. 2016, 20, 800–806. [Google Scholar] [CrossRef]
- Mazini-Filho, M.L.; Aidar, F.J.; Costa-Moreira, O.; Gama de Matos, D.; Patrocínio de Oliveira, C.E.; Rezende de Oliveira-Venturini, G.; Paula-Costa, S.; Magalhaes-Curty, V.; Caputo-Ferreira, M.E. Comparison of the effect of two physical exercise programs on the functional autonomy, balance and flexibility of elderly women. Med. Sport 2017, 70, 288–298. [Google Scholar]
- Teodoro, J.L.; da Silva, L.X.N.; Fritsch, C.G.; Baroni, B.M.; Grazioli, R.; Boeno, F.P.; Lopez, P.; Gentil, P.; Bottaro, M.; Pinto, R.S.; et al. Concurrent training performed with and without repetitions to failure in older men: A randomized clinical trial. Scand J. Med. Sci. Sports 2019, 29, 1141–1152. [Google Scholar] [CrossRef]
- Santos, G.O.R.; Wolf, R.; Silva, M.M.; Rodacki, A.L.F.; Pereira, G. Does exercise intensity increment in exergame promote changes in strength, ¿functional capacity and perceptual parameters in pre-frail older women? A randomized controlled trial. Exp. Gerontol. 2019, 116, 25–30. [Google Scholar] [CrossRef]
- Dueñas, E.P.; Ramírez, L.P.; Ponce, E.; Curcio, C.L. Efecto sobre el temor a caer y la funcionalidad de tres programas de intervención. Ensayo clínico aleatorizado [Effect on fear of falling and functionality of three intervention programs. A randomised clinical trial]. Rev. Esp. Geriatr. Gerontol. 2019, 54, 68–74. [Google Scholar] [CrossRef]
- Pirauá, A.L.T.; Cavalcante, B.R.; de Oliveira, V.M.A.; Beltrao, N.B.; De Amorin Batista, G.; Pitangui, A.C.R.; Behm, D.; De Araújo, R.C. Effect of 24-week strength training on unstable surfaces on mobility, balance, and concern about falling in older adults. Scand J. Med. Sci. Sports 2019, 29, 1805–1812. [Google Scholar] [CrossRef]
- Arantes, P.M.M.; Días, J.M.D.; Fonseca, F.F.; Oliveira, A.M.B.; Oliveira, M.C.; Pereira, L.S.M.; Dias, R.C. Effect of a Program Based on Balance Exercises on Gait, Functional Mobility, Fear of Falling, and Falls in Prefrail Older Women: A Randomized Clinical Trial. Top. Geriatr. Rehabil. 2015, 31, 113–120. [Google Scholar] [CrossRef]
- Lima, L.G.; Bonardi, J.M.; Campos, G.O.; Bertani, R.F.; Scher, L.M.; Louzada-Junior, P.; Moriguti, J.C.; Ferrioli, E.; Lima, N.K. Effect of aerobic training and aerobic and resistance training on the inflammatory status of hypertensive older adults. Aging Clin. Exp. Res. 2015, 27, 483–489. [Google Scholar] [CrossRef]
- De Oliveira, D.V.; Da Cunha, P.M.; Dos Santos-Campos, R.; Do-Nascimento, M.A.; Antunes, M.D.; Do Nascimento, J.R.A.; Mayhew, J.L.; Cavaglieri, C.R. Effect of circuit resistance training on blood biomarkers of cardiovascular disease risk in older women. J. Phys. Educ. 2019, 30. [Google Scholar] [CrossRef] [Green Version]
- Langoni, C.D.S.; Resende, T.L.; Barcellos, A.B.; Cecchele, B.; Knob, M.S.; Silva, T.D.N.; da Rosa, J.N.; Diogo, T.S.; Filho, I.G.D.S.; Schwanke, C.H.A. Effect of Exercise on Cognition, Conditioning, Muscle Endurance, and Balance in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Trial. J. Geriatr. Phys. Ther. 2019, 42, E15–E22. [Google Scholar] [CrossRef]
- Nascimento, M.A.D.; Gerage, A.M.; Silva, D.R.P.D.; Ribeiro, A.S.; Machado, D.G.D.S.; Pina, F.L.C.; Tomeleri, C.M.; Venturini, D.; Barbosa, D.S.; Mayhew, J.L.; et al. Effect of resistance training with different frequencies and subsequent detraining on muscle mass and appendicular lean soft tissue, IGF-1, and testosterone in older women. Eur. J. Sport Sci. 2019, 19, 199–207. [Google Scholar] [CrossRef]
- Dantas, F.F.; Brasileiro-Santos Mdo, S.; Batista, R.M.; do Nascimento, L.S.; Castellano, L.R.; Ritti-Dias, R.M.; Lima, K.C.; Santos-Ada, C. Effect of Strength Training on Oxidative Stress and the Correlation of the Same with Forearm Vasodilatation and Blood Pressure of Hypertensive Elderly Women: A Randomized Clinical Trial. PLoS ONE 2016, 11, e0161178. [Google Scholar] [CrossRef]
- Leandro, M.P.G.; de Moura, J.L.S.; Barros, G.W.P.; da Silva-Filho, A.P.; Farias, A.C.O.; Carvalho, P.R.C. Effect of the aerobic component of combined training on the blood pressure of hypertensive elderly women. Rev. Bras. Med. Esporte 2019, 25, 469–473. [Google Scholar] [CrossRef]
- de Carvalho-Fonseca, R.G.; Silva, A.M.; Teixeira, L.F.; Silva, V.R.; Dos Reis, L.M.; Silva-Santos, A.T. Effect of the Auricular Acupoint Associated with Physical Exercise in Elderly People: A Randomized Clinical Test. J. Acupunct. Meridian Stud. 2018, 11, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Tiggemann, C.L.; Días, C.P.; Radaelli, R.; Massa, J.C.; Bortoluzzi, R.; Schoenell, M.C.; Noll, M.; Alberton, C.L.; Kruel, L.F. Effect of traditional resistance and power training using rated perceived exertion for enhancement of muscle strength, power, and functional performance. Age (Dordr) 2016, 38, 42. [Google Scholar] [CrossRef] [Green Version]
- da Silva, R.G.; da Silva, D.R.P.; Pina, F.L.C.; do Nascimento, M.A.; Ribeiro, A.S.; Cyrino, E.S. Effect of two different weekly resistance training frequencies on muscle strength and blood pressure in normotensive older women. Rev. Bras. Cineantropometria Desempenho Hum. 2017, 19, 118–127. [Google Scholar]
- Taglietti, M.; Facci, L.M.; Trelha, C.S.; de Melo, F.C.; Da Silva, D.W.; Sawczuk, G.; Ruivo, T.M.; de Souza, T.B.; Sforza, C.; Cardoso, J.R. Effectiveness of aquatic exercises compared to patient-education on health status in individuals with knee osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2018, 32, 766–776. [Google Scholar] [CrossRef] [Green Version]
- Franco, M.R.; Sherrington, C.; Tiedemann, A.; Pereira, L.S.; Perracini, M.R.; Faria, C.R.; Pinto, R.Z.; Pastre, C.M. Effectiveness of Senior Dance on risk factors for falls in older adults (DanSE): A study protocol for a randomised controlled trial. BMJ Open 2016, 30, e013995. [Google Scholar] [CrossRef]
- Ferreira, C.B.; Teixeira, P.D.S.; Alves Dos Santos, G.; Dantas Maya, A.T.; Americano Do Brasil, P.; Souza, V.C.; Córdova, C.; Ferreira, A.P.; Lima, R.M.; Nobrega, O.T. Effects of a 12-Week Exercise Training Program on Physical Function in Institutionalized Frail Elderly. J. Aging Res. 2018, 2018, 1–8. [Google Scholar] [CrossRef] [Green Version]
- López, N.; Véliz, A.; Soto-Añari, M.; Ollari, J.; Chesta, S.; Allegri, R. Effects of a combined program of physical activity and cognitive training in Chilean patients with mild Alzheimer. Neurol. Argent 2015, 7, 131–139. [Google Scholar] [CrossRef]
- Suzuki, F.S.; Evangelista, A.L.; Teixeira, C.V.L.S.; Paunksnis, M.R.R.; Rica, R.L.; de Toledo Evangelista, R.A.G.; Joao, G.A.; Doro, M.R.; Sita, D.M.; Serra, A.J.; et al. Effects of a multicomponent exercise program on the functional fitness in elderly women. Rev. Bras. Med. Esporte 2018, 24, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Ortiz-Ortiz, M.; Gómez-Miranda, L.M.; Chacón-Araya, Y.; Moncada-Jiménez, J. Effects of a physical activity program on depressive symptoms and functional capacity of institutionalized mexican older adults. J. Phys. Educ. Sport 2019, 19, 890–896. [Google Scholar]
- Guedes, J.M.; Bortoluzzi, M.G.; Matte, L.P.; De Andrade, C.M.; Zulpo, N.C.; Sebben, V.; Filho, H.T. Effects of combined training on the strength, endurance and aerobic power in the elderly women. Rev. Bras. Med. Esporte 2016, 22, 480–484. [Google Scholar] [CrossRef] [Green Version]
- Agner, V.F.C.; Garcia, M.C.; Taffarel, A.A.; Mourao, C.B.; da Silva, I.P.; da Silva, S.P.; Peccin, M.S.; Lombardi, I.J. Effects of concurrent training on muscle strength in older adults with metabolic syndrome: A randomized controlled clinical trial. Arch. Gerontol. Geriatr. 2018, 75, 158–164. [Google Scholar] [CrossRef]
- Rodrigues-Krause, J.; Farinha, J.B.; Ramis, T.R.; Macedo, R.C.O.; Boeno, F.P.; Dos Santos, G.C.; Vargas, J.J.; Lopez, P.; Grazioli, R.; Costa, R.R.; et al. Effects of dancing compared to walking on cardiovascular risk and functional capacity of older women: A randomized controlled trial. Exp. Gerontol. 2018, 114, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, R.; Fuchs, S.C.; Kruel, L.F.M.; Cadore, E.L.; Alberton, C.L.; Pinto, R.S.; Radaelli, R.; Schoenell, M.; Izquierdo, M.; Tanaka, H.; et al. Effects of different concurrent resistance and aerobic training frequencies on muscle power and muscle quality in trained elderly men: A randomized clinical trial. Aging Dis. 2016, 7, 697–704. [Google Scholar] [CrossRef] [Green Version]
- Ramirez-Campillo, R.; Diaz, D.; Martinez-Salazar, C.; Valdés-Badilla, P.; Delgado-Floody, P.; Méndez-Rebolledo, G.; Cañas-Jamet, R.; Cristi-Moreno, C.; García-Moreno, A.; Celis-Morales, C.; et al. Effects of different doses of high-speed resistance training on physical performance and quality of life in older women: A randomized controlled trial. Clin. Interv. Aging 2016, 11, 1797–1804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neto, A.G.R.; Santos, M.S.; Silva, R.J.S.; de Santana, J.M.; da Silva-Grigoletto, M.E. Effects of different neuromuscular training protocols on the functional capacity of elderly women. Rev. Bras. Med. Esporte 2018, 24, 140–144. [Google Scholar] [CrossRef]
- Cavalcante, E.F.; Ribeiro, A.S.; do Nascimento, M.A.; Silva, A.M.; Tomeleri, C.M.; Nabuco, H.C.G.; Pina, F.L.C.; Mayhew, J.L.; Silva-Grigoletto, M.E.D.; da Silva, D.R.P.; et al. Effects of Different Resistance Training Frequencies on Fat in Overweight/Obese Older Women. Int. J. Sports Med. 2018, 39, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Días, C.P.; Toscan, R.; de Camargo, M.; Pereira, E.P.; Griebler, N.; Baroni, B.M.; Tiggeman, C.L. Effects of eccentric-focused and conventional resistance training on strength and functional capacity of older adults. Age (Dordr) 2015, 37, 99. [Google Scholar] [CrossRef] [Green Version]
- Henrique, P.P.B.; Colussi, E.L.; De Marchi, A.C.B. Effects of Exergame on Patients’ Balance and Upper Limb Motor Function after Stroke: A Randomized Controlled Trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 2351–2357. [Google Scholar] [CrossRef]
- Ramírez-Villada, J.F.; Cadena-Duarte, L.L.; Gutiérrez-Galvis, A.R.; Argothy-Bucheli, R.; Moreno-Ramírez, Y. Effects of explosive and impact exercises on gait parameters in elderly women. Rev. Fac. Med. 2019, 67, 493–501. [Google Scholar] [CrossRef] [Green Version]
- de Resende-Neto, A.G.; Oliveira Andrade, B.C.; Cyrino, E.S.; Behm, D.G.; De-Santana, J.M.; Da Silva-Grigoletto, M.E. Effects of functional and traditional training in body composition and muscle strength components in older women: A randomized controlled trial. Arch. Gerontol. Geriatr. 2019, 84, 103902. [Google Scholar] [CrossRef]
- De Lourdes Feitosa Neta, M.; De Resende-Neto, A.G.; Dantas, E.H.M.; De Almeida, M.B.; Wichi, R.B.; Da Silva Grigoletto, M.E. Effects of functional training on strength, muscle power and quality of life in pre-frail older women. Motricidade 2016, 12, 61–68. [Google Scholar]
- Bacha, J.M.R.; Gomes, G.C.V.; de Freitas, T.B.; Viveiro, L.A.P.; da Silva, K.G.; Bueno, G.C.; Varise, E.M.; Torriani-Pasin, C.; Castilho-Alonso, A.; Silva-Luna, N.M.; et al. Effects of Kinect Adventures Games Versus Conventional Physical Therapy on Postural Control in Elderly People: A Randomized Controlled Trial. Games Health 2018, 7, 24–36. [Google Scholar] [CrossRef]
- Dos Santos, L.; Ribeiro, A.S.; Cavalcante, E.F.; Nabuco, H.C.; Antunes, M.; Schoenfeld, B.J.; Cyrino, E.S. Effects of Modified Pyramid System on Muscular Strength and Hypertrophy in Older Women. Int. J. Sports Med. 2018, 39, 613–618. [Google Scholar] [CrossRef]
- Gomeñuka, N.A.; Oliveira, H.B.; Silva, E.S.; Costa, R.R.; Kanitz, A.C.; Liedtke, G.V.; Schuch, F.B.; Peyré-Tartaruga, L.A. Effects of Nordic walking training on quality of life, balance and functional mobility in elderly: A randomized clinical trial. PLoS ONE 2019, 14, e0211472. [Google Scholar] [CrossRef]
- De Oliveira, L.C.; De Oliveira, R.G.; De Almeida Pires-Oliveira, D.A. Effects of pilates on muscle strength, postural balance and quality of life of older adults: A randomized, controlled, clinical trial. J. Phys. Ther. Sci. 2015, 27, 871–876. [Google Scholar] [CrossRef] [Green Version]
- Vale, R.G.D.S.; Da Gama, D.R.N.; Oliveira, F.B.D.; Almeida, D.S.D.M.; De Castro, J.B.P.; Meza, E.I.A.; Mattos, R.D.S.; Nunes, R.A.M. Effects of resistance training and chess playing on the quality of life and cognitive performance of elderly women: A randomized controlled trial. J. Phys. Educ. Sport 2018, 18, 1469–1477. [Google Scholar]
- Santiago, L.Ǎ.M.; Neto, L.G.L.; Pereira, G.B.; Leite, R.D.; Mostarda, C.T.; De Oliveira Brito Monzani, J.; Sousa, W.R.; Rodrigues Pinheiro, A.J.M.; Navarro, F. Effects of Resistance Training on Immunoinflammatory Response, TNF-alpha Gene Expression, and Body Composition in Elderly Women. J. Aging Res. 2018. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC6230406/ (accessed on 30 July 2020).
- Botton, C.E.; Umpierre, D.; Rech Pfeifer, L.O.; Machado, C.L.F.; Teodoro, J.L.; Días, A.S.; Pinto, R.S. Effects of resistance training on neuromuscular parameters in elderly with type 2 diabetes mellitus: A randomized clinical trial. Exp. Gerontol. 2018, 113, 141–149. [Google Scholar] [CrossRef]
- Gadelha, A.B.; Paiva, F.M.; Gauche, R.; de Oliveira, R.J.; Lima, R.M. Effects of resistance training on sarcopenic obesity index in older women: A randomized controlled trial. Arch. Gerontol. Geriatr. 2016, 65, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Barbosa Rezende, A.A.; Fernandes De Miranda, E.; Souza Ramalho, H.; Borges Da Silva, J.D.; Silva Carlotto Herrera, S.D.; Rossone Reis, G.; Dantas, E.H.M. Effects of sensory motor training of lower limb in sedentary elderly as part of functional autonomy. Rev. Andaluza Med. Deporte 2015, 8, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Martins, W.R.; Safons, M.P.; Bottaro, M.; Blasczyk, J.C.; Diniz, L.R.; Fonseca, M.C.F.; Bonini-Rocha, A.C.; Jacó de Oliveira, R. Effects of short term elastic resistance training on muscle mass and strength in untrained older adults: A randomized clinical trial. BMC Geriatr. 2015, 15, 99. [Google Scholar] [CrossRef] [Green Version]
- Gallo, L.H.; Demantova Gurjão, A.L.; Gobbi, S.; Ceccato, M.; Garcia Prado, A.K.; Jambassi Filho, J.C.; Gomes, A. Effects of static stretching on functional capacity in older women: Randomized controlled trial. J. Exerc. Physiol. Online 2015, 18, 13–22. [Google Scholar]
- Ruaro, M.F.; Santana, J.O.; Gusmão, N.; De Franca, E.; Carvalho, B.N.; Farinazo, K.B.; Bonorino, S.L.; Corralo, V.; Antonio De Sá, C.; Caperuto, E. Effects of strength training with and without blood flow restriction on quality of life in elderly women. J. Phys. Educ. Sport 2019, 19, 531–539. [Google Scholar]
- Silva, C.M.D.S.E.; Gomes Neto, M.; Saquetto, M.B.; Conceição, C.S.D.; Souza-Machado, A. Effects of upper limb resistance exercise on aerobic capacity, muscle strength, and quality of life in COPD patients: A randomized controlled trial. Clin. Rehabil. 2018, 32, 1636–1644. [Google Scholar] [CrossRef]
- Miranda-Aguilar, D.; Valdés-Badilla, P.; Herrera-Valenzuela, T.; Guzmán-Muñoz, E.; Magnani-Branco, B.H.; Méndez-Rebolledo, G.; Lopéz-Fuenzalida, A. ¿Bandas elásticas o equipos de gimnasio para el entrenamiento de adultos mayores? (¿Elastic bands or gym equipment for the training of older adults?). Retos 2019, 37, 370–378. [Google Scholar] [CrossRef]
- Cadore, E.L.; Menger, E.; Teodoro, J.L.; Da Silva, L.X.N.; Boeno, F.P.; Umpierre, D.; Botton, C.E.; Ferrari, R.; Dos Santos-Cunha, G.; Izquierdo, M.; et al. Functional and physiological adaptations following concurrent training using sets with and without concentric failure in elderly men: A randomized clinical trial. Exp. Gerontol. 2018, 110, 182–190. [Google Scholar] [CrossRef]
- De Resende Neto, A.G.; De Lourdes Feitosa Neta, M.; Santos, M.S.; La Scala Teixeira, C.V.; De Sá, C.A.; Da Silva-Grigoletto, M.E. Functional training versus traditional strength training: Effects on physical fitness indicators in pre-frail elderly women. Motricidade 2016, 12, 44–53. [Google Scholar]
- Silva, I.G.; Silva, B.S.A.; Freire, A.P.C.F.; Santos, A.P.S.D.; Lima, F.F.; Ramos, D.; Ramos, E.M.C. Functionality of patients with Chronic Obstructive Pulmonary Disease at 3 months follow-up after elastic resistance training: A randomized clinical trial. Pulmonology 2018, 24, 354–357. [Google Scholar] [CrossRef]
- Da Silva, M.A.R.; Baptista, L.C.; Neves, R.S.; De França, E.; Loureiro, H.; Rezende, M.A.C.; da Silva-Ferrerira, V.; Texeira-Veríssimo, M.; Martins, A. High intensity interval training improves health-related quality of life in adults and older adults with diagnosed cardiovascular risk. J. Phys. Educ. Sport 2019, 19, 611–618. [Google Scholar]
- Ramirez-Campillo, R.; Alvarez, C.; Garcìa-Hermoso, A.; Celis-Morales, C.; Ramirez-Velez, R.; Gentil, P.; Izquierdo, M. High-speed resistance training in elderly women: Effects of cluster training sets on functional performance and quality of life. Exp. Gerontol. 2018, 110, 216–222. [Google Scholar] [CrossRef]
- Brandão, G.S.; Gomes, G.S.B.F.; Brandão, G.S.; Callou-Sampaio, A.A.; Donner, C.F.; Oliveira, L.V.F.; Camelier, A.A. Home exercise improves the quality of sleep and daytime sleepiness of elderlies: A randomized controlled trial. Multidiscip. Resp. Med. 2018, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hall-López, J.A.; Ochoa-Martínez, P.Y.; Alarcón-Meza, E.I.; Moncada-Jiménez, J.A.; Garcia Bertruy, O.; Martin-Dantas, E.H. Hydrogymnastics training program on physical fitness in elderly women. Rev. Int. Med. Cienc. Act. Fis. Deporte 2017, 17, 283–298. [Google Scholar]
- Medeiros, L.B.; Ansai, J.H.; De Souza-Buto, M.S.; Barroso, V.V.; Farche, A.C.S.; Rossi, P.G.; Andrade, L.P.; Takahashi, A.C. Impact of a dual task intervention on physical performance of older adults who practice physical exercise. Rev. Bras. Cineantropometria Desempenho Hum. 2018, 20, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Vargas, M.Á.; Rosas, M.E. Impact of an-aerobic physical activity program in hypertensive elderly adults. Rev. Latinoam. Hipertens. 2019, 14, 142–149. [Google Scholar]
- Scarabottolo, C.C.; Garcia-Júnior, J.R.; Gobbo, L.A.; Alves, M.J.; Ferreira, A.D.; Zanuto, E.A.C.; Oliveira, W.; Destro-Christofaro, D.G. Influence of physical exercise on the functional capacity in institutionalized elderly. Rev. Bras. Med. Esporte 2017, 23, 200–203. [Google Scholar] [CrossRef] [Green Version]
- Damorim, I.R.; Santos, T.M.; Barros, G.W.P.; Carvalho, P.R.C. Kinetics of Hypotension during 50 Sessions of Resistance and Aerobic Training in Hypertensive Patients: A Randomized Clinical Trial. Arq. Bras. Cardiol. 2017, 108, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Leal, L.C.; Abrahin, O.; Rodrigues, R.P.; Da Silva, M.C.; Araújo, P.M.; De Sousa, E.C.; Pimentel, C.P.; Cortinhas-Alves, E.A. Low-volume resistance training improves the functional capacity of older individuals with Parkinson’s disease. Geriatr. Gerontol. Int. 2019, 19, 635–640. [Google Scholar] [CrossRef]
- Souza, D.; Barbalho, M.; Vieira, C.A.; Martins, W.R.; Cadore, E.L.; Gentil, P. Minimal dose resistance training with elastic tubes promotes functional and cardiovascular benefits to older women. Exp. Gerontol. 2019, 115, 132–138. [Google Scholar] [CrossRef]
- Santos, G.D.; Nunes, P.V.; Stella, F.; Brum, P.S.; Yassuda, M.S.; Ueno, L.M.; Gattaz, W.F.; Forlenza, O.V. Multidisciplinary rehabilitation program: Effects of a multimodal intervention for patients with Alzheimer’s disease and cognitive impairment without dementia. Rev. Psiquiatr. Clin. 2015, 42, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Moreira, N.B.; Gonçalves, G.; da Silva, T.; Zanardini, F.E.H.; Bento, P.C.B. Multisensory exercise programme improves cognition and functionality in institutionalized older adults: A randomized control trial. Physiother. Res. Int. 2018, 23, e1708. [Google Scholar] [CrossRef] [PubMed]
- Martinez, A.; Selaive, R.; Astorga, S.; Olivares, P. Neuromuscular training in institutionalized older adults: A functional approach to preventing fall. Nutr. Clin. Diet. Hosp. 2018, 38, 40–45. [Google Scholar]
- Santana, M.; Pina, J.; Duarte, G.; Neto, M.; Machado, A.; Dominguez-Ferraz, D. Nintendo wii effects on cardiorespiratory fitness in older adults: A randomized clinical trial. a pilot trial. Fisioterapia 2016, 38, 71–77. [Google Scholar] [CrossRef]
- Gomeñuka, N.A.; Oliveira, H.B.; da Silva, E.S.; Passos-Monteiro, E.; da Rosa, R.G.; Carvalho, A.R.; Costa, R.R.; Rodríguez, M.C.; Pellegrini, B.; Peyré-Tartaruga, L.A. Nordic walking training in elderly, a randomized clinical trial. Part II: Biomechanical and metabolic adaptations. Sports Med. Open 2020, 6. [Google Scholar] [CrossRef] [Green Version]
- Coelho-Júnior, H.J.; de Oliveira-Gonçalvez, I.; Sampaio, R.A.C.; Sewo Sampaio, P.Y.; Cadore, E.L.; Izquierdo, M.; Marzetti, E.; Uchida, M.C. Periodized and non-periodized resistance training programs on body composition and physical function of older women. Exp. Gerontol. 2019, 121, 10–18. [Google Scholar]
- Pestana, M.D.S.; Netto, E.M.; Pestana, M.C.S.; Pestana, V.S.; Schinoni, M.I. Pilates versus resistance exercise on the serum levels of hs-CRP, in the abdominal circumference and body mass index (BMI) in elderly individuals. Motricidade 2016, 12, 128. [Google Scholar] [CrossRef]
- Gambassi, B.B.; Almeida, F.J.F.; Sauaia, B.A.; Novais, T.M.G.; Furtado, A.E.A.; Chaves, L.F.C. Resistance training contributes to variability in heart rate and quality of the sleep in elderly women without comorbidities. J. Exerc. Physiol. Online 2015, 18, 112–123. [Google Scholar]
- Tomeleri, C.M.; Ribeiro, A.S.; Souza, M.F.; Schiavoni, D.; Schoenfeld, B.J.; Venturini, D.; Barbosa, D.S.; Landucci, K.; Sardinha, L.B.; Cyrino, E. Resistance training improves inflammatory level, lipid and glycemic profiles in obese older women: A randomized controlled trial. Exp. Gerontol. 2016, 84, 80–87. [Google Scholar] [CrossRef]
- Ribeiro, A.S.; Schoenfeld, B.J.; Pina, F.L.C.; Souza, M.; Do Nascimento, M.A.; Santos, L.; Antunes, M.; Cyrino, E. Resistance Training in Older Women: Comparison of Single Vs. Multiple Sets on Muscle Strength and Body Composition. Isokinet. Exerc. Sci. 2015, 53–60. [Google Scholar] [CrossRef]
- Cunha, P.M.; Ribeiro, A.S.; Nunes, J.P.; Tomeleri, C.M.; Nascimiento, M.A.; Moraes, G.K.; Sugihara, P.; Barbosa, D.; Venturini, D.; Cyrino, E. Resistance training performed with single-set is sufficient to reduce cardiovascular risk factors in untrained older women: The randomized clinical trial. Active Aging Longitudinal Study. Arch. Gerontol. Geriatr. 2019, 81, 171–175. [Google Scholar] [CrossRef]
- Ribeiro, A.S.; Schoenfeld, B.J.; Souza, M.F.; Tomeleri, C.M.; Silva, A.M.; Teixeira, D.C.; Sardinha, L.; Cyrino, E. Resistance training prescription with different load-management methods improves phase angle in older women. Eur. J. Sport Sci. 2017, 17, 913–921. [Google Scholar] [CrossRef]
- de Lima, T.A.; Ferreira-Moraes, R.; Alves, W.M.G.D.C.; Alves, T.G.G.; Pimentel, C.P.; Sousa, E.C.; Abrahin, O.; Cortinhas-Alvees, E.A. Resistance training reduces depressive symptoms in elderly people with Parkinson disease: A controlled randomized study. Scand J. Med. Sci. Sports 2019, 29, 1957–1967. [Google Scholar] [CrossRef]
- Tomeleri, C.M.; Souza, M.F.; Burini, R.C.; Cavaglieri, C.R.; Ribeiro, A.S.; Antunes, M.; Nunes, J.P.; Venturini, D.; Barbosa, D.S.; Sardinha, L.B.; et al. Resistance training reduces metabolic syndrome and inflammatory markers in older women: A randomized controlled trial. J. Diabetes 2018, 10, 328–337. [Google Scholar] [CrossRef]
- Oliveira-Dantas, F.F.; Brasileiro-Santos, M.D.S.; Thomas, S.G.; Silva, A.S.; Silva, D.C.; Browne, R.A.V.; Farias-Junior, L.F.; Costa, E.; da Cruz, A. Short-Term Resistance Training Improves Cardiac Autonomic Modulation and Blood Pressure in Hypertensive Older Women: A Randomized Controlled Trial. J. Strength Cond. Res. 2020, 34, 37–45. [Google Scholar] [CrossRef]
- Lopes, P.B.; Pereira, G.; Lodovico, A.; Bento, P.C.B.; Rodacki, A.L.F. Strength and Power Training Effects on Lower Limb Force, Functional Capacity, and Static and Dynamic Balance in Older Female Adults. Rejuvenation Res. 2016, 19, 385–393. [Google Scholar] [CrossRef]
- Da Silva, P.B.; Antunes, F.N.; Graef, P.; Cechetti, F.; Pagnussat, A.D.S. Strength training associated with task-oriented training to enhance upper-limb motor function in elderly patients with mild impairment after stroke: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2015, 94, 11–19. [Google Scholar] [CrossRef]
- Alves, W.M.; Alves, T.G.; Ferreira, R.M.; De Sousa, E.C.; Pimentel, C.P.; De Lima, T.A.; Abrahin, O.; Alves, E.A. Strength training improves the respiratory muscle strength and quality of life of elderly with Parkinson disease. J. Sports Med. Phys. Fitness 2019, 59, 1756–1762. [Google Scholar] [CrossRef]
- Ferreira, R.M.; Alves, W.M.G.D.C.; de Lima, T.A.; Gibson-Alves, T.G.; Alves-Filho, P.A.; Pimentel, C.P.; Correa, E.; Cortinhas-Alves, E.A. The effect of resistance training on the anxiety symptoms and quality of life in elderly people with Parkinson’s disease: A randomized controlled trial. Arq. Neuropsiquiatr. 2018, 76, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Rosa, C.; Vilaga-Alves, J.; Neves, E.B.; Saavedra, F.J.F.; Reckziegel, M.B.; Pohl, H.H.; Zanini, D.; Machado, V. The effect of weekly low frequency exercise on body composition and blood pressure of elderly women. Arch. Med. Deporte 2017, 34, 9–14. [Google Scholar]
- Rodacki, A.L.F.; Cepeda, C.P.C.; Lodovico, A.; Ugrinowitsch, C. The Effects of a Dance-Based Program on the Postural Control in Older Women. Top. Geriatr. Rehabil. 2017, 33, 244–249. [Google Scholar] [CrossRef]
- Aragão-Santos, J.C.; De Resende-Neto, A.G.; Nogueira, A.C.; Feitosa-Neta, M.L.; Brandao, L.H.; Chaves, L.M.; Da Silva-Grigoletto, M.E. The effects of functional and traditional strength training on different strength parameters of elderly women: A randomized and controlled trial. J. Sports Med. Phys. Fitness 2019, 59, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Ferraz, D.D.; Trippo, K.V.; Duarte, G.P.; Neto, M.G.; Bernardes-Santos, K.O.; Filho, J.O. The Effects of Functional Training, Bicycle Exercise, and Exergaming on Walking Capacity of Elderly Patients with Parkinson Disease: A Pilot Randomized Controlled Single-blinded Trial. Arch. Phys. Med. Rehabil. 2018, 99, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Sbardelotto, M.L.; Pedroso, G.S.; Pereira, F.T.; Soratto, H.R.; Brescianini, S.M.; Effting, P.S.; Thirupathi, A.; Nesi, R.T.; Silveira, P.CL.; Pinho, R.A. The effects of physical training are varied and occur in an exercise type-dependent manner in elderly men. Aging Dis. 2017, 8, 887–898. [Google Scholar] [CrossRef] [Green Version]
- Antunes, H.K.; Santos-Galduroz, R.F.; De Aquino-Lemos, V.; Amodeu-Bueno, O.F.; Rzezak, P.; Goncalves-De Santana, M.; De Melo, M.T. The influence of physical exercise and leisure activity on neuropsychological functioning in older adults. Age (Dordr) 2015, 37, 9815. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, I.F.D.; Leme, G.L.M.; Scheicher, M.E. The Influence of Video Game Training with and without Subpatelar Bandage in Mobility and Gait Speed on Elderly Female Fallers. J. Aging Res. 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Barbalho, M.S.M.; Gentil, P.; Izquierdo, M.; Fisher, J.; Steele, J.; Raiol, R.A. There are no no-responders to low or high resistance training volumes among older women. Exp. Gerontol. 2017, 99, 18–26. [Google Scholar] [CrossRef]
- de Oliveira Silva, F.; Ferreira, J.V.; Plácido, J.; Sant’Anna, P.; Araújo, J.; Marinho, V.; Laks, J.; Deslandes, A.C. Three months of multimodal training contributes to mobility and executive function in elderly individuals with mild cognitive impairment, but not in those with Alzheimer’s disease: A randomized controlled trial. Maturitas 2019, 126, 28–33. [Google Scholar] [CrossRef]
- Lixandrão, M.E.; Damas, F.; Chacon-Mikahil, M.P.; Cavaglieri, C.R.; Ugrinowitsch, C.; Bottaro, M.; Vechin, F.C.; Conceicao, R.B.; Libardi, C.A. Time Course of Resistance Training-Induced Muscle Hypertrophy in the Elderly. J. Strength Cond. Res. 2016, 30, 159–163. [Google Scholar]
- Ribeiro, A.S.; Schoenfeld, B.J.; Souza, M.F.; Tomeleri, C.M.; Venturini, D.; Barbosa, D.S.; Cyrino, E.S. Traditional and pyramidal resistance training systems improve muscle quality and metabolic biomarkers in older women: A randomized crossover study. Exp. Gerontol. 2016, 79, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Da Silveira Fontenele De Meneses, Y.P.; Cabral, P.U.L.; Orsano, F.E.; Da Silveira, C.M.L. Vascular function and nitrite levels in elderly women before and after hydrogymnastics exercises. J. Phys. Educ. 2019, 30. [Google Scholar] [CrossRef] [Green Version]
- Monteiro-Junior, R.S.; Figueiredo, L.F.D.S.; Maciel-Pinheiro, P.T.; Abud, E.L.R.; Engedal, K.; Barca, M.L.; Nascimento, O.J.M.; Laks, J.; Deslandes, A.C. Virtual Reality-Based Physical Exercise With Exergames (PhysEx) Improves Mental and Physical Health of Institutionalized Older Adults. J. Am. Med. Dir. Assoc. 2017, 18, 454. [Google Scholar] [CrossRef]
- Aveiro, M.C.; Avila, M.A.; Pereira-Baldon, V.S.; Ceccatto-Oliveira, A.S.B.; Gramani-Say, K.; Oishi, J.; Driusso, P. Water- versus land-based treatment for postural control in postmenopausal osteoporotic women: A randomized, controlled trial. Climacteric 2017, 20, 427–435. [Google Scholar] [CrossRef]
- Silva, M.R.; Alberton, C.L.; Portella, E.G.; Nunes, G.N.; Martin, D.G.; Pinto, S.S. Water-based aerobic and combined training in elderly women: Effects on functional capacity and quality of life. Exp. Gerontol. 2018, 106, 54–60. [Google Scholar] [CrossRef]
- De Oliveira, V.H.; Câmara, G.L.G.; Azevedo, K.P.M.; Neto, E.C.A.; Dos Santos, I.K.; Medeiros, H.J.; Knackfuss, M.I. Weight training program with imposed and self-selected intensity on body composition in elderly: A randomized clinical trial. Rev. Andaluza. Med. Deporte 2019, 12, 11–14. [Google Scholar]
- Simao, A.P.; Mendonca, V.A.; Avelar, N.C.P.; Fonseca, S.F.D.; Santos, J.M.; Oliveira, A.C.C.; Tossige-Gomes, R.; Ribeiro, V.G.C.; Cunha, C.D.; Balthazar, C.E.; et al. Whole body vibration training on muscle strength and brain-derived neurotrophic factor levels in elderly woman with knee osteoarthritis: A randomized clinical trial study. Front. Physiol. 2019, 10, 756. [Google Scholar] [CrossRef] [PubMed]
- Grupo Banco Mundial. Población Mundial Total. Washington, DC, USA. 2019 [04 de agosto de 2020]. Available online: https://www.bancomundial.org/ (accessed on 20 February 2021).
- Carvajal-Tapia, A.; Carvajal-Rodríguez, E. Producción científica en ciencias de la salud en los países de América Latina, 2006 2015: Análisis a partir de SciELO. Rev. Interam. Bibl. 2019, 42, 15–21. [Google Scholar] [CrossRef]
- Organización de las Naciones Unidas para la Educación, la Ciencia y la Cultura (UNESCO). Informe de la UNESCO para la ciencia hacia 2030: Panorámica de América Latina y el Caribe; Ediciones UNESCO: París, Francia, 2015. [Google Scholar]
- Sallis, J.; Bull, F.; Guthold, R.; Heath, G.W.; Inoue, S.; Kelly, P.; Oyeyemi, A.L.; Perez, L.G.; Richards, J.; Hallal, P.C.; et al. Progress in physical activity over the Olympic quadrennium. Lancet 2016, 388, 1325–1336. [Google Scholar] [CrossRef]
- Organización Mundial de la Salud. Informe Mundial Sobre el Envejecimiento y la Salud; Ginebra, OMS: Ginebra, Suiza, 2015. [Google Scholar]
- Peranovich, A. Enfermedades crónicas y factores de riesgo en adultos mayores de Argentina: Años 2001–2009. Saúde Debate 2016, 40, 125–135. [Google Scholar] [CrossRef] [Green Version]
- Hay–Smith, E.J.; Englas, K.; Dumoulin, Ch.; Ferreira, C.H.; Frawley, H.; Weatherall, M. The Consensus on Exercise Reporting Template (CERT) in a systematic review of exercise-based rehabilitation effectiveness: Completeness of reporting, rater agreement, and utility. Eur. J. Phys. Rehabil. Med. 2019, 55, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Roller, M.; Kachingwe, A.; Beling, J.; Ickes, D.M.; Cabot, A.; Shrier, G. Pilates Reformer exercises for fall risk reduction in older adults: A randomized controlled trial. J. Bodyw. Mov. Ther. 2018, 22, 983–998. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Li, G.; Wang, X.; Huiru, Y.; Jia, Y.; Leng, M.; Li, H.; Chen, L. Effect of exergames on physical outcomes in frail elderly: A systematic review [published online ahead of print, 2019 Sep 13]. Aging Clin. Exp. Res. 2019. [Google Scholar] [CrossRef]
- Pacheco, T.B.F.; de Medeiros, C.S.P.; de Oliveira, V.H.B.; Vieira, E.R.; de Cavalcanti, F.A.C. Effectiveness of exergames for improving mobility and balance in older adults: A systematic review and meta-analysis. Syst. Rev. 2020, 9, 163. [Google Scholar] [CrossRef]
- Waller, B.; Ogonowska-Słodownik, A.; Vitor, M.; Rodionova, K.; Lambeck, J.; Heinonen, A.; Daly, D. The effect of aquatic exercise on physical functioning in the older adult: A systematic review with meta-analysis. Age Ageing 2016, 45, 593–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, C.C.; Tu, Y.K.; Wang, T.G.; Huang, Y.T.; Chien, K.L. Effects of resistance training, endurance training and whole-body vibration on lean body mass, muscle strength and physical performance in older people: A systematic review and network meta-analysis. Age Ageing 2018, 47, 367–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboutorabi, A.; Arazpour, M.; Bahramizadeh, M.; Farahmand, F.; Fadayevatan, R. Effect of vibration on postural control and gait of elderly subjects: A systematic review. Aging Clin. Exp. Res. 2018, 30, 713–726. [Google Scholar] [CrossRef]
- Jepsen, D.B.; Thomsen, K.; Hansen, S.; Jørgensen, N.R.; Masud, T.; Ryg, J. Effect of whole-body vibration exercise in preventing falls and fractures: A systematic review and meta-analysis. BMJ Open 2017, 7, e018342. [Google Scholar] [CrossRef]
- Rogan, S.; de Bruin, E.D.; Radlinger, L.; Joehr, C.; Wyss, C.; Stuck, N.J.; Bruelhart, Y.; de Bie, R.A.; Hilfiker, R. Effects of whole-body vibration on proxies of muscle strength in old adults: A systematic review and meta-analysis on the role of physical capacity level. Eur. Rev. Aging Phys. Act 2015, 12, 12. [Google Scholar] [CrossRef] [Green Version]
- Hart, P.D.; Buck, D.J. The effect of resistance training on health-related quality of life in older adults: Systematic review and meta-analysis. Health Promot. Perspect. 2019, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bouaziz, W.; Vogel, T.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Lang, P.O. Health benefits of aerobic training programs in adults aged 70 and over: A systematic review. Arch. Gerontol. Geriatr. 2017, 69, 110–127. [Google Scholar] [CrossRef]
- Lopez, P.; Pinto, R.S.; Radaelli, R.; Rech, A.; Grazioli, R.; Izquierdo, M.; Cadore, E.L. Benefits of resistance training in physically frail elderly: A systematic review. Aging Clin. Exp. Res. 2018, 30, 889–899. [Google Scholar] [CrossRef]
- Guizelini, P.C.; de Aguiar, R.A.; Denadai, B.S.; Caputo, F.; Greco, C.C. Effect of resistance training on muscle strength and rate of force development in healthy older adults: A systematic review and meta-analysis. Exp. Gerontol. 2018, 102, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Hollings, M.; Mavros, Y.; Freeston, J.; Fiatarone-Singh, M. The effect of progressive resistance training on aerobic fitness and strength in adults with coronary heart disease: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Prev. Cardiol. 2017, 24, 1242–1259. [Google Scholar] [CrossRef]
- Galloza, J.; Castillo, B.; Micheo, W. Benefits of Exercise in the Older Population. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 659–669. [Google Scholar] [CrossRef]
- Jadczak, A.D.; Makwana, N.; Luscombe-Marsh, N.; Visvanathan, R.; Schultz, T.J. Effectiveness of exercise interventions on physical function in community-dwelling frail older people: An umbrella review of systematic reviews. JBI Database Syst. Rev. Implement Rep. 2018, 16, 752–775. [Google Scholar] [CrossRef]
- Abdullah-Alfadhel, S.A.; Vennu, V.; Alotaibi, A.D.; Algarni, A.M.; Saad-Bindawas, S.M. The effect of a multicomponent exercise programme onelderly adults’ risk of falling in nursing homes: A systematic review. J. Pak. Med. Assoc. 2020, 70, 699–704. [Google Scholar]
- Izquierdo, M.; Casas, A.; Zambom, F.; Martínez, N.; Alonso, C.; Rodriguez, L.; VIVIFRAIL. Guía Práctica Para la Prescripción de un Programa de Entrenamiento Físico Multicomponente Para la Prevención de la Fragilidad y Caídas en Mayores de 70 años. Navarra, España. 2017. Available online: http://vivifrail.com/es/inicio/ (accessed on 24 July 2020).
- Li, S.Y.H.; Bressington, D. The effects of mindfulness-based stress reduction on depression, anxiety, and stress in older adults: A systematic review and meta-analysis. Int. J. Ment. Health Nurs. 2019, 28, 635–656. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Cabello, A.; Vila-Maldonado, S.; Pedrero-Chamizo, R.; Villa-Vicente, J.G.; Gusi, G.; Espino, L.; González, M.; Casajus, J.; Ara, I. La actividad física organizada en las personas mayores, una herramienta para mejorar la condición física en la senectud. Rev. Esp. Salud Pública 2018, 92, e201803013. [Google Scholar]
- Kruisselbrink, L.D.; Dodge, A.M.; Swanburg, S.L.; & MacLeod, A.L. Influence of Same-Sex and Mixed-Sex Exercise Settings on the Social Physique Anxiety and Exercise Intentions of Males and Females. J. Sport Exerc. Psychol. 2004, 26, 616–622. [Google Scholar] [CrossRef]
- Rodríguez, E.; Ara, I.; Mata, E.A.; Aguado, X. Jump and balance performance in an active young and elderly Spanish population. Apunts Med. Esport 2012, 47. [Google Scholar]
- Claros, J.; Cruz, M.V.; Beltrán, Y. Effects of physical exercise on functional fitness and stability in older adults. Rev. Hacia. Promoción Salud 2012, 17, 79–90. [Google Scholar]
- Zech, A.; Hübscher, M.; Vogt, L.; Banzer, W.; Hänsel, F.; Pfeifer, K. Balance Trainning for Neuromuscular Control and Performance Enhancement: A systematic Review. J. Athl. Train. 2010, 45, 392–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bize, R.; Johnson, J.A.; Plotnikoff, R.C. Physical activity level and health-related quality of life in the general adult population: A systematic review. Prev. Med. 2007, 45, 401–415. [Google Scholar] [CrossRef]
- Anokye, N.K.; Trueman, P.; Green, C.; Pavey, T.G.; Taylor, R.S. Physical activity and health related quality of life. BMC Public Health 2012, 12, 624. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criterion | Description |
|---|---|
|
|
|
|
|
|
|
|
|
|
| Ref. | Authors (Year) Country | Initial/Final Sample | Percentage that Ended the Study (%) | Withdrawal | Age Range | Sex | Health | Recruitment | Place of Intervention | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reason | (Years) | ♀ | ♂ | Condition | ||||||||||||||||||
| AT | PR | NMC | NS | 60–70 | 71–80 | 80 o+ | (%) | (%) | CD | NDD | CMD | CA | COM | HC | INST | HC | SC | UC | ||||
| [40] | Queiroz J. (2016) Brazil | 62/62 | 100 | 1 | 1 | 0 | 100 | - | - | - | - | 1 | ||||||||||
| [41] | Antunes A. (2015) Brazil | 45/45 | 100 | 1 | 1 | 0 | 100 | - | - | - | - | 1 | ||||||||||
| [42] | Santos S. (2017) Brazil | 40/26 | 65 | 1 | 1 | 1 | 1 | 31 | 69 | 1 | 1 | 1 | ||||||||||
| [43] | de Oliveira R. (2017) Brazil | 24/23 | 96 | 1 | 1 | 1 | 1 | 56 | 44 | 1 | 1 | 1 | ||||||||||
| [44] | Campos L. (2016) Brazil | 32/32 | 100 | 1 | 100 | - | - | - | - | 1 | 1 | 1 | ||||||||||
| [45] | Mazinifilho M. (2017) Brazil | 79/79 | 100 | 1 | 1 | 100 | 1 | |||||||||||||||
| [46] | Teodoro J. (2019) Brazil | 36/36 | 100 | 1 | 1 | 100 | - | - | - | - | 1 | |||||||||||
| [47] | Santos G. (2019) Brazil | 34/18 | 53 | 1 | 1 | 1 | 100 | - | 1 | 1 | ||||||||||||
| [48] | Dueñas E. (2019) Colombia | 125/105 | 84 | 1 | 1 | 1 | 1 | 1 | 84 | 16 | 1 | 1 | 1 | 1 | ||||||||
| [49] | Torres A. (2019) Brazil | 64/56 | 88 | 1 | 1 | 1 | 91 | 9 | 1 | |||||||||||||
| [50] | Arantes P. (2015) Brazil | 30/28 | 93 | 1 | 1 | 1 | 1 | 100 | - | 1 | ||||||||||||
| [51] | Lima L. (2015) Brazil | 44/44 | 100 | 1 | 1 | 84 | 16 | - | 1 | 1 | ||||||||||||
| [52] | de Oliveira D. (2019) Brazil | 24/19 | 79 | 1 | 1 | 1 | 100 | |||||||||||||||
| [53] | da Silveira Ch. (2019) Brazil | 60/52 | 87 | 1 | 1 | 1 | 1 | 1 | 77 | 23 | 1 | 1 | 1 | |||||||||
| [54] | do Nascimento M. (2019) Brazil | 62/45 | 72 | 1 | 1 | 1 | 1 | 100 | 0 | 1 | ||||||||||||
| [55] | Oliveira F. (2016) Brazil | 25/25 | 100 | 1 | 1 | 1 | 1 | |||||||||||||||
| [56] | Galvao M. (2019) Brazil | 30/24 | 80 | 1 | 1 | 1 | 1 | 100 | 1 | 1 | ||||||||||||
| [57] | Carvalo R. (2018) Brazil | 22/21 | 95 | 1 | 1 | 1 | 75 | 25 | - | 1 | 1 | |||||||||||
| [58] | Tiggemann C. (2016) Brazil | 30/25 | 83 | 1 | 1 | 1 | 1 | 1 | 100 | 1 | ||||||||||||
| [59] | da Silva R. (2017) Brazil | 30/30 | 100 | 1 | 1 | 100 | 1 | 1 | ||||||||||||||
| [60] | Taglietti M. (2018) Brazil | 60/49 | 81 | 1 | 1 | 1 | 1 | 68 | 32 | 1 | 1 | 1 | ||||||||||
| [61] | Franco M. (2016) Brazil | 82/71 | 87 | 1 | 1 | 1 | 1 | 93 | 7 | - | 1 | 1 | ||||||||||
| [62] | Batisti C. (2018) Brazil | 45/37 | 82 | 1 | 1 | 1 | 1 | NS | NS | 1 | 1 | |||||||||||
| [63] | Lopez N. (2015) Chile | 80/60 | 75 | 1 | 1 | 1 | 1 | 1 | 68 | 32 | 1 | 1 | 1 | |||||||||
| [64] | Shiguemitsu F. (2018) Brazil | 37/31 | 84 | 1 | 100 | 1 | ||||||||||||||||
| [65] | Ortiz-Ortiz M. (2019) Mexico | 50/50 | 100 | 1 | 1 | 1 | 60 | 40 | 1 | 1 | ||||||||||||
| [66] | Mansur J. (2016) Brazil | 35/35 | 100 | 1 | 1 | 100 | 0 | - | 1 | |||||||||||||
| [67] | Clemente A. (2018) Brazil | 41/35 | 86 | 1 | 1 | 1 | 1 | 66 | 34 | 1 | 1 | 1 | ||||||||||
| [68] | Rodrigues-Krause J. (2018) Brazil | 30/27 | 87 | 1 | 1 | 100 | 1 | - | 1 | 1 | ||||||||||||
| [69] | Ferrari R. (2016) Brazil | 24/23 | 96 | 1 | 1 | 1 | 100 | - | - | - | - | |||||||||||
| [70] | Ramirez-Campillo R. (2016) Chile | 24/24 | 100 | 1 | 1 | 1 | 100 | 0 | 1 | 1 | ||||||||||||
| [71] | de Resende A. (2018) Brazil | 32/32 | 100 | 1 | 1 | 100 | - | - | - | 1 | ||||||||||||
| [72] | Cavalcante E. (2018) Brazil | 63/57 | 91 | 1 | 1 | 1 | 100 | 1 | 1 | |||||||||||||
| [73] | Pieta C. (2015) Brazil | 26/19 | 73 | 1 | 1 | 1 | 100 | 0 | ||||||||||||||
| [74] | Henrique P. (2019) Brazil | 31/31 | 100 | 1 | 1 | 1 | 55 | 45 | 1 | 1 | 1 | |||||||||||
| [75] | Ramírez-Villada J. (2019) Colombia | 60/47 | 79 | 1 | 1 | 100 | 1 | 1 | ||||||||||||||
| [76] | Gomes A. (2019) Brazil | 47/47 | 100 | 1 | 1 | 100 | - | |||||||||||||||
| [77] | Feitosa N. (2016) Brazil | 30/23 | 77 | 1 | 1 | 100 | 1 | |||||||||||||||
| [78] | Ribeiro J. (2018) Brazil | 50/46 | 92 | 1 | 1 | 1 | 74 | 26 | 1 | 1 | ||||||||||||
| [79] | dos Santos L. (2018) Brazil | 39/39 | 100 | 1 | 1 | 100 | - | 1 | ||||||||||||||
| [80] | Gomeñuka N. (2019) Brazil | 33/26 | 79 | 1 | 1 | 1 | 1 | 73 | 27 | 1 | 1 | 1 | ||||||||||
| [81] | Campos L. (2015) Brazil | 32/32 | 100 | 1 | NS | NS | - | 1 | 1 | |||||||||||||
| [82] | de Souza R. (2018) Brazil | 42/27 | 64 | 1 | 1 | 1 | 1 | 100 | 1 | |||||||||||||
| [83] | Macedo L. (2018) Brazil | 23/19 | 83 | 1 | 1 | 1 | 1 | 100 | 1 | 1 | ||||||||||||
| [84] | Botton C. (2018) Brazil | 44/26 | 59 | 1 | 1 | 1 | 1 | 41 | 59 | 1 | 1 | 1 | 1 | |||||||||
| [85] | Bonadias. A. (2016) Brazil | 133/133 | 100 | 1 | 1 | 100 | 1 | 1 | 1 | 1 | 1 | |||||||||||
| [86] | Barbosa A. (2015) Brazil | 30/30 | 100 | 1 | 1 | 100 | 1 | 1 | ||||||||||||||
| [87] | Rodrigues W. (2015) Brazil | 47/40 | 85 | 1 | 1 | 1 | 70 | 30 | - | - | - | - | 1 | 1 | 1 | |||||||
| [88] | Gallo L. (2015) Brazil | 31/26 | 84 | 1 | 1 | 1 | 100 | 1 | 1 | |||||||||||||
| [89] | Ruaro M. (2019) Brazil | 40/33 | 83 | 1 | 1 | 1 | 1 | 100 | 1 | |||||||||||||
| [90] | Da silva C. (2018) Brazil | 58/51 | 88 | 1 | 1 | 1 | 59 | 41 | 1 | 1 | 1 | |||||||||||
| [91] | Mirando A. (2020) Chile | 21/12 | 57 | 1 | 1 | 86 | 14 | - | 1 | |||||||||||||
| [92] | Cadore E. (2018) Brazil | 65/52 | 80 | 1 | 1 | 1 | 100 | - | - | - | - | 1 | ||||||||||
| [93] | de Resende A. (2016) Brazil | 55/44 | 80 | 1 | 1 | 1 | 100 | 1 | ||||||||||||||
| [94] | Silva I. (2018) Brazil | 48/43 | 90 | 1 | 1 | 1 | 39 | 61 | 1 | |||||||||||||
| [95] | Rabelo M. (2019) Brazil | 39/39 | 100 | 1 | 1 | 74 | 26 | 1 | 1 | |||||||||||||
| [96] | Ramirez-Campillo R. (2018) Chile | 74/52 | 70 | 1 | 1 | 1 | 100 | - | - | - | ||||||||||||
| [97] | Brandao G. (2018) Brazil | 131/125 | 95 | 1 | 1 | 1 | 88 | 12 | 1 | 1 | ||||||||||||
| [98] | Lopez J. (2017) Mexico | 31/26 | 84 | 1 | 1 | 1 | 100 | - | - | 1 | 1 | |||||||||||
| [99] | Medeiros L. (2018) Brazil | 78/71 | 91 | 1 | 1 | 1 | 77 | 23 | - | 1 | ||||||||||||
| [100] | Vargas M. (2019) Ecuador | 50/50 | 100 | 1 | 30 | 70 | 1 | 1 | ||||||||||||||
| [101] | Covolo-Scarabottolo C. (2017) Brazil | 35/30 | 86 | 1 | 1 | 1 | 1 | 53 | 47 | 1 | 1 | |||||||||||
| [102] | Damorim I. (2017) Brazil | 64/55 | 86 | 1 | 1 | 1 | 71 | 29 | 1 | 1 | ||||||||||||
| [103] | Leal L. (2019) Brazil | 54/54 | 100 | 1 | 50 | 50 | 1 | 1 | ||||||||||||||
| [104] | Souza D. (2019) Brazil | 25/21 | 84 | 1 | 1 | 1 | 100 | - | - | - | - | 1 | ||||||||||
| [105] | Santos G. (2015) Brazil | 70/62 | 86 | 1 | 1 | 1 | 1 | 60 | 40 | 1 | 1 | 1 | ||||||||||
| [106] | Moreira N. (2018) Brazil | 46/45 | 98 | 1 | 1 | 1 | 100 | - | - | - | - | 1 | ||||||||||
| [107] | Martinez A. (2018) Chile | 33/33 | 100 | 1 | 1 | 1 | 39 | 61 | 1 | |||||||||||||
| [108] | Santana M. (2016) Brazil | 23/16 | 70 | 1 | 1 | 1 | 1 | 87 | 13 | 1 | ||||||||||||
| [109] | Gomeñuka N. (2020) Brazil | 33/26 | 79 | 1 | 1 | 1 | 72 | 28 | 1 | 1 | ||||||||||||
| [110] | Coelho-Júnior H. (2019) Brazil | 45/36 | 80 | 1 | 1 | 1 | 100 | - | - | - | 1 | |||||||||||
| [111] | Silva M. (2016) Brazil | 78/45 | 58 | 1 | 1 | 1 | 1 | 82 | 18 | |||||||||||||
| [112] | Gambassi B. (2015) Brazil | 17/16 | 94 | 1 | 1 | 100 | 1 | |||||||||||||||
| [113] | Tomeleri C. (2016) Brazil | 38/35 | 92 | 1 | 1 | 1 | 100 | 1 | 1 | |||||||||||||
| [114] | Alex S. (2015) Brazil | 30/30 | 100 | 1 | 1 | 100 | - | 1 | 1 | |||||||||||||
| [115] | Cunha P. (2019) Brazil | 48/48 | 100 | 1 | 1 | 100 | - | |||||||||||||||
| [116] | Ribeiro. S. (2017) Brazil | 76/68 | 89 | 1 | 1 | 1 | 100 | 1 | 1 | |||||||||||||
| [117] | Alcantar T. (2019) Brazil | 33/33 | 100 | 1 | 1 | NS | NS | 1 | 1 | |||||||||||||
| [118] | Tomeleri M. (2018) Brazil | 53/45 | 85 | 1 | 1 | 1 | 100 | - | ||||||||||||||
| [119] | Oliveira-Dantas F. (2020) Brazil | 25/25 | 100 | 1 | 1 | 100 | 1 | 1 | ||||||||||||||
| [120] | Lopez P. (2016) Brazil | 55/37 | 67 | 1 | 1 | 1 | 100 | - | - | 1 | ||||||||||||
| [121] | da Silva P. (2015) Brazil | 20/20 | 100 | 1 | 1 | 65 | 35 | 1 | 1 | |||||||||||||
| [122] | Alves W. (2019) Brazil | 32/28 | 88 | 1 | 1 | 1 | 50 | 50 | 1 | 1 | ||||||||||||
| [123] | Morales F. (2018) Brazil | 35/35 | 100 | 1 | NS | NS | 1 | 1 | 1 | |||||||||||||
| [124] | Rosa C. (2017) Brazil | 92/55 | 60 | 1 | 1 | 1 | 1 | 1 | 100 | 1 | ||||||||||||
| [125] | Rodacki A. (2017) Brazil | 38/30 | 79 | 1 | 1 | 1 | 100 | 1 | ||||||||||||||
| [126] | Aragao-Santos J. (2019) Brazil | 44/44 | 100 | 1 | 1 | 100 | ||||||||||||||||
| [127] | Dominguez D. (2018) Brazil | 72/62 | 86 | 1 | 1 | 1 | 1 | 40 | 60 | 1 | 1 | 1 | ||||||||||
| [128] | Sbardelotto M. (2017) Brazil | 55/55 | 100 | 1 | 1 | 100 | 1 | |||||||||||||||
| [129] | Moreira H. (2015) Brazil | 51/51 | 100 | 1 | 100 | |||||||||||||||||
| [130] | De Carvalho I. (2018) Brazil | 20/20 | 100 | 1 | 1 | 100 | 1 | |||||||||||||||
| [131] | Mendes M. (2017) Brazil | 420/376 | 90 | 1 | 1 | 1 | 100 | - | ||||||||||||||
| [132] | de Oliveira F. (2019) Brazil | 56/46 | 82 | 1 | 1 | 1 | 1 | 1 | 59 | 41 | 1 | 1 | 1 | |||||||||
| [133] | Lixandrao M. (2016) Brazil | 14/14 | 100 | 1 | 1 | 43 | 57 | - | - | |||||||||||||
| [134] | Ribeiro A. (2016) Brazil | 29/25 | 86 | 1 | 1 | 1 | 100 | 1 | 1 | |||||||||||||
| [135] | Silveira Y. (2019) Brazil | 83/40 | 48 | 1 | 1 | 1 | 1 | 100 | 1 | |||||||||||||
| [136] | Monteiro-junior R. (2017) Brazil | 29/11 | 38 | 1 | 1 | 33 | 67 | 1 | 1 | |||||||||||||
| [137] | Chaves M. (2017) Brazil | 36/36 | 100 | 1 | 1 | 100 | 1 | 1 | 1 | |||||||||||||
| [138] | Ribeiro S. (2018) Brazil | 48/33 | 69 | 1 | 1 | 100 | ||||||||||||||||
| [139] | de Oliveira V. (2019) Brazil | 52/43 | 83 | 1 | 1 | NS | NS | 1 | ||||||||||||||
| [140] | Simão A. (2019) Brazil | 15/15 | 100 | 1 | 1 | 1 | 100 | 1 | 1 | |||||||||||||
| Ref. | Authors | Intervention | Intervention | Session | Professional | Type of Intervention | Components and Time of Each Intervention | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Duration | Frequency | Duration | in Charge | (Experimental Group) | WS | CS | AER | STR | FLE | GAI | COO | BAL | PRO | ||||||||
| (Month) | (Sessions/Week) | (min) | HP | QP | NS | PEI | HI | NTI | DSI | IC | min | min | min | min | min | min | min | ||||
| [40] | Queiroz J. | 3 | 2 | 90 | 1 | EG | 1 | 1 | |||||||||||||
| [41] | Antunes A. | 6 | 3 | 20–60 | 1 | EG | 20–60 | NS | |||||||||||||
| [42] | Santos S. | 2 | 2 | 60 | 1 | EG1 | NS | NS | NS | NS | |||||||||||
| EG2 | NS | NS | |||||||||||||||||||
| [43] | de Oliveira R. | 6 | 2 | 60 | 1 | EG1 | 1 | 1 | NS | NS | NS | NS | |||||||||
| EG2 | 1 | 1 | 50 | ||||||||||||||||||
| [44] | Campos L. | 3 | 2 | 60 | 1 | EG1 | |||||||||||||||
| EG2 | 1 | 60 | |||||||||||||||||||
| [45] | Mazinifilho M. | 3 | 3 | 50/50 | 1 | EG1 | 1 | 1 | 15 | 15 | |||||||||||
| EG2 | 1 | 1 | 20 | 20 | |||||||||||||||||
| [46] | Teodoro J. | 5 | 2 | 65–85 | 1 | EG1 | 1 | 20–35 | 40 | ||||||||||||
| EG2 | 1 | 20–35 | 40 | ||||||||||||||||||
| EG3 | 1 | 20–35 | 40 | ||||||||||||||||||
| [47] | Santos G. | 3 | 3 | 40 | 1 | EG1 | 1 | 1 | NS | 20 | NS | ||||||||||
| EG2 | 1 | 1 | 10* | 20 | 10* | ||||||||||||||||
| EG3 | 1 | 1 | 10* | 20 | 10* | ||||||||||||||||
| [48] | Dueñas E. | 2 | 1 | 60 | 1 | EG1 | NS | NS | NS | ||||||||||||
| EG2 | |||||||||||||||||||||
| EG3 | |||||||||||||||||||||
| [49] | Torres A. | 6 | 3 | 1 | EG1 | NS | |||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [50] | Arantes P. | 3 | 2 | 60 | 1 | EG | 60 | ||||||||||||||
| [51] | Lima L. | 2.5 | 3 | NS | 1 | EG1 | 1 | 1 | 30 | ||||||||||||
| EG2 | 1 | 1 | 30 | NS | |||||||||||||||||
| [52] | de Oliveira D. | 3.5 | 40 | 1 | EG | 1 | 1 | NS | NS | NS | |||||||||||
| [53] | da Silveira Ch. | 6 | 2 | 60 | 1 | EG | 1 | 20–30 | NS | ||||||||||||
| [54] | do Nascimento M. | 3 | 2,/3 | 1 | EG1 | NS | |||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [55] | Oliveira F. | 2.5 | 2,−3 | 1 | EG | NS | |||||||||||||||
| [56] | Galvao M. | 2 | 3 | 60 | 1 | EG1 | 30 | 30 | |||||||||||||
| EG2 | 30 | 30 | |||||||||||||||||||
| EG3 | 30 | 30 | |||||||||||||||||||
| [57] | Carvalo R. | 2 | 2 | 100 | 1 | EG | NS | NS | NS | NS | |||||||||||
| [58] | Tiggemann C. | 3 | 2 | 1 | EG1 | NS | |||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [59] | da Silva R. | 6 | 2,/3 | 1 | EG1 | NS | |||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [60] | Taglietti M. | 2 | 2 | 60 | 1 | EG | 1 | 1 | 20 | 15 | 10 | ||||||||||
| [61] | Franco M. | 3 | 2 | 60 | 1 | EG | |||||||||||||||
| [62] | Batisti C. | 3 | 3 | 40 | 1 | EG | 10,−20 | 15–30 | 10 | 10 | 10 | ||||||||||
| [63] | Lopez N. | 6 | 5 | 60 | 1 | EG | 1 | 40 | 10 | ||||||||||||
| [64] | Shiguemitsu F. | 14 | 2 | 75 | 1 | EG | 1 | NS | NS | NS | NS | NS | |||||||||
| [65] | Ortiz-Ortiz M. | 3 | 5 | 40–50 | 1 | EG | 1 | 1 | NS | NS | NS | NS | |||||||||
| [66] | Mansur J. | 2 | 2 | 30 | 1 | EG1 | 15–30 | 30 | |||||||||||||
| EG2 | 45 | ||||||||||||||||||||
| EG3 | 45 | ||||||||||||||||||||
| [67] | Clemente A. | 6 | 2 | 90 | 1 | EG | 1 | 35 | 50 | ||||||||||||
| [68] | Rodrigues-Krause J. | 2 | 3 | 60 | 1 | EG1 | |||||||||||||||
| EG2 | 1 | 1 | 40 | ||||||||||||||||||
| [69] | Ferrari R. | 2.5 | 2,/3 | 1 | EG1 | 30 | NS | ||||||||||||||
| EG2 | 30 | NS | |||||||||||||||||||
| [70] | Ramirez-Campillo R. | 3 | 2,/3 | 60 | 1 | EG1 | 1 | NS | |||||||||||||
| EG2 | 1 | NS | |||||||||||||||||||
| [71] | de Resende A. | 2 | 3 | 60 | 1 | EG1 | 1 | 30 | NS | NS | |||||||||||
| EG2 | 1 | 15 | 30 | 15 | |||||||||||||||||
| [72] | Cavalcante E. | 3 | 2,/3 | 30 | 1 | EG1 | 1 | NS | |||||||||||||
| EG2 | 1 | NS | |||||||||||||||||||
| [73] | Pieta C. | 3 | 2 | 1 | EG1 | 1 | NS | ||||||||||||||
| EG2 | 1 | NS | |||||||||||||||||||
| [74] | Henrique P. | 3 | 2 | 30 | 1 | EG | |||||||||||||||
| [75] | Ramírez-Villada J. | 8 | 3 | 60 | 1 | EG | NS | NE | NE | ||||||||||||
| [76] | Gomes A. | 2–3 | 3 | 45 | 1 | EG1 | 1 | 15 | 20 | 15 | 15 | ||||||||||
| EG2 | 1 | 15 | 20 | ||||||||||||||||||
| [77] | Feitosa N. | 3 | 3 | 50 | 1 | EG | 1 | NS | 25 | NS | NS | ||||||||||
| [78] | Ribeiro J. | 1.75 | 2 | 60 | 1 | EG1 | |||||||||||||||
| EG2 | 1 | 1 | 10 | 10 | 10 | 10 | 10 | ||||||||||||||
| [79] | dos Santos L. | 2 | 3 | NS | 1 | EG1 | NS | ||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [80] | Gomeñuka N. | 3 | 3 | 30–60 | 1 | EG1 | |||||||||||||||
| EG2 | 1 | 1 | 30–50 | ||||||||||||||||||
| [81] | Campos L. | 3 | 2 | 60 | 1 | EG | |||||||||||||||
| [82] | de Souza R. | 4 | 3 | 60 | 1 | EG | 1 | 1 | 40 | ||||||||||||
| [83] | Macedo L. | 2 | 3 | 50 | 1 | 1 | EG | NS | |||||||||||||
| [84] | Botton C. | 3 | 3 | NS | 1 | EG | 1 | NS | |||||||||||||
| [85] | Bonadias A. | 6 | 3 | NS | 1 | EG | NS | ||||||||||||||
| [86] | Barbosa A. | 2 | 3 | 30 | 1 | EG | 30 | ||||||||||||||
| [87] | Rodrigues W. | 2 | 2 | NS | 1 | 1 | EG | 1 | NS | ||||||||||||
| [88] | Gallo L. | 2 | 3 | 40 | 1 | EG | 40 | ||||||||||||||
| [89] | Ruaro M. F. | 3.5 | 2 | NS | 1 | EG | NS | ||||||||||||||
| [90] | Da silva C. M. | 2 | 3 | 30–60 | 1 | EG | 1 | 1 | 25 | 5–15 | |||||||||||
| [91] | Mirando A. D. | 1.5 | 2 | 60 | 1 | EG | 1 | 1 | NS | NS | |||||||||||
| [92] | Cadore E. | 3 | 2 | NS | 1 | EG1 | NS | NS | |||||||||||||
| EG2 | NS | NS | |||||||||||||||||||
| EG3 | NS | NS | |||||||||||||||||||
| [93] | de resende A. | 3 | 3 | 60 | 1 | EG1 | 25 | 15 | |||||||||||||
| EG2 | 15 | 25 | |||||||||||||||||||
| [94] | Silva I. | 3 | 3 | 60 | 1 | EG1 | NS | NS | |||||||||||||
| EG2 | NS | NS | |||||||||||||||||||
| EG3 | NS | NS | |||||||||||||||||||
| [95] | Rabelo M. | 3 | 3 | 50 | 1 | EG1 | 1 | 25 | 20 | ||||||||||||
| EG2 | |||||||||||||||||||||
| [96] | Ramirez-Campillo R. | 3 | 3 | 60 | 1 | EG1 | 50 | ||||||||||||||
| EG2 | 50 | ||||||||||||||||||||
| [97] | Brandao G. | 3 | 3 | 40 | 1 | EG | 1 | 1 | NS | NS | NS | NS | NS | ||||||||
| [98] | Lopez J. | 3 | 5 | 50 | 1 | EG | 1 | 1 | 30 | NS | |||||||||||
| [99] | Medeiros L. | 3 | 3 | 50 | 1 | EG | 1 | 1 | 10 | NS | 10 | NS | |||||||||
| [100] | Vargas M. | 6 | 3 | 30–60 | 1 | EG | 1 | 1 | 15–40 | ||||||||||||
| [101] | Covolo-Scarabottolo C. | 3 | 2 | 40–50 | 1 | EG | NS | NS | NS | NS | |||||||||||
| [102] | Damorim I. | 4 | 3 | 30 | 1 | EG1 | NS | ||||||||||||||
| EG2 | 30 | ||||||||||||||||||||
| [103] | Leal L. | 6 | 2 | 30–40 | 1 | EG | 30–40 | ||||||||||||||
| [104] | Souza D. | 3.5 | 2 | NS | 1 | EG1 | NS | ||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [105] | Santos G. D. | 3 | 2 | NS | 1 | EG | |||||||||||||||
| [106] | Moreira N. | 4 | 3 | 50 | 1 | EG | 1 | 1 | NS | NS | NS | ||||||||||
| [107] | Martinez A. | 3 | 3 | 63 | 1 | EG | 1 | 1 | NS | ||||||||||||
| [108] | Santana M. | 2 | 3 | 30 | 1 | EG1 | |||||||||||||||
| EG2 | 30 | ||||||||||||||||||||
| [109] | Gomeñuka N. | 2 | 3 | NS | 1 | EG1 | |||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [110] | Coelho-Júnior H. | 4.5 | 2 | 40 | 1 | EG1 | 1 | NS | |||||||||||||
| EG2 | 1 | NS | |||||||||||||||||||
| [111] | Silva M. | 5 | 2 | 60 | 1 | EG | NS | NS | |||||||||||||
| [112] | Gambassi B. | 3 | 2 | NS | 1 | EG | NS | ||||||||||||||
| [113] | Tomeleri C. | 2 | 3 | 45 | 1 | EG | 1 | 45 | |||||||||||||
| [114] | Alex S. | 4.2 | 6 | NS | 1 | EG | 1 | 1 | NS | ||||||||||||
| [115] | Cunha P. | 3 | 3 | 20 | 1 | EG | NS | ||||||||||||||
| [116] | Ribeiro. S. | 2 | 3 | NS | 1 | EG1 | 1 | 1 | NS | ||||||||||||
| EG2 | 1 | 1 | NS | ||||||||||||||||||
| [117] | Alcantar T. | 5 | 2 | 40 | 1 | EG | 1 | 1 | NS | ||||||||||||
| [118] | Tomeleri M. | 3 | 3 | NS | 1 | EG | 1 | 1 | NS | ||||||||||||
| [119] | Oliveira-Dantas F. | 2.5 | 2/3 | NS | 1 | EG | NS | ||||||||||||||
| [120] | Lopez P. | 3 | 3 | 60 | 1 | EG1 | NS | ||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [121] | da Silva P. | 1.5 | 2 | 30 | 1 | EG1 | NS | ||||||||||||||
| G2 | NS | ||||||||||||||||||||
| [122] | Alves W. | 4 | 2 | 30–40 | EG | 1 | 30–35 | ||||||||||||||
| [123] | Morales F. | 6 | 2 | 30–40 | 1 | EG | NS | ||||||||||||||
| [124] | Rosa C. | 6 | 2 | 60 | 1 | G1 | 1 | 1 | 40–45 | 40–45 | |||||||||||
| EG2 | 1 | 1 | 40–45 | 40–45 | |||||||||||||||||
| [125] | Rodacki A. | 2 | 3 | 60 | 1 | EG | 1 | 1 | NS | NS | NS | ||||||||||
| [126] | Aragao-Santos J. | 3 | 3 | 50 | 1 | EG1 | 1 | 1 | 15 | 25 | 15 | 15 | |||||||||
| EG2 | 1 | 1 | 15 | 25 | |||||||||||||||||
| [127] | Dominguez D. | 2 | 3 | 50 | 1 | EG1 | 1 | ||||||||||||||
| EG2 | 1 | NS | |||||||||||||||||||
| EG3 | 1 | NS | NS | NS | NS | ||||||||||||||||
| [128] | Sbardelotto M. | 2 | 3 | 60 | 1 | EG1 | 1 | 1 | 30 | 30 | |||||||||||
| EG2 | 1 | 1 | 15 | 30 | |||||||||||||||||
| EG3 | 1 | 1 | 35 | ||||||||||||||||||
| [129] | Moreira H. | 6 | 3 | 60 | 1 | EG1 | |||||||||||||||
| EG2 | 60 | ||||||||||||||||||||
| [130] | De Carvalho I. | 3 | 2 | 30 | 1 | EG1 | 30 | ||||||||||||||
| EG2 | 30 | ||||||||||||||||||||
| [131] | Mendes M. | 3 | 2 | NE | 1 | EG1 | NS | ||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [132] | de Oliveira F. | 3 | 2 | 60 | 1 | EG | 1 | 1 | 20 | 20 | |||||||||||
| [133] | Lixandrao M. | 2.5 | 2 | NS | 1 | G | 1 | NS | |||||||||||||
| [134] | Ribeiro A. | 9 | 3 | NS | 1 | G1 | 1 | NS | |||||||||||||
| G2 | 1 | NS | |||||||||||||||||||
| [135] | Silveira Y. | 4 | 3 | 50 | 1 | EG | 1 | 1 | 15 | 25 | |||||||||||
| [136] | Monteiro-junior R. | 2 | 2 | 30–45 | 1 | EG | NS | NS | |||||||||||||
| [137] | Chaves M. | 3 | 2 | 45 | 1 | EG1 | NS | ||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [138] | Ribeiro S. | 3 | 2 | NS | 1 | EG1 | NS | NS | |||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [139] | de Oliveira V. | 4 | 2 | NS | 1 | EG1 | NS | ||||||||||||||
| EG2 | NS | ||||||||||||||||||||
| [140] | Simão A. | 3 | 3 | NS | 1 | EG1 | 1 | NS | NS | ||||||||||||
| EG2 | 1 | NS | NS | ||||||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vásquez-Araneda, E.; Solís-Vivanco, R.I.; Mahecha-Matsudo, S.; Zapata-Lamana, R.; Cigarroa, I. Characteristics of Physical Exercise Programs for Older Adults in Latin America: A Systematic Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 2812. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062812
Vásquez-Araneda E, Solís-Vivanco RI, Mahecha-Matsudo S, Zapata-Lamana R, Cigarroa I. Characteristics of Physical Exercise Programs for Older Adults in Latin America: A Systematic Review of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2021; 18(6):2812. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062812
Chicago/Turabian StyleVásquez-Araneda, Eduardo, Rodrigo Ignacio Solís-Vivanco, Sandra Mahecha-Matsudo, Rafael Zapata-Lamana, and Igor Cigarroa. 2021. "Characteristics of Physical Exercise Programs for Older Adults in Latin America: A Systematic Review of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 18, no. 6: 2812. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062812