
Non-Institutional Childbirths and the Associated Socio-Demographic Factors in Gambella Regional State, Ethiopia

 ,
,  ,
,  and
and
Abstract
:1. Background
2. Materials and Methods
2.1. Study design
2.2. Study Area
2.3. Data Analysis
3. Results
3.1. Socio-Demographic Characteristics of the Respondents
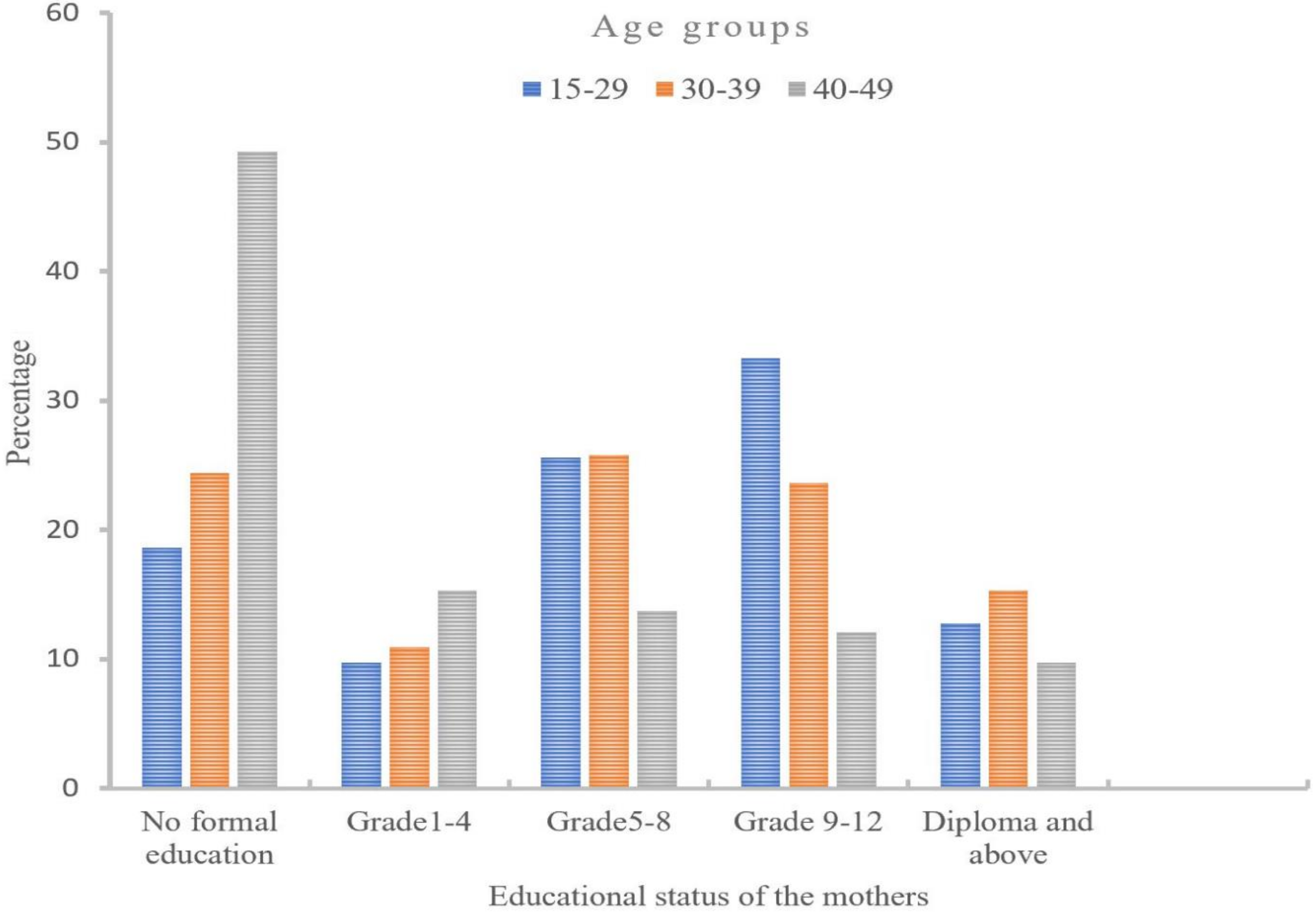
3.2. Proportion of Respondent’s Education Status by Age Groups
3.3. Factors Facilitated Mothers to Pursue Non-Institutional Childbirths
3.4. Plan for the Place of Delivery Service Utilization
3.5. Factors Associated with Non-Institutional Childbirths and Socio-Demographic Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johns, B. Trends in maternal mortality: 1990–2015: Estimates from WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Popul. Dev. Rev. 2016, 42, 726. [Google Scholar] [CrossRef] [Green Version]
- Kebede, A.; Hassen, K.; Nigussie Teklehaymanot, A. Factors associated with institutional delivery service utilization in Ethiopia. Int. J. Women’s Health 2016, 8, 463–475. [Google Scholar] [CrossRef] [Green Version]
- Kuruvilla, S.; Bustreo, F.; Kuo, T.; Mishra, C.K.; Taylor, K.; Fogstad, H.; Gupta, G.R.; Gilmore, K.; Temmerman, M.; Thomas, J.; et al. The Global strategy for women’s, children’s and adolescents’ health (2016–2030): A roadmap based on evidence and country experience. Bull. World Health Organ. 2016, 94, 398–400. [Google Scholar] [CrossRef]
- Filippi, V.; Chou, D.; Ronsmans, C.; Graham, W.; Say, L. Levels and causes of maternal mortality and morbidity. Reprod. Matern. Newborn Child Health Dis. Control Priorities 2016, 3, 51–70. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.M.; Rawal, L.B.; Chowdhury, S.A.; Murray, J.; Arscott-Mills, S.; Jack, S.; Hinton, R.; Alam, P.M.; Kuruvilla, S. Cross-country analysis of strategies for achieving progress towards global goals for women’s and children’s health. Bull. World Health Organ. 2016, 94, 351–361. [Google Scholar] [CrossRef]
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.-B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health 2014, 2, 323–333. [Google Scholar] [CrossRef] [Green Version]
- Alkema, L.; Chou, D.; Hogan, D.; Zhang, S.; Moller, A.B.; Gemmill, A.; Fat, D.M.; Boerma, T.; Temmerman, M.; Mathers, C. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario based projections to 2030 a systematic analysis by the U.N. Maternal Mortality Estimation Inter-Agency Group. Lancet 2016, 387, 462–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinney, M.V.; Kerber, K.J.; Black, R.E.; Cohen, B.; Nkrumah, F.; Coovadia, H.; Nampala, P.M.; Lawn, J.E. Sub-Saharan Africa’s mothers, newborns, and children: Where and why do they die? PLOS Med. 2010, 7, e1000294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CSA. Ethiopia Demographic and Health Survey 2016: Key Indicators Report; Addis Ababa, CSA and ICF, FR328: Rockville, MD, USA, 2016. [Google Scholar]
- Weldemariam, S.; Kiros, A.; Welday, M. Utilization of institutional delivery service and associated factors among mothers in North West Ethiopian. BMC Res. Notes 2018, 11, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, J.; Kwast, B. Epidemiologic study of vesicovaginal fistulas in Ethiopia. Int. Urogynecology J. 1993, 4, 278–281. [Google Scholar] [CrossRef]
- Ahmed, S.; Tunçalp, Ö. Burden of obstetric fistula: From measurement to action. Lancet Glob. Health 2015, 3, 243–244. [Google Scholar] [CrossRef] [Green Version]
- Moran, N.F.; Moodley, J. The effect of HIV infection on maternal health and mortality. Br. Int. J. Gynecol. Obstet. 2012, 119. [Google Scholar] [CrossRef] [PubMed]
- FMoH. Best Practice in Health: First National Workshops: Regional Presentations; FMoH: Addis Ababa, Ethiopia, 2006.
- Anshebo, D.; Geda, B.; Mecha, A.; Liru, A.; Ahmed, R. Utilization of institutional delivery and associated factors among mothers in Hosanna Town, Hadiya Zone, Southern Ethiopia: A community-based cross-sectional study. PLoS ONE 2020, 15, e0243350. [Google Scholar] [CrossRef] [PubMed]
- Lathrop, E.; Jamieson, D.J.; Danel, I. HIV and maternal mortality. Int. J. Gynecol. Obstet. 2014, 127, 213–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CSA. Summary and Statistical Report of the 2007 Population and Housing Census. CSA: Addis Ababa, Ethiopia, 2008. Available online: http://196.189.45.87:8080/handle/123456789/88805 (accessed on 7 May 2019).
- Norheim, O.F.; Jha, P.; Admasu, K.; Godal, T.; Hum, R.J.; Kruk, M.E.; Gómez-Dantés, O.; Mathers, C.D.; Pan, H.; Sepúlveda, J. Avoiding 40 % of the premature deaths in each country, 2010–2030: A review of national mortality trends to help quantify the U.N. Sustainable Development Goal for health. Lancet 2015, 385, 239–252. [Google Scholar] [CrossRef] [Green Version]
- Abeje, G.; Azage, M.; Setegn, T. Factors associated with Institutional delivery service utilization among mothers in Bahir Dar City administration, Amhara region: A community-based cross-sectional study. Reprod. Health 2014, 11, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadele, N.; Lamaro, T. Utilization of institutional delivery service and associated factors in Bench Maji zone, Southwest Ethiopia: A community-based, cross-sectional study. BMC Health Serv. Res. 2017, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagos, S.; Shaweno, D.; Assegid, M.; Mekonnen, A.; Afework, M.F.; Ahmed, S. Utilization of institutional delivery service at Wukro and Butajera districts in the Northern and South Central Ethiopia. BMC Pregnancy Childbirth 2014, 14, 178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsegay, Y.; Gebrehiwot, T.; Goicolea, I.; Edin, K.; Lemma, H.; Sebastian, M.S. Determinants of antenatal and delivery care utilization in Tigray region, Ethiopia: A cross-sectional study. Int. J. Equity Health 2013, 12, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekonnen, W.; Worku, A. Levels and proximate determinants of fertility in Butajira District, South Central Ethiopia. Ethiop. J. Health Dev. 2011, 25, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Mugweni, E.; Ehlers, V.J.; Roos, J.H. Factors contributing to low institutional deliveries in the Marondera district of Zimbabwe. Curationis 2008, 31, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Hidengwa, H. Comparison of Factors Associated with Utilization and Non-Utilization of Child Delivery Services among Multiparous and Grandmultiparous Women at Oshakati Intermediate Hospital and Nearby Health Centres, Oshana Region, Namibia. University of Namibia. 2018. Available online: http://hdl.handle.net/11070/2289 (accessed on 10 May 2019).
- Carter, A.; Factors that Contribute to the Low Uptake of Skilled Care during Delivery in Malindi, Kenya. Independent Study Project, Kenya. 2010. Available online: https://digitalcollections.sit.edu/isp_collection/821 (accessed on 13 May 2019).
- Mekonnen, M.G.; Yalew, K.N.; Umer, J.Y.; Melese, M. Determinants of delivery practices among Afar pastoralists of Ethiopia. Pan Afr. Med J. 2012, 13 (Suppl. S1). [Google Scholar]
- Wolelie, A.; Aychiluhm, M.; Awoke, W. Institutional delivery service utilization and associated factors in Banja District, Awie Zone, Amhara Regional State, Ethiopia. Open J. Epidemiol. 2014, 04, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Worku, A.; Jemal, M.; Gedefaw, A. Institutional delivery service utilization in Woldia, Ethiopia. Sci. J. Public Health 2013, 1, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Exavery, A.; Kanté, A.M.; Njozi, M.; Tani, K.; Doctor, H.V.; Hingora, A.; Phillips, J.F. Access to institutional delivery care and reasons for home delivery in three districts of Tanzania. Int. J. Equity Health 2014, 13, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | All Respondents | Non-Healthcare Institutional Birth | Healthcare Institutional Birth | χ2 | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Number | Percent | Number | Percent | Number | Percent | |||
| Age groups | ||||||||
| 15–29 | 258 | 39.0 | 178 | 69.0 | 80 | 31.0 | 1.241 | 0.538 |
| 30–40 | 275 | 41.9 | 198 | 72.0 | 77 | 28.0 | ||
| 40–49 | 124 | 18.9 | 92 | 74.2 | 32 | 25.8 | ||
| Marital Status | ||||||||
| Married | 531 | 80.8 | 365 | 68.7 | 166 | 31.3 | 8.409 | 0.015 |
| Single | 60 | 9.0 | 49 | 81.7 | 11 | 18.3 | ||
| Others * | 66 | 10.0 | 54 | 81.8 | 12 | 18.2 | ||
| Occupation | ||||||||
| Housewife | 387 | 58.9 | 287 | 74.2 | 100 | 25.8 | 13.373 | 0.004 |
| Employee | 93 | 14.2 | 52 | 55.9 | 41 | 44.1 | ||
| Merchant | 42 | 6.4 | 33 | 78.6 | 9 | 21.4 | ||
| Others ** | 135 | 20.5 | 96 | 71.1 | 39 | 28.9 | ||
| Educational status | ||||||||
| No formal education | 176 | 26.8 | 139 | 79 | 37 | 21.0 | 14.306 | 0.006 |
| Grade 1–4 | 74 | 11.3 | 56 | 75.7 | 18 | 24.3 | ||
| Grade 5–8 | 154 | 23.4 | 108 | 70.1 | 46 | 29.9 | ||
| Grade 9–12 | 166 | 25.3 | 115 | 69.3 | 51 | 30.7 | ||
| Diploma and above | 87 | 57.5 | 50 | 57.5 | 37 | 42.5 | ||
| Religion | ||||||||
| Christian | 621 | 94.5 | 444 | 71.5 | 177 | 28.5 | 0.453 | 0.797 |
| Muslim | 13 | 2.0 | 9 | 69.2 | 4 | 30.8 | ||
| Others *** | 23 | 3.5 | 15 | 65.2 | 8 | 34.8 | ||
| Monthly income | ||||||||
| Below 1000 ETB | 426 | 64.8 | 314 | 73.7 | 112 | 26.3 | 5.348 | 0.148 |
| 1001–3000 ETB | 155 | 23.6 | 105 | 67.7 | 50 | 32.3 | ||
| 3001–6000 ETB | 64 | 9.7 | 43 | 67.2 | 21 | 32.8 | ||
| 6001 ETB and above | 12 | 1.8 | 6 | 50.0 | 6 | 50.0 | ||
| Ethnicity | ||||||||
| Anywaa | 235 | 35.8 | 156 | 66.4 | 79 | 33.6 | 16.795 | 0.005 |
| Nuer | 226 | 34.4 | 178 | 78.8 | 48 | 21.2 | ||
| Majang | 87 | 13.2 | 67 | 77.0 | 20 | 23.0 | ||
| Komo | 8 | 1.2 | 6 | 75.0 | 2 | 25.0 | ||
| Opuo | 10 | 1.5 | 5 | 50.0 | 5 | 50.0 | ||
| Others **** | 91 | 13.9 | 56 | 61.5 | 35 | 38.5 | ||
| Variable | Place of Birth | χ2 | p-Value | |||
|---|---|---|---|---|---|---|
| Institutional Birth | Non-institutional Birth | |||||
| Number | Percent | Number | Percent | |||
| Plan for the place of delivery | ||||||
| Yes | 160 | 41 | 230 | 59 | 70.375 | 0.006 |
| No | 29 | 10.9 | 238 | 89.1 | ||
| For yes where to delivery | ||||||
| Non-institutional birth | 1 | 1.7 | 57 | 98.3 | 43.496 | <0.001 |
| Institutional birth | 159 | 47.9 | 173 | 52.1 | ||
| Variable | Place of Birth | OR (95 % CI) | p-Value | AOR (95 % CI) | p-Value | |
|---|---|---|---|---|---|---|
| Non-Institutional Birth n (%) | Institutional Birth n (%) | |||||
| Age groups | ||||||
| 15–29 | 178 (69.0%) | 80 (31.0%) | 0.77 (0.47–1.25) | 0.296 | ||
| 30–40 | 198 (72.0%) | 77 (28.0%) | 0.89 (0.55–1.44) | 0.649 | ||
| 40–49 | 92 (74.2%) | 32 (25.8%) | 1 | |||
| Marital Status | ||||||
| Married | 365 (68.7%) | 166 (31.3%) | 0.49 (0.25–0.93) | 0.031 | 0.36 (0.17–0.74) | 0.006 |
| Single | 49 (81.7%) | 11 (18.3%) | 0.99 (0.40–2.44) | 0.982 | 1.36 (0.53–3.47) | 0.524 |
| Others * | 54 (81.8%) | 12(18.2%) | 1 | 1 | ||
| Occupation | ||||||
| Housewife | 287 (74.2%) | 100 (25.8%) | 0.47 (0.69–0.91) | 0.039 | 1.87 (1.14–3.05) | 0.012 |
| Employee | 52 (55.9%) | 41 (44.1%) | 0.52 (0.29–0.89) | 0.019 | 0.57 (0.31–0.82) | 0.029 |
| Merchant | 33 (78.6%) | 9 (21.4%) | 1.49 (0.65–3.40) | 0.344 | 1.44 (0.61–3.37) | 0.397 |
| Others ** | 96 (71.1%) | 39 (28.9%) | 1 | 1 | ||
| Educational status | ||||||
| No formal education | 139 (79.0%) | 37 (21.0%) | 2.78 (1.59–4.86) | <0.01 | 2.49 (1.40–4.41) | 0.002 |
| Grade 1–4 | 56 (75.7%) | 18 (24.3%) | 2.30 (1.16–4.54) | 0.016 | 2.15 (1.08–4.27) | 0.029 |
| Grade 5–8 | 108 (70.1%) | 46 (29.9%) | 1.74 (1.00–3.00) | 0.048 | 1.77 (1.01–3.08) | 0.045 |
| Grade 9–12 | 115 (69.3%) | 51 (30.7%) | 1.67 (0.97–2.85) | 0.062 | 1.74 (1.00–3.01) | 0.049 |
| Diploma and above | 50 (57.5%) | 37 (42.5%) | 1 | 1 | ||
| Religion | ||||||
| Christian | 444 (71.5%) | 177 (28.5%) | 1.34 (0.55–3.21) | 0.515 | ||
| Muslim | 9 (69.2%) | 4 (30.8%) | 1.20 (0.27–5.15) | 0.806 | ||
| Others *** | 15 (65.2%) | 8 (34.8%) | 1 | |||
| Monthly income | ||||||
| Below 1000 ETB | 314 (73.7%) | 112 (26.3%) | 2.80 (0.88–8.87) | 0.079 | ||
| 1001–3000 ETB | 105 (67.7%) | 50 (32.3%) | 2.10 (0.64–6.83) | 0.218 | ||
| 3001–6000 ETB | 43 (67.2%) | 21 (32.8%) | 2.05 (0.58–7.11) | 0.26 | ||
| 6001 ETB and above | 6 (50.0%) | 6 (50.0%) | 1 | |||
| Ethnicity | ||||||
| Anywaa | 156 (66.4%) | 79 (33.6%) | 1.23 (0.74–2.03) | 0.411 | 1.24 (0.74–2.07) | 0.408 |
| Nuer | 178 (78.8%) | 48 (21.2%) | 2.32 (1.36–3.93) | 0.002 | 2.12 (1.23–3.63) | 0.006 |
| Majang | 67 (77.0%) | 20 (23.0%) | 2.09 (1.08–4.02) | 0.027 | 1.98 (1.02–3.83) | 0.043 |
| Komo | 6 (75.0%) | 2 (25.0%) | 1.88 (0.35–9.81) | 0.457 | 1.49 (0.28–7.95) | 0.636 |
| Opuo | 5 (50.0%) | 5 (50.0%) | 0.63 (0.16–2.31) | 0.482 | 0.57 (0.15–2.14) | 0.404 |
| Others **** | 56 (61.5%) | 35 (38.5%) | 1 | 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gora, G.A.; Umer, M.F.; Ojulu, P.O.; Betaw, S.T.; Cham, A.O.; Gora, O.A.; Qi, X. Non-Institutional Childbirths and the Associated Socio-Demographic Factors in Gambella Regional State, Ethiopia. Int. J. Environ. Res. Public Health 2021, 18, 2859. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062859
Gora GA, Umer MF, Ojulu PO, Betaw ST, Cham AO, Gora OA, Qi X. Non-Institutional Childbirths and the Associated Socio-Demographic Factors in Gambella Regional State, Ethiopia. International Journal of Environmental Research and Public Health. 2021; 18(6):2859. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062859
Chicago/Turabian StyleGora, Gnkambo Agwa, Muhammad Farooq Umer, Peter Obang Ojulu, Sintayehu Tsegaye Betaw, Akwoma Okugn Cham, Ojulu Agwa Gora, and Xin Qi. 2021. "Non-Institutional Childbirths and the Associated Socio-Demographic Factors in Gambella Regional State, Ethiopia" International Journal of Environmental Research and Public Health 18, no. 6: 2859. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062859