
Sleep Debt and Social Jetlag Associated with Sleepiness, Mood, and Work Performance among Workers in Japan



Abstract
:1. Introduction
2. Materials and Methods
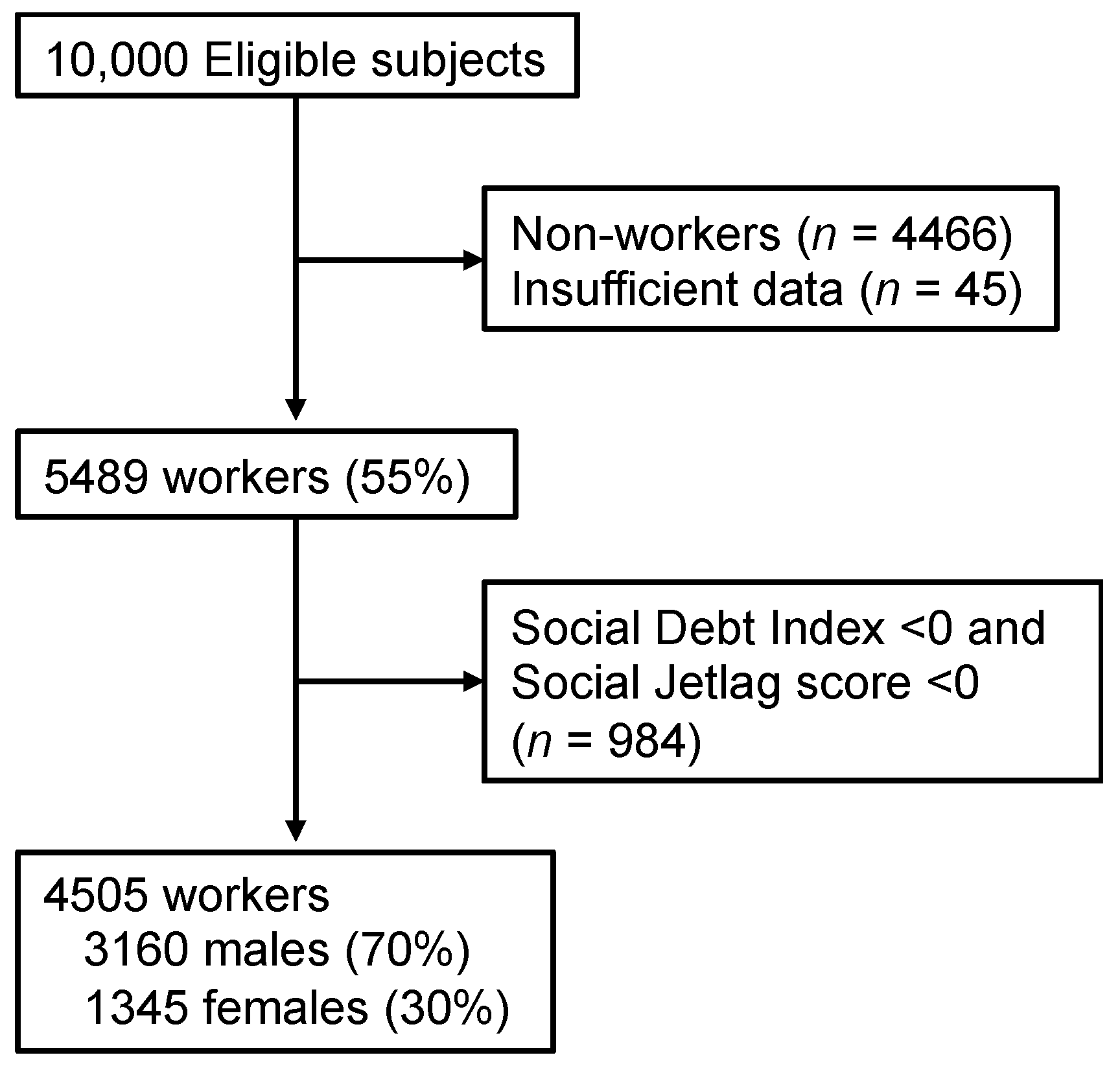
2.1. Participants
2.2. Assessments
2.2.1. Demographic Information
2.2.2. Japanese Version of the Epworth Sleepiness Scale (ESS)
2.2.3. 12-Item Version of the Center for Epidemiological Studies Depression Scale (CES-D)
2.2.4. WHO Health and Work Performance Questionnaire-Presenteeism (WHO-HPQ Presenteeism)
2.2.5. Sleep Habits: SDI and SJL
2.3. Statistical Analysis
3. Results
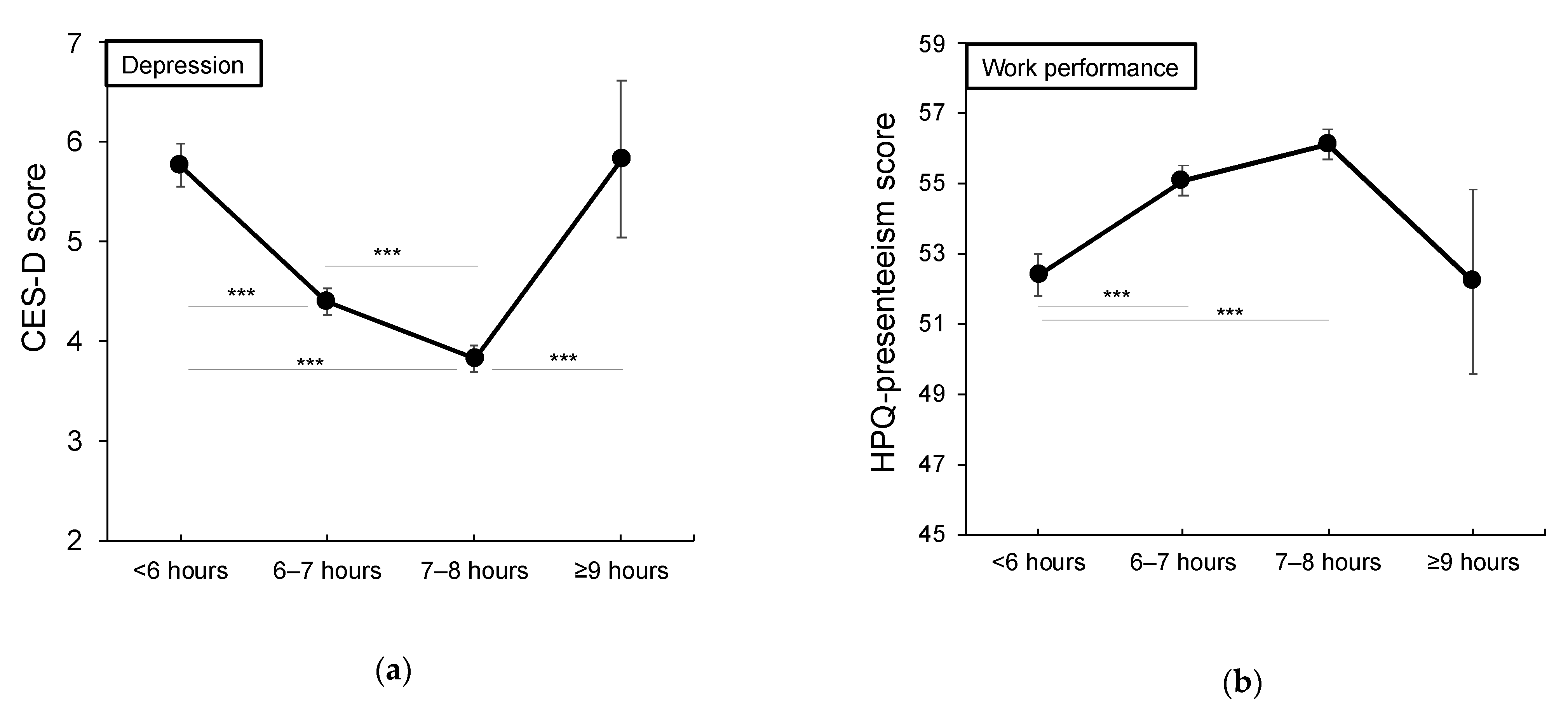
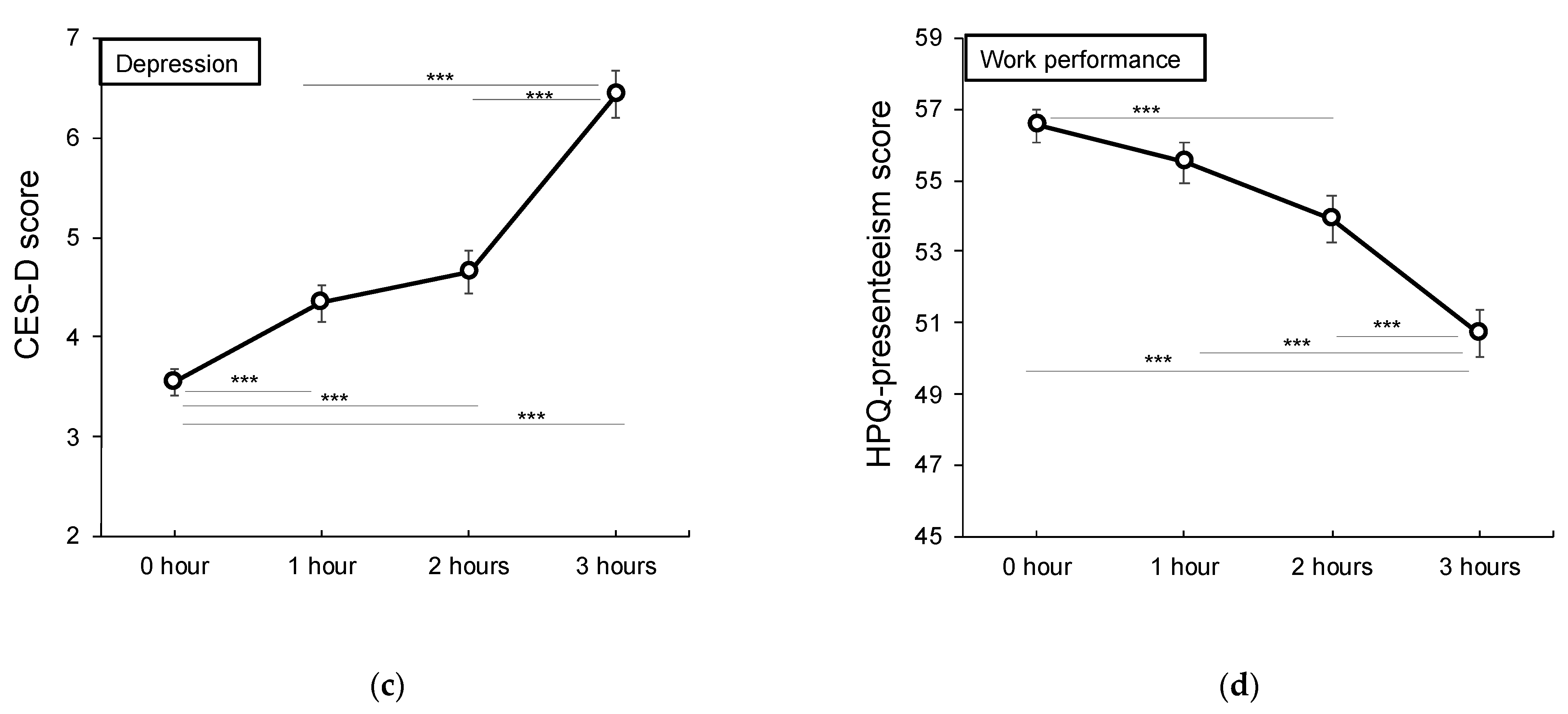
3.1. Association of SDI and Sleep Duration with Depression, Sleepiness, and Performance
3.2. Comparison of Demographic Data within the SDI Group and SJL Group
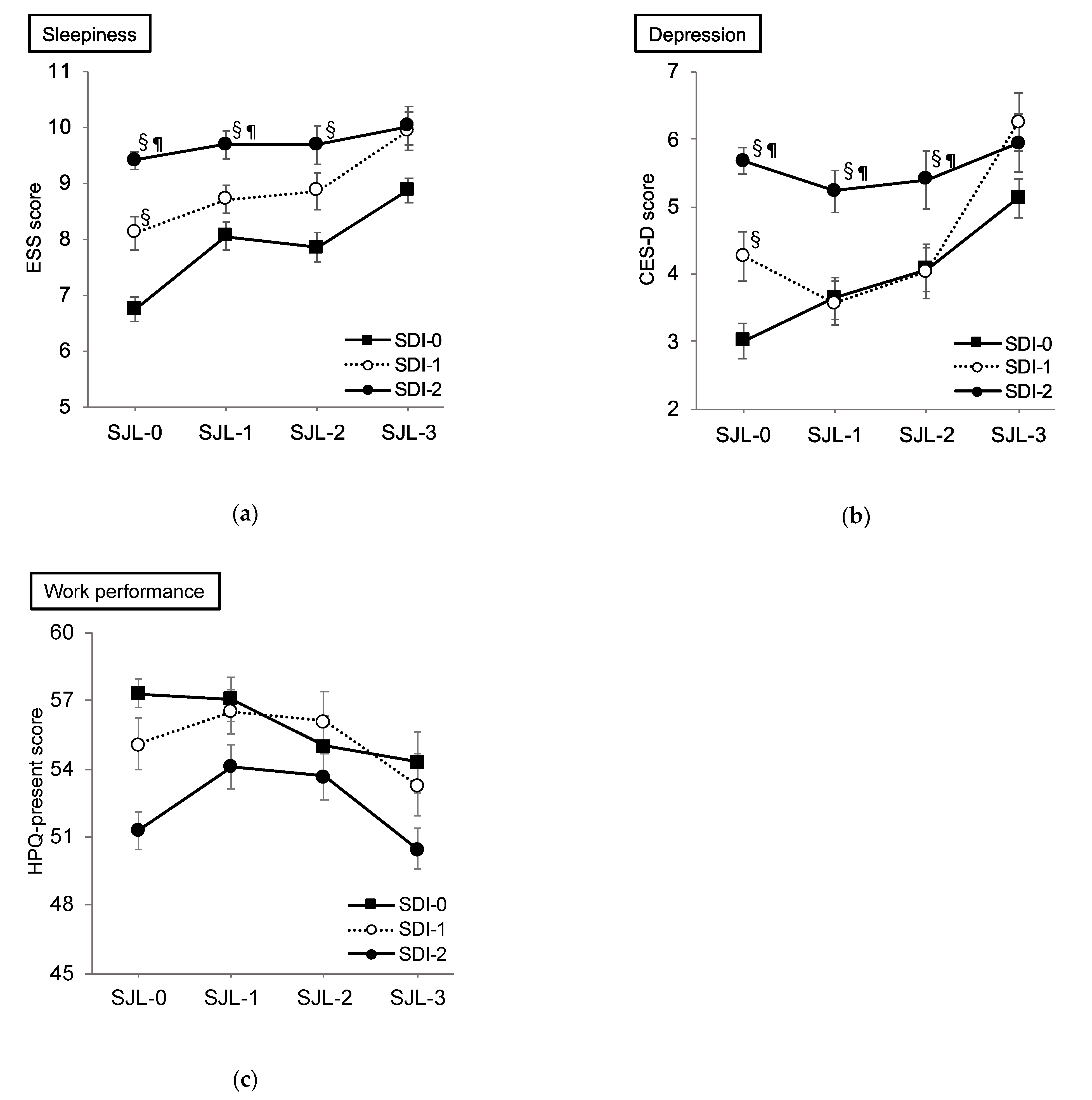
3.3. Effect of SDI and SJL on Sleepiness
3.4. Effect of SDI and SJL on Depression
3.5. Effect of SDI and SJL on Work Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jewett, M.; Dijk, D.; Kronauer, R.; Dinges, D. Dose-Response Relationship between Sleep Duration and Human Psychomotor Vigilance and Subjective Alertness. Sleep 1999, 22, 171–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnet, M.H.; Arand, D.L. Clinical Effects of Sleep Fragmentation versus Sleep Deprivation. Sleep Med. Rev. 2003, 7, 297–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiffer, D.; Minonzio, M.; Dipaola, F.; Bertola, M.; Zamuner, A.R.; Dalla Vecchia, L.A.; Solbiati, M.; Costantino, G.; Furlan, R.; Barbic, F. Effects of Clockwise and Counterclockwise Job Shift Work Rotation on Sleep and Work-Life Balance on Hospital Nurses. Int. J. Environ. Res. Public Health 2018, 15, 2038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labor and Welfare. Japan National Health and Nutrition Survey in 2017. Available online: https://www.mhlw.go.jp/stf/houdou/0000177189_00001.html (accessed on 29 January 2021).
- Roenneberg, T.; Kuehnle, T.; Juda, M.; Kantermann, T.; Allebrandt, K.; Gordijn, M.; Merrow, M. Epidemiology of the Human Circadian Clock. Sleep Med. Rev. 2007, 11, 429–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittmann, M.; Dinich, J.; Merrow, M.; Roenneberg, T. Social Jetlag: Misalignment of Biological and Social Time. Chronobiol. Int. 2006, 23, 497–509. [Google Scholar] [CrossRef]
- Islam, Z.; Akter, S.; Kochi, T.; Hu, H.; Eguchi, M.; Yamaguchi, M.; Kuwahara, K.; Kabe, I.; Mizoue, T. Association of Social Jetlag with Metabolic Syndrome among Japanese Working Population: The Furukawa Nutrition and Health Study. Sleep Med. 2018, 51, 53–58. [Google Scholar] [CrossRef]
- Carskadon, M.A.; Dement, W.C. Nocturnal Determinants of Daytime Sleepiness. Sleep 1982, 5, S73–S81. [Google Scholar] [CrossRef] [Green Version]
- Kaneita, Y.; Ohida, T.; Uchiyama, M.; Takemura, S.; Kawahara, K.; Yokoyama, E.; Miyake, T.; Harano, S.; Suzuki, K.; Fujita, T. The Relationship between Depression and Sleep Disturbances: A Japanese Nationwide General Population Survey. J. Clin. Psychiatry 2006, 67, 196–203. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014; pp. 182–186. [Google Scholar]
- Lee, Y.J.; Park, J.; Kim, S.; Cho, S.-J.; Kim, S.J. Academic Performance among Adolescents with Behaviorally Induced Insufficient Sleep Syndrome. J. Clin. Sleep Med. 2015, 11, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Doi, Y.; Ishihara, K.; Uchiyama, M. Associations of Chronotype with Social Jetlag and Behavioral Problems in Preschool Children. Chronobiol. Int. 2015, 32, 1101–1108. [Google Scholar] [CrossRef]
- Díaz-Morales, J.F.; Escribano, C. Social Jetlag, Academic Achievement and Cognitive Performance: Understanding Gender/Sex Differences. Chronobiol. Int. 2015, 32, 822–831. [Google Scholar] [CrossRef] [Green Version]
- Silva, C.M.; Mota, M.C.; Miranda, M.T.; Paim, S.L.; Waterhouse, J.; Crispim, C.A. Chronotype, Social Jetlag and Sleep Debt Are Associated with Dietary Intake among Brazilian Undergraduate Students. Chronobiol. Int. 2016, 33, 740–748. [Google Scholar] [CrossRef]
- Levandovski, R.; Dantas, G.; Fernandes, L.C.; Caumo, W.; Torres, I.; Roenneberg, T.; Hidalgo, M.P.L.; Allebrandt, K.V. Depression Scores Associate With Chronotype and Social Jetlag in a Rural Population. Chronobiol. Int. 2011, 28, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Shan, Z.; Ma, H.; Xie, M.; Yan, P.; Guo, Y.; Bao, W.; Rong, Y.; Jackson, C.L.; Hu, F.B.; Liu, L. Sleep Duration and Risk of Type 2 Diabetes: A Meta-Analysis of Prospective Studies. Diabetes Care 2015, 38, 529. [Google Scholar] [CrossRef] [Green Version]
- Matsui, K.; Kuriyama, K.; Yoshiike, T.; Nagao, K.; Ayabe, N.; Komada, Y.; Okajima, I.; Ito, W.; Ishigooka, J.; Nishimura, K.; et al. The Effect of Short or Long Sleep Duration on Quality of Life and Depression: An Internet-Based Survey in Japan. Sleep Med. 2020, 76, 80–85. [Google Scholar] [CrossRef]
- Ito, W.; Komada, Y.; Okajima, I.; Inoue, Y. Excessive Daytime Sleepiness in Adults with Possible Attention Deficit/Hyperactivity Disorder (ADHD): A Web-Based Cross-Sectional Study. Sleep Med. 2017, 32, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Komada, Y.; Okajima, I.; Kitamura, S.; Inoue, Y. A Survey on Social Jetlag in Japan: A Nationwide, Cross-Sectional Internet Survey. Sleep Biol. Rhythm. 2019, 17, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Kohyama, J. Pupils with Negative Social Jetlag in Japan Are Hypothesised to Constitute a Discrete Population. Med. Hypotheses. 2020, 144, 110249. [Google Scholar] [CrossRef] [PubMed]
- Takegami, M.; Suzukamo, Y.; Wakita, T.; Noguchi, H.; Chin, K.; Kadotani, H.; Inoue, Y.; Oka, Y.; Nakamura, T.; Green, J.; et al. Development of a Japanese Version of the Epworth Sleepiness Scale (JESS) Based on Item Response Theory. Sleep Med. 2009, 10, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Poulin, C.; Hand, D.; Boudreau, B. Validity of a 12-Item Version of the CES-D Used in the National Longitudinal Study of Children and Youth. Chronic Dis. Can. 2005, 26, 65–72. [Google Scholar]
- Suzuki, T.; Miyaki, K.; Sasaki, Y.; Song, Y.; Tsutsumi, A.; Kawakami, N.; Shimazu, A.; Takahashi, M.; Inoue, A.; Kurioka, S.; et al. Optimal Cutoff Values of WHO-HPQ Presenteeism Scores by ROC Analysis for Preventing Mental Sickness Absence in Japanese Prospective Cohort. PLoS ONE 2014, 9, e111191. [Google Scholar] [CrossRef]
- Doki, S.; Sasahara, S.; Suzuki, S.; Hirai, Y.; Oi, Y.; Usami, K.; Matsuzaki, I. Relationship between Sickness Presenteeism and Awareness and Presence or Absence of Systems for Return to Work among Workers with Mental Health Problems in Japan: An Internet-Based Cross-Sectional Study. J. Occup. Health 2015, 57, 532–539. [Google Scholar] [CrossRef] [Green Version]
- Torsvall, L.; Åkerstedt, T. A Diurnal Type Scale: Construction, Consistency and Validation in Shift Work. Scand. J. Work Environ. Health 1980, 6, 283–290. [Google Scholar] [CrossRef]
- Roenneberg, T.; Allebrandt, K.V.; Merrow, M.; Vetter, C. Social Jetlag and Obesity. Curr. Biol. 2012, 22, 939–943. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sleep Debt Index (hours) | Social Jetlag (hours) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total n = 4505 | ≥0 n = 1693 | ≥1 n = 1087 | ≥2 n = 1725 | ≥0 n = 1702 | ≥1 n = 1157 | ≥2 n = 1157 | ≥3 n = 855 | ||
| Age, (SD) | 43.57 (11.63) | 45.48 (12.24) | 43.29 (11.40) | 41.87 (10.87) | 46.16 (11.98) | 43.87 (11.22) | 42.02 (10.80) | 39.42 (10.79) | |
| Gender, n (%) | M F | 3160 (70) 1345 (30) | 1253 (28) 440 (10) | 740 (16) 347 (8) | 1167 (26) 558 (12) | 1273 (28) 429 (10) | 816 (18) 341 (25) | 538 (12) 253 (6) | 533 (12) 322 (7) |
| Smoking habits, n (%) | Y N | 1135 (25) 3370 (75) | 411 (9) 1282 (29) | 282 (6) 805 (18) | 442 (10) 1283 (29) | 377 (8) 1325 (29) | 264 (6) 893 (20) | 213 (5) 578 (13) | 281 (6) 574 (13) |
| Drinking habits, n (%) | Y N | 2549 (57) 1956 (43) | 985 (22) 708 (16) | 618 (14) 469 (10) | 946 (21) 779 (17) | 1001 (22) 701 (16) | 641 (14) 516 (12) | 432 (19) 359 (8) | 281 (6) 574 (13) |
| Living alone, n (%) | Y N | 871 (19) 3634 (81) | 298 (7) 1395 (31) | 220 (5) 867 (19) | 353 (8) 1372 (31) | 225 (6) 1447 (32) | 215 (5) 942 (21) | 166 (4) 625 (14) | 235 (5) 620 (14) |
| ESS | CES-D | HPQ-Presenteeism | ||||
|---|---|---|---|---|---|---|
| Groups | Mean | SD | Mean | SD | Mean | SD |
| SDI-0 | ||||||
| SJL-0 | 6.74 | 5.05 | 3.01 | 5.55 | 57.31 | 19.22 |
| SJL-1 | 8.06 § | 4.44 | 3.64 | 5.15 | 57.07 | 19.51 |
| SJL-2 | 7.85 § | 4.56 | 4.07 | 5.32 | 55.00 | 17.66 |
| SJL-3 | 8.88 § | 4.87 | 5.13 §¶ | 6.37 | 54.28 | 16.72 |
| SDI-1 | ||||||
| SJL-0 | 8.11 | 4.49 | 4.27 | 6.61 | 55.09 | 18.99 |
| SJL-1 | 8.71 | 4.49 | 3.57 | 5.27 | 56.52 | 19.73 |
| SJL-2 | 8.87 | 5.03 | 4.04 | 5.62 | 56.11 | 18.35 |
| SJL-3 | 9.95 §¶ | 4.97 | 6.25 §¶† | 7.04 | 53.30 | 19.49 |
| SDI-2 | ||||||
| SJL-0 | 9.41 | 5.27 | 5.68 | 7.09 | 51.27 | 20.15 |
| SJL-1 | 9.70 | 5.03 | 5.23 | 6.32 | 54.10 | 18.63 |
| SJL-2 | 9.70 | 4.98 | 5.41 | 6.33 | 53.68 | 18.70 |
| SJL-3 | 10.33 | 5.03 | 5.94 | 6.52 | 50.46 | 20.81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okajima, I.; Komada, Y.; Ito, W.; Inoue, Y. Sleep Debt and Social Jetlag Associated with Sleepiness, Mood, and Work Performance among Workers in Japan. Int. J. Environ. Res. Public Health 2021, 18, 2908. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062908
Okajima I, Komada Y, Ito W, Inoue Y. Sleep Debt and Social Jetlag Associated with Sleepiness, Mood, and Work Performance among Workers in Japan. International Journal of Environmental Research and Public Health. 2021; 18(6):2908. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062908
Chicago/Turabian StyleOkajima, Isa, Yoko Komada, Wakako Ito, and Yuichi Inoue. 2021. "Sleep Debt and Social Jetlag Associated with Sleepiness, Mood, and Work Performance among Workers in Japan" International Journal of Environmental Research and Public Health 18, no. 6: 2908. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062908