
The Mediating Role of Lean Soft Tissue in the Relationship between Somatic Maturation and Bone Density in Adolescent Practitioners and Non-Practitioners of Sports

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Body Composition Measures
2.3. Anthropometry
2.4. Somatic Maturation
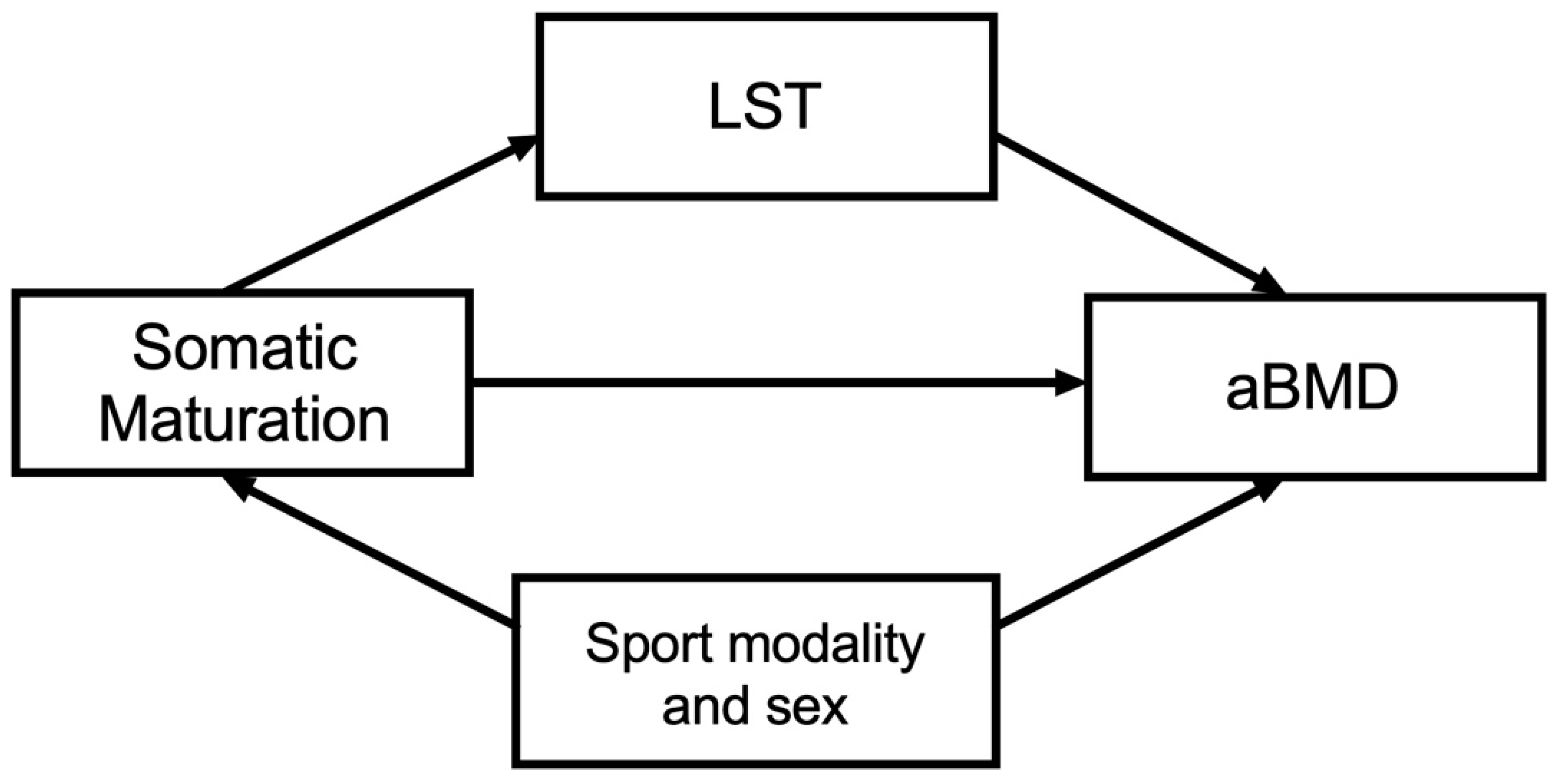
2.5. Statistical Analysis
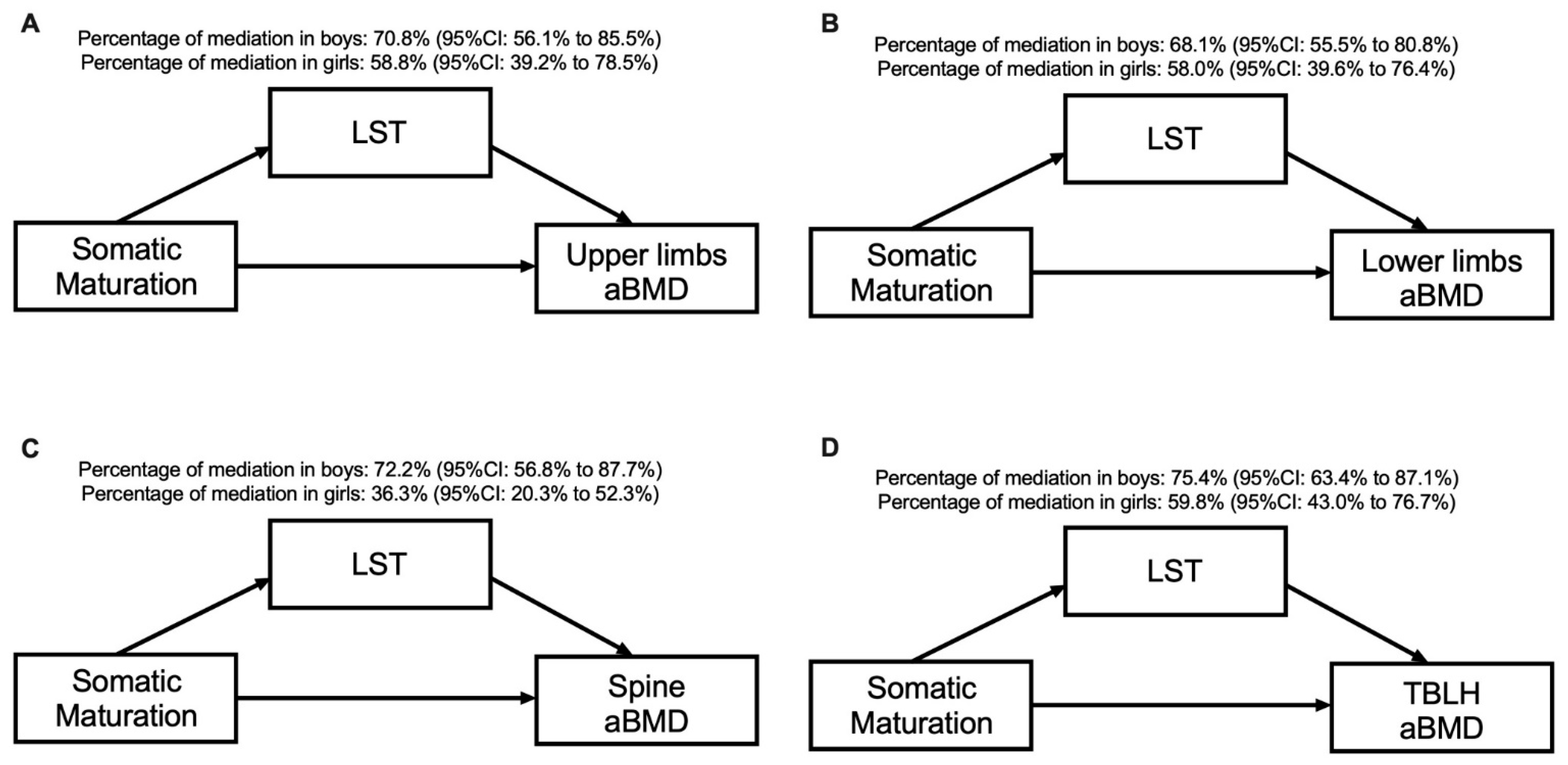
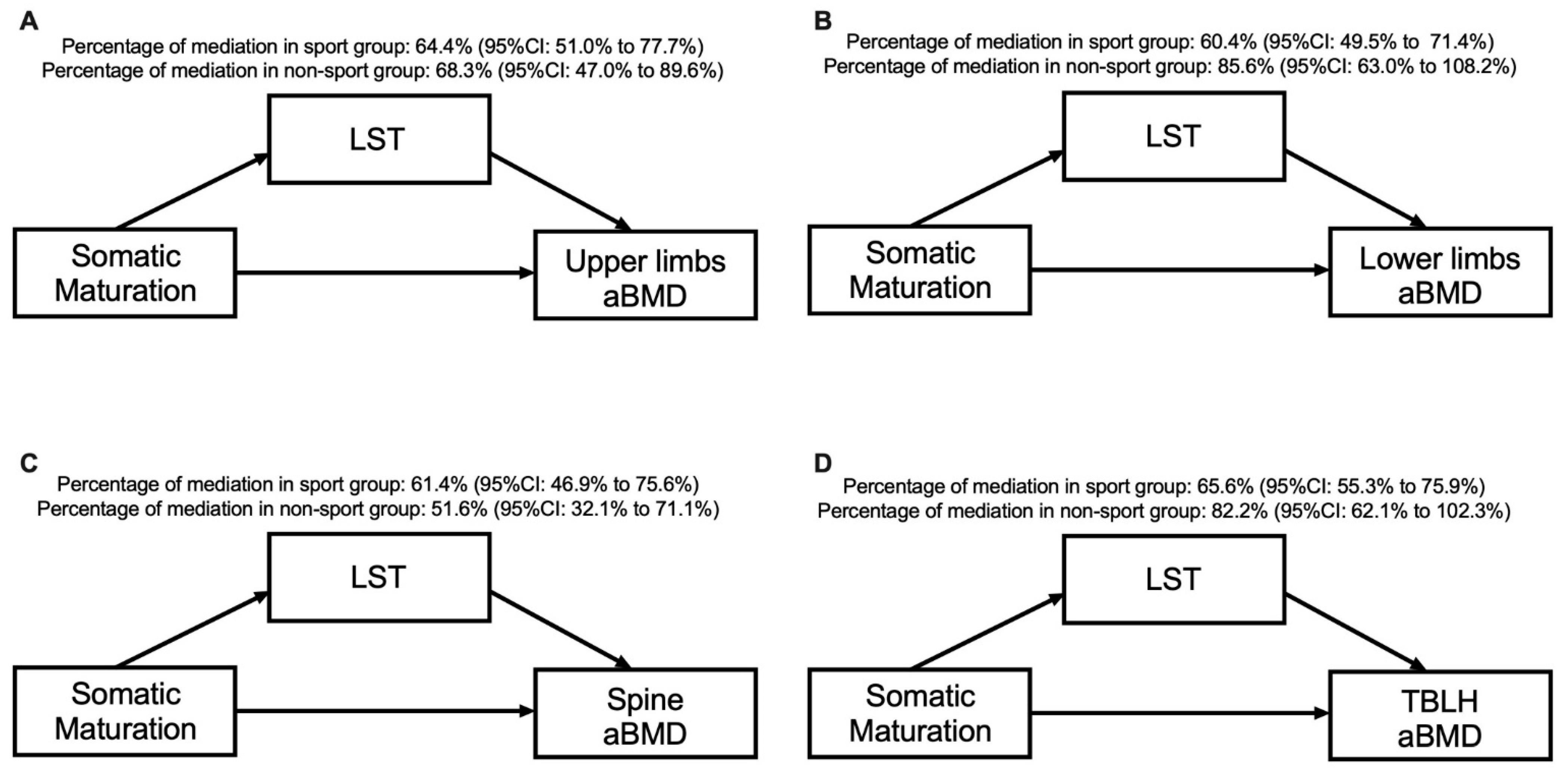
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malina, R.M.; Bouchard, C.; Bar-Or, O. Growth, Maturation, and Physical Activity, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2004; ISBN 0880118822. [Google Scholar]
- Lynch, K.R.; Anokye, N.K.; Vlachopoulos, D.; Barbieri, F.A.; Turi-Lynch, B.C.; Codogno, J.S.; Agostinete, R.R.; Fernandes, R.A. Impact of sports participation on incidence of bone traumatic fractures and health-care costs among adolescents: ABCD—Growth Study. Phys. Sportsmed. 2019, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Christoffersen, T.; Emaus, N.; Dennison, E.; Furberg, A.-S.; Gracia-Marco, L.; Grimnes, G.; Nilsen, O.A.; Vlachopoulos, D.; Winther, A.; Ahmed, L.A. The association between childhood fractures and adolescence bone outcomes: A population-based study, the Tromsø Study, Fit Futures. Osteoporos. Int. 2018, 29, 441–450. [Google Scholar] [CrossRef]
- Schoenau, E.; Frost, H.M. The “Muscle-Bone Unit” in Children and Adolescents. Calcif. Tissue Int. 2002, 70, 405–407. [Google Scholar] [CrossRef] [PubMed]
- Ross, M.H.; Pawlina, W. Chapter 8 Bone. In Histology: A Text and Atlas: With Correlated Cell and Molecular Biology; Lippincott Williams & Wilkins, a Wolters Kluwer Business: Baltimore, MD, USA, 2011; pp. 218–242. ISBN 978-0-7817-7200-6. [Google Scholar]
- Ross, M.H.; Pawlina, W. Chapter 11 Muscle Tisse. In Histology: A Text and Atlas: With Correlated Cell and Molecular Biology; Lippincott Williams & Wilkins, a Wolters Kluwer Business: Baltimore, MD, USA, 2011; pp. 310–331. ISBN 978-0-7817-7200-6. [Google Scholar]
- Baxter-Jones, A.D.; Faulkner, R.A.; Forwood, M.R.; Mirwald, R.L.; Bailey, D.A. Bone mineral accrual from 8 to 30 years of age: An estimation of peak bone mass. J. Bone Miner. Res. 2011, 26, 1729–1739. [Google Scholar] [CrossRef]
- Ubago-Guisado, E.; Vlachopoulos, D.; Barker, A.R.; Christoffersen, T.; Metcalf, B.; Gracia-Marco, L. Effect of maturational timing on bone health in male adolescent athletes engaged in different sports: The PRO-BONE study. J. Sci. Med. Sport 2019, 22, 253–258. [Google Scholar] [CrossRef]
- Jackowski, S.A.; Erlandson, M.C.; Mirwald, R.L.; Faulkner, R.A.; Bailey, D.A.; Kontulainen, S.A.; Cooper, D.M.L.; Baxter-Jones, A.D.G. Effect of maturational timing on bone mineral content accrual from childhood to adulthood: Evidence from 15years of longitudinal data. Bone 2011, 48, 1178–1185. [Google Scholar] [CrossRef]
- Vlachopoulos, D.; Ubago-Guisado, E.; Barker, A.R.; Metcalf, B.S.; Fatouros, I.G.; Avloniti, A.; Knapp, K.M.; Moreno, L.A.; Williams, C.A.; Gracia-Marco, L. Determinants of Bone Outcomes in Adolescent Athletes at Baseline: The PRO-BONE Study. Med. Sci. Sports Exerc. 2017, 49, 1389–1396. [Google Scholar] [CrossRef] [PubMed]
- Frost, H.M.; Schönau, E. The “muscle-bone unit” in children and adolescents: A 2000 overview. J. Pediatr. Endocrinol. Metab. 2000, 13, 571–590. [Google Scholar] [CrossRef]
- Jackowski, S.A.; Faulkner, R.A.; Farthing, J.P.; Kontulainen, S.A.; Beck, T.J.; Baxter-Jones, A.D.G. Peak lean tissue mass accrual precedes changes in bone strength indices at the proximal femur during the pubertal growth spurt. Bone 2009, 44, 1186–1190. [Google Scholar] [CrossRef]
- Kuh, D.; Muthuri, S.G.; Moore, A.; Cole, T.J.; Adams, J.E.; Cooper, C.; Hardy, R.; Ward, K.A. Pubertal timing and bone phenotype in early old age: Findings from a British birth cohort study. Int. J. Epidemiol. 2016, 45, 1113–1124. [Google Scholar] [CrossRef]
- Silva, C.C.; Goldberg, T.B.L.; Nga, H.S.; Kurokawa, C.S.; Capela, R.C.; Teixeira, A.S.; Dalmas, J.C. Impact of skeletal maturation on bone metabolism biomarkers and bone mineral density in healthy Brazilian male adolescents. J. Pediatr. Rio J. 2011, 87, 450–456. [Google Scholar] [CrossRef] [Green Version]
- Agostinete, R.R.; Ito, I.H.; Kemper, H.; Pastre, C.M.; Rodrigues-Júnior, M.A.; Luiz-de-Marco, R.; Fernandes, R.A. Somatic maturation and the relationship between bone mineral variables and types of sports among adolescents: Cross-sectional study. Sao Paulo Med. J. 2017, 135, 253–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ubago-Guisado, E.; Vlachopoulos, D.; Ferreira de Moraes, A.C.; Torres-Costoso, A.; Wilkinson, K.; Metcalf, B.; Sánchez-Sánchez, J.; Gallardo, L.; Gracia-Marco, L. Lean mass explains the association between muscular fitness and bone outcomes in 13-year-old boys. Acta Paediatr. 2017, 106, 1658–1665. [Google Scholar] [CrossRef]
- Vlachopoulos, D.; Barker, A.R.; Ubago-Guisado, E.; Fatouros, I.G.; Knapp, K.M.; Williams, C.A.; Gracia-Marco, L. Longitudinal Adaptations of Bone Mass, Geometry, and Metabolism in Adolescent Male Athletes: The PRO-BONE Study. J. Bone Miner. Res. 2017, 32, 2269–2277. [Google Scholar] [CrossRef]
- International Society for Clinical Densitometry. Skeletal Health Assessment. In Children from Infancy to Adolescence; ISCD: Middletown, CT, USA, 2013. [Google Scholar]
- Agostinete, R.R.; Vlachopoulos, D.; Werneck, A.O.; Maillane-Vanegas, S.; Lynch, K.R.; Naughton, G.; Fernandes, R.A. Bone accrual over 18 months of participation in different loading sports during adolescence. Arch. Osteoporos. 2020, 15, 64. [Google Scholar] [CrossRef]
- Gordon, C.; Chumlea, W.; Roche, A. Stature, recumbent length, and weight. In Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988; pp. 3–8. [Google Scholar]
- Moore, S.A.; McKay, H.A.; Macdonald, H.; Nettlefold, L.; Baxter-Jones, A.D.G.; Cameron, N.; Brasher, P.M.A. Enhancing a Somatic Maturity Prediction Model. Med. Sci. Sports Exerc. 2015, 47, 1755–1764. [Google Scholar] [CrossRef]
- Valeri, L.; Vanderweele, T.J. Mediation analysis allowing for exposure-mediator interactions and causal interpretation: Theoretical assumptions and implementation with SAS and SPSS macros. Psychol. Methods 2013, 18, 137–150. [Google Scholar] [CrossRef] [Green Version]
- Agostinete, R.R.; Fernandes, R.A.; Narciso, P.H.; Maillane-Vanegas, S.; Werneck, A.; Vlachopoulos, D. Categorizing 10 Sports According to Bone and Soft Tissue Profiles in Adolescents. Med. Sci. Sports Exerc. 2020, 52, 2673–2681. [Google Scholar] [CrossRef]
- Discacciati, A.; Bellavia, A.; Lee, J.J.; Mazumdar, M.; Valeri, L. Med4way: A Stata command to investigate mediating and interactive mechanisms using the four-way effect decomposition. Int. J. Epidemiol. 2019, 48, 15–20. [Google Scholar] [CrossRef]
- Rauch, F.; Bailey, D.A.; Baxter-Jones, A.; Mirwald, R.; Faulkner, R. The “muscle-bone unit” during the pubertal growth spurt. Bone 2004, 34, 771–775. [Google Scholar] [CrossRef]
- Frost, H.M. Bone “mass” and the “mechanostat”: A proposal. Anat. Rec. 1987, 219, 1–9. [Google Scholar] [CrossRef]
- Bailey, D.A.; Baxter-Jones, A.D.G.; Mirwald, R.L.; Faulkner, R.A. Bone growth and exercise studies: The complications of maturation. J. Musculoskelet. Neuronal Interact. 2003, 3, 335–337. [Google Scholar]
- Luliano-Burns, S.; Mirwald, R.L.; Bailey, D.A. Timing and magnitude of peak height velocity and peak tissue velocities for early, average, and late maturing boys and girls. Am. J. Hum. Biol. 2001, 13, 1–8. [Google Scholar] [CrossRef]
- Guo, S.S.; Chumlea, W.C.; Roche, A.F.; Siervogel, R.M. Age- and maturity-related changes in body composition during adolescence into adulthood: The Fels Longitudinal Study. Int. J. Obes. Relat. Metab. Disord. 1997, 21, 1167–1175. [Google Scholar] [CrossRef] [Green Version]
- Cobayashi, F.; Lopes, L.A.; Taddei, J.A.A.C. Bone mineral density in overweight and obese adolescents. J. Pediatr. Rio J. 2005, 81, 337–342. [Google Scholar] [CrossRef]
- El Hage, R.P.; Courteix, D.; Benhamou, C.-L.; Jacob, C.; Jaffré, C. Relative importance of lean and fat mass on bone mineral density in a group of adolescent girls and boys. Eur. J. Appl. Physiol. 2009, 105, 759–764. [Google Scholar] [CrossRef]
- Schoenau, E.; Neu, C.M.; Rauch, F.; Manz, F. The development of bone strength at the proximal radius during childhood and adolescence. J. Clin. Endocrinol. Metab. 2001, 86, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Vlachopoulos, D.; Barker, A.R.; Ubago-Guisado, E.; Williams, C.A.; Gracia-Marco, L. The effect of a high-impact jumping intervention on bone mass, bone stiffness and fitness parameters in adolescent athletes. Arch. Osteoporos. 2018, 13, 128. [Google Scholar] [CrossRef] [Green Version]
- Forero-Bogotá, M.A.; Ojeda-Pardo, M.L.; García-Hermoso, A.; Correa-Bautista, J.E.; González-Jiménez, E.; Schmidt-RíoValle, J.; Navarro-Pérez, C.F.; Gracia-Marco, L.; Vlachopoulos, D.; Martínez-Torres, J.; et al. Body Composition, Nutritional Profile and Muscular Fitness Affect Bone Health in a Sample of Schoolchildren from Colombia: The Fuprecol Study. Nutrients 2017, 9, 106. [Google Scholar] [CrossRef]
- Lozano-Berges, G.; Matute-Llorente, Á.; González-Agüero, A.; Gómez-Bruton, A.; Gómez-Cabello, A.; Vicente-Rodríguez, G.; Casajús, J.A. Soccer helps build strong bones during growth: A systematic review and meta-analysis. Eur. J. Pediatr. 2018, 177, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Ito, I.H.; Kemper, H.C.G.; Agostinete, R.R.; Lynch, K.R.; Christofaro, D.G.D.; Ronque, E.R.; Fernandes, R.A. Impact of Martial Arts (Judo, Karate, and Kung Fu) on Bone Mineral Density Gains in Adolescents of Both Genders: 9-Month Follow-Up. Pediatr. Exerc. Sci. 2017, 29, 496–503. [Google Scholar] [CrossRef]
- Kohrt, W.M.; Bloomfield, S.A.; Little, K.D.; Nelson, M.E.; Yingling, V.R. American College of Sports Medicine American College of Sports Medicine Position Stand: Physical activity and bone health. Med. Sci. Sports Exerc. 2004, 36, 1985–1996. [Google Scholar] [CrossRef] [Green Version]
- Jürimäe, J.; Gruodyte-Raciene, R.; Baxter-Jones, A.D.G. Effects of Gymnastics Activities on Bone Accrual during Growth: A Systematic Review. J. Sports Sci. Med. 2018, 17, 245–258. [Google Scholar]
- Tenforde, A.S.; Fredericson, M. Influence of sports participation on bone health in the young athlete: A review of the literature. PMR 2011, 3, 861–867. [Google Scholar] [CrossRef]
- Eliakim, A.; Nemet, D.; Cooper, D.M. Exercise, Training and the GH-IGF-I Axis. In The Endocrine System in Sports and Exercise; Blackwell Publishing Ltd.: Oxford, UK, 2005; pp. 165–179. [Google Scholar]
- Constable, A.M.; Vlachopoulos, D.; Barker, A.R.; Moore, S.A.; Soininen, S.; Haapala, E.A.; Väistö, J.; Westgate, K.; Brage, S.; Mahonen, A.; et al. The independent and interactive associations of physical activity intensity and vitamin D status with bone mineral density in prepubertal children: The PANIC Study. Osteoporos. Int. 2021. [Google Scholar] [CrossRef]
- Kozieł, S.M.; Malina, R.M. Modified Maturity Offset Prediction Equations: Validation in Independent Longitudinal Samples of Boys and Girls. Sports Med. 2018, 48, 221–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natale, V.; Rajagopalan, A. Worldwide variation in human growth and the World Health Organization growth standards: A systematic review. BMJ Open 2014, 4, e003735. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 559) | Males (n = 401) Mean ± SD | Females (n = 157) Mean ± SD | p |
|---|---|---|---|
| Chronological age, years | 14.2 ± 2.0 | 14.0 ± 2.0 | 0.336 |
| Somatic maturation *, years | 0.69 ± 1.71 | 1.76 ± 1.67 | <0.001 |
| Age at PHV, years | 13.5 ± 0.6 | 12.3 ± 0.6 | <0.001 |
| Body mass, kg | 60.1 ± 15.3 | 53.1 ± 12.1 | <0.001 |
| Stature, cm | 168.4 ± 12.4 | 159.5 ± 8.9 | <0.001 |
| LST, kg | 45.5 ± 11.3 | 33.7 ± 5.4 | <0.001 |
| Body fat, kg | 10.8 ± 8.4 | 16.3 ± 8.7 | <0.001 |
| Upper limbs aBMD, g/cm2 | 0.813 ± 0.140 | 0.766 ± 0.091 | 0.003 |
| Lower limbs aBMD, g/cm2 | 1.286 ± 0.205 | 1.166 ± 0.118 | <0.001 |
| Spine aBMD, g/cm2 | 1.025 ± 0.173 | 1.078 ± 0.151 | <0.001 |
| TBLH aBMD, g/cm2 | 1.061 ± 0.155 | 0.995 ± 0.100 | <0.001 |
| Sport Group (n = 402) | Non-sport Group (n = 156) | ||
| Chronological age, years | 14.0 ± 1.9 | 14.4 ± 2.4 | 0.088 |
| Somatic maturation *, years | 0.97 ± 1.68 | 1.06 ± 1.97 | 0.555 |
| Age at PHV, years | 13.1 ± 0.8 | 13.3 ± 0.9 | <0.001 |
| Body mass, kg | 59.4 ± 14.8 | 54.8 ± 14.2 | 0.001 |
| Stature, cm | 166.9 ± 12.3 | 163.4 ± 11.8 | 0.004 |
| LST, kg | 43.7 ± 11.6 | 38.3 ± 9.7 | <0.001 |
| Body fat, kg | 12.1 ± 8.9 | 12.9 ± 8.8 | 0.381 |
| Upper limbs aBMD, g/cm2 | 0.813 ± 0.134 | 0.764 ± 0.112 | <0.001 |
| Lower limbs aBMD, g/cm2 | 1.279 ± 0.196 | 1.182 ± 0.164 | <0.001 |
| Spine aBMD, g/cm2 | 1.056 ± 0.162 | 0.997 ± 0.177 | <0.001 |
| TBLH aBMD, g/cm2 | 1.063 ± 0.146 | 0.989 ± 0.127 | <0.001 |
| LST | Upper Limbs aBMD | Lower Limbs aBMD | Spine aBMD | TBLH aBMD | |
|---|---|---|---|---|---|
| r/p-Value | r/p-Value | r/p-Value | r/p-Value | r/p-Value | |
| Somatic Maturation | |||||
| Males | 0.898/<0.001 | 0.731/<0.001 | 0.818/<0.001 | 0.744/<0.001 | 0.820/0.001 |
| Females | 0.593/<0.001 | 0.554/<0.001 | 0.576/<0.001 | 0.619/<0.001 | 0.599/<0.001 |
| Sport group | 0.920/<0.001 | 0.690/<0.001 | 0.792/<0.001 | 0.680/<0.001 | 0.781/<0.001 |
| Non-sport group | 0.813/<0.001 | 0.648/0.001 | 0.647/<0.001 | 0.719/<0.001 | 0.665/<0.001 |
| LST | |||||
| Males | -- | 0.770/<0.001 | 0.840/<0.001 | 0.771/<0.001 | 0.863/<0.001 |
| Females | -- | 0.683/<0.001 | 0.704/<0.001 | 0.609/<0.001 | 0.744/<0.001 |
| Sport group | -- | 0.681/<0.001 | 0.757/<0.001 | 0.647/<0.001 | 0.761/<0.001 |
| Non-Sport group | -- | 0.700/<0.001 | 0.735/<0.001 | 0.701/<0.001 | 0.750/<0.001 |
| Total Effect | Controlled Direct Effect | Reference Interaction | Mediated Interaction | Pure Indirect Effect | |
|---|---|---|---|---|---|
| aBMD Males | |||||
| Upper limbs | 0.00602 (0.00548 to 0.00657) | 0.00176 (0.00081 to 0.00271) | −0.00005 (−0.00011 to 0.00053) | 0.00005 (0.00003 to 0.00007) | 0.00427 (0.00343 to 0.00510) |
| Lower limbs | 0.00892 (0.00821 to 0.00963) | 0.00284 (0.00163 to 0.00406) | −0.00002 (−0.00006 to 0.00002) | 0.00002 (−0.00001 to 0.00005) | 0.00608 (0.00500 to 0.00716) |
| Spine | 0.00720 (0.00653 to 0.00788) | 0.00200 (0.00081 to 0.00319) | −0.00001 (−0.00004 to 0.00002) | 0.00001 (−0.00002 to 0.00004) | 0.00520 (0.00416 to 0.00625) |
| TBLH | 0.00690 (0.00637 to 0.00743) | 0.00170 (0.00084 to 0.00256) | −0.00002 (−0.00006 to 0.00083) | 0.00002 (0.000002 to 0.00005) | 0.00520 (0.00442 to 0.00598) |
| aBMD Females | |||||
| Upper limbs | 0.00304 (0.00233 to 0.00376) | 0.00125 (0.00049 to 0.00201) | 0.00001 (−0.00003 to 0.00004) | −0.00001 (−0.00003 to 0.00001) | 0.00179 (0.00120 to 0.00238) |
| Lower limbs | 0.00409 (0.00317 to 0.00501) | 0.00172 (0.00076 to 0.00267) | 0.00001 (−0.00003 to 0.00005) | −0.00001 (−0.00003 to 0.00001) | 0.00237 (0.00162 to 0.00313) |
| Spine | 0.00558 (0.00447 to 0.00670) | 0.00356 (0.00227 to 0.00484) | 0.00003 (−0.00007 to 0.00013) | −0.00003 (−0.00006 to 0.00001) | 0.00203 (0.00115 to 0.00290) |
| TBLH | 0.00361 (0.00285 to 0.00436) | 0.00145 (0.00069 to 0.00220) | 0.00001 (−0.00003 to 0.00005) | −0.00001 (−0.00003 to 0.00001) | 0.00216 (0.00152 to 0.00279) |
| Total Effect | Controlled Direct Effect | Reference Interaction | Mediated Interaction | Pure Indirect Effect | |
|---|---|---|---|---|---|
| aBMD | |||||
| Sport group | |||||
| Upper limbs | 0.00592 (0.00536 to 0.00648) | 0.00211 (0.00123 to 0.00299) | −0.00005 (−0.00010 to 0.00033) | 0.00005 (0.00002 to 0.00007) | 0.00381 (0.00306 to 0.00456) |
| Lower limbs | 0.00885 (0.00814 to 0.00957) | 0.00350 (0.00241 to 0.00459) | −0.00003 (−0.00007 to 0.00001) | 0.00003 (−0.000003 to 0.00006) | 0.00535 (0.00441 to 0.00630) |
| Spine | 0.00702 (0.00631 to 0.00773) | 0.00271 (0.00156 to 0.00285) | −0.000004 (−0.00004 to 0.00003) | 0.000004 (−0.00005 to 0.00003) | 0.00431 (0.00335 to 0.00527) |
| TBLH | 0.00688 (0.00634 to 0.00741) | 0.00237 (0.00159 to 0.00315) | −0.00002 (−0.00005 to 0.00001) | 0.00002 (0.000001 to 0.00004) | 0.00451 (0.00381 to 0.00520) |
| Non-sport group | |||||
| Upper limbs | 0.00041 (0.00034 to 0.00048) | 0.00013 (0.00003 to 0.00023) | −0.0000001 (−0.000002 to 0.000002) | 0.0000001 (−0.0000002 to 0.0000003) | 0.00028 (0.00020 to 0.00036) |
| Lower limbs | 0.00056 (0.00046 to 0.00066) | 0.00008 (−0.00005 to 0.00021) | 0.0000002 (−0.000005 to 0.000006) | −0.0000002 (−0.000001 to 0.0000001) | 0.00048 (0.00036 to 0.00060) |
| Spine | 0.00064 (0.00054 to 0.00074) | 0.00031 (0.00016 to 0.00046) | 0.0000002 (−0.000006 to 0.000006) | 0.0000002 (−0.0000006 to 0.0000001) | 0.00033 (0.00021 to 0.00045) |
| TBLH | 0.00046 (0.00038 to 0.00054) | 0.00008 (−0.00002 to 0.00018) | 0.0000001 (−0.000003 to 0.000003) | −0.0000001 (−0.0000004 to 0.0000001) | 0.00038 (0.00029 to 0.00047) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agostinete, R.R.; Werneck, A.O.; Maillane-Vanegas, S.; Gracia-Marco, L.; Ubago-Guisado, E.; Constable, A.M.; Fernandes, R.A.; Vlachopoulos, D. The Mediating Role of Lean Soft Tissue in the Relationship between Somatic Maturation and Bone Density in Adolescent Practitioners and Non-Practitioners of Sports. Int. J. Environ. Res. Public Health 2021, 18, 3008. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063008
Agostinete RR, Werneck AO, Maillane-Vanegas S, Gracia-Marco L, Ubago-Guisado E, Constable AM, Fernandes RA, Vlachopoulos D. The Mediating Role of Lean Soft Tissue in the Relationship between Somatic Maturation and Bone Density in Adolescent Practitioners and Non-Practitioners of Sports. International Journal of Environmental Research and Public Health. 2021; 18(6):3008. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063008
Chicago/Turabian StyleAgostinete, Ricardo R., André O. Werneck, Santiago Maillane-Vanegas, Luis Gracia-Marco, Esther Ubago-Guisado, Annie M. Constable, Romulo A. Fernandes, and Dimitris Vlachopoulos. 2021. "The Mediating Role of Lean Soft Tissue in the Relationship between Somatic Maturation and Bone Density in Adolescent Practitioners and Non-Practitioners of Sports" International Journal of Environmental Research and Public Health 18, no. 6: 3008. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063008