
The Effect of a High-Intensity PrO2Fit Inspiratory Muscle Training Intervention on Physiological and Psychological Health in Adults with Bronchiectasis: A Mixed-Methods Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inspiratory Muscle Training Intervention
2.2. Anthropometrics
2.3. Physiological Measures
2.4. Psychological Measurements
2.5. Data Analysis
2.5.1. Cardiopulmonary Exercise Testing and Supramaximal Verification
2.5.2. Interview Analysis
2.6. Statistical Analysis
3. Results
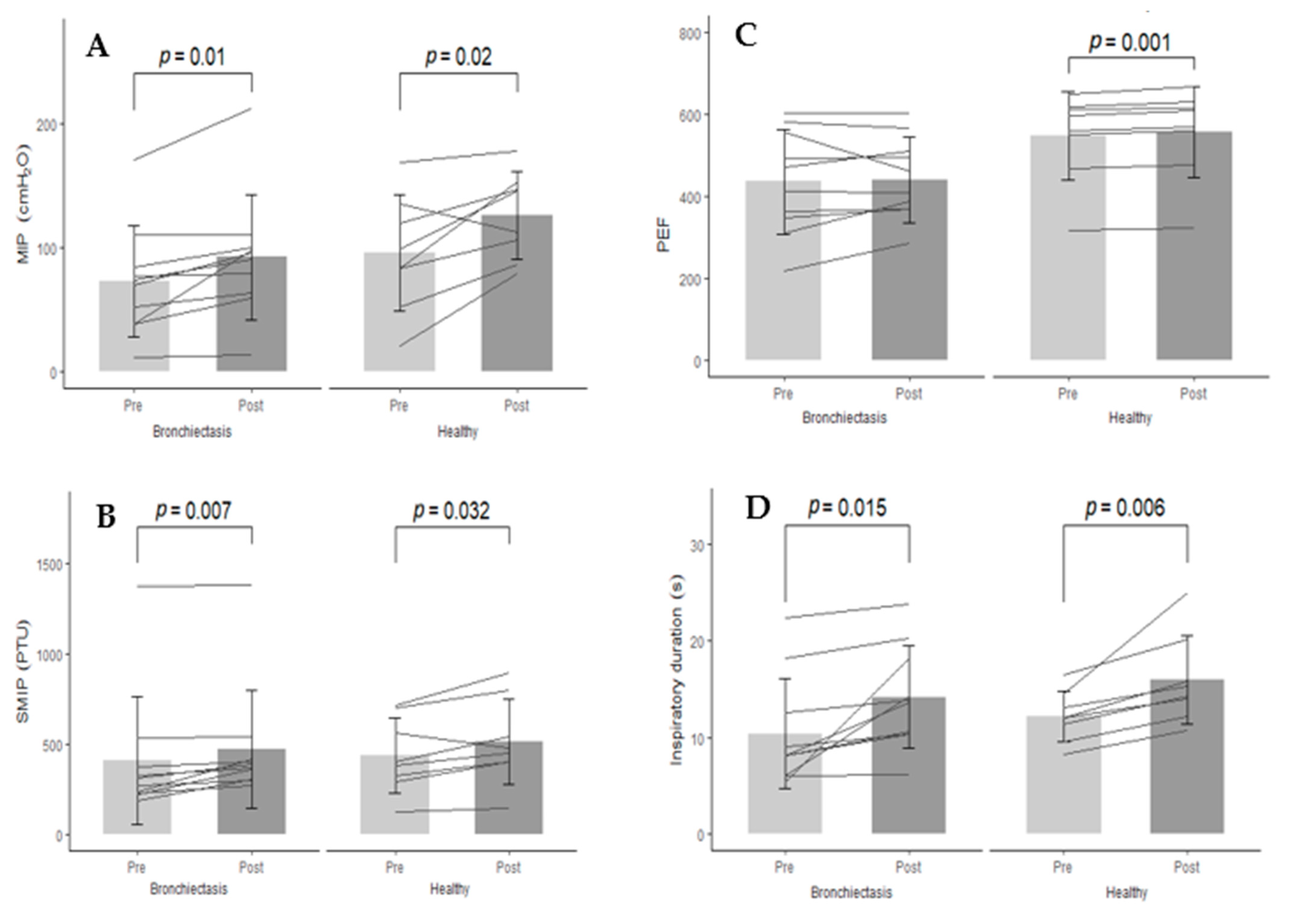
3.1. Effects of Inspiratory Muscle Training
3.2. Eight-Week Top-Up Period
3.3. Qualitative Experiences
3.3.1. Relationship with Physical Activity and Exercise
Positives
“I love walking the dogs, because it gets you out into the open air… it is good for you mentally as well I think. It does make you feel better doesn’t it? You feel very virtuous when you’ve done some [physical activity].”[B10]
“I like the freedom of it… I find it really helpful for my mental health. The knowledge that my body is capable of doing things. I like the sense of achievement.”[H1]
Barriers to Exercise
“Having this bronchiectasis limits the amount of physical activity and exercise I can do… I look forward to it [physical activity and exercise] mentally, but I am very much aware of my limitations very soon… I wish I could do a lot more walking and I would really enjoy that much more if I could.”[B3]
“I’ve got to take my time on everything, but anything that’s up and down, I mean like the stairs, up is physical, but down is just as hard.”[B1]
“I don’t enjoy it [physical activity], I haven’t got the time to do it. It’s time more than anything [that is a barrier], you come home from work and you’re tired, you don’t want to start doing exercises.”[B6]
“Time is always the biggest one [barrier to exercise and physical activity]. It always is isn’t it? Time and mental sort of motivation… One of the downsides of my job is that I’m spending a lot of time sitting down. I’ve come from a previously very active job… to then go to a really sedentary job has been really hard and that’s really affected my activity.”[H5]
Motivations to Exercise
“Since the diagnosis I realise I need to be more active in order to keep my lungs healthy and the sputum moving around... So, the more active you are the better it [bronchiectasis] is. I try to be a little bit more active, whereas before [diagnosis] I might have thought ‘I won’t do any exercise tonight’, I think ‘right I’ve got to do it because of the bronchiectasis’.”[B10]
“The idea, certainly with the grandchildren, is to be as fit as you can around them so that you can keep up with them! It has been quite physically demanding [looking after the grandchildren].”[B8]
“The benefit [of exercising] is I know it is good for me. It’s probably the best drug in the world, if you could bottle it. I do it for my own health and that it makes me feel better about myself.”[H5]
External Influences
“I think there is a moral obligation to exercise and at least remain healthy, because it matters to other people what happens to us. Obesity and smoking causes demand on the health service… problems just get worse as you get older and then it drags other people in because they have to look after you… It’s a drag on your friends and relatives and you have to consider the effect of your own decisions on other people.”[H9]
“It depends who you hang around with. If you hang around with lots of sports people you tend to learn off your group. Whereas, if you haven’t got that social side to it, then maybe you won’t exercise as much.”[H1]
“If I wasn’t particularly active, I think I would feel guilty. I don’t know if that is something that is put on me myself or more because of the media aspect… I’m probably going to have more health complications, probably going to be overweight. I don’t know if it is a societal thing or a personal thing [pressure to be active], but I’d feel guilty if I didn’t [exercise].”[H1]
3.3.2. Inspiratory Muscle Training Intervention
Enjoyment
“I was looking forward to doing it, because I want to do anything that’s going to help. I’ve been so poorly with my chest this year that anything that will help, I will try.”[B2]
Motivations
“I was determined, I wanted to do this [IMT]… the main reason is that it gives me that discipline, I am more than happy to follow a training programme and then the motivation followed ‘I will do this’.”[B3]
“They [decreasing rest times] were good. That really set a goal for you, you know. It was hard, but I was motivated to do it, it did push you a bit more!”[B1]
“That made it harder at the time [levels and decreasing rest times]. I think it was good, it kept it more engaging… it kind of has a reward element to it, I suppose.”[H9]
“Less motivated to do it [IMT] than I am to do exercise. I think once you’ve done exercise you feel good about it afterwards, you feel like you have achieved something. Whereas, after doing the PrO2 training, it just felt like something that I had to do, I had to get through, but no reward at the end.”[H1]
“I’m guessing you might get more significant results if someone sort of sedentary was using it. I don’t feel like it was helping me in anything other than being able to do the test better.”[H6]
Accessibility
“If I had to go somewhere to use it, I probably would not have done it… I would have had to have made more of an effort and having something small and portable, why would I want to go somewhere else with it?... Having it at home I can do it easily”[B4]
“I think it’s better to have it at home than having it elsewhere, it would never have worked [training elsewhere]… It’s just convenient really, doing it at your own time at your own pace without anyone watching.”[H2]
“It’s quite portable and convenient as opposed to setting an hour of your day aside to physically go and do exercise… It’s a lot more flexible in terms of time of day or motivation. You can adapt to it quite well.”[H10]
Feedback
“You can set your goals then… I found having that sort of feedback was very helpful”[B7]
“It [feedback] changed my behaviour for the better, I was aiming for something, I knew what I was meant to be doing. I think having that goal in mind helps the person try and exercise.”[H7]
“It is nice to know how you are doing, but it’s also nice to have something to compete against. If somebody would have asked me before ‘are you competitive’? I would have said no, not really, but yes, in this instance I certainly am!”[B5]
“You wouldn’t have pushed yourself as much [if you didn’t have the visual feedback]”[B4]
“I wouldn’t have tried as hard because you don’t know how you’ve done. You wouldn’t be as motivated to try then.”[H2]
“Then I got really frustrated if I couldn’t get to the end.”[H4]
3.3.3. Perceived Improvements
“I’m not doing anything different in my life other than using the device… Some of the things I do now, the recovery time after doing them is about half [the recovery time] was before. I have never got this far into a winter without a cold turning into a chest infection. My lungs aren’t producing the same levels of mucus as they typically do which is a great improvement. Physically I’m feeling better, now that’s [IMT] got to be worth doing.”[B8]
“My stamina has got better I would say that, I was quite pleased with that actually. I found it easier walking up the stairs, I was fitter. It’s all hills round me and two months ago I wouldn’t have been able to do an hour [walk]… but now it’s ok!”[B1]
“What I like about it was that it helped me to clear a lot of sputum much better than the Acapella [an airway clearance device]… I haven’t had any infections, and this is my tenth week without antibiotics or infection. I think my record before was three weeks!... When you have bronchiectasis, as long as you can keep your lungs clear, happy days. That is the most important thing.”[B2]
“I definitely think my lung capacity is improved… I decided to go for a little run and I was really shocked my breathing had improved… I definitely felt the benefit from it, which was surprising actually. I think it has definitely made a difference. I know a couple of friends of mine are quite jealous.”[H10]
“There’s definitely been an improvement in my training over time, but I don’t know whether that was necessarily because of this device.”[H5]
3.3.4. Future Improvements
Adherence
“Tiresome three times a week… it was getting to be a bit of a pain after eight weeks… Possibly if it could get condensed to fit into your lifestyle more.”[B4]
“If you could condense it into a shorter training period, that would definitely help in making me complete more sessions.”[H5]
Extrinsic Feedback
“I would have liked something like a smiley face or a ‘hip hip hooray! You’ve done it, well done’!”[B1]
“I think from a sort of motivation point of view, it may sound silly, but just to have a ‘well done, that was better than last time, you’ve improved this much,’ ‘you’re nearly there, keep on going,’ and ‘you’re doing better than you have previously done.’ So, that would help motivate you.”[H6]
“If it set you targets to achieve within a certain period. That would make it far more worthwhile.”[B4]
“You could have a set target from the data… you know ‘can I get closer to the target’? Without targets, it was difficult to know what you could improve on or whether you were improving.”[H9]
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Onen, Z.P.; Gulbay, B.E.; Sen, E.; Yildiz, Ö.A.; Saryal, S.; Acican, T.; Karabiyikoglu, G. Analysis of the factors related to mortality in patients with bronchiectasis. Respir. Med. 2007, 101, 1390–1397. [Google Scholar] [CrossRef] [Green Version]
- Ozalp, O.; Inal-Ince, D.; Calik, E.; Vardar-Yagli, N.; Saglam, M.; Savci, S.; Arikan, H.; Bosnak-Guclu, M.; Coplu, L. Extrapulmonary features of bronchiectasis: Muscle function, exercise capacity, fatigue, and health status. Multidiscip. Respir. Med. 2012, 7, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, P.J. Inflammation: A two-edged sword—The model of bronchiectasis. Eur. J. Respir. Dis. Suppl. 1986, 147, 6–15. [Google Scholar]
- Koulouris, N.; Retsou, S.; Kosmas, E.; Dimakou, K.; Malagari, K.; Mantzikopoulos, G.; Koutsoukou, A.; Milic-Emili, J.; Jordanoglou, J. Tidal expiratory flow limitation, dyspnoea and exercise capacity in patients with bilateral bronchiectasis. Eur. Respir. J. 2003, 21, 743–748. [Google Scholar] [CrossRef] [Green Version]
- Newall, C.; Stockley, R.A.; Hill, S.L. Exercise training and inspiratory muscle training in patients with bronchiectasis. Thorax 2005, 60, 943–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozalp, O.; Inal-Ince, D.; Cakmak, A.; Calik-Kutukcu, E.; Saglam, M.; Savci, S.; Vardar-Yagli, N.; Arikan, H.; Karakaya, J.; Coplu, L. High-intensity inspiratory muscle training in bronchiectasis: A randomized controlled trial. Respirology 2018, 24, 246–253. [Google Scholar] [CrossRef]
- Liaw, M.-Y.; Wang, Y.-H.; Tsai, Y.-C.; Huang, K.-T.; Chang, P.-W.; Chen, Y.-C.; Lin, M.-C. Inspiratory muscle training in bronchiectasis patients: A prospective randomized controlled study. Clin. Rehabil. 2011, 25, 524–536. [Google Scholar] [CrossRef] [PubMed]
- Moran, F.; Piper, A.; Elborn, J.S.; Bradley, J.M. Respiratory muscle pressures in non-CF bronchiectasis: Repeatability and reliability. Chronic Respir. Dis. 2010, 7, 165–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troosters, T.; Gosselink, R.; Decramer, M. Respiratory muscle assessment. In Lung Function Testing: European Respiratory Monograph; Gosselink, R., Stam, H., Eds.; European Respiratory Society Journals Ltd.: Sheffield, UK, 2005; pp. 57–72. [Google Scholar]
- Hoffman, M.; Assis, M.G.; Augusto, V.M.; Silveira, B.M.F.; Parreira, V.F. The effects of inspiratory muscle training based on the perceptions of patients with advanced lung disease: A qualitative study. Braz. J. Phys. Ther. 2018, 22, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Sinnerton, J.; Gillen, P. Exploring people’s perceptions of a pulmonary rehabilitation program and maintenance options. J. Nurs. Health Chronic Illn. 2009, 1, 229–236. [Google Scholar] [CrossRef]
- Wanke, T.; Formanek, D.; Lahrmann, H.; Brath, H.; Wild, M.; Wagner, C.; Zwick, H. Effects of combined inspiratory muscle and cycle ergometer training on exercise performance in patients with COPD. Eur. Respir. J. 1994, 7, 2205–2211. [Google Scholar] [CrossRef] [Green Version]
- Weiner, P.; Azgad, Y.; Ganam, R. Inspiratory Muscle Training Combined with General Exercise Reconditioning in Patients with COPD. Chest 1992, 102, 1351–1356. [Google Scholar] [CrossRef]
- Hill, K.; Jenkins, S.C.; Philippe, D.L.; Cecins, N.; Shepherd, K.L.; Green, D.J.; Hillman, D.R.; Eastwood, P.R. High-intensity inspiratory muscle training in COPD. Eur. Respir. J. 2006, 27, 1119–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturdy, G.; Hillman, D.; Green, D.; Jenkins, S.; Cecins, N.; Eastwood, P. Feasibility of High-Intensity, Interval-Based Respiratory Muscle Training in COPD. Chest 2003, 123, 142–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Valero, R.; Jimenez-Cebrian, A.M.; Moral-Munoz, J.A.; De-la-Casa-Almelda, M.; Rodriguez-Huguet, M.; Casuso-Holgado, M. The Efficacy of Therapeutic Respiratory Muscle Training Interventions in People with Bronchiectasis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-García, M.A.; Perpiñá-Tordera, M.; Román-Sánchez, P.; Soler-Cataluña, J.J. Quality-of-life determinants in patients with clinically stable bronchiectasis. Chest 2005, 128, 739–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’leary, C.J.; Wilson, C.B.; Hansell, D.M.; Cole, P.J.; Wilson, R.; Jones, P.W. Relationship between psychological well-being and lung health status in patients with bronchiectasis. Respir. Med. 2002, 96, 686–692. [Google Scholar] [CrossRef] [Green Version]
- Cahalin, L.P.; Arena, R.; Guazzi, M.; Myers, J.; Cipriano, G.; Chiappa, G.; Lavie, C.J.; Forman, D.E. Inspiratory muscle training in heart disease and heart failure: A review of the literature with a focus on method of training and outcomes. Expert Rev. Cardiovasc. Ther. 2013, 11, 161–177. [Google Scholar] [CrossRef]
- Weiner, P.; Magadle, R.; Beckerman, M.; Weiner, M.; Berar-Yanay, N. Maintenance of inspiratory muscle training in COPD patients: One year follow-up. Eur. Respir. J. 2004, 23, 61–65. [Google Scholar] [CrossRef] [Green Version]
- Formiga, M.F.; Campos, M.A.; Cahalin, L.P. Inspiratory Muscle Performance of Former Smokers and Nonsmokers Using the Test of Incremental Respiratory Endurance. Respir. Care 2018, 63, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Cahalin, L.; Ross, A. Novel methods of inspiratory muscle training via the Test of Incremental Respiratory Endurance (TIRE). Exerc. Sport Sci. Rev. 2015, 43, 84–92. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quanjer, P.; Stanojevic, S.; Cole, T.; Baur, X.; Hall, G.; Culver, B.; Enright, P.; Hankinson, J.L.; Ip, M.S.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.; Linderholm, H. Perceived Exertion and Pulse Rate during Graded Exercise in Various Age Groups. Acta Me. Scand. 2009, 181, 194–206. [Google Scholar] [CrossRef]
- Williams, G.C.; Saizow, R.B.; Ryan, R.M. The importance of self-determination theory for medical education. Acad. Med. 1999, 74, 992–995. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.Y.Y.; Ntoumanis, N.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Duda, J.L.; Williams, G.C. Self-Determination Theory Applied to Health Contexts. Perspect. Psychol. Sci. 2012, 7, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaer4obic threshold by gas exchange. J. Appl. Physiol. 1985, 60, 2020–2027. [Google Scholar] [CrossRef] [PubMed]
- Causer, A.J.; Shute, J.K.; Cummings, M.H.; Shepherd, A.I.; Bright, V.; Connett, G.; Allenby, M.I.; Carroll, M.P.; Daniels, T.; Saynor, Z.L. Cardiopulmonary exercise testing with supramaximal verification produces a safe and valid assessment of Vo2max in people with cystic fibrosis: A retrospective analysis. J. Appl. Physiol. 2018, 125, 1277–1283. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. What can “thematic analysis” offer health and wellbeing researchers? Int. J. Qual. Stud. Health Well-Being 2014, 9, 26152. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Boddy, L.M.; Knowles, Z.R.; Davies, I.G.; Warburton, G.L.; Mackintosh, K.A.; Houghton, L.; Fairclough, S.J. Using formative research to develop the healthy eating component of the CHANGE! school-based curriculum intervention. BMC Public Health 2012, 12, 710. [Google Scholar] [CrossRef] [Green Version]
- Mackintosh, K.A.; Knowles, Z.R.; Ridgers, N.D.; Fairclough, S.J. Using formative research to develop CHANGE! A curriculum-based physical activity promoting intervention. BMC Public Health 2011, 11, 831. [Google Scholar] [CrossRef] [Green Version]
- Bekhet, A.K.; Zauszniewski, J.A. Methodological triangulation: An approach to understanding data. Nurse Res. 2012, 20, 40–43. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Anlysis for the Behavioural Sciences (Revised); Academic Press: Cambridge, MA, USA, 1988. [Google Scholar]
- Harver, A.; Mahler, D.; Daubenspeck, J. Targeted Inspiratory Muscle Training Improves Respiratory Muscle Function and Reduced Dyspnea in Patients with Chronic Obstructive Pulmonary disease. Ann. Intern. Med. 1989, 111, 117–124. [Google Scholar] [CrossRef]
- Enright, S.; Chatham, K.; Ionescu, A.A.; Unnithan, V.B.; Shale, D.J. Inspiratory Muscle Training Improves Lung Function and Exercise Capacity in Adults With Cystic Fibrosis. Chest 2004, 126, 405–411. [Google Scholar] [CrossRef]
- Jamaati, H.R.; Heshmat, B.; Tamadon, R.; Rad, A.H.; Mohajerani, S.A.; Radmand, G.; Hashemian, S.M.R. Asso-ciation between Severity of Chronic Obstructive Pulmonary Disease and Lung Function Tests. Tanaffos 2013, 12, 36–41. [Google Scholar]
- Nambiar, V.; Ravindra, S.; Kumar, B.N. Maximal inspiratory and expiratory pressures in men with chronic obstructive pulmonary disease: A cross-sectional study. Indian J. Respir. Care 2018, 7, 88. [Google Scholar] [CrossRef]
- Severin, R.; Arena, R.; Lavie, C.J.; Bond, S.; Phillips, S.A. Respiratory Muscle Performance Screening for Infectious Disease Management Following COVID-19: A Highly Pressurized Situation. Am. J. Med. 2020, 133, 1025–1032. [Google Scholar] [CrossRef] [PubMed]
- Formiga, M.F.; Roach, K.E.; Vital, I.; Urdaneta, G.; Balestrini, K.; Calderon-Candelario, R.A.; Campos, M.A.; Cahalin, L.P. Reliability and validity of the test of incremental respiratory endurance measures of inspiratory muscle performance in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 1569–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Formiga, M.F.; Vital, I.; Urdaneta, G.; Balestrini, K.; Cahalin, L.P.; Campos, M.A. The BODE index and inspiratory muscle performance in COPD: Clinical findings and implications. SAGE Open Med. 2018, 6, 1–7. [Google Scholar] [CrossRef]
- Paolillo, S.; Agostoni, P. Prognostic Role of Cardiopulmonary Exercise Testing in Clinical Practice. Ann. Am. Thorac. Soc. 2017, 14, S53–S58. [Google Scholar] [CrossRef]
- Houghton, A.R.; Harrison, M.; Cowley, A.J.; Hampton, J.R. Assessing exercise capacity, quality of life and haemodynamics in heart failure: Do the tests tell us the same thing? Eur. J. Hear. Fail. 2002, 4, 289–295. [Google Scholar] [CrossRef] [Green Version]
- Crapo, R.O.; Casaburi, R.; Coates, A.L.; Enright, P.L.; MacIntyre, N.R.; McKay, R.T.; Johnson, D.; Wanger, J.S.; Zeballos, R.J.; Bittner, V.; et al. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. Res. Involv. Engag. 2015, 1, 1–9. [Google Scholar] [CrossRef]
- Vollaard, N.B.J.; Constantin-Teodosiu, D.; Fredriksson, K.; Rooyackers, O.; Jansson, E.; Greenhaff, P.L.; Timmons, J.A.; Sundberg, C.J. Systematic analysis of adaptations in aerobic capacity and submaximal energy metabolism provides a unique insight into determinants of human aerobic performance. J. Appl. Physiol. 2009, 106, 1479–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Supple, D.; Roberts, A.; Hudson, V.; Masefield, S.; Fitch, N.; Rahmen, M.; Flood, B.; De Boer, W.; Powell, P.; Wagers, S. From tokenism to meaningful engagement: Best practices in patient involvement in an EU project. Res. Involv. Engag. 2015, 1, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Dudgeon, E.K.; Crichton, M.; Chalmers, J.D. “The missing ingredient”: The patient perspective of health- related quality of life in bronchiectasis: A qualitative study. BMC Pulm. Med. 2018, 18, 81. [Google Scholar] [CrossRef]
- Manganello, J.A. Health literacy and adolescents: A framework and agenda for future research. Health Educ. Res. 2007, 23, 840–847. [Google Scholar] [CrossRef]
- Williams, G.C.; McGregor, H.A.; Zeldman, A.; Freedman, Z.R.; Deci, E.L. Testing a Self-Determination Theory Process Model for Promoting Glycemic Control Through Diabetes Self-Management. Health Psychol. 2004, 23, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Kinoshita, K.; MacIntosh, E.; Sato, S. The Relationship between Avoidance Goals and Goal Attainment: A Moderated Mediation Analysis. Res. Q. Exerc. Sport 2019, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Denford, S.; Van Beurden, S.; O’Halloran, P.; Williams, C.A. Barriers and facilitators to physical activity among children, adolescents, and young adults with cystic fibrosis: A systematic review and thematic synthesis of qualitative research. BMJ Open 2020, 10, e035261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, A.R.; Tunney, M.M.; Quittner, A.L.; Elborn, J.S.; Bradley, J.M.; Hughes, C.M. Treatment adherence and health outcomes in patients with bronchiectasis. BMC Pulm. Med. 2014, 14, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, J.E. Novel Physiotherapy Devices in Cystic Fibrosis and Bronchiectasis: Efficacy of TIRE and AcapellaÒ. Ph.D. Thesis, University of Ulster, Antrim, UK, 2005. [Google Scholar]
- Kim, C.S.; Iglesias, A.J.; Sackner, M.A. Mucus clearance by two-phase gas-liquid flow mechanism: Asymmetric periodic flow model. J. Appl. Physiol. 1987, 62, 959–971. [Google Scholar] [CrossRef] [PubMed]
- Naraparaju, S.; Vaishali, K.; Venkatesan, P.; Acharya, V. A comparison of the Acapella and a threshold inspiratory muscle trainer for sputum clearance in bronchiectasis—A pilot study. Physiother. Theory Pract. 2010, 26, 353–357. [Google Scholar] [CrossRef]
- Goeminne, P.C.; Hernandez, F.; Diel, R.; Filonenko, A.; Hughes, R.; Juelich, F.; Solomon, G.M.; Upton, A.; Wichmann, K.; Xu, W.; et al. The economic burden of bronchiectasis—Known and unknown: A systematic review. BMC Pulm. Med. 2019, 19, 54. [Google Scholar] [CrossRef] [Green Version]
- Chalmers, J.D.; Aliberti, S.; Blasi, F. Management of bronchiectasis in adults. Eur. Respir. J. 2015, 45, 1446–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaton, D.E.; Boers, M.; Wells, G.A. Many faces of the minimal clinically important difference (MCID): A literature review and directions for future research. Curr. Opin. Rheumatol. 2002, 14, 109–114. [Google Scholar] [CrossRef]
- ModiCrystal, A.C.; Lim, C.S.; Driscoll, K.A.; Piazza-Waggoner, C.; Quittner, A.L.; Wooldridge, J. Changes in Pediatric Health-Related Quality of Life in Cystic Fibrosis After IV Antibiotic Treatment for Pulmonary Exacerbations. J. Clin. Psychol. Med. Settings 2010, 17, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Ranganathan, P.; Pramesh, C.S.; Buyse, M. Common pitfalls in statistical analysis: Clinical versus statistical significance. Perspect. Clin. Res. 2015, 6, 169–170. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total (n = 18) | Bronchiectasis (n = 10) | Healthy (n = 8) | p Value |
|---|---|---|---|---|
| Anthropometrics | ||||
| Age (years) | 51.9 ± 17.2 | 64.5 ± 10.3 | 36.1 ± 8.5 | <0.05 * |
| Sex (female/male) | (5/13) | (3/7) | (2/6) | 0.886 |
| Height (cm) | 172.6 ± 10.9 | 169.5 ± 11.2 | 176.4 ± 9.7 | 0.183 |
| Weight (kg) | 76.9 ± 16.8 | 81.2 ± 19.7 | 71.5 ± 11.2 | 0.238 |
| BMI (kg·m−2) | 25.8 ± 5.5 | 28.3 ± 6.3 | 22.8 ± 1.8 | 0.024 * |
| WHR (cm) | 1.0 ± 0.1 | 1.0 ± 0.1 | 0.9 ± 0.6 | 0.106 |
| Parameters | Mean Difference from Baseline–8 Weeks (n = 10) | % of Participants with Clinically Significant Increase | % of Participants with Clinically Significant Decrease | Effect Size | Mean Difference from 8 Weeks–16 Weeks (n = 3) | % of Participants with Clinically Significant Increase | % of Participants with Clinically Significant Decrease | Effect Size |
|---|---|---|---|---|---|---|---|---|
| Lung Function | ||||||||
| MIP (cmH2O) | 19.6 ± 18.9 * | 40% | 0% | 0.4 | 23.7 ± 27.5 | 0% | 33% | 0.5 |
| MEP (cmH2O) | 3.2 ± 20.3 | 20% | 10% | 0.1 | 4.7 ± 4.1 | 0% | 0% | 0.2 |
| SMIP (PTU) | 66.1 ± 57.8 * | 50% | 0% | 0.7 | 65.8 ± 57.6 | 0% | 0% | 0.2 |
| ID (s) | 3.8 ± 4.0 * | 60% | 0% | 0.2 | 3.4 ± 4.1 | 0% | 0% | 0.1 |
| FEV1 (l) | 0.01 ± 0.2 | 0% | 0% | 0.01 | 0.1 ± 0.1 | 0% | 0% | −0.1 |
| FEV1 %predicted | 0.4 ± 11.7 | 30% | 60% | 0.02 | 7.0 ± 6.7 | 67% | 0% | 0.5 |
| FVC (l) | 0.01 ± 0.2 | 10% | 0% | −0.02 | 0.1 ± 0.1 | 0% | 0% | −0.2 |
| FVC %predicted | −2.0 ± 14.1 | 40% | 40% | −0.2 | 9.0 ± 13.1 | 33% | 0% | 0.9 |
| PEF (L·min−1) | 5.0 ± 49.7 | 20% | 10% | 0.04 | 5.0 ± 9.5 | 0% | 0% | −0.04 |
| FEV1/FVC | 2.1 ± 10.2 | 10% | 0% | 0.1 | 1.3 ± 1.5 | 0% | 0% | 0.1 |
| Exercise Capacity | ||||||||
| Vo2 max (ml·kg−1·min−1) | 0.1 ± 1.7 | 10% | 10% | −0.04 | 4.3 ± 5.1 | 0% | 100% | 2.0 |
| 8 Weeks | 95% Confidence Interval | p Value between Groups | |||||
|---|---|---|---|---|---|---|---|
| Bronchiectasis | Healthy | Mean Difference | SEM | Lower | Upper | ||
| Treatment Self-Regulation | |||||||
| Autonomous | 4.9 ± 1.4 * | 2.1 ± 0.7 | 2.8 | 0.5 | 1.7 | 4.0 | <0.01 * |
| Controlled | 1.7 ± 0.7 | 1.5 ± 0.3 | 0.2 | 0.3 | −0.4 | 0.8 | 0.411 |
| Amotivation | 1.4 ± 0.6 | 4.3 ± 0.4 * | −2.9 | 0.3 | −3.4 | −2.4 | <0.01 * |
| Perceived Competence | 5.5 ± 1.3 * | 4.6 ± 1.1 | 0.9 | 0.6 | −0.31 | 2.1 | 0.128 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McCreery, J.L.; Mackintosh, K.A.; Mills-Bennett, R.; McNarry, M.A. The Effect of a High-Intensity PrO2Fit Inspiratory Muscle Training Intervention on Physiological and Psychological Health in Adults with Bronchiectasis: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 3051. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063051
McCreery JL, Mackintosh KA, Mills-Bennett R, McNarry MA. The Effect of a High-Intensity PrO2Fit Inspiratory Muscle Training Intervention on Physiological and Psychological Health in Adults with Bronchiectasis: A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2021; 18(6):3051. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063051
Chicago/Turabian StyleMcCreery, Jessica L., Kelly A. Mackintosh, Rebekah Mills-Bennett, and Melitta A. McNarry. 2021. "The Effect of a High-Intensity PrO2Fit Inspiratory Muscle Training Intervention on Physiological and Psychological Health in Adults with Bronchiectasis: A Mixed-Methods Study" International Journal of Environmental Research and Public Health 18, no. 6: 3051. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063051