
Device-Measured Physical Activity, Sedentary Behaviors, Built Environment, and Adiposity Gain in Older Women: A Seven-Year Prospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
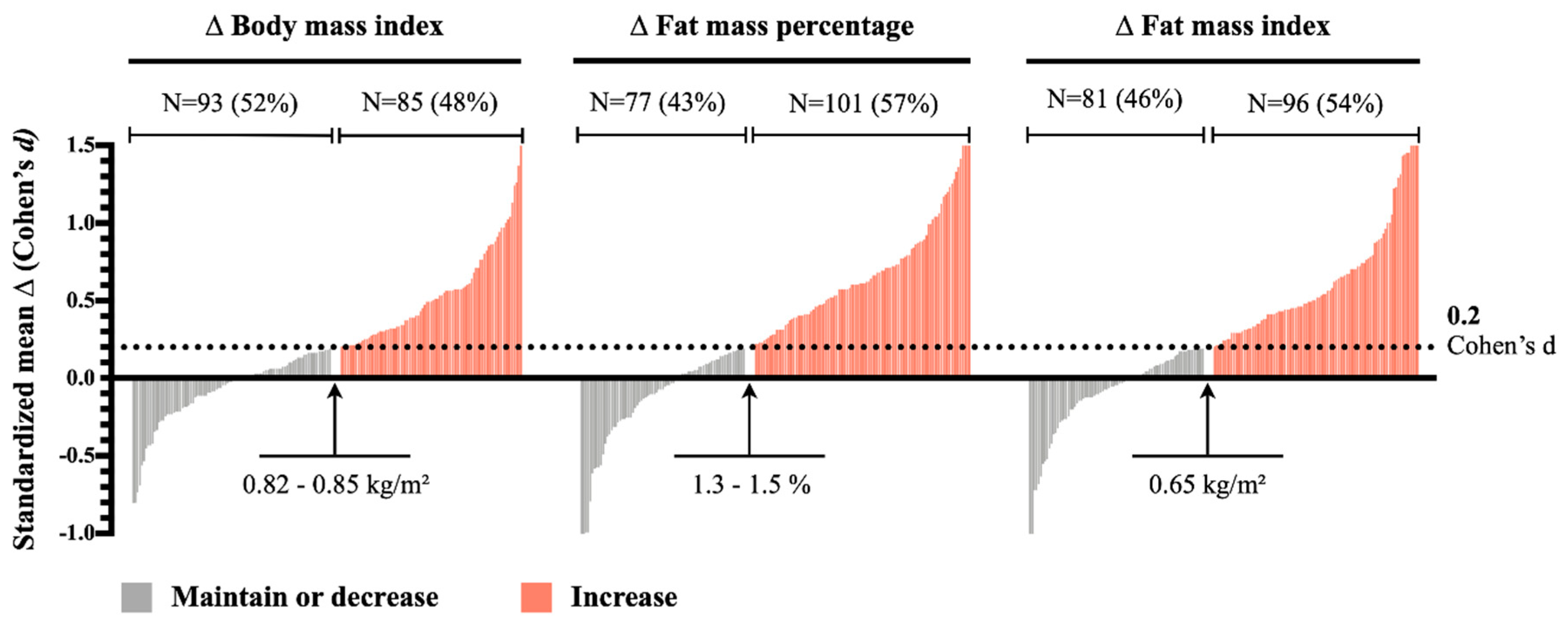
2.2. Adiposity Indicators
2.3. Intrapersonal and Built Environmental Variables
2.4. Physical Activity and Sedentary Behavior
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Handy, D.E.; Castro, R.; Loscalzo, J. Epigenetic Modifications. Circulation 2011, 123, 2145–2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doak, C.M.; Wijnhoven, T.M.A.; Schokker, D.F.; Visscher, T.L.S.; Seidell, J.C. Age standardization in mapping adult overweight and obesity trends in the WHO European Region. Obes. Rev. 2011, 13, 174–191. [Google Scholar] [CrossRef]
- Davis, S.R.; Castelo-Branco, C.; Chedraui, P.; Lumsden, M.A.; Nappi, R.E.; Shah, D.; Villaseca, P. Writing Group of the International Menopause Society for World Menopause Day 2012. Understanding weight gain at menopause. Climacteric 2012, 15, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Salihu, H.M.; Bonnema, S.M.; Alio, A.P. Obesity: What is an elderly population growing into? Maturitas 2009, 63, 7–12. [Google Scholar] [CrossRef]
- Genton, L.; Karsegard, V.L.; Chevalley, T.; Kossovsky, M.P.; Darmon, P.; Pichard, C. Body composition changes over 9 years in healthy elderly subjects and impact of physical activity. Clin. Nutr. 2011, 30, 436–442. [Google Scholar] [CrossRef]
- Raguso, C.A.; Kyle, U.; Kossovsky, M.P.; Roynette, C.; Paoloni-Giacobino, A.; Hans, D.; Genton, L.; Pichard, C. A 3-year longitudinal study on body composition changes in the elderly: Role of physical exercise. Clin. Nutr. 2006, 25, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; Lehnert, T.; Ernst, A.; Lange, C.; Wiese, B.; Prokein, J.; Weyerer, S.; Werle, J.; Pentzek, M.; Fuchs, A.; et al. Prevalence and determinants of overweight and obesity in old age in Germany. BMC Geriatr. 2015, 15, 83. [Google Scholar] [CrossRef] [Green Version]
- Owen, N.; Bauman, A.; Brown, W. Too much sitting: A novel and important predictor of chronic disease risk? Br. J. Sports Med. 2008, 43, 81–83. [Google Scholar] [CrossRef] [Green Version]
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary Behaviors and Subsequent Health Outcomes in Adults: A Systematic Review of Longitudinal Studies, 1996–2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef] [PubMed]
- De Araújo, C.A.H.; Giehl, M.W.C.; Danielewicz, A.L.; De Araujo, P.G.; D’Orsi, E.; Boing, A.F. Ambiente construído, renda contextual e obesidade em idosos: Evidências de um estudo de base populacional. Cad. Saúde Pública 2018, 34, e00060217. [Google Scholar] [CrossRef]
- Letarte, L.; Pomerleau, S.; Tchernof, A.; Biertho, L.; Waygood, E.O.D.; Lebel, A. Neighbourhood effects on obesity: Scoping review of time-varying outcomes and exposures in longitudinal designs. BMJ Open 2020, 10, e034690. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Conrtrol and Prevention. Healthy Places-Healthy Places Terminology. Available online: https://www.cdc.gov/healthyplaces/terminology.htm (accessed on 4 January 2021).
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too Much Sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.V.; Frontera, W.R.; Roubenoff, R.; Evans, W.J.; Singh, M.A.F. Longitudinal changes in body composition in older men and women: Role of body weight change and physical activity. Am. J. Clin. Nutr. 2002, 76, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Sims, S.T.; Kubo, J.; Desai, M.; Bea, J.; Beasley, J.M.; Manson, J.E.; Allison, M.; Seguin, R.A.; Chen, Z.; Michael, Y.L.; et al. Changes in Physical Activity and Body Composition in Postmenopausal Women over Time. Med. Sci. Sports Exerc. 2013, 45, 1486–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainsworth, B.E.; Caspersen, C.J.; Matthews, C.E.; Mâsse, L.C.; Baranowski, T.; Zhu, W. Recommendations to Improve the Accuracy of Estimates of Physical Activity Derived From Self Report. J. Phys. Act. Health 2012, 9, S76–S84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, T.J.; Owen, C.G.; Victor, C.R.; Adams, R.; Ekelund, U.; Cook, D.G. A Comparison of Questionnaire, Accelerometer, and Pedometer. Med. Sci. Sports Exerc. 2009, 41, 1392–1402. [Google Scholar] [CrossRef]
- Guo, W.; Key, T.J.; Reeves, G.K. Accelerometer compared with questionnaire measures of physical activity in relation to body size and composition: A large cross-sectional analysis of UK Biobank. BMJ Open 2019, 9, e024206. [Google Scholar] [CrossRef] [Green Version]
- Cuberek, R.; Pelclová, J.; Gába, A.; Pechová, J.; Svozilová, Z.; Přidalová, M.; Štefelová, N.; Hron, K. Adiposity and changes in movement-related behaviors in older adult women in the context of the built environment: A protocol for a prospective cohort study. BMC Public Health 2019, 19, 1–7. [Google Scholar] [CrossRef]
- Pelclová, J.; Gába, A.; Tlučáková, L.; Pośpiech, D. Association between physical activity (PA) guidelines and body composition variables in middle-aged and older women. Arch. Gerontol. Geriatr. 2012, 55, e14–e20. [Google Scholar] [CrossRef]
- Gába, A.; Kapuš, O.; Cuberek, R.; Botek, M. Comparison of multi- and single-frequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for assessment of body composition in post-menopausal women: Effects of body mass index and accelerometer-determined physical activity. J. Hum. Nutr. Diet. 2014, 28, 390–400. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Hecksteden, A.; Pitsch, W.; Rosenberger, F.; Meyer, T. Repeated testing for the assessment of individual response to exercise training. J. Appl. Physiol. 2018, 124, 1567–1579. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Cerin, E.; Saelens, B.E.; Sallis, J.F.; Frank, L.D. Neighborhood Environment Walkability Scale. Med. Sci. Sports Exerc. 2006, 38, 1682–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Mâsse, L.C.; Tilert, T.; Mcdowell, M. Physical Activity in the United States Measured by Accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Gorman, E.; Hanson, H.M.; Yang, P.H.; Khan, K.M.; Liu-Ambrose, T.; Ashe, M.C. Accelerometry analysis of physical activity and sedentary behavior in older adults: A systematic review and data analysis. Eur. Rev. Aging Phys. Act. 2014, 11, 35–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Ross, R.; Chaput, J.-P.; Giangregorio, L.M.; Janssen, I.; Saunders, T.J.; E Kho, M.; Poitras, V.J.; Tomasone, J.R.; El-Kotob, R.; McLaughlin, E.C.; et al. Canadian 24-Hour Movement Guidelines for Adults aged 18-64 years and Adults aged 65 years or older: An integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 2020, 45, S57–S102. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Craig, C.L.; Brown, W.J.; Clemes, S.A.; De Cocker, K.; Giles-Corti, B.; Hatano, Y.; Inoue, S.; Matsudo, S.M.; Mutrie, N.; et al. How many steps/day are enough? for adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 79. [Google Scholar] [CrossRef] [Green Version]
- Buffa, R.; Floris, G.U.; Putzu, P.F.; Marini, E. Body composition variations in ageing. Coll. Antropol. 2011, 35, 259–265. [Google Scholar] [PubMed]
- Letarte, L.; Lebel, A.; Waygood, E.; Tchernof, A.; Biertho, L. Longitudinal designs to study neighbourhood effects on the development of obesity: A scoping review protocol. BMJ Open 2018, 8, e017704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galgani, J.; Ravussin, E. Energy metabolism, fuel selection and body weight regulation. Int. J. Obes. 2008, 32, S109–S119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sink, K.M.; Espeland, M.A.; Castro, C.M.; Church, T.S.; A Cohen, R.; Dodson, J.A.; Guralnik, J.M.; Hendrie, H.C.; Jennings, J.M.; Katula, J.; et al. Effect of a 24-Month Physical Activity Intervention vs Health Education on Cognitive Outcomes in Sedentary Older Adults. JAMA 2015, 314, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.R.; Ekelund, U. Physical Activity in the Prevention of Weight Gain: The Impact of Measurement and Interpretation of Associations. Curr. Obes. Rep. 2019, 8, 66–76. [Google Scholar] [CrossRef]
- Baumeister, S.E.; Ricci, C.; Kohler, S.; Fischer, B.; Töpfer, C.; Finger, J.D.; Leitzmann, M.F. Physical activity surveillance in the European Union: Reliability and validity of the European Health Interview Survey-Physical Activity Questionnaire (EHIS-PAQ). Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzmarzyk, P.T.; Powell, K.E.; Jakicic, J.M.; Troiano, R.P.; Piercy, K.; Tennant, B. Sedentary Behavior and Health: Update from the 2018 Physical Activity Guidelines Advisory Committee. Med. Sci. Sports Exerc. 2019, 51, 1227–1241. [Google Scholar] [CrossRef]
- Gibbs, B.B.; Gabriel, K.P.; Carnethon, M.R.; Gary-Webb, T.; Jakicic, J.M.; Rana, J.S.; Reis, J.P.; Siddique, J.; Sternfeld, B.; Lewis, C.E. Sedentary Time, Physical Activity, and Adiposity: Cross-sectional and Longitudinal Associations in CARDIA. Am. J. Prev. Med. 2017, 53, 764–771. [Google Scholar] [CrossRef]
- Pulsford, R.M.; Stamatakis, E.; Britton, A.R.; Brunner, E.J.; Hillsdon, M.M. Sitting Behavior and Obesity: Evidence from the Whitehall II Study. Am. J. Prev. Med. 2013, 44, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Van Uffelen, J.G.; Watson, M.J.; Dobson, A.J.; Brown, W.J. Sitting Time Is Associated With Weight, but Not With Weight Gain in Mid-Aged Australian Women. Obesity 2010, 18, 1788–1794. [Google Scholar] [CrossRef]
- Pedisic, Z.; Grunseit, A.; Ding, D.; Chau, J.Y.; Banks, E.; Stamatakis, E.; Jalaludin, B.B.; Bauman, A.E. High sitting time or obesity: Which came first? Bidirectional association in a longitudinal study of 31,787 Australian adults. Obesity 2014, 22, 2126–2130. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Kolle, E.; Steene-Johannessen, J.; Dalene, K.E.; Nilsen, A.K.O.; Anderssen, S.A.; Hansen, B.H. Objectively measured sedentary time and physical activity and associations with body weight gain: Does body weight determine a decline in moderate and vigorous intensity physical activity? Int. J. Obes. 2017, 41, 1769–1774. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Powell, K.E.; Campbell, W.W.; Dipietro, L.; Pate, R.R.; Pescatello, L.S.; Collins, K.A.; Bloodgood, B.; Piercy, K.L. Physical Activity and the Prevention of Weight Gain in Adults: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1262–1269. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.-M. Physical Activity and Weight Gain Prevention. JAMA 2010, 303, 1173–1179. [Google Scholar] [CrossRef] [Green Version]
- Moholdt, T.; Wisløff, U.; Lydersen, S.; Nauman, J. Current physical activity guidelines for health are insufficient to mitigate long-term weight gain: More data in the fitness versus fatness debate (The HUNT study, Norway). Br. J. Sports Med. 2014, 48, 1489–1496. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.T.; Thompson, P.D. Dose-Dependent Effects of Training and Detraining on Weight in 6406 Runners during 7.4 Years*. Obesity 2006, 14, 1975–1984. [Google Scholar] [CrossRef] [Green Version]
- Laddu, D.R.; Cawthon, P.M.; Parimi, N.; Hoffman, A.R.; Orwoll, E.; Miljkovic, I.; Stefanick, M.L. Trajectories of the relationships of physical activity with body composition changes in older men: The MrOS study. BMC Geriatr. 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Congdon, P. Obesity and Urban Environments. Int. J. Environ. Res. Public Health 2019, 16, 464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greendale, G.A.; Sternfeld, B.; Huang, M.; Han, W.; Karvonen-Gutierrez, C.; Ruppert, K.; Cauley, J.A.; Finkelstein, J.S.; Jiang, S.-F.; Karlamangla, A.S. Changes in body composition and weight during the menopause transition. JCI Insight 2019, 4. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| n | Baseline | Seven-Year Follow-Up | Change (Follow-Up Minus Baseline) | |
|---|---|---|---|---|
| Age (years) | 178 | 62.8 (4.1) | ||
| Adiposity indicators | ||||
| BMI (kg/m2) | 178 | 26.3 (4.1) | 27.2 (4.3) | 0.9 (1.7) * |
| Fat mass (%) | 178 | 34.4 (6.7) | 36.6 (6.8) | 2.4 (3.7) * |
| FMI (kg/m2) | 178 | 9.3 (3.1) | 10.2 (3.3) | 1.0 (1.6) * |
| Intrapersonal | ||||
| Low satisfaction with life (N, %) | 114 | 20, 18 | ||
| Education | ||||
| Primary (N, %) | 178 | 85, 48 | ||
| University studies (N, %) | 178 | 93, 52 | ||
| Family status | ||||
| Married or living with a partner (N, %) | 122 | 87, 71 | ||
| Widow or single (N, %) | 122 | 35, 29 | ||
| Employment | ||||
| Retired (N, %) | 176 | 129, 73 | ||
| Employed (N, %) | 176 | 36, 21 | ||
| Unemployed (N, %) | 176 | 11, 6 | ||
| Perceived environmental | ||||
| Low density | 125 | 63, 50 | ||
| Low proximity (N, %) | 82 | 31, 38 | ||
| Low accessibility (N, %) | 74 | 22, 30 | ||
| Low street connectivity (N, %) | 125 | 42, 34 | ||
| Low walking/cycling infrastructure | 125 | 42, 34 | ||
| Low aesthetics (N, %) | 125 | 52, 42 | ||
| Low safety (N, %) | 125 | 64, 51 | ||
| Physical activity and sedentary behavior | ||||
| Sedentary behavior (min/day) | 178 | 437 (85) | ||
| LPA (min/day) | 178 | 369 (83) | ||
| MVPA (min/day) | 178 | 41 (24) | ||
| Total PA (counts/min) | 178 | 400 (124) | ||
| Step count (steps/day) | 178 | 9817 (2976) | ||
| Be sedentary (≥8 h ST/day) | 178 | 86, 48 | ||
| Meet PA recommendations | ||||
| No: ≤150 min/day MVPA (N, %) | 178 | 39, 22 | ||
| Yes: 150–300 min/day MVPA (N, %) | 178 | 61, 34 | ||
| Yes: ≥300 min/day MVPA (N, %) | 178 | 78, 44 | ||
| Meet step recommendations (N, %) | 178 | 102, 57 | ||
| Participation in organized PA (N, %) | 125 | 88, 70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molina-Garcia, P.; Medrano, M.; Pelclová, J.; Zając-Gawlak, I.; Tlučáková, L.; Přidalová, M. Device-Measured Physical Activity, Sedentary Behaviors, Built Environment, and Adiposity Gain in Older Women: A Seven-Year Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 3074. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063074
Molina-Garcia P, Medrano M, Pelclová J, Zając-Gawlak I, Tlučáková L, Přidalová M. Device-Measured Physical Activity, Sedentary Behaviors, Built Environment, and Adiposity Gain in Older Women: A Seven-Year Prospective Study. International Journal of Environmental Research and Public Health. 2021; 18(6):3074. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063074
Chicago/Turabian StyleMolina-Garcia, Pablo, María Medrano, Jana Pelclová, Izabela Zając-Gawlak, Lenka Tlučáková, and Miroslava Přidalová. 2021. "Device-Measured Physical Activity, Sedentary Behaviors, Built Environment, and Adiposity Gain in Older Women: A Seven-Year Prospective Study" International Journal of Environmental Research and Public Health 18, no. 6: 3074. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063074