
Flash Glucose Monitoring and Patient Satisfaction: A Meta-Review of Systematic Reviews

 ,
,  ,
,  and
and
Abstract
:1. Introduction
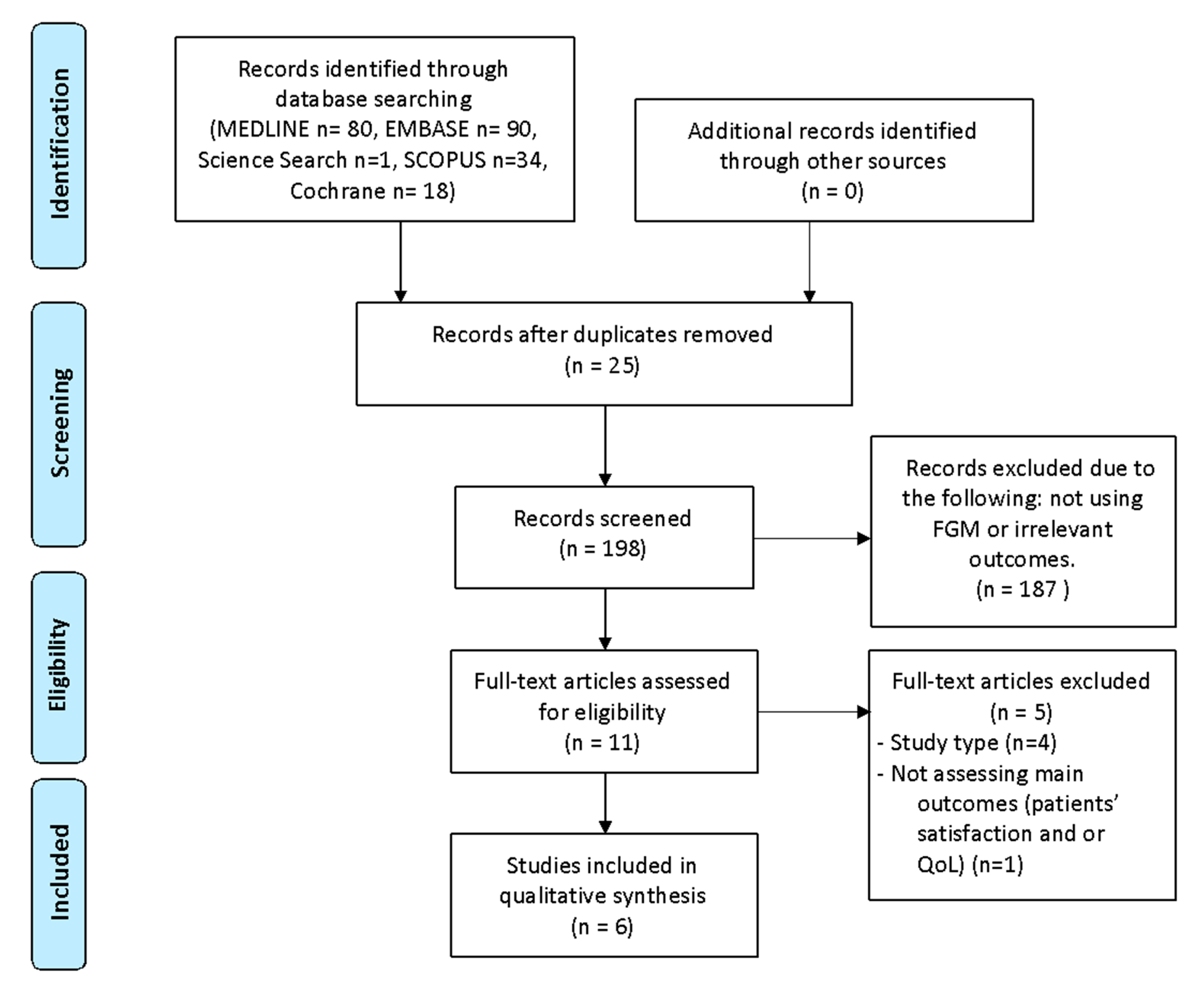
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Data Synthesis
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Quality of Life
3.3. Patients’ Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADDQoL | Audit of Diabetes-Dependent Quality-of-life |
| AMSTAR | Assessment of Multiple Systematic Reviews |
| CGM | Continuous glucose monitoring |
| DDS | Diabetes Distress Scale |
| DQoL | Diabetes Quality of Life |
| DTSQ | Diabetes Treatment Satisfaction Questionnaire |
| FGM | Flash glucose monitoring |
| HBA1C | Glycated haemoglobin |
| HRQoL | Health-related quality of life |
| MDI | Multiple doses of insulin |
| PEDSQoL | Paediatrics Quality of Life Inventory |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | International Prospective Register of Systematic Reviews |
| QoL | Quality of life |
| RCTS | Randomised controlled trials |
| SMBG | Self-monitoring of blood glucose |
| SUCRA | Surface under the cumulative ranking curve |
| T1D | Type 1 diabetes |
| T2D | Type 2 diabetes |
| WHO | World Health Organization |
References
- American Diabetes Association. 4. Lifestyle Management. Diabetes Care 2017, 40 (Suppl. 1), S33–S43. Available online: https://care.diabetesjournals.org/content/40/Supplement_1/S33 (accessed on 3 November 2020). [CrossRef] [Green Version]
- Grant, A.K.; Golden, L. Technological Advancements in the Management of Type 2 Diabetes. Curr. Diabetes Rep. 2019, 19, 163. [Google Scholar] [CrossRef]
- Cappon, G.; Acciaroli, G.; Vettoretti, M.; Facchinetti, A.; Sparacino, G. Wearable continuous glucose monitoring sensors: A revolution in diabetes treatment. Electronics 2017, 6, 65. [Google Scholar] [CrossRef] [Green Version]
- The Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Group. Continuous Glucose Monitoring and Intensive Treatment of Type 1 Diabetes. N. Engl. J. Med. 2008, 359, 1464–1476. Available online: https://0-doi-org.brum.beds.ac.uk/10.1056/NEJMoa0805017 (accessed on 3 November 2020). [CrossRef] [Green Version]
- Leelarathna, L.; Wilmot, E.G. Flash forward: A review of flash glucose monitoring. Diabetes Med. 2018, 35, 472–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palylyk-Colwell, E.; Ford, C. Flash Glucose Monitoring System for Diabetes. Diabetes Med. 2019, 35, 1–13. Available online: https://pubmed.ncbi.nlm.nih.gov/32231476/ (accessed on 6 November 2020).
- White, N.D.; Knezevich, E. Flash Glucose Monitoring Technology Impact on Diabetes Self-Care Behavior. Am. J. Lifestyle Med. 2019, 14, 130–132. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/29369576 (accessed on 6 November 2020). [PubMed]
- National Institute for Health and Care Excellence (NICE). FreeStyle Libre for Glucose Monitoring (MIB110). 2017; pp. 1–20. Available online: https://www.nice.org.uk/advice/mib110 (accessed on 6 November 2020).
- Rodríguez-Almagro, J.; García-Manzanares, Á.; Lucendo, A.J.; Hernández-Martínez, A. Health-related quality of life in diabetes mellitus and its social, demographic and clinical determinants: A nationwide cross-sectional survey. J. Clin. Nurs. 2018, 27, 4212–4223. [Google Scholar] [CrossRef]
- Saisho, Y. Use of Diabetes Treatment Satisfaction Questionnaire in Diabetes Care: Importance of Patient-Reported Outcomes. Int. J. Environ. Res. Public Health 2018, 15, 947. [Google Scholar] [CrossRef] [Green Version]
- Jing, X.; Chen, J.; Dong, Y.; Han, D.; Zhao, H.; Wang, X.; Gao, F.; Li, C.; Cui, Z.; Liu, Y.; et al. Related factors of quality of life of type 2 diabetes patients: A systematic review and meta-analysis. Health Qual. Life Outcomes 2018, 16, 189. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. Available online: https://0-www-bmj-com.brum.beds.ac.uk/content/358/bmj.j4008 (accessed on 22 November 2020).
- Bolinder, J.; Antuna, R.; Geelhoed-Duijvestijn, P.; Kröger, J.; Weitgasser, R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: A multicentre, non-masked, randomised controlled trial. Lancet 2016, 388, 2254–2263. Available online: http://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/pii/S0140673616315355 (accessed on 26 November 2020). [CrossRef]
- Haak, T.; Hanaire, H.; Ajjan, R.; Hermanns, N.; Riveline, J.-P.; Rayman, G. Use of Flash Glucose-Sensing Technology for 12 months as a Replacement for Blood Glucose Monitoring in Insulin-treated Type 2 Diabetes. Diabetes Ther. 2017, 8, 573–586. [Google Scholar] [CrossRef]
- Yaron, M.; Roitman, E.; Aharon-Hananel, G.; Landau, Z.; Ganz, T.; Yanuv, I.; Rozenberg, A.; Karp, M.; Ish-Shalom, M.; Singer, J.; et al. Effect of Flash Glucose Monitoring Technology on Glycemic Control and Treatment Satisfaction in Patients With Type 2 Diabetes. Diabetes Care 2019, 42, 1178–1184. Available online: https://care.diabetesjournals.org/content/42/7/1178 (accessed on 26 November 2020). [CrossRef] [PubMed]
- Ajjan, R.A.; Jackson, N.; Thomson, S.A. Reduction in HbA1c using professional flash glucose monitoring in insulin-treated type 2 diabetes patients managed in primary and secondary care settings: A pilot, multicentre, randomised controlled trial. Diabetes Vasc. Dis. Res. 2019, 16, 385–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermanns, N.; Ehrmann, D.; Schipfer, M.; Kröger, J.; Haak, T.; Kulzer, B. The impact of a structured education and treatment programme (FLASH) for people with diabetes using a flash sensor-based glucose monitoring system: Results of a randomized controlled trial. Diabetes Res. Clin. Pract. 2019, 150, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Oskarsson, P.; Antuna, R.; Geelhoed-Duijvestijn, P.; Krӧger, J.; Weitgasser, R.; Bolinder, J. Impact of flash glucose monitoring on hypoglycaemia in adults with type 1 diabetes managed with multiple daily injection therapy: A pre-specified subgroup analysis of the IMPACT randomised controlled trial. Diabetologia 2018, 61, 539–550. [Google Scholar] [CrossRef] [Green Version]
- Mitsuishi, S.; Nishimura, R.; Harashima, S.-I.; Kawamura, T.; Tsujino, D.; Koide, K.; Nishimura, A.; Utsunomiya, K.; Inagaki, N.; Atsumi, Y. The Effect of Novel Glucose Monitoring System (Flash Glucose Monitoring) on Mental Well-being and Treatment Satisfaction in Japanese People with Diabetes. Adv. Ther. 2018, 35, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Kramer, G.; Michalak, L.; Müller, U.A.; Kloos, C.; Werner, C.; Kuniss, N. Association between Flash Glucose Monitoring and Metabolic Control as well as Treatment Satisfaction in Outpatients With Diabetes Type 1. Exp. Clin. Endocrinol. Diabetes 2019. [Google Scholar] [CrossRef] [PubMed]
- Overend, L.; Simpson, E.; Grimwood, T. Qualitative analysis of patient responses to the ABCD FreeStyle Libre audit questionnaire. Pract. Diabetes 2019, 36, 45–50. Available online: https://0-wchh-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/pdi.2213 (accessed on 27 November 2020). [CrossRef]
- Al Hayek, A.A.; Al Dawish, M.A. The Potential Impact of the FreeStyle Libre Flash Glucose Monitoring System on Mental Well-Being and Treatment Satisfaction in Patients with Type 1 Diabetes: A Prospective Study. Diabetes Ther. 2019, 10, 1239–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nana, M.; Moore, S.L.; Ang, E.; Lee, Z.X.; Bondugulapati, L.N.R. Flash glucose monitoring: Impact on markers of glycaemic control and patient-reported outcomes in individuals with type 1 diabetes mellitus in the real-world setting. Diabetes Res. Clin. Pract. 2019, 157, 107893. [Google Scholar] [CrossRef]
- Ish-Shalom, M.; Wainstein, J.; Raz, I.; Mosenzon, O. Improvement in Glucose Control in Difficult-to-Control Patients with Diabetes Using a Novel Flash Glucose Monitoring Device. J. Diabetes Sci. Technol. 2016, 10, 1412–1413. [Google Scholar] [CrossRef]
- Dover, A.R.; Stimson, R.H.; Zammitt, N.N.; Gibb, F.W. Flash Glucose Monitoring Improves Outcomes in a Type 1 Diabetes Clinic. J. Diabetes Sci. Technol. 2017, 11, 442–443. [Google Scholar] [CrossRef] [Green Version]
- Flash glucose monitoring system for people with type 1 or type 2 diabetes: A health technology assessment. Ont. Health Technol. Assess Ser. 2019, 19, 1–108.
- Pease, A.; Lo, C.; Earnest, A.; Kiriakova, V.; Liew, D.; Zoungas, S. The Efficacy of Technology in Type 1 Diabetes: A Systematic Review, Network Meta-analysis, and Narrative Synthesis. Diabetes Technol. Ther. 2020, 22, 411–421. [Google Scholar] [CrossRef]
- Al Hayek, A.A.; Robert, A.A.; Al Dawish, M.A. Acceptability of the FreeStyle Libre Flash Glucose Monitoring System: The Experience of Young Patients with Type 1 Diabetes. Clin. Med. Insights Endocrinol. Diabetes 2020, 13, 1179551420910122. [Google Scholar] [CrossRef] [Green Version]
- The DCCT Research Group. Reliability and Validity of a Diabetes Quality-of-Life Measure for the Diabetes Control and Complications Trial (DCCT). Diabetes Care 1988, 11, 725–732. Available online: https://care.diabetesjournals.org/content/11/9/725 (accessed on 2 December 2020). [CrossRef] [PubMed]
- Polonsky, W.H.; Fisher, L.; Earles, J.; Dudl, R.J.; Lees, J.; Mullan, J.; Jackson, R.A. Assessing psychosocial distress in diabetes: Development of the diabetes distress scale. Diabetes Care 2005, 28, 626–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Burwinkle, T.M.; Jacobs, J.R.; Gottschalk, M.; Kaufman, F.; Jones, K.L. The PedsQL{\texttrademark} in Type 1 and Type 2 Diabetes. Diabetes Care 2003, 26, 631–637. Available online: https://care.diabetesjournals.org/content/26/3/631 (accessed on 5 December 2020). [CrossRef] [Green Version]
- Bradley, C.; Todd, C.; Gorton, T.; Symonds, E.; Martin, A.; Plowright, R. The development of an individualized questionnaire measure of perceived impact of diabetes on quality of life: The ADDQoL. Qual. Life Res. 1999, 8, 79–91. [Google Scholar] [CrossRef]
- Bradley, C. (Ed.) Diabetes Treatment Satifaction Questionnaire (DTSQ). In Handbook of Psychology and Diabetes: A Guide to Psychological Measurement in Diabetes Research and Practise; Overseas Publishers Association: London, UK, 1994; pp. 111–132. [Google Scholar]
- Nieuwesteeg, A.; Pouwer, F.; van der Kamp, R.; van Bakel, H.; Aanstoot, H.-J.; Hartman, E. Quality of life of children with type 1 diabetes: A systematic review. Curr. Diabetes Rev. 2012, 8, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Ang, E.; Lee, Z.X.; Moore, S.; Nana, M. Flash glucose monitoring (FGM): A clinical review on glycaemic outcomes and impact on quality of life. J. Diabetes Complicat. 2020, 34, 107559. [Google Scholar] [CrossRef]
- Bidonde, J.; Fagerlund, B.C.; Frønsdal, K.B.; Lund, U.H.; Robberstad, B. FreeStyle Libre Flash Glucose Self-Monitoring System: A Single-Technology Assessment. NIPH Syst. Rev.; 2017. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK482068/pdf/Bookshelf_NBK482068 (accessed on 5 December 2020).
- Cowart, K.; Updike, W.; Bullers, K. Systematic Review of Randomized Controlled Trials Evaluating Glycemic Efficacy and Patient Satisfaction of Intermittent-Scanned Continuous Glucose Monitoring in Patients with Diabetes. Diabetes Technol. Ther. 2020, 22, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Alva, S.; Bailey, T.; Brazg, R.; Budiman, E.S.; Castorino, K.; Christiansen, M.P.; Forlenza, G.; Kipnes, M.; Liljenquist, D.R.; Liu, H. Accuracy of a 14-Day Factory-Calibrated Continuous Glucose Monitoring System With Advanced Algorithm in Pediatric and Adult Population With Diabetes. J. Diabetes Sci. Technol. 2020. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, F.; den Brinker, M.; De Block, C. The road from intermittently scanned glucose monitoring to hybrid closed-loop systems: Part A. Keys to success: Subject profiles, choice of systems, education. Ther. Adv. Endocrinol. Metab. 2019, 10, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Rodbard, D. Continuous glucose monitoring: A review of recent studies demonstrating improved glycemic outcomes. Diabetes Technol. Ther. 2017, 19, S25–S37. [Google Scholar] [CrossRef] [PubMed]
- Mancini, G.; Berioli, M.G.; Santi, E.; Rogari, F.; Toni, G.; Tascini, G.; Crispoldi, R.; Ceccarini, G.; Esposito, S. Flash Glucose Monitoring: A Review of the Literature with a Special Focus on Type 1 Diabetes. Nutrients 2018, 10, 992. [Google Scholar] [CrossRef] [Green Version]
- Rai, S.; Hulse, A.; Kumar, P. Feasibility and acceptability of ambulatory glucose profile in children with Type 1 diabetes mellitus: A pilot study. Indian J. Endocrinol. Metab. 2016, 20, 790–794. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 1 | Finger-stick test | 14 | T2D |
| 2 | Continuous glucose monitoring | 15 | type 2 diabetes mellitus |
| 3 | #1 OR #2 | 16 | Diabetes mellitus, Type 2 |
| 4 | Flash glucose monitoring | 17 | T1D |
| 5 | Freestyle Libre | 18 | type 1 diabetes |
| 6 | Intermittent-scanned continuous glucose monitoring | 19 | type 1 diabetes mellitus |
| 7 | #4 OR #5 OR #6 | 20 | Diabetes mellitus, Type 1 |
| 8 | Quality of life | 21 | #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 |
| 9 | Patient Satisfaction | 22 | systematic review |
| 10 | Health-related quality of life | 23 | review |
| 11 | HRQoL | 24 | meta-analysis |
| 12 | QoL | 25 | #22 OR #23 OR #24 |
| 13 | #8 OR #9 OR #10 OR #11 OR #12 | 26 | 3 AND 7 AND 13 AND 21 AND 25 |
| First Author (Year) | Search Databases and Search Period | Design of Included Studies, n | Total Sample, n Intervention/Comparator | Patients’ Satisfaction and QoL Design of Included Studies, n | First Author of Included Studies in Each Systematic Review with QoL and/or Patients’ Satisfaction Results | Meta-Analysis |
|---|---|---|---|---|---|---|
| Ang (2020) | MEDLINE, EMBASE, period not reported | RCTs PC RP Letters n = 16 | 1901 T1D and T2D adult patients. FCG/CGM or not specified | RCTs, n = 2 PC, n = 3 RP, n = 1 Letter, n = 2 | Bolinder [14], Yaron [16], Mitsuishi [20], Kramer [21], Nana [24], Overend [22], Ish-Shalom [25], Dover [26] | No |
| Bidonde (2017) | MEDLINE, Embase, Cochrane Library, Centre for Reviews and Dissemination: Database of Abstracts of Reviews of Effects, Health Technology Assessment database and other sources up to 18 January 2017 | RCTs n = 2 and their protocols | 465 T1D and T2D adult patients. FCG/SMBG | RCTs, n = 2 | Bolinder [14], Haak [15] | Yes |
| Cowart (2020) | Embase, PubMed, and the Cochrane Library CENTRAL Register of Controlled Trials, from each index’s inception through 8 November 2019 | RCTs n = 9 | 689 all T1D and T2D children, adolescents, adults and gestational diabetes. FCG/SMBG | RCTs, n = 4 | Haak [15], Ajjan [17], Yaron [16], Hermanns [18] | No |
| Dicembrini (2019) | MEDLINE up to 1 September 2018 | RCTs n = 12 | 224 T2D adult patients. FCG/SMBG | RCTs, n = 1 | Haak [15] | No |
| Ontario Health (2019) | MEDLINE, Embase, the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, the Health Technology Assessment Database, and the National Health Service Economic Evaluation Database up to April, 2018 | RCTs Observational studies n = 6 | 918 T1D and T2D with no restriction of age. FCG/SMBG | RCTs = 1 Observational n = 2 | Al Hayek [29], Bolinder [14], Mitsuishi [20] | No |
| Pease (2020) | MEDLINE, MEDLINE In-Process, EMBASE, PubMed, All Evidence-Based Medicine Reviews, Web of Science, PsycINFO, CINAHL PROSPERO (inception–24 April 2019) | RCTs n = 52 | 3975 T1D adults. Comparison among CGM, SMBG and FGM. | RCTs, n = 2 | Bolinder [14], Oskarsson [19] | Yes |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ang et al. 2020 | Yes | No | Yes | Partial Yes | Yes | Yes | No | Partial Yes | No | No | No MA | No MA | No | No | No | Yes | Low |
| Bidonde et al. 2017 | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Moderate |
| Cowart et al. 2020 | Yes | No | Yes | Partial Yes | Yes | No | No | Yes | Yes | Yes | No MA | No MA | Yes | No | No | Yes | Critically low |
| Dicembrini et al. 2019 | Yes | Yes | Yes | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Ontario Health 2019 | Yes | Yes | Yes | Yes | Yes | Yes | No | Partial Yes | Yes | No | No MA | No MA | Yes | Yes | No | Yes | High |
| Pease el at 2020 | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| First Author (Year) | T1DM | T2DM | ||||||
|---|---|---|---|---|---|---|---|---|
| QoL | p or 95% CI | Patients’ Satisfaction | p or 95% CI | QoL | p or 95% CI | Patient’s Satisfaction | p or 95% CI | |
| Ang (2020) | (1) No significant differences in DQoL scores (1RCT) (2) Significant improvement with DDS score with FGM (1RCT and 1 letter). | p = 0.052 p 0.001 and p = 0.006 | (1) Better DTSQ score in FGM (1RCT) (2) Better DTSQ score in FGM by 12.6 ± 5.5 points (1PC). | <0.001 NR | (1) No significant differences in ADDQoL (1RCT) | NR | (1) FGM group scored better in the DTSQ (2.47 ± 0.77 vs. 2.18 ± 0.83) (1RCT) | p = 0.053 |
| T1DM AND T2DM TOGETHER (1PC) | ||||||||
| (1) Better DTSQ score after use of FGM. | p = 0.001 | (1) WHO-5 scored better with FGM | p = <0.001 | |||||
| Bidonde (2017) | (1) DQoL mean difference between groups = −0.10 (1RCT) | 95% CI = −0.25 to 0.05 | (1) DTSQ mean difference between groups = 6.20 (1RCT) | 95% CI = 4.54 to 7.86 | (1) DQoL mean difference between groups = 0.00 (1RCT) | 95% CI = −0.16 to 0.16 | (1) DTSQ mean difference between groups = 4.00 (1RCT) | 95% CI = 2.32 to 5.68 |
| T1DM AND T2DM TOGETHER (M-A including 2RCT) | ||||||||
| (1) DTSQ mean difference between groups = 5.10 | I2 = 70% 95% CI = 2.95 to 7.26. | (1) DQoL mean difference between groups = −0.05 | I2 0% 95% CI = −0.16 to 0.05 | |||||
| Cowart (2020) | (1) Significant improvement in DQoL score in FGM group = −0.2 ± 0.4 vs. 0.0 ± 0.06 (1RCT) | p = 0.025 | (1) DTSQ score was better in the FGM group compared with SMBG (13.1 ± 0.50 vs. 9.0 ± 0.72) (1RCT) (2) DTSQ adjusted mean FGM vs. SMBG: 3.45 ± 1.54 vs. 3.54 ± 1.52 | p = <0.001 p = 0.02 | ||||
| Dicembrini (2019) | (1) DQoL showed better results for FGM vs. SMBG (1RCT) | NR | ||||||
| Ontario Health (2019) | (1) PedsQoL mean difference in favour of FGM vs. SMBG = 3.4 (1.31–5.49) (1PC). (2) DQoL mean difference between FGM and SMBG = −0.08 (95% CI −0.16 to 0.00) (1RCT). (3) WHO-5 mean difference between FGM and SMBG = 2.1 (1PC). | p = 0.002 p = 0.052 95% CI = 0.45 to 3.75. | (1) No significant increase in QoL scores (1RCT) (2) WHO-5 mean difference between FGM and SMBG = 1.0 (1PC) | NR 95% CI = −1.16 to 3.16 | ||||
| T1DM AND T2DM TOGETHER (1PC) | ||||||||
| (1) WHO-5 mean difference between groups (in favour of FGM) = 1.7 | 95% CI = 0.35 to 3.05 | |||||||
| Pease (2020) | (1) DQoL mean difference among groups = −0.08 (SE = 0.039) (1RCT) (2) Only the “satisfaction with treatment” subscore was significantly different and favoured FGM over SMBG (1RCT). (3) DDS mean difference −0.03 (SE = 0.089); (1RCT) and mean difference NR (1RCT). SUCRA: MDI + FGM second-best option (66.3%) | p = 0.052 p = <0.001 p = 0.763 and NR | DTSQ score: favoured FGM over SMBG: 13.3 (5.4) vs. 6.8 (6.2) | NR | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díez-Fernández, A.; Rodríguez-Huerta, M.D.; Mirón-González, R.; Laredo-Aguilera, J.A.; Martín-Espinosa, N.M. Flash Glucose Monitoring and Patient Satisfaction: A Meta-Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2021, 18, 3123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063123
Díez-Fernández A, Rodríguez-Huerta MD, Mirón-González R, Laredo-Aguilera JA, Martín-Espinosa NM. Flash Glucose Monitoring and Patient Satisfaction: A Meta-Review of Systematic Reviews. International Journal of Environmental Research and Public Health. 2021; 18(6):3123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063123
Chicago/Turabian StyleDíez-Fernández, Ana, María Dolores Rodríguez-Huerta, Rubén Mirón-González, José Alberto Laredo-Aguilera, and Noelia María Martín-Espinosa. 2021. "Flash Glucose Monitoring and Patient Satisfaction: A Meta-Review of Systematic Reviews" International Journal of Environmental Research and Public Health 18, no. 6: 3123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063123