
Evaluation of the Role of Leisure Time Physical Activity and Sedentary Behavior Simultaneously on the Income-Overweight/Obesity Relationship

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Dataset and Sample
2.2. Overweight/Obese Weight Status
2.3. Income
2.4. Leisure Time Physical Activity
2.5. Sedentary Behavior Time
2.6. Control Variables
2.7. Statistical Analyses
3. Results
3.1. Descriptive Statistics
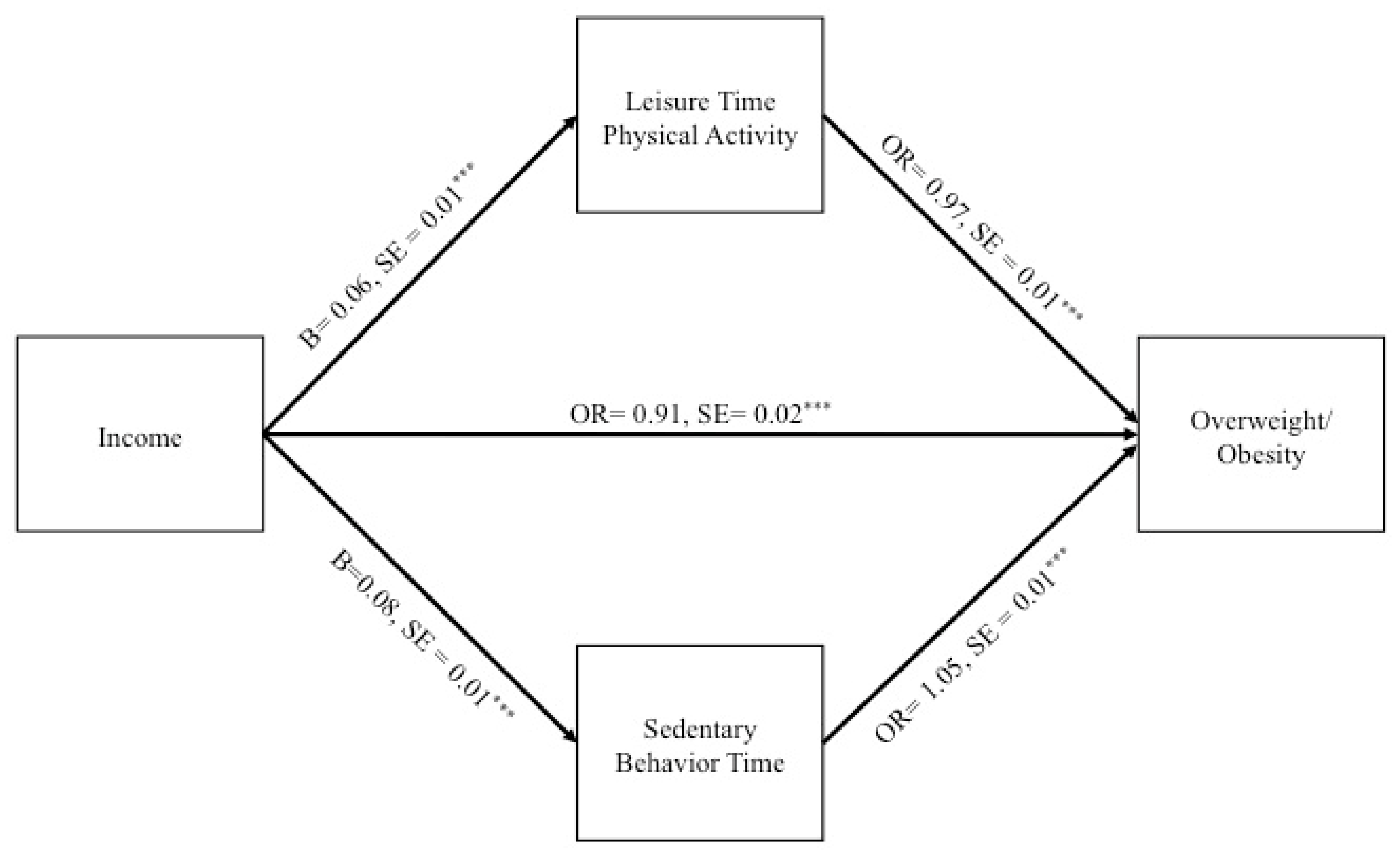
3.2. Structural Equation Modeling
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fryar, C.D.; Carroll, M.D.; Ogden, C.L. Prevalence of Overweight, Obesity, and Extreme Obesity Among Adults Aged 20 and Over: United States, 1960–1962 through 2011–2014; National Center for Health Statistics Data, Health E-Stats: Hyattsville, MD, USA, 2016.
- Paeratakul, S.; Lovejoy, J.C.; Ryan, D.H.; Bray, G.A. The relation of gender, race and socioeconomic status to obesity and obesity comorbidities in a sample of US adults. Int. J. Obes. 2002, 26, 1205–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Health Statistics Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities; National Center for Health Statistics Health: Hyattsville, MD, USA, 2015.
- Mokdad, A.H.; Ford, E.S.; Bowman, B.A.; Dietz, W.H.; Vinicor, F.; Bales, V.S.; Marks, J.S. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 2003, 289, 76–79. [Google Scholar] [CrossRef]
- King, G.A.; Fitzhugh, E.C.; Bassett, D.R., Jr.; McLaughlin, J.E.; Strath, S.J.; Swartz, A.M.; Thompson, D.L. Relationship of leisure-time physical activity and occupational activity to the prevalence of obesity. Int. J. Obes. 2001, 25, 606–612. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services; Centers for Disease Control and Prevention; National Center for Chronic Disease Prevention and Health Promotion. Physical Activity and Health: A Report of the Surgeon General; DIANE Publishing: Atlanta, GA, USA, 1996.
- Wanner, M.; Martin, B.W.; Autenrieth, C.S.; Schaffner, E.; Meier, F.; Brombach, C.; Stolz, D.; Bauman, A.; Rochat, T.; Schindler, C.; et al. Associations between domains of physical activity, sitting time, and different measures of overweight and obesity. Prev. Med. Rep. 2016, 3, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Mao, Y. Obesity and leisure time physical activity among Canadians. Prev. Med. 2006, 42, 261–265. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention National Center for Chronic Disease Prevention and Health Promotion, Division of Nutrition, Physical Activity, and Obesity. Data, Trend and Maps. Available online: https://www.cdc.gov/nccdphp/dnpao/data-trends-maps/index.html (accessed on 24 April 2020).
- Ford, E.S.; Merritt, R.K.; Heath, G.W.; Powell, K.E.; Washburn, R.A.; Kriska, A.; Haile, G. Physical activity behaviors in lower and higher socioeconomic status populations. Am. J. Epidemiol. 1991, 133, 1246–1256. [Google Scholar] [CrossRef]
- Elhakeem, A.; Cooper, R.; Bann, D.; Hardy, R. Childhood socioeconomic position and adult leisure-time physical activity: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 92. [Google Scholar] [CrossRef] [Green Version]
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary behaviors and subsequent health outcomes in adults a systematic review of longitudinal studies, 1996–2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef]
- Hu, F.B.; Li, T.Y.; Colditz, G.A.; Willett, W.C.; Manson, J.E. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA 2003, 289, 1785–1791. [Google Scholar] [CrossRef] [Green Version]
- Ching, P.L.; Willett, W.C.; Rimm, E.B.; Colditz, G.A.; Gortmaker, S.L.; Stampfer, M.J. Activity level and risk of overweight in male health professionals. Am. J. Public Health 1996, 86, 25–30. [Google Scholar] [CrossRef] [Green Version]
- O’Donoghue, G.; DEDIPAC Consortium; Perchoux, C.; Mensah, K.; Lakerveld, J.; Van Der Ploeg, H.; Bernaards, C.; Chastin, S.F.M.; Simon, C.; O’Gorman, D.; et al. A systematic review of correlates of sedentary behaviour in adults aged 18–65 years: A socio-ecological approach. BMC Public Health 2016, 16, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2017. [Google Scholar]
- Kozo, J.; Sallis, J.F.; Conway, T.L.; Kerr, J.; Cain, K.; Saelens, B.E.; Frank, L.D.; Owen, N. Sedentary behaviors of adults in relation to neighborhood walkability and income. Health Psychol. 2012, 31, 704–713. [Google Scholar] [CrossRef]
- Garcia, J.M.; Duran, A.T.; Schwartz, J.E.; Booth, J.N., III; Hooker, S.P.; Willey, J.Z.; Cheung, Y.K.; Park, C.; Williams, S.K.; Sims, M.; et al. Types of sedentary behavior and risk of cardiovascular events and mortality in Blacks: The Jackson Heart Study. J. Am. Heart Assoc. 2019, 8, e010406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS) National Health and Nutrition Examination Survey Data. Available online: https://wwwn.cdc.gov/nchs/nhanes/NhanesCitation.aspx (accessed on 1 December 2018).
- Johnson, C.L.; Dohrmann, S.M.; Burt, V.L.; Mohadjer, L.K. National health and nutrition examination survey: Sample design, 2011–2014. Vital Health Stat. 2014, 162, 1–33. [Google Scholar]
- Adminstration for Community Living. Administration on Aging; Older Americans Act (OAA). Available online: https://acl.gov/about-acl/authorizing-statutes/older-americans-act (accessed on 21 February 2019).
- Centers for Disease Control and Prevention. Healthy Weight: Assessing Your Weight. Available online: http://www.cdc.gov/healthyweight/assessing/ (accessed on 7 August 2017).
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the Healthy Eating Index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gidlow, C.; Johnston, L.H.; Crone, D.; Ellis, N.; James, D. A systematic review of the relationship between socio-economic position and physical activity. Health Educ. J. 2006, 65, 338–367. [Google Scholar] [CrossRef]
- Beenackers, M.A.; Kamphuis, C.B.M.; Giskes, K.; Brug, J.; Kunst, A.E.; Burdorf, A.; Van Lenthe, F.J. Socioeconomic inequalities in occupational, leisure-time, and transport related physical activity among European adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 116. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.; McCourt, O.; Sawyer, A.; Ucci, M.; Marmot, A.; Wardle, J.; Fisher, A. A review of occupational physical activity and sedentary behaviour correlates. Occup. Med. 2016, 66, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Bennie, J.; Timperio, A.; Dunstan, D.; Crawford, D.; Salmon, J. Environmental correlates of physical activity in Australian workplaces. Int. J. Work. Health Manag. 2010, 3, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Schofield, G.; Badlands, H.; Oliver, M. Objectively-measured physical activity in New Zealand workers. J. Sci. Med. Sport 2005, 8, 143–151. [Google Scholar] [CrossRef] [Green Version]
- Steele, R.; Mummery, K. Occupational physical activity across occupational categories. J. Sci. Med. Sport 2003, 6, 398–407. [Google Scholar] [CrossRef]
- Murillo, R.; Reesor-Oyer, L.M.; Hernandez, D.C.; Liu, Y.; Obasi, E.M. Neighborhood walkability and overweight/obese weight status among Latino adults. Am. J. Health Promot. 2020, 34, 599–607. [Google Scholar] [CrossRef]
- Reitzel, L.R.; Okamoto, H.; Hernandez, D.C.; Regan, S.D.; McNeill, L.H.; Obasi, E.M. The built food environment and dietary intake among African-American adults. Am. J. Health Behav. 2016, 40, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celis-Morales, C.A.; Perez-Bravo, F.; Ibañez, L.; Salas, C.; Bailey, M.E.S.; Gill, J.M.R. Objective vs. self-reported physical activity and sedentary time: Effects of measurement method on relationships with risk biomarkers. PLoS ONE 2012, 7, e36345. [Google Scholar] [CrossRef]


{kind=link}
| Full Sample (n = 10,348) | Normal Weight (n = 3136) | Overweight/Obese (n = 7212) | F | Effect Size Cohen’s D or Odds Ratio | |
|---|---|---|---|---|---|
| Dependent variable | |||||
| Weight status ^ | |||||
| Overweight/obese | 69% | --- | --- | ||
| Normal weight | 31% | --- | --- | ||
| Independent variable | |||||
| Income (FPL) ^ | 3.04 (0.05) | 3.11 (0.07) | 3.01 (0.05) * | 4.08 | 0.02 |
| Mediating variables | |||||
| Leisure time physical activity (weekly hours) | 3.48 (0.10) | 4.30 (0.17) | 3.11 (0.09) *** | 58.37 | 0.14 |
| Sedentary behavior (Daily hours) | 6.25 (0.07) | 5.98 (0.10) | 6.37 (0.08) *** | 12.41 | 0.06 |
| Demographic characteristics | |||||
| Age | 39.47 (0.23) | 36.79 (0.41) | 40.69 (0.22) *** | 89.92 | 0.20 |
| Sex | |||||
| Female | 50% | 56% | 48% *** | 42.78 | 0.72 |
| Male | 50% | 44% | 52% | ||
| Race/ethnicity | |||||
| White | 67% | 70% | 65% ** | 9.26 | 0.82 |
| Black | 11% | 8% | 13% *** | 42.97 | 1.59 |
| Hispanic | 15% | 11% | 17% *** | 33.11 | 1.64 |
| Other | 7% | 11% | 5% *** | 43.68 | 0.44 |
| Nativity status | |||||
| Foreign born | 17% | 19% | 17% | 3.44 | 1.17 |
| Native born | 83% | 81% | 83% | ||
| Marital status | |||||
| Single | 37% | 42% | 35% *** | 24.59 | 0.74 |
| Married/cohabiting | 63% | 58% | 65% | ||
| Education | |||||
| Less than high school degree | 14% | 12% | 15% ** | 11.67 | 1.29 |
| High school degree | 55% | 50% | 56% *** | 15.05 | 1.26 |
| College graduate or greater | 31% | 37% | 29% *** | 30.93 | 0.67 |
| Employment | |||||
| Employed | 74% | 73% | 75% | 2.54 | 1.09 |
| Unemployed | 26% | 27% | 25% | ||
| Health insurance | |||||
| Insured | 77% | 77% | 75% | 0.02 | 1.01 |
| Uninsured | 23% | 23% | 25% | ||
| Health behaviors | |||||
| Healthy Eating Index | 52.54 (0.27) | 54.08 (0.43) | 51.84 (0.25) *** | 35.31 | 0.10 |
| Average alcoholic drinks per day | 0.60 (0.02) | 0.66 (0.04) | 0.58 (0.02) * | 4.52 | 0.04 |
| Smoking status | |||||
| Smoker | 23% | 27% | 21% *** | 15.37 | 0.74 |
| Non-smoker | 77% | 73% | 79% | ||
| Average hours sleep per night | 6.83 (0.02) | 6.97 (0.03) | 6.76 (0.02) *** | 39.63 | 0.12 |
| Indirect Effect | B | SE | 95% Bootstrap CI |
|---|---|---|---|
| Income → Leisure time physical activity → Overweight/obesity | −0.005 | 0.001 | −0.01, −0.003 |
| Income → Sedentary behavior time→ Overweight/obesity | 0.008 | 0.002 | 0.005, 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reesor-Oyer, L.; Murillo, R.; LaVoy, E.C.; O’Connor, D.P.; Liu, Y.; Hernandez, D.C. Evaluation of the Role of Leisure Time Physical Activity and Sedentary Behavior Simultaneously on the Income-Overweight/Obesity Relationship. Int. J. Environ. Res. Public Health 2021, 18, 3127. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063127
Reesor-Oyer L, Murillo R, LaVoy EC, O’Connor DP, Liu Y, Hernandez DC. Evaluation of the Role of Leisure Time Physical Activity and Sedentary Behavior Simultaneously on the Income-Overweight/Obesity Relationship. International Journal of Environmental Research and Public Health. 2021; 18(6):3127. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063127
Chicago/Turabian StyleReesor-Oyer, Layton, Rosenda Murillo, Emily C. LaVoy, Daniel P. O’Connor, Yu Liu, and Daphne C. Hernandez. 2021. "Evaluation of the Role of Leisure Time Physical Activity and Sedentary Behavior Simultaneously on the Income-Overweight/Obesity Relationship" International Journal of Environmental Research and Public Health 18, no. 6: 3127. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063127