
Dose-Response Association of Tai Chi and Cognition among Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Screening and Selection Strategy
2.4. Data Extraction
2.5. Assessment of Methodological Quality
2.6. Statistical Analyses
3. Results
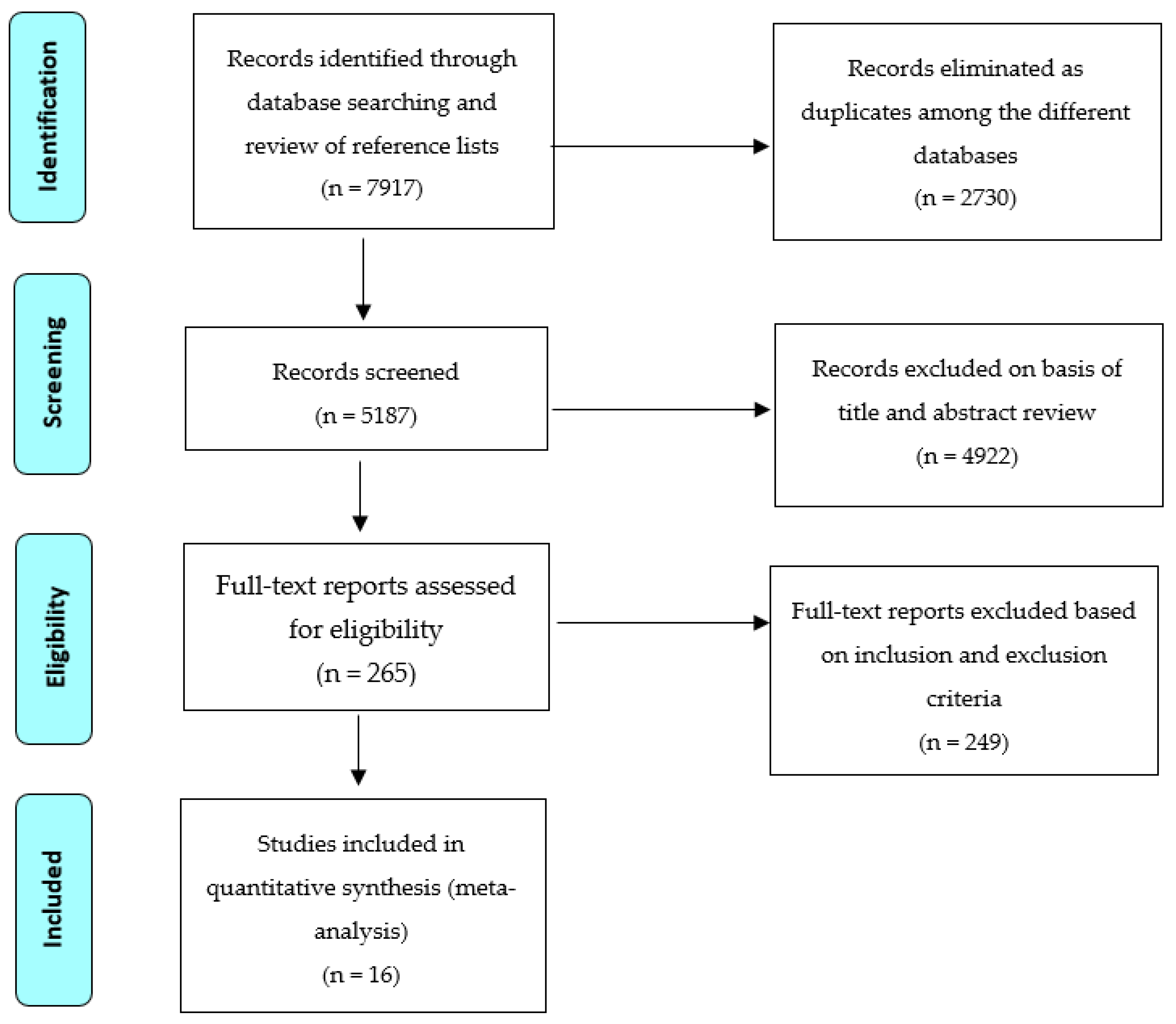
3.1. Selection of Eligible Studies
3.2. Study Characteristics
3.3. Methodological Quality of Included Studies
3.4. Meta-Analysis Results
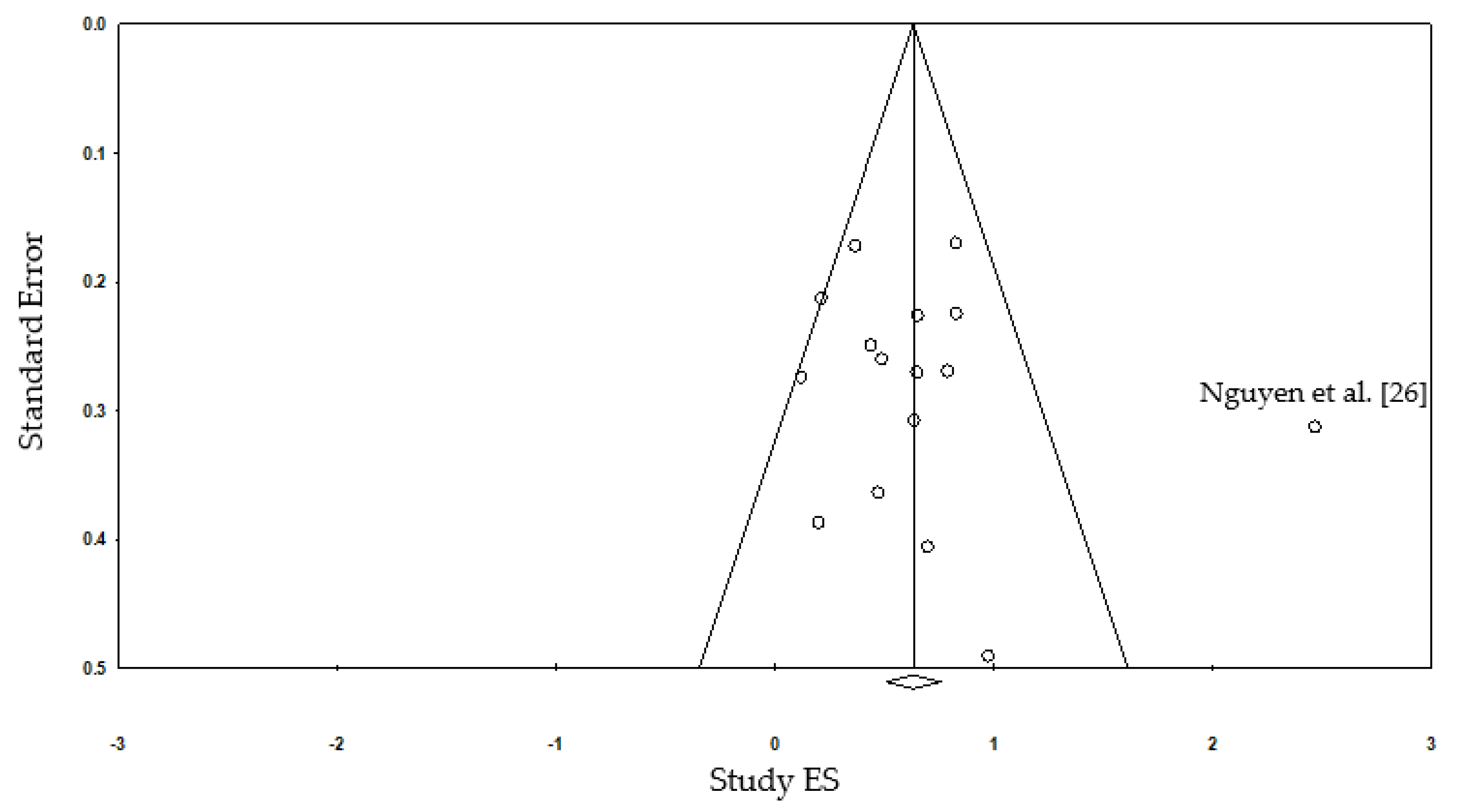
3.5. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 10 July 2020).
- 2020 Alzheimer’s Disease Facts and Figures. Alzheimers Dement. 2020, 16, pp. 391–460. Available online: https://0-alz--journals-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1002/alz.12068 (accessed on 10 July 2020). [CrossRef] [PubMed]
- Hurd, M.D.; Martorell, P.; Delavande, A.; Mullen, K.J.; Langa, K.M. Monetary costs of dementia in the United States. N. Engl. J. Med. 2013, 368, 1326–1334. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.-L. The growing costs and burden of family caregiving of older adults: A review of paid sick leave and family leave policies. Gerontologist 2016, 56, 391–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.K.; Nien, Y.H.; Tsai, C.L.; Etnier, J.L. Physical activity and cognition in older adults: The potential of Tai Chi Chuan. J. Aging Phys. Act. 2010, 18, 451–472. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Siu, K.C.; Fu, S.N.; Hui-Chan, C.W.Y.; Tsang, W.W.N. Effects of Tai Chi training on postural control and cognitive performance while dual tasking—A randomized clinical trial. J. Complement. Integr. Med. 2016, 13, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Tao, J.; Liu, J.; Egorova, N.; Chen, X.; Sun, S.; Xue, X.; Kong, J. Increased hippocampus–medial prefrontal cortex resting-state functional connectivity and memory function after Tai Chi Chuan practice in elder adults. Front. Aging Neurosci. 2016, 8, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Piliae, R.E.; Newell, K.A.; Cherin, R.; Lee, M.J.; King, A.C.; Haskell, W.L. Effects of Tai Chi and western exercise on physical and cognitive functioning in healthy community-dwelling older adults. J. Aging Phys. Act. 2010, 18, 261–279. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.M.; Taylor-Piliae, R.E. Effects of Tai Chi on cognitive function in community dwelling older adults: A review. Geriatr. Nurs. 2014, 35, 9–19. [Google Scholar] [CrossRef]
- Wayne, P.M.; Walsh, J.N.; Taylor-Piliae, R.E.; Wells, R.E.; Papp, K.V.; Donovan, N.J.; Yeh, G.Y. The impact of Tai Chi on cognitive performance in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2014, 62, 25–39. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, Y.; Burgess, E.O.; Wu, J. The effects of Tai Chi exercise on cognitive function in older adults: A meta-analysis. J. Sport Health Sci. 2013, 2, 193–203. [Google Scholar] [CrossRef] [Green Version]
- Zheng, G.; Liu, F.; Li, S.; Huang, M.; Tao, J.; Chen, L. Tai Chi and the protection of cognitive ability: A systematic review of prospective studies in healthy adults. Am. J. Prev. Med. 2015, 49, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Xiang, Y.Q.; Ungvari, G.S.; Chiu, H.F.K.; Ning, Y.P.; Yu, X.; Forester, B.P.; Xiang, Y.T. Tai Chi for mild cognitive impairment: A systematic review. Psychogeriatrics 2017, 17, 514–516. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Br. Med. J. 2009, 339, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Man, D.W.K.; Tsang, W.W.N.; Hui-Chan, C.W.Y. Do older Tai Chi practitioners have better attention and memory function? J. Altern. Complement. Med. 2010, 16, 1259–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortimer, J.A.; Ding, D.; Borenstein, A.R.; DeCarli, C.; Guo, Q.; Wu, Y.; Chu, S. Changes in brain volume and cognition in a randomized trial of exercise and social interaction in a community-based sample of non-demented Chinese elders. J. Alzheimers Dis. 2012, 30, 757–766. [Google Scholar] [CrossRef] [Green Version]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.; Rothstein, H.R. Introduction to Meta-Analysis; Wiley: West Sussex, UK, 2009; ISBN 9780470057247. [Google Scholar]
- Chu, D.M.; Lim-Khoo, W. Comparison of performance in minimental state examination (MMSE) and montreal cognitive assessment scale (MOCA) of elderly engaged in Tai Chi versus aerobic physical exercise. Alzheimers Dement. 2014, 10, 607. [Google Scholar] [CrossRef]
- Overton-McCoy, A. The Association between Tai Chi and Memory in Older Adults. Ph.D. Thesis, Capella University, Minneapolis, MN, USA, 2010. [Google Scholar]
- Kasai, J.Y.T.; Busse, A.L.; Magaldi, R.M.; Soci, M.A.; Rosa, P.d.M.; Curiati, J.A.E.; Jacob Filho, W. Effects of Tai Chi Chuan on cognition of elderly women with mild cognitive impairment. Einstein (São Paulo) 2010, 8, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Sungkarat, S.; Boripuntakul, S.; Chattipakorn, N.; Watcharasaksilp, K.; Lord, S.R. Effects of Tai Chi on cognition and fall risk in older adults with mild cognitive impairment: A randomized controlled trial. J. Am. Geriatr. Soc. 2017, 65, 721–727. [Google Scholar] [CrossRef]
- Hung, H.C.; Chang, Y.J.; Lai, R.S.; Chen, T.C.C. Effects of community-based Tai Chi exercise on health-related physical fitness and cognitive functions in the elderly. J. Nurs. Healthc. Res. 2013, 9, 271–281. [Google Scholar]
- Lu, X.; Siu, K.C.; Fu, S.N.; Hui-Chan, C.W.Y.; Tsang, W.W.N. Tai Chi practitioners have better postural control and selective attention in stepping down with and without a concurrent auditory response task. Eur. J. Appl. Physiol. 2013, 113, 1939–1945. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.H.; Kruse, A. A randomized controlled trial of Tai Chi for balance, sleep quality and cognitive performance in elderly Vietnamese. Clin. Interv. Aging 2012, 7, 185–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orozco Calderón, G.; Anaya Chávez, M.; Santiago Vite, J.; Viedma, R.G.; Del, M. Cognition, activities of daily living and psychological variables in elderly women practitioners of Tai Chi Chuan. RETOS-Neuvas Tend. en Educ. Fis. Deporte y Recreacion 2016, 30, 222–225. [Google Scholar]
- Sun, J.; Kanagawa, K.; Sasaki, J.; Ooki, S.; Xu, H.; Wang, L. Tai Chi improves cognitive and physical function in the elderly: A randomized controlled trial. J. Phys. Ther. Sci. 2015, 27, 1467–1471. [Google Scholar] [CrossRef] [Green Version]
- Tsang, W.W.N.; Kwok, J.C.Y.; Hui-Chan, C.W.Y. Effects of aging and Tai Chi on a finger-pointing task with a choice paradigm. Evid. Based Complement. Alternat. Med. 2013, 2013, 653437. [Google Scholar] [CrossRef] [PubMed]
- Varghese, R.; Hui-Chan, C.W.Y.; Bhatt, T. Reduced cognitive-motor interference on voluntary balance control in older Tai Chi practitioners. J. Geriatr. Phys. Ther. 2016, 39, 190–199. [Google Scholar] [CrossRef]
- Kyzas, P.A.; Loizou, K.T.; Ioannidis, J.P. Selective reporting biases in cancer prognostic factor studies. J. Natl. Cancer Inst. 2005, 97, 1043–1055. [Google Scholar] [CrossRef]
- Hopewell, S.; Clarke, M.; Mallet, S. Grey literature and systematic reviews. In Publication Bias in Meta-Analysis; Rothstein, H.R., Sutton, A.J., Borenstein, M., Eds.; Wiley: West Sussex, UK, 2005; pp. 49–72. ISBN 9780470870143. [Google Scholar]
- Gangadhar, B.; Hariprasad, V.; Varambally, S.; Shivakumar, V.; Kalmady, S.; Venkatasubramanian, G. Yoga increases the volume of the hippocampus in elderly subjects. Indian J. Psychiatry 2013, 55, 394–396. [Google Scholar] [CrossRef]
- O’Shea, A.; Cohen, R.A.; Porges, E.C.; Nissim, N.R.; Woods, A.J. Cognitive aging and the hippocampus in older adults. Front. Aging Neurosci. 2016, 8, 298. [Google Scholar] [CrossRef]
- Colcombe, S.J.; Erickson, K.I.; Scalf, P.E.; Kim, J.S.; Prakash, R.; McAuley, E.; Elavsky, S.; Marquez, D.X.; Hu, L.; Kramer, A.F. Aerobic exercise training increases brain volume in aging humans. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1166–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erickson, K.I.; Prakash, R.S.; Voss, M.W.; Chaddock, L.; Hu, L.; Morris, K.S.; White, S.M.; Wójcicki, T.R.; McAuley, E.; Kramer, A.F. Aerobic fitness is associated with hippocampal volume in elderly humans. Hippocampus 2009, 19, 1030–1039. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Li, C.; Zou, L.; Liu, X.; Song, W. The effects of mind-body exercise on cognitive performance in elderly: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2018, 15, 2791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiesa, A.; Calati, R.; Sterretti, A. Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clin. Psychol. Rev. 2011, 31, 449–464. [Google Scholar] [CrossRef]
- Kim, T.H.M.; Pascual-Leone, J.; Johnson, J.; Tamim, H. The mental-attention Tai Chi effect with older adults. BMC Psychol. 2016, 4, 29. [Google Scholar] [CrossRef] [Green Version]
- Lupien, S.J.; de Leon, M.; de Santi, S.; Convit, A.; Tarshish, C.; Nair, N.P.; Thakur, M.; McEwen, B.S.; Hauger, R.L.; Meaney, M.J. Cortisol levels during human aging predict hippocampal atrophy and memory deficits. Nat. Neurosci. 1998, 1, 69–73. [Google Scholar] [CrossRef]
- Colcombe, S.J.; Erickson, K.I.; Raz, N.; Webb, A.G.; Cohen, N.J.; McAuley, E.; Kramer, A.F. Aerobic fitness reduces brain tissue loss in aging humans. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 176–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, A.C.; Huddleston, D.E.; Brickman, A.M.; Sosunov, A.A.; Hen, R.; McKhann, G.M.; Sloan, R.; Gage, F.H.; Brown, T.R.; Small, S.A. An in vivo correlate of exercise-induced neurogenesis in the adult dentate gyrus. Proc. Natl. Acad. Sci. USA 2007, 104, 5638–5643. [Google Scholar] [CrossRef] [Green Version]
- Voss, M.W.; Prakash, R.S.; Erickson, K.I.; Basak, C.; Chaddock, L.; Kim, J.S.; Alves, H.; Heo, S.; Szabo, A.N.; White, S.M.; et al. Plasticity of brain networks in a randomized intervention trial of exercise training in older adults. Front. Aging Neurosci. 2010, 2, 32. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.; Wang, C.; Ho, R.T.; Ziea, E.T.; Wong, V.C.T. Tai Chi exercise for patients with heart disease: A systematic review of controlled clinical trials. Altern. Ther. Health Med. 2012, 18, 16–22. [Google Scholar] [PubMed]
- Wolf, S.L.; O’Grady, M.; Easley, K.A.; Guo, Y.; Kressig, R.W.; Kutner, M. The influence of intense Tai Chi training on physical performance and hemodynamic outcomes in transitionally frail, older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.W.K.; Sit, J.W.H.; Chair, S.Y.; Leung, D.Y.P.; Lee, D.T.F.; Wong, E.M.L.; Fung, L.C.W. Evaluation of the effectiveness of Tai Chi versus brisk walking in reducing cardiovascular risk factors: Protocol for a randomized controlled trial. Int. J. Environ. Res. Public Health 2016, 13, 682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stagg, N.J.; Mata, H.P.; Ibrahim, M.M.; Henriksen, E.J.; Porreca, F.; Vanderah, T.W.; Philip Malan, T. Regular exercise reverses sensory hypersensitivity in a rat neuropathic pain model: Role of endogenous opioids. Anesthesiology 2011, 114, 940–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polaski, A.M.; Phelps, A.L.; Kostek, M.C.; Szucs, K.A.; Kolber, B.J. Exercise-induced hypoalgesia: A meta-analysis of exercise dosing for the treatment of chronic pain. PLoS ONE 2019, 14, e0210418. [Google Scholar] [CrossRef] [Green Version]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Sanders, L.M.J.; Hortobágyi, T.; la Bastide-van Gemert, S.; van der Zee, E.A.; van Heuvelen, M.J.G. Dose-response relationship between exercise and cognitive function in older adults with and without cognitive impairment: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0210036. [Google Scholar] [CrossRef]
- Chang, J.Y.; Tsai, P.F.; Beck, C.; Hagen, J.L.; Huff, D.C.; Anand, K.J.S.; Roberson, P.K.; Rosengren, K.S.; Beuscher, L. The effect of Tai Chi on cognition in elders with cognitive impairment. Medsurg Nurs. 2011, 20, 63–69. [Google Scholar]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, D.E.; Bellettiere, J.; Gardiner, P.A.; Villarreal, V.N.; Crist, K.; Kerr, J. Independent associations between sedentary behaviors and mental, cognitive, physical and functional health among older adults in retirement communities. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 78–83. [Google Scholar] [CrossRef] [Green Version]
- Vaynman, S.; Gomez-Pinilla, F. Revenge of the “sit”: How lifestyle impacts neuronal and cognitive health through molecular systems that interface energy metabolism with neuronal plasticity. J. Neurosci. Res. 2006, 84, 699–715. [Google Scholar] [CrossRef]
- Voss, M.; Carr, L.; Cole, R.; Weng, T. Revenge of the “sit” II: Does lifestyle impact neuronal and cognitive health through distinct mechanisms associated with sedentary behavior and physical activity? Ment. Health Phys. Act. 2014, 7, 9–24. [Google Scholar] [CrossRef]
- Sutton, A.J. Publication bias. In The Handbook of Research Synthesis and Meta-Analysis, 2nd ed.; Cooper, H., Hedges, L.V., Valentine, J.C., Eds.; Russell Sage Foundation: New York, NY, USA, 2009; pp. 435–452. ISBN 978-0871541635. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Studies/ Locations | Study Design | Study Population | Tai Chi Style | Intervention Modality | Total Tai Chi Dose | Control Group | Cognitive Outcome Measurement |
|---|---|---|---|---|---|---|---|
| Chu et al. 2014 [20] Philippines | Cross-sectional | I: n = 30 I (mean age): 69.30 C: n = 30 C (mean age): 64.60 No reported cognitive impairment | Not Specified | At least 30 min a day, 3 times/week for 6 months | 2160 min | No exercise | MMSE 1 MoCA 2 |
| Hung et al. 2013 [24] Taiwan | Quasi experimental | I: n = 41 I (mean age): 76.61 C: n = 41 C (mean age): 76.29 No cognitive impairment | Not Specified | 90 min/session 3 times/week for 12 weeks * including warm up and cool down | 1440 min | No exercise | MMSE 1 |
| Kasai et al. 2010 [22] Brazil | Non-randomized experimental | I: n = 13 I (mean age): 73.54 C: n = 13 C (mean age): 75.54 Mild Cognitive Impairment | Yang-style | 60 min/session 2 times/week for 13 weeks * including warm up and cool down | 1560 min * including warm up and cool down | No exercise | RBMT 3 SMC 4 DSF 5 DSB 6 |
| Lu et al. 2013 [25] Hong Kong | Cross-sectional | I: n = 28 I (mean age): 73.60 C: n = 30 C (mean age): 72.40 No cognitive impairment | Not Specified | Minimum weekly 1.5 h practice for 3 years | 14,040 min | No exercise | Auditory Stroop Test Center of Pressure Path (mm)/Area (cm2) |
| Lu et al. 2016 [6] Hong Kong | RCT | I: n = 13 I (mean age): 72.80 C: n = 14 C (mean age): 67.30 No cognitive impairment | Yang style | 60 min/session 3 times/week for 16 weeks | 2880 min | No exercise, attended weekly series of music, English, handicrafts and fall prevention classes along with social gatherings | Auditory Stroop Test Center of Pressure Path (mm)/Area (cm2) Time to Complete Step-Down Performance |
| Man et al. 2010 [15] Hong Kong | Cross-sectional | I: n = 42 I (mean age): 68.90 C: n = 44 C (mean age): 68.20 No cognitive impairment | Ng style | at least 45 min per session, 3 times/week for 3 years | 21060 min | No exercise | HKLLT 7 |
| Mortimer et al. 2012 [16] China | RCT | I: n = 29 I (mean age): 67.3 C: n = 24 C2: n = 27 C (mean age): 68.2 C2 (mean age): 67.90 No cognitive impairment | Not Specified | 20 min/session 3 times/week for 40 weeks | 2400 min | C: No exercise C2: Social interaction | Mattis Dementia Rating Scale BNT 8 Clock Drawing Test Trail Making Test WAIS-R 9 Similarities Test Category Verbal Fluency Test Auditory Verbal Learning Test Stroop Test Rey-Osterrieth Complex Figure Bell Cancellation Test WAIS-R 9 Digit Span |
| Nguyen et al. 2012 [26] Vietnam | RCT | I: n = 48 I (mean age): 69.32 C: n = 48 C (mean age): 68.73 No cognitive impairment | 24-form | 30 min/session 2 times/week for 24 weeks | 1440 min | No exercise | Trail Making Test |
| Orozco Calderon et al. 2016 [27] Mexico | Cross-sectional | I: n = 17 I (mean age): 70.65 C: n = 15 C (mean age): 67.40 No reported cognitive impairment | Yang-style | 4 h/week for 4.5 years | Not specified | No exercise | COGNISTAT Test |
| Overton-McCoy 2010 [21] USA | Cross-sectional | I: n = 75 I (mean age): 70.80 C: n = 75 C (mean age): 71.31 No cognitive impairment | Not Specified | 1–2 times per week; average of 60 min per week for a minimum of one month | Not specified | No exercise | MMSE 1 15-item BNT 8 15-item BNT 8 Latency Score |
| Sun et al. 2015 [28] China | RCT | I: n = 72 I (mean age): 68.30 C n = 66 C (mean age): 70.10 No cognitive impairment | 24-form Yang-style | 60 min/session 2 times/week for 6 months * including warm up and cool down | 3120 min * including warm up and cool down | No exercise | MMSE 1 FAB 10 |
| Sungkarat et al. 2017 [23] Thailand | RCT | I: n = 33 I (mean age): 68.3 C: n = 33 C (mean age): 67.5 Mild Cognitive Impairment | 10-form | 30 min/session 3 times/week for 15 weeks | 1350 min | Health education related to cognitive and fall prevention | Logical Memory Delayed Recall Score; DSF 5 DSB 6 Block Design Score Trail Making Test Hand Reaction Time |
| Tao et al. 2016 [7] China | RCT | I: n = 21 I (mean age): 62.38 C: n = 25 C (mean age): 59.76 No cognitive impairment | 24-form Yang-style | 30 min/session 5 times/week for 12 weeks | 1800 min | Health education | Weschler Memory Scale—Chinese Revision |
| Taylor-Piliae et al. 2010 [8] USA | RCT | I: n = 37 I (mean age): 70.60 C: n = 56 C (mean age): 68.20 No reported cognitive impairment | 12 short-form Yang-style | Daily practice encouraged for 6 months | Not specified | Health education | Animal-Naming Test DSF 5 DSB 6 |
| Tsang et al. 2013 [29] Hong Kong | Cross-sectional | I: n = 31 I (mean age): 70.30 C: n = 30 C (mean age): 72.30 No cognitive impairment | Not Specified | Minimum 90 min/week for 3 years | 14,040 min | No exercise | EMG 11 Reaction Time EMG 11 Movement Time End-Point Accuracy Wrong Movement |
| Varghese et al. 2016 [30] USA | Cross-sectional | I: n = 10 I (mean age): 65.90 C: n = 10 C (mean age): 66.40 No cognitive impairment | Not Specified | Minimum 100 h in past year | Not specified | No exercise | Reaction Time Maximal Excursion Value (%) Cognitive Score |
| Studies | Average Component Ratings (1–3 score) | Average Global Rating (1–3 Score) | |||||
|---|---|---|---|---|---|---|---|
| Selection Bias | Study Design | Confounders | Blinding | Data Collection Methods | Withdrawals and Dropouts | ||
| Chu et al. 2014 [20] | 3.00 | 2.00 | 3.00 | 2.00 | 1.00 | 1.33 | 3.00 |
| Hung et al. 2013 [24] | 2.00 | 1.00 | 1.00 | 2.00 | 1.00 | 1.00 | 1.00 |
| Kasai et al. 2010 [22] | 2.33 | 1.00 | 1.00 | 2.00 | 1.00 | 1.00 | 1.33 |
| Lu et al. 2013 [25] | 2.00 | 2.00 | 1.00 | 2.33 | 1.00 | 1.33 | 1.33 |
| Lu et al. 2016 [6] | 2.00 | 1.00 | 1.00 | 2.00 | 1.00 | 1.00 | 1.00 |
| Man et al. 2010 [15] | 1.33 | 2.00 | 1.00 | 2.00 | 1.00 | 1.00 | 1.00 |
| Mortimer et al. 2012 [16] | 1.67 | 1.00 | 1.00 | 2.00 | 1.00 | 1.00 | 1.00 |
| Nguyen et al. 2012 [26] | 2.00 | 1.00 | 1.33 | 2.33 | 1.00 | 1.33 | 1.67 |
| Orozco Calderon et al. 2016 [27] | 2.00 | 2.00 | 1.00 | 2.00 | 1.00 | 1.33 | 1.00 |
| Overton-McCoy 2010 [21] | 2.00 | 2.00 | 3.00 | 3.00 | 1.00 | 1.00 | 3.00 |
| Sun et al. 2015 [28] | 2.33 | 1.00 | 1.00 | 2.00 | 1.00 | 1.00 | 1.33 |
| Sungkarat et al. 2017 [23] | 2.00 | 1.00 | 1.00 | 2.00 | 1.00 | 1.00 | 1.00 |
| Tao et al. 2016 [7] | 2.00 | 1.00 | 1.00 | 2.00 | 1.00 | 2.00 | 1.00 |
| Taylor-Piliae et al. 2010 [8] | 2.33 | 1.00 | 1.00 | 2.00 | 1.00 | 1.33 | 1.33 |
| Tsang et al. 2013 [29] | 2.00 | 2.00 | 1.00 | 2.33 | 2.00 | 2.00 | 1.67 |
| Varghese et al. 2016 [30] | 2.00 | 2.00 | 1.00 | 2.33 | 1.00 | 1.33 | 1.33 |
| Moderator Variable | Slope | p-Value |
|---|---|---|
| Tai Chi session duration (min) (12 studies) | −0.0025 min−1 | 0.8115 |
| Tai Chi practice duration per week (min) (including warm-up and cool-down) (15 studies) | −0.0020 min−1 | 0.2380 |
| Study duration (weeks) (15 studies) | −0.0005 wk−1 | 0.7913 |
| Tai Chi practice duration for entire study (min) (16 studies) | −0.0000 min−1 | 0.6588 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, M.-L.; Wotiz, S.B.; Banks, S.M.; Connors, S.A.; Shi, Y. Dose-Response Association of Tai Chi and Cognition among Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3179. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063179
Chen M-L, Wotiz SB, Banks SM, Connors SA, Shi Y. Dose-Response Association of Tai Chi and Cognition among Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(6):3179. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063179
Chicago/Turabian StyleChen, Mei-Lan, Stephanie B. Wotiz, Starr M. Banks, Sabine A. Connors, and Yuyin Shi. 2021. "Dose-Response Association of Tai Chi and Cognition among Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 6: 3179. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063179