
Self-Reported Satisfaction to Treatment, Quality of Life and General Health of Type 2 Diabetes Patients with Inadequate Glycemic Control from North-Eastern Romania

 , ,
, , 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology for Collecting Patient-Reported Outcomes
2.2. Statistical Analysis
3. Results
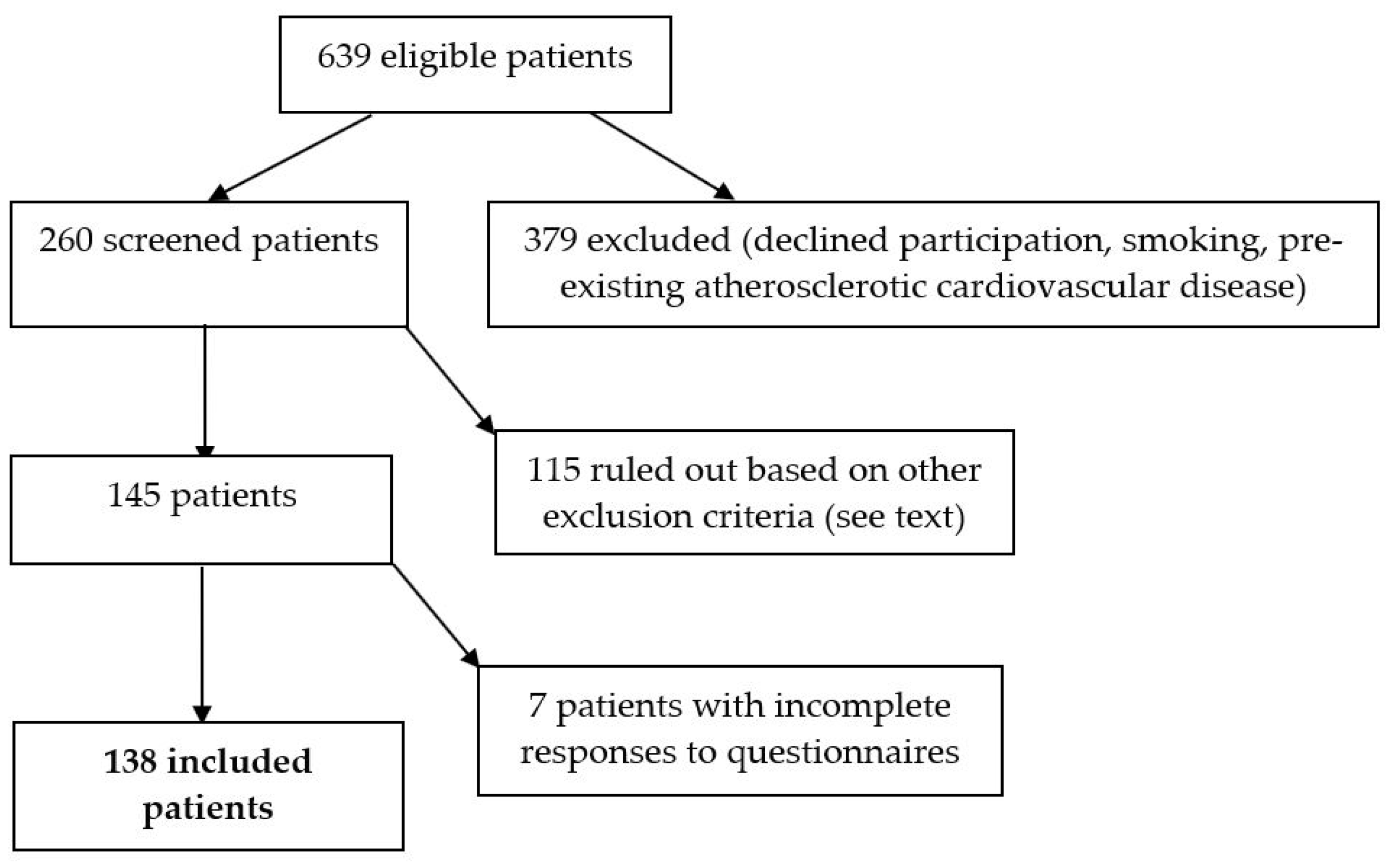
3.1. General and Clinical Characteristics of the Study Cohort
3.2. Patient-Reported Outcomes
4. Discussion
4.1. Satisfaction to Treatment (DTSQ)
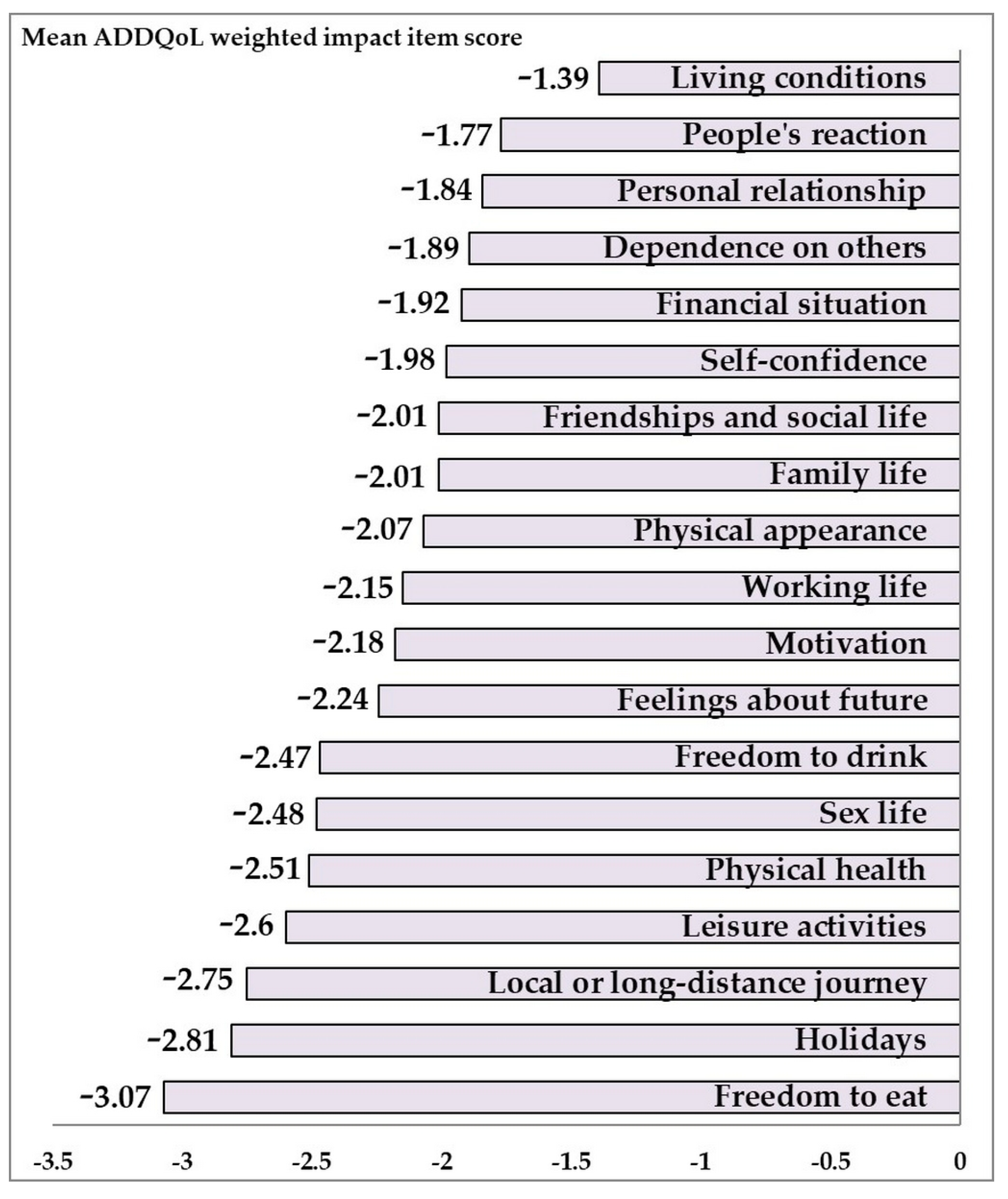
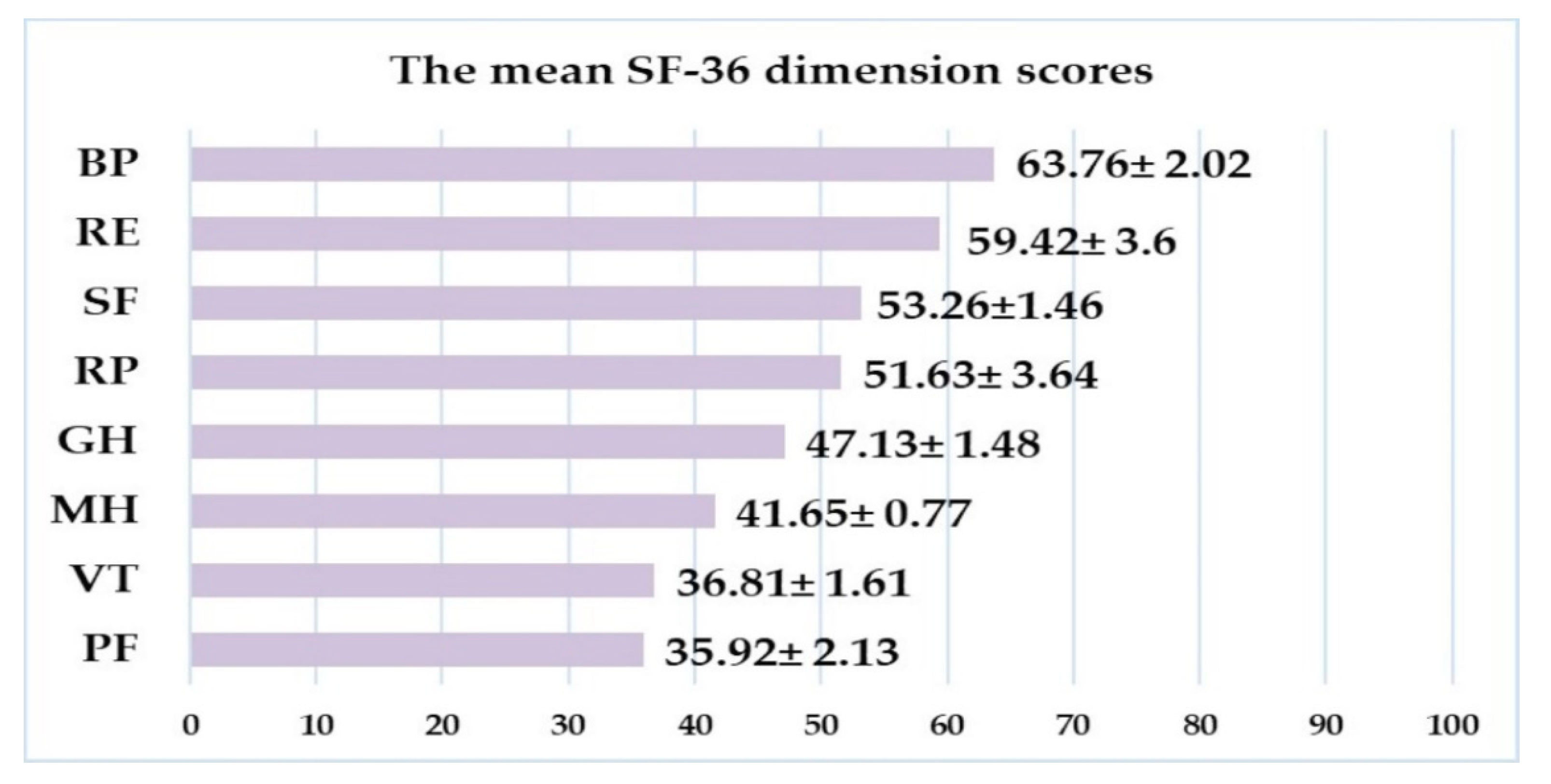
4.2. Quality of Life (ADDQoL and SF-36)
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- Mota, M.; Popa, S.; Mota, E.; Mitrea, A.; Catrinoiu, D.; Cheta, D.; Guja, C.; Hancu, N.; Ionescu-Tirgoviste, C.; Lichiardopol, R.; et al. Prevalence of diabetes mellitus and prediabetes in the adult Romanian population: PREDATORR study. J. Diabetes 2015, 8, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Buse, J.; Wexler, D.; Tsapas, A.; Rossing, P.; Mingrone, G.; Mathieu, C.; D’Alessio, D.; Davies, M. 2019 update to: Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2019, 63, 221–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeFronzo, R.A. Pathogenesis of Type 2 Diabetes Mellitus. In Diabetes Epidemiology, Genetics, Pathogenesis, Diagnosis, Prevention, and Treatment; Bonora, E., DeFronzo, R., Eds.; Springer: Cham, Switzerland, 2018; pp. 181–253. [Google Scholar]
- Cosentino, F.; Grant, P.; Aboyans, V.; Bailey, C.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.; Hansen, T.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2019, 41, 255–323. [Google Scholar] [CrossRef] [Green Version]
- Young-Hyman, D.; de Groot, M.; Hill-Briggs, F.; Gonzalez, J.; Hood, K.; Peyrot, M. Psychosocial Care for People with Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2126–2140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S48–S65. [Google Scholar] [CrossRef] [Green Version]
- Robinson, D.J.; Coons, M.; Haensel, H.; Vallis, M.; Yale, J.-F. Diabetes Canada 2018 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada: Diabetes and Mental Health. Can. J. Diabetes 2018, 42, S130–S141. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, M.A.; Moles, R.J.; Harrison, J.; Chen, T.F. Health Outcomes and Quality of Life. In Encyclopedia of Pharmacy Practice and Clinical Pharmacy; Bahar, Z.-U.-D., Ed.; Elsevier: Amsterdam, The Netherlands, 2019; Volume 3A, pp. 59–72. [Google Scholar]
- Chen, Y.; Tan, Y.; Cheen, M.; Wee, H. Patient-Reported Outcome Measures in Registry-Based Studies of Type 2 Diabetes Mellitus: A Systematic Review. Curr. Diabetes Rep. 2019, 19, 1–17. [Google Scholar] [CrossRef]
- Trikkalinou, A.; Papazafiropoulou, A.; Melidonis, A. Type 2 diabetes and quality of life. World J. Diabetes 2017, 8, 120. [Google Scholar] [CrossRef] [PubMed]
- Palamenghi, L.; Carlucci, M.; Graffigna, G. Measuring the Quality of Life in Diabetic Patients: A Scoping Review. J. Diabetes Res. 2020, 2020, 1–19. [Google Scholar] [CrossRef]
- Speight, J.; Reaney, M.; Barnard, K. Not all roads lead to Rome—a review of quality of life measurement in adults with diabetes. Diabetes Med. 2009, 26, 315–327. [Google Scholar] [CrossRef]
- El Achhab, Y.; Nejjari, C.; Chikri, M.; Lyoussi, B. Disease-specific health-related quality of life instruments among adults diabetic: A systematic review. Diabetes Res. Clin. Pract. 2008, 80, 171–184. [Google Scholar] [CrossRef]
- Speight, J.; Holmes-Truscott, E.; Hendrieckx, C.; Skovlund, S.; Cooke, D. Assessing the impact of diabetes on quality of life: What have the past 25 years taught us? Diabet. Med. 2020, 37, 483–492. [Google Scholar] [CrossRef] [Green Version]
- Nair, R.; Kachan, P. Outcome tools for diabetes-specific quality of life. Can. Fam Physician 2017, 63, e310–e315. [Google Scholar]
- Tang, T.; Yusuf, F.; Polonsky, W.; Fisher, L. Assessing quality of life in diabetes: II-Deconstructing measures into a simple framework. Diabetes Res. Clin. Pract. 2017, 126, 286–302. [Google Scholar] [CrossRef]
- ICHOM Diabetes in Adults Working Group, Type 1 and Type 2 Diabetes in Adults, November 2018, Data Collection Reference Guide. Version 1.0.0 Revised February 28th. 2019. Available online: https://ichom.org/files/medical-conditions/diabetes-in-adults/dia-reference-guide.pdf (accessed on 3 November 2020).
- Sasseville, M.; Chouinard, M.; Fortin, M. Patient-reported outcomes in multimorbidity intervention research: A scoping review. Int. J. Nurs. Stud. 2018, 77, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Sayah, F.; Qiu, W.; Xie, F.; Johnson, J. Comparative performance of the EQ-5D-5L and SF-6D index scores in adults with type 2 diabetes. Qual. Life Res. 2017, 26, 2057–2066. [Google Scholar] [CrossRef] [PubMed]
- Ara, R.; Brazier, J. Predicting the Short Form-6D Preference-Based Index Using the Eight Mean Short Form-36 Health Dimension Scores: Estimating Preference-Based Health-Related Utilities When Patient Level Data Are not Available. Value Health 2009, 12, 346–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinyard, L.; Geremakis, C. Assessing Health Related Quality of Life in Persons with Diabetes: A Comparison of Generic Measures. Open Public Health J. 2016, 9, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Grigorescu, E.-D.; Lacatusu, C.-M.; Floria, M.; Mihai, B.-M.; Cretu, I.; Sorodoc, L. Left Ventricular Diastolic Dysfunction in Type 2 Diabetes—Progress and Perspectives. Diagnostics 2019, 9, 121. [Google Scholar] [CrossRef] [Green Version]
- Nagueh, S.; Smiseth, O.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, C.; Gamsu, D.S. Guidelines for encouraging psychological well-being: Report of a Working Group of the World Health Organization Regional Office for Europe and International Diabetes Federation European Region St Vincent Declaration Action Programme for Diabetes. Diabet. Med. 1994, 11, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C.; Todd, C.; Gorton, T.; Symonds, E.; Martin, A.; Plowright, R. The development of an individualized questionnaire measure of perceived impact of diabetes on quality of life: The ADDQoL. Qual. Life Res. 1999, 8, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Bala, C.; Mocanu, A. Aspecte psihosociale în nutriție și bolile metabolice. In Diabetul Zaharat, Nutriția Și Bolile Metabolice; Hâncu, N., Roman, G., Vereșiu, I.A., Eds.; Echinox: Cluj-Napoca, Romania, 2010; Volume 1, pp. 245–249. [Google Scholar]
- Classification of Diabetes Mellitus. Geneva: World Health Organization 2019. Available online: http://apps.who.int/iris/bitstream/handle/10665/325182/9789241515702-eng.pdf (accessed on 1 February 2021).
- Saisho, Y. Use of Diabetes Treatment Satisfaction Questionnaire in Diabetes Care: Importance of Patient-Reported Outcomes. Int. J. Environ. Res. Public Health 2018, 15, 947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, C. The Diabetes Treatment Satisfaction Questionnaire (DTSQ). Available online: https://www.healthpsychologyresearch.com/sites/default/files/guidelines/DTSQ%20Summary%20rev_11.8.15_web.pdf (accessed on 30 November 2015).
- Bradley, C.; Speight, J. Patient perceptions of diabetes and diabetes therapy: Assessing quality of life. Diabetes/Metab. Res. Rev. 2002, 18, 64–69. [Google Scholar] [CrossRef]
- Ware, J.; Kosinski, M.; Bjorner, J.; Turner-Bowker, D.; Gandek, B.; Maruish, M. Development. User’s Manual for the SF-36v2® Health Survey; Quality Metric Incorporated: Lincoln, RI, USA, 2007. [Google Scholar]
- Poder, T.; Fauteux, V.; He, J.; Brazier, J. Consistency Between Three Different Ways of Administering the Short Form 6 Dimension Version 2. Value Health 2019, 22, 837–842. [Google Scholar] [CrossRef]
- Kharroubi, S.A.; Beyh, Y.; Abdul Fattah, E.; Young, T. The Importance of Accounting for Parameter Uncertainty in SF-6D Value Sets and Its Impact on Studies that Use the SF-6D to Measure Health Utility. Int. J. Environ. Res. Public Health 2020, 17, 3949. [Google Scholar] [CrossRef] [PubMed]
- Poder, T.; Wang, L.; Carrier, N. EQ-5D-5L and SF-6Dv2 utility scores in people living with chronic low back pain: A survey from Quebec. BMJ Open 2020, 10, e035722. [Google Scholar] [CrossRef]
- Mulhern, B.; Bansback, N.; Norman, R.; Brazier, J. Valuing the SF-6Dv2 Classification System in the United Kingdom Using a Discrete-choice Experiment with Duration. Med. Care 2020, 58, 566–573. [Google Scholar] [CrossRef]
- Levterova, B.; Dimitrova, D.; Levterov, G.; Dragova, E. Instruments for Disease-Specific Quality-of-Life Measurement in Patients with Type 2 Diabetes Mellitus—A Systematic Review. Folia Med. 2013, 55, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Holmes-Truscott, E.; Cooke, D.; Hendrieckx, C.; Coates, E.; Heller, S.; Speight, J. A comparison of the acceptability and psychometric properties of scales assessing the impact of type 1 diabetes on quality of life—Results of ‘YourSAY: Quality of Life’. Diabet. Med. 2021, 37, e14524. [Google Scholar] [CrossRef]
- Abbatecola, A.; Spazzafumo, L.; Fabbietti, P.; Testa, R.; Rabini, R.; Bonfigli, A.; Corsonello, A.; Lattanzio, F.; Paolisso, G. Diabetes-related quality of life is enhanced by glycaemic improvement in older people. Diabet. Med. 2014, 32, 243–249. [Google Scholar] [CrossRef]
- Boels, A.; Vos, R.; Hermans, T.; Zuithoff, N.; Müller, N.; Khunti, K.; Rutten, G. What determines treatment satisfaction of patients with type 2 diabetes on insulin therapy? An observational study in eight European countries. BMJ Open 2017, 7, e016180. [Google Scholar] [CrossRef]
- Bradley, C.; Eschwège, E.; de Pablos-Velasco, P.; Parhofer, K.; Simon, D.; Vandenberghe, H.; Gönder-Frederick, L. Predictors of Quality of Life and Other Patient-Reported Outcomes in the PANORAMA Multinational Study of People with Type 2 Diabetes. Diabetes Care 2017, 41, 267–276. [Google Scholar] [CrossRef] [Green Version]
- Kuznetsov, L.; Griffin, S.; Davies, M.; Lauritzen, T.; Khunti, K.; Rutten, G.; Simmons, R. Diabetes-specific quality of life but not health status is independently associated with glycaemic control among patients with type 2 diabetes: A cross-sectional analysis of the ADDITION-Europe trial cohort. Diabetes Res. Clin. Pract. 2014, 104, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Bak, E.; Marcisz, C.; Nowak-Kapusta, Z.; Dobrzyn-Matusiak, D.; Marcisz, E.; Krzeminska, S. Psychometric properties of the Audit of Diabetes-Dependent Quality of Life (ADDQoL) in a population-based sample of Polish adults with type 1 and 2 diabetes. Health Qual. Life Outcomes 2018, 16, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundershausen, R.; Müller, S.; Hashim, M.; Kienhöfer, J.; Kipper, S.; Wilke, T. Quality of Life, Glycemic Control, Safety and Tolerability Associated with Liraglutide or Insulin Initiation in Patients with Type 2 Diabetes in Germany: Results from the Prospective, Non-interventional LIBERTY Study. Exp. Clin. Endocrinol. Diabetes 2018, 128, 170–181. [Google Scholar] [CrossRef]
- Levterova, B.; Orbetzova, M.; Levterov, G.; Dimitrova, D.; Todorov, P. Assessment of the impact of type 2 diabetes on the quality of life by Audit of Diabetes-Dependent Quality-of-Life (ADDQoL-19). Biotechnol. Biotechnol. Equip. 2018, 32, 1627–1634. [Google Scholar] [CrossRef]
- Nicolucci, A.; Cucinotta, D.; Squatrito, S.; Lapolla, A.; Musacchio, N.; Leotta, S.; Vitali, L.; Bulotta, A.; Nicoziani, P.; Coronel, G. Clinical and socio-economic correlates of quality of life and treatment satisfaction in patients with type 2 diabetes. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Papazafiropoulou, A.; Bakomitrou, F.; Trikallinou, A.; Ganotopoulou, A.; Verras, C.; Christofilidis, G.; Bousboulas, S.; Μelidonis, A. Diabetes-dependent quality of life (ADDQOL) and affecting factors in patients with diabetes mellitus type 2 in Greece. BMC Res. Notes 2015, 8, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Arditi, C.; Zanchi, A.; Peytremann-Bridevaux, I. Health status and quality of life in patients with diabetes in Switzerland. Prim. Care Diabetes 2019, 13, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Jing, X.; Chen, J.; Dong, Y.; Han, D.; Zhao, H.; Wang, X.; Gao, F.; Li, C.; Cui, Z.; Liu, Y.; et al. Related factors of quality of life of type 2 diabetes patients: A systematic review and meta-analysis. Health Qual. Life Outcomes 2018, 16, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Engström, M.S.; Leksell, J.; Johansson, U.; Borg, S.; Palaszewski, B.; Franzén, S.; Gudbjörnsdottir, S.; Eeg-Olofsson, K. Health-related quality of life and glycaemic control among adults with type 1 and type 2 diabetes—a nationwide cross-sectional study. Health Qual. Life Outcomes 2019, 17, 1–11. [Google Scholar]
- MacDonald, C.; Nielsen, S.; Bjørner, J.; Johansen, M.; Christensen, R.; Vaag, A.; Lieberman, D.; Pedersen, B.; Langberg, H.; Ried-Larsen, M.; et al. One-year intensive lifestyle intervention and improvements in health- related quality of life and mental health in persons with type 2 diabetes: A secondary analysis of the U-TURN randomized controlled trial. BMJ Open Diabetes Res. Care 2021, 9, e001840. [Google Scholar] [CrossRef]
- Jódar, E.; Michelsen, M.; Polonsky, W.; Réa, R.; Sandberg, A.; Vilsbøll, T.; Warren, M.; Harring, S.; Ziegler, U.; Bain, S. Semaglutide improves health-related quality of life versus placebo when added to standard of care in patients with type 2 diabetes at high cardiovascular risk (SUSTAIN 6). Diabetes Obes. Metab. 2020, 22, 1339–1347. [Google Scholar] [CrossRef] [PubMed]
- Turk, E.; Rupel, V.P.; Tapajner, A.; Leyshon, S.; Isola, A. An Audit of Diabetes-Dependent Quality of Life (ADDQOL) in Older Patients with Diabetes Mellitus Type 2 in Slovenia. Value Health Reg. Issues 2013, 2, 248–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avramopoulos, I. Glycaemic control, treatment satisfaction and quality of life in type 2 diabetes patients in Greece: The PANORAMA study Greek results. World J. Diabetes 2015, 6, 208. [Google Scholar] [CrossRef]
- Russel-Szymczyk, M.; Valov, V.; Savova, A.; Manova, M. Cost-effectiveness of insulin degludec versus insulin glargine U100 in adults with type 1 and type 2 diabetes mellitus in Bulgaria. BMC Endocr. Disord. 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Capehorn, M.; Hallén, N.; Baker-Knight, J.; Glah, D.; Hunt, B. Evaluating the Cost-Effectiveness of Once-Weekly Semaglutide 1 mg Versus Empagliflozin 25 mg for Treatment of Patients with Type 2 Diabetes in the UK Setting. Diabetes Ther. 2021, 12, 537–555. [Google Scholar] [CrossRef]
- Boucher, J.; Evert, A. Effective Nutrition Counseling and Education. In American Diabetes Association Guide to Nutrition Therapy for Diabetes; Evert, A.B., Franz, M.J., Eds.; American Diabetes Association: Alexandria, VA, USA, 2017; Chapter 24; pp. 501–516. [Google Scholar]
- Alcubierre, N.; Rubinat, E.; Traveset, A.; Martinez-Alonso, M.; Hernandez, M.; Jurjo, C.; Mauricio, D. A prospective cross-sectional study on quality of life and treatment satisfaction in type 2 diabetic patients with retinopathy without other major late diabetic complications. Health Qual. Life Outcomes 2014, 12, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Roschkov, S.; Alkhodair, A.; O’Neill, B.; Chik, C.; Tsuyuki, R.; Gyenes, G. The Effect of Nurse Practitioner-Led Intervention in Diabetes Care for Patients Admitted to Cardiology Services. Can. J. Diabetes 2017, 41, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Visockienė, Ž.; Narkauskaitė-Nedzinskienė, L.; Puronaitė, R.; Mikaliūkštienė, A. Validation of the LITHUANIAN version of the 19-item audit of diabetes dependent quality of life (ADDQOL–LT) questionnaire in patients with diabetes. Health Qual. Life Outcomes 2018, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Han, Y.; Shi, J.; Li, R.; Li, S.; Jin, N.; Gu, Y.; Guo, H. Effect of peer education on self-management and psychological status in type 2 diabetes patients with emotional disorders. J. Diabetes Invest. 2014, 6, 479–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouwer, F.; Speight, J. Psyhological Factors and Diabetes Mellitus. In Textbook of Diabetes; Holt, R., Cockram, A., Flyvbjerg, A., Goldstein, B., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2017; Chapter 56; pp. 825–827. [Google Scholar]
- Lavrakas, P. Encyclopedia of Survey Research Methods; SAGE Publications: Thousand Oaks, CA, USA, 2008. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (N = 138) | Variables | Value |
|---|---|---|---|
| Age, years * | 57.86 (8.82) | Glycemia (mg/dL) ** | 162 (46) |
| Gender, N (%) | Insulin (µIU/mL) ** | 11.2 (9.39) | |
| Women | 70 (50.7) | C-peptide (ng/mL) ** | 3.26 (2.22) |
| Men | 68 (49.3) | hs-CRP (mg/dL) ** | 5.35 (9.18) |
| Diabetes duration, years ** | 5 (8) | HbA1c (%) ** | 7.8 (1.12) |
| <5 (N, %) | 63 (45.7) | <7.5 (N, %) | 46 (33.3) |
| 5–10 (N, %) | 39 (28.2) | 7.5–8 (N, %) | 42 (30.4) |
| ≥10 (N, %) | 36 (26.1) | ≥8 (N, %) | 50 (36.3) |
| BMI (kg/m2) * | 32.65 (5.50) | Total cholesterol (mg/dL) * | 195.33 (46.14) |
| Hypertension, N (%) | 93 (67.39) | HDL-cholesterol (mg/dL) * | 56.79 (15.27) |
| Dyslipidemia, N (%) | 99 (71.74) | LDL-cholesterol (mg/dL) * | 103.12 (38.96) |
| Steatohepatitis, N (%) | 104 (75.46) | Triglycerides (mg/dL) * | 202.57 (90.46) |
| Neuropathy, N (%) | 61 (44.20) | Uric acid (mg/dL) * | 5.48 (1.43) |
| Retinopathy, N (%) | 10 (7.24) | eGFR (mL/min/1.73 m2 * | 82 (16.37) |
| Diastolic dysfunction, N (%) | 83 (60.14) | ACR (mg/g) * | 27.14 (48.64) |
| Items of DTSQ’s Specific Domains | Scores * | % of Patients with Positive Answers ** |
|---|---|---|
| 1. Current treatment satisfaction | 4.46 ± 0.12 5 (2) | 79 |
| 2. Unacceptable high glucose | 3.23 ± 0.15 3.5 (3) | 50 |
| 3. Unacceptable low glucose | 1.02 ± 0.12 0 (2) | 8 |
| 4. Convenience | 4.72 ± 0.11 5 (2) | 84 |
| 5. Flexibility | 4.42 ± 0.13 5 (3) | 76.8 |
| 6. Understanding | 4.42 ± 0.12 5 (3) | 72.5 |
| 7. Willing to recommend | 2.85 ± 0.21 3 (6) | 45.7 |
| 8. Satisfaction to continue | 4.58 ± 0.13 5 (2) | 76 |
| Specific Life Domain | Impacting Rating | Importance Rating | Weighted Impact Score |
| Leisure activities | −1.86 ± 0.91 | 2.12 ± 0.64 | −2.60 ± 1.73 |
| Working life (34) * | −1.26 ± 0.95 | 1.91 ± 0.73 | −2.15 ± 1.85 |
| Local or long-distance journeys | −1.34 ± 0.94 | 2.20 ± 0.74 | −2.75 ± 2.08 |
| Holidays (18) * | −1.37 ± 0.91 | 2.24 ± 0.73 | −2.81 ± 1.81 |
| Physical health | −1.37 ± 0.83 | 2.01 ± 0.69 | −2.51 ± 1.55 |
| Family life (1) * | −1.36 ± 0.96 | 1.58 ± 0.63 | −2.01 ± 1.57 |
| Friendship and social life | −1.10 ± 0.97 | 2.03 ± 0.66 | −2.01 ± 1.83 |
| Personal relationship (14) * | −1.14 ± 1.01 | 1.74 ± 0.68 | −1.84 ± 1.69 |
| Sex life (25) * | −1.29 ± 0.97 | 2.12 ± 0.81 | −2.48 ± 2.04 |
| Physical appearance | −1.15 ± 0.98 | 2.03 ± 0.62 | −2.07 ± 1.68 |
| Self-confidence | −1.20 ± 0.93 | 1.72 ± 0.63 | −1.98 ± 1.65 |
| Motivation | −2.18 ± 1.82 | 2.00 ± 0.65 | −1.20 ± 0.99 |
| People’s reaction | −0.89 ± 1.00 | 2.33 ± 0.88 | −1.77 ± 2.16 |
| Feelings about feature | −1.33 ± 1.01 | 1.93 ± 0.70 | −2.24 ± 1.87 |
| Financial situation | −1.05 ± 1.04 | 1.96 ± 0.77 | −1.92 ± 2.12 |
| Living condition | −0.74 ± 1.04 | 1.91 ± 0.72 | −1.39 ± 2.33 |
| Dependence on others | −0.99 ± 1.03 | 1.98 ± 0.88 | −1.89 ± 2.10 |
| Freedom to eat | −1.62 ± 1.01 | 2.15 ± 0.80 | −3.07 ± 2.09 |
| Freedom to drink | −1.20 ± 1.06 | 2.49 ± 0.86 | −2.47 ± 2.22 |
| Characteristics | Total (N = 138) | SF-6Dv2 (Mean, 95% CI) | p Value |
|---|---|---|---|
| Age (years) * | 57.86 ± 8.82 | 0.591 (0.583–0.598) | 0.883 |
| <50 | 30 (21.7) | 0.591 (0.571–0.610) | |
| 50–64 | 77 (55.8) | 0.592 (0.582–0.602) | |
| ≥65 | 31 (22.5) | 0.587 (0.583–0.598) | |
| Gender, N (%) | 0.415 | ||
| Women | 70 (50.7) | 0.588 (0.577–0.598) | |
| Men | 68 (49.3) | 0.594 (0.582–0.605) | |
| Diabetes duration, years ** | 5 (8) | 0.249 | |
| <5 (N, %) | 63 (45.7) | 0.585 (0.574–0.596) | |
| 5–10 (N, %) | 39 (28.2) | 0.600 (0.584–0.616) | |
| ≥10 (N, %) | 36 (26.1) | 0.590 (0.577–0.603) | |
| BMI (kg/m2) * | 32.65 (5.50) | 0.94 | |
| <24.9 (N, %) | 6 (4.35) | 0.584 (0.557–0.612) | |
| 25–29.9 (N, %) | 41 (29.71) | 0.591 (0.575–0.606) | |
| ≥30 (N, %) | 91 (65.94) | 0.591 (0.582–0.600) | |
| HbA1c (%) ** | 7.8 (1.12) | 0.946 | |
| <7.5 (N, %) | 46 (33.3) | 0.589 (0.576–0.602) | |
| 7.5–8 (N, %) | 42 (30.4) | 0.591 (0.577–0.605) | |
| ≥8 (N, %) | 50 (36.3) | 0.592 (0.583–0.598) | |
| With Neuropathy, N (%) | 61 (44.2) | 0.592 (0.582–0.602) | 0.696 |
| Without Neuropathy N (%) | 77 (55.8) | 0.578 (0.578–0.600) | |
| With Hypertension, N (%) | 93 (67.4) | 0.591 (0.582–0.599) | 0.931 |
| Without Hypertension, N (%) | 45 (32.6) | 0.590 (0.575–0.605) | |
| With Dyslipidemia, N (%) | 99 (71.7) | 0.595 (0.586–0.604) | 0.064 |
| Without Dyslipidemia, N (%) | 39 (28.3) | 0.579 (0.565–0.594) | |
| DTSQ ** | 26 (10) | 0.346 | |
| ≤26, N (%) | 71 (51.4) | 0.587 (0.577–0.598) | |
| >26, N (%) | 67 (48.6) | 0.594 (0.583–0.605) | |
| ADDQoL ** | −2.21 (1.76) | 0.787 | |
| ≤−2.21, N (%) | 73 (52.9) | 0.592 (0.581–0.603) | |
| >−2.21, N (%) | 65 (47.1) | 0.590 (0.579–0.600) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grigorescu, E.-D.; Lăcătușu, C.-M.; Crețu, I.; Floria, M.; Onofriescu, A.; Ceasovschih, A.; Mihai, B.-M.; Șorodoc, L. Self-Reported Satisfaction to Treatment, Quality of Life and General Health of Type 2 Diabetes Patients with Inadequate Glycemic Control from North-Eastern Romania. Int. J. Environ. Res. Public Health 2021, 18, 3249. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063249
Grigorescu E-D, Lăcătușu C-M, Crețu I, Floria M, Onofriescu A, Ceasovschih A, Mihai B-M, Șorodoc L. Self-Reported Satisfaction to Treatment, Quality of Life and General Health of Type 2 Diabetes Patients with Inadequate Glycemic Control from North-Eastern Romania. International Journal of Environmental Research and Public Health. 2021; 18(6):3249. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063249
Chicago/Turabian StyleGrigorescu, Elena-Daniela, Cristina-Mihaela Lăcătușu, Ioana Crețu, Mariana Floria, Alina Onofriescu, Alexandr Ceasovschih, Bogdan-Mircea Mihai, and Laurențiu Șorodoc. 2021. "Self-Reported Satisfaction to Treatment, Quality of Life and General Health of Type 2 Diabetes Patients with Inadequate Glycemic Control from North-Eastern Romania" International Journal of Environmental Research and Public Health 18, no. 6: 3249. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063249