
Trends in Healthcare Access in Japan during the First Wave of the COVID-19 Pandemic, up to June 2020

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miller, I.F.; Becker, A.D.; Grenfell, B.T.; Metcalf, C.J.E. Disease and healthcare burden of COVID-19 in the United States. Nat. Med. 2020, 26, 1212–1217. [Google Scholar] [CrossRef]
- Mori, M.; Ikeda, N.; Taketomi, A.; Asahi, Y.; Takesue, Y.; Orimo, T.; Ono, M.; Kuwayama, T.; Nakamura, S.; Yamada, Y.; et al. COVID-19: Clinical issues from the Japan Surgical Society. Surg. Today 2020, 50, 794–808. [Google Scholar] [CrossRef]
- O’Dowd, A. Covid-19 pandemic is magnifying healthcare inequalities, says England’s regulator. BMJ 2020, 371, m4035. [Google Scholar] [CrossRef]
- Germain, S.; Yong, A. COVID-19 highlighting inequalities in access to healthcare in England: A case study of ethnic minority and migrant women. Fem. Leg. Stud. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Okereke, M.; Ukor, N.A.; Adebisi, Y.A.; Ogunkola, I.O.; Favour Iyagbaye, E.; Adiela Owhor, G.; Lucero-Prisno, D.E., 3rd. Impact of COVID-19 on access to healthcare in low- and middle-income countries: Current evidence and future recommendations. Int. J. Health Plan. Manag. 2020. [Google Scholar] [CrossRef]
- Desai, S.M.; Guyette, F.X.; Martin-Gill, C.; Jadhav, A.P. Collateral damage—Impact of a pandemic on stroke emergency services. J. Stroke Cerebrovasc. Dis. 2020, 29, 104988. [Google Scholar] [CrossRef]
- Rosenbaum, L. The untold toll—The pandemic’s effects on patients without Covid-19. N. Engl. J. Med. 2020, 382, 2368–2371. [Google Scholar] [CrossRef]
- GOV.UK. Direct and Indirect Impacts of COVID-19 on Excess Deaths and Morbidity, 15 July 2020. Available online: https://www.gov.uk/government/publications/dhsconsgadho-direct-and-indirect-impacts-of-covid-19-on-excess-deaths-and-morbidity-15-july-2020 (accessed on 9 March 2021).
- Woolf, S.H.; Chapman, D.A.; Sabo, R.T.; Weinberger, D.M.; Hill, L. Excess Deaths From COVID-19 and Other Causes, March-April 2020. JAMA 2020, 324, 510–513. [Google Scholar] [CrossRef]
- Woolf, S.H.; Chapman, D.A.; Sabo, R.T.; Weinberger, D.M.; Hill, L.; Taylor, D.D.H. Excess deaths from COVID-19 and other causes, March–July 2020. JAMA 2020, 324, 1562–1564. [Google Scholar] [CrossRef]
- Czeisler, M.E.; Marynak, K.; Clarke, K.E.N.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D.; et al. Delay or avoidance of medical care because of COVID-19-related concerns—United States, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef]
- National Institute of Infectious Diseases. Estimation of Excess Deaths in Japan [Japanese]. 2020. Available online: https://www.niid.go.jp/niid/ja/from-idsc/493-guidelines/9945-excess-mortality-20oct.html (accessed on 9 March 2021).
- Kaufman, H.W.; Chen, Z.; Niles, J.; Fesko, Y. Changes in the Number of US Patients with Newly Identified Cancer before and during the Coronavirus Disease 2019 (COVID-19) Pandemic. JAMA Netw. Open 2020, 3, e2017267. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef]
- Ministry of Health, Labor and Welfare. Medical Facility Surveys and Hospital Reports. Available online: https://www.mhlw.go.jp/toukei/list/79-1a.html (accessed on 9 March 2021).
- Roy, S.; Ghosh, P. Factors affecting COVID-19 infected and death rates inform lockdown-related policymaking. PLoS ONE 2020, 15, e0241165. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Khalse, M. Epidemiological determinants of COVID-19-related patient outcomes in different countries and plan of action: A retrospective analysis. Cureus 2020, 12, e8440. [Google Scholar] [CrossRef] [PubMed]
- Garcia, S.; Albaghdadi, M.S.; Meraj, P.M.; Schmidt, C.; Garberich, R.; Jaffer, F.A.; Dixon, S.; Rade, J.J.; Tannenbaum, M.; Chambers, J.; et al. Reduction in ST-segment elevation cardiac catheterization laboratory activations in the United States during COVID-19 pandemic. J. Am. Coll. Cardiol. 2020, 75, 2871–2872. [Google Scholar] [CrossRef]
- Bernstein, L.; Sellers, F.S. Patients with Heart Attacks, Strokes and Even Appendicitis Vanish from Hospitals. 2020. Available online: https://www.washingtonpost.com/health/patients-with-heart-attacks-strokes-and-even-appendicitis-vanish-from-hospitals/2020/04/19/9ca3ef24-7eb4-11ea-9040-68981f488eed_story.html (accessed on 9 March 2021).
- Ogiwara, K. Coronavirus Disease (COVID-19) Situation Report in Japan. 2020. Available online: https://toyokeizai.net/sp/visual/tko/covid19/en.html (accessed on 9 March 2021).
- Tokyo Shimbun. The Number of Home Care Service Users Decreased by 100,000 [Japanese]. 2020. Available online: https://www.tokyo-np.co.jp/article/54461 (accessed on 9 March 2021).
- World Health Organization. Gender and COVID-19; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Nomura, S.; Kawashima, T.; Yoneoka, D.; Tanoue, Y.; Eguchi, A.; Gilmour, S.; Kawamura, Y.; Harada, N.; Hashizume, M. Trends in suicide in Japan by gender during the COVID-19 pandemic, up to September 2020. Psychiatry Res. 2020, 295, 113622. [Google Scholar] [CrossRef] [PubMed]
- Nikkei Medical. 46.5% of Hospitals Saw a Decrease in Patient Volume; Some Departments Saw a 60% Drop in Patient Volume [Japanese]. 2020. Available online: https://medical.nikkeibp.co.jp/leaf/all/report/t344/202007/566334.html (accessed on 9 March 2021).
- Russo, V.; Cassini, R.; Caso, V.; Donno, C.; Laezza, A.; Naddei, M.; Fiorelli, A.; Golino, P.; Nigro, G. Nursing Teleconsultation for the Outpatient Management of Patients with Cardiovascular Disease during COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2087. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Rapacciuolo, A.; Pafundi, P.C.; de Divitiis, M.; Volpicelli, M.; Ruocco, A.; Rago, A.; Uran, C.; Nappi, F.; Attena, E.; et al. Cardiac implantable electronic devices replacements in patients followed by remote monitoring during COVID-19 lockdown. Eur. Heart J. 2021. [Google Scholar] [CrossRef]
- Russo, V.; Pafundi, P.C.; Rapacciuolo, A.; de Divitiis, M.; Volpicelli, M.; Ruocco, A.; Rago, A.; Uran, C.; Nappi, F.; Attena, E.; et al. Cardiac pacing procedures during coronavirus disease 2019 lockdown in Southern Italy: Insights from Campania Region. J. Cardiovasc. Med. 2021. (Publish Ahead of Print). [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhou, L.; Yang, Y.; Peng, W.; Wang, W.; Chen, X. Therapeutic and triage strategies for 2019 novel coronavirus disease in fever clinics. Lancet Respir. Med. 2020, 8, e11–e12. [Google Scholar] [CrossRef] [Green Version]
- Japan Hospital Association; All Japan Hospital Association; Association of Japanese Healthcare Corporations. Survey of Hospital Management after the Spread of COVID-19 [Japanese]. 2020. Available online: https://www.hospital.or.jp/pdf/06_20200806_01.pdf (accessed on 9 March 2021).




{kind=link}
{kind=link}
{kind=link}
| Observed | Excess | Percent Excess | Exiguous | Percent Deficit | |||
|---|---|---|---|---|---|---|---|
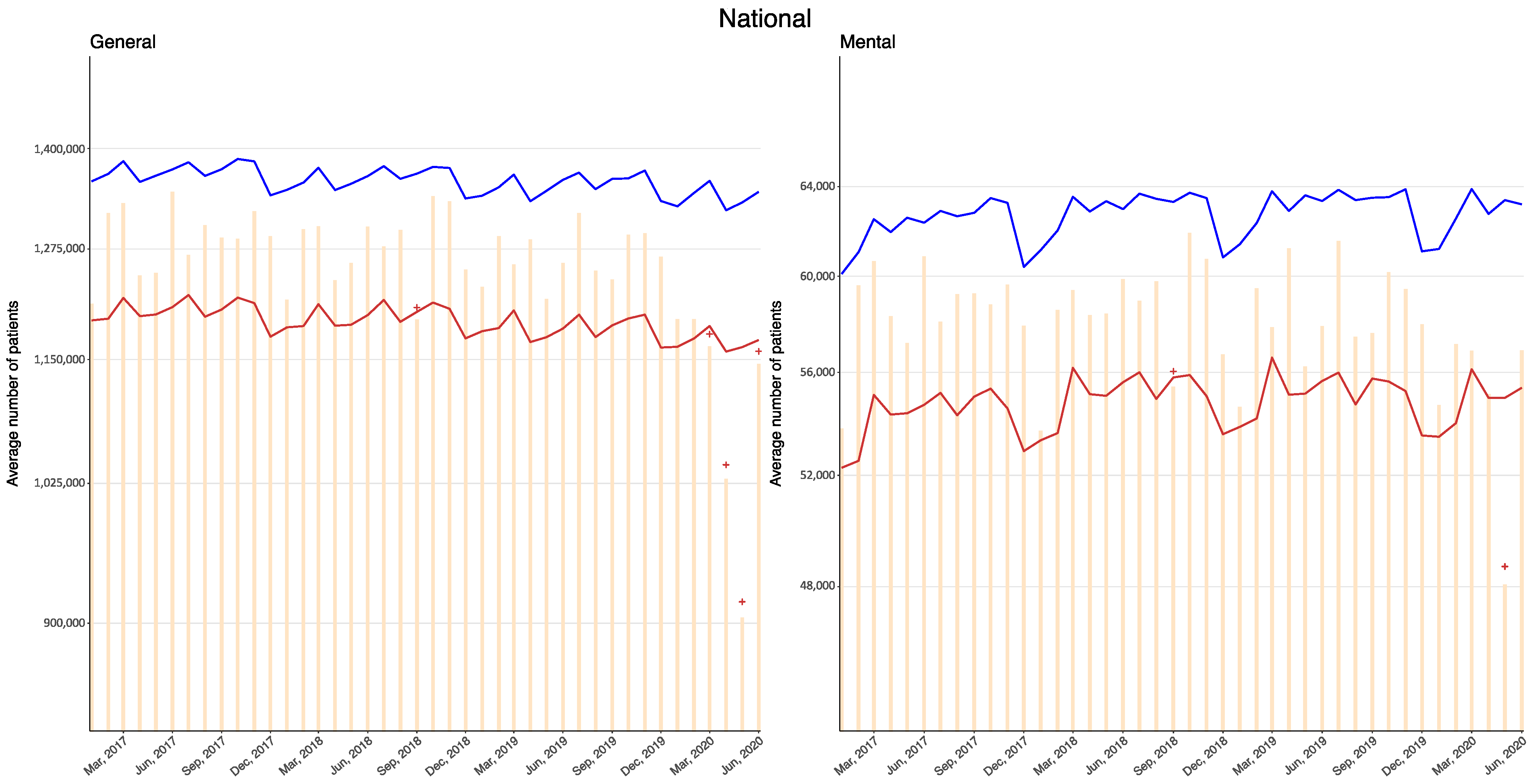
| (1) Average number of outpatients per day at hospitals | |||||||
| General hospitals | |||||||
| January | 1,194,286 | 0–0 | 0.00–0.00 | 0–49,539 | 0.00–3.98 | ||
| February | 1,194,077 | 0–0 | 0.00–0.00 | 0–62,457 | 0.00–4.97 | ||
| March | 1,164,224 | 0–0 | 0.00–0.00 | 22,448–106,788 | 1.77–8.40 | ** | |
| April | 1,029,399 | 0–0 | 0.00–0.00 | 129,350–209,486 | 10.44–16.91 | ** | |
| May | 904,647 | 0–0 | 0.00–0.00 | 259,029–341,330 | 20.79–27.39 | ** | |
| June | 1,145,535 | 0–0 | 0.00–0.00 | 25,704–110,787 | 2.05–8.82 | ** | |
| Psychiatric hospitals | |||||||
| January | 54,687 | 0–0 | 0.00–0.00 | 0–2566 | 0.00–4.48 | ||
| February | 57,140 | 0–0 | 0.00–0.00 | 0–1038 | 0.00–1.78 | ||
| March | 568,70 | 0–0 | 0.00–0.00 | 0–3063 | 0.00–5.11 | ||
| April | 55,129 | 0–0 | 0.00–0.00 | 0–3669 | 0.00–6.24 | ||
| May | 48,083 | 0–0 | 0.00–0.00 | 6898–11,014 | 11.67–18.64 | ** | |
| June | 56,883 | 0–0 | 0.00–0.00 | 0–2329 | 0.00–3.93 | ||
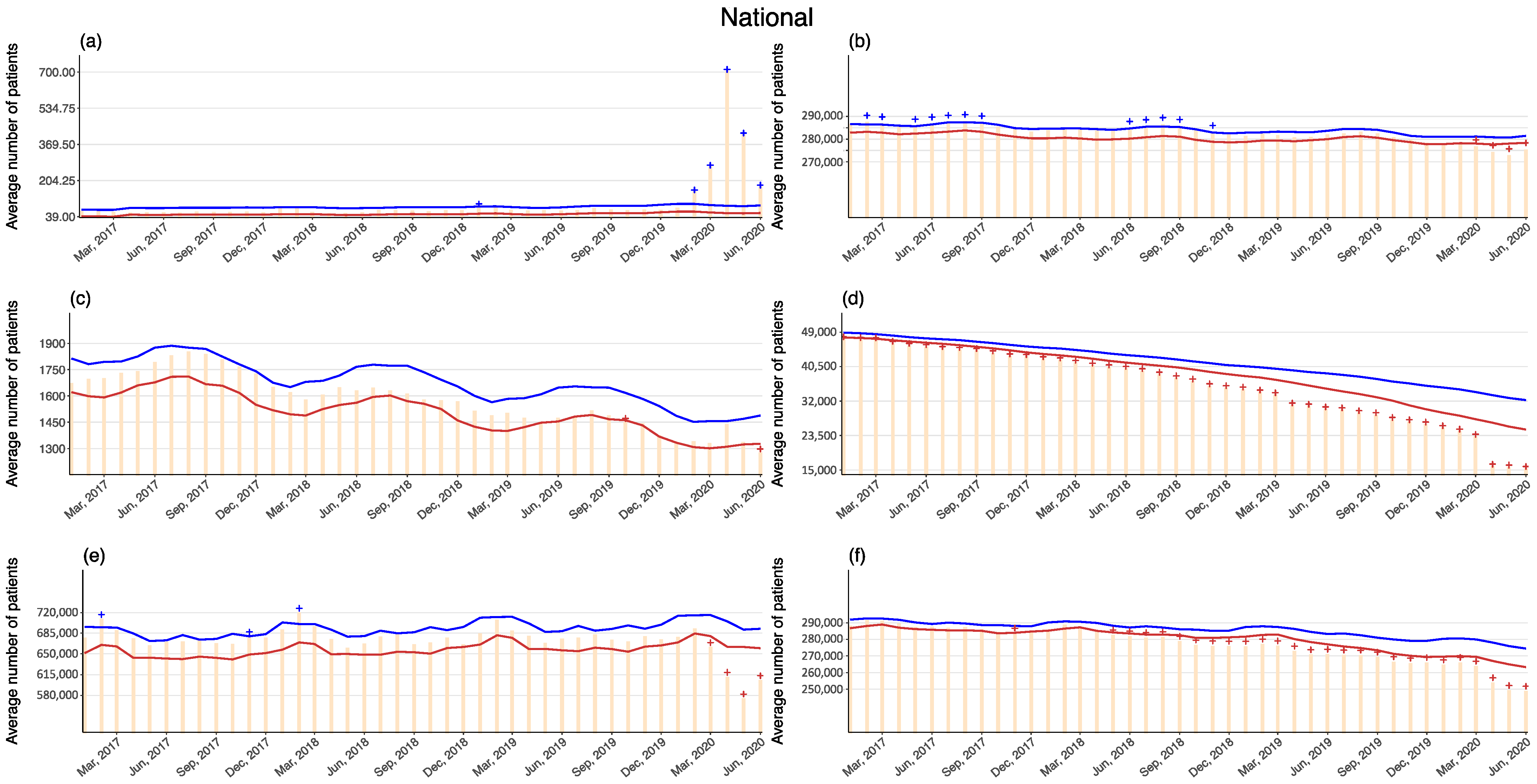
| (2) Average number of hospitalized patients per day | |||||||
| (a) Infectious disease care beds | |||||||
| January | 79 | 0–1 | 0.00–1.05 | 0–0 | 0.00–0.00 | ||
| February | 154 | 57–76 | 72.47–95.79 | 0–0 | 0.00–0.00 | * | |
| March | 267 | 175–193 | 235.58–259.42 | 0–0 | 0.00–0.00 | * | |
| April | 705 | 617–635 | 878.74–904.07 | 0–0 | 0.00–0.00 | * | |
| May | 414 | 327–345 | 471.57–497.04 | 0–0 | 0.00–0.00 | * | |
| June | 176 | 86–104 | 119.36–144.28 | 0–0 | 0.00–0.00 | * | |
| (b) Psychiatric care beds | |||||||
| January | 278,200 | 0–0 | 0.00–0.00 | 0–1217 | 0.00–0.44 | ||
| February | 278,345 | 0–0 | 0.00–0.00 | 0–1266 | 0.00–0.45 | ||
| March | 276,793 | 0–0 | 0.00–0.00 | 1225–2714 | 0.44–0.97 | ** | |
| April | 274,334 | 0–0 | 0.00–0.00 | 3362–4942 | 1.20–1.77 | ** | |
| May | 272,879 | 0–0 | 0.00–0.00 | 5182–6477 | 1.85–2.32 | ** | |
| June | 275,436 | 0–0 | 0.00–0.00 | 2871–4413 | 1.03–1.58 | ** | |
| (c) Tuberculosis care beds | |||||||
| January | 1336 | 0–0 | 0.00–0.00 | 0–74 | 0.00–5.20 | ||
| February | 1343 | 0–0 | 0.00–0.00 | 0–37 | 0.00–2.63 | ||
| March | 1333 | 0–0 | 0.00–0.00 | 0–45 | 0.00–3.21 | ||
| April | 1439 | 0–57 | 0.00–4.06 | 0–0 | 0.00–0.00 | ||
| May | 1338 | 0–0 | 0.00–0.00 | 0–58 | 0.00–4.10 | ||
| June | 1279 | 0–0 | 0.00–0.00 | 52–127 | 3.70–8.98 | ** | |
| (d) Nursing care beds | |||||||
| January | 264,611 | 0–0 | 0.00–0.00 | 5661–10,702 | 2.06–3.89 | ** | |
| February | 266,089 | 0–0 | 0.00–0.00 | 3792–9073 | 1.38–3.30 | ** | |
| March | 263,790 | 0–0 | 0.00–0.00 | 5558–10,790 | 2.02–3.93 | ** | |
| April | 254,053 | 0–0 | 0.00–0.00 | 12,761–18,318 | 4.69–6.73 | ** | |
| May | 249,345 | 0–0 | 0.00–0.00 | 15,497–20,979 | 5.73–7.76 | ** | |
| June | 248,918 | 0–0 | 0.00–0.00 | 14,258–19,865 | 5.30–7.39 | ** | |
| (e) General beds | |||||||
| January | 678,772 | 0–0 | 0.00–0.00 | 0–12,995 | 0.00–1.88 | ||
| February | 693,259 | 0–0 | 0.00–0.00 | 0–6517 | 0.00–0.93 | ||
| March | 661,980 | 0–0 | 0.00–0.00 | 18,248–35,869 | 2.61–5.14 | ** | |
| April | 611,787 | 0–0 | 0.00–0.00 | 50,126–71,440 | 7.34–10.46 | ** | |
| May | 575,307 | 0–0 | 0.00–0.00 | 86,236–100,975 | 12.75–14.93 | ** | |
| June | 606,442 | 0–0 | 0.00–0.00 | 53,019–69,453 | 7.84–10.28 | ** | |
| (f) Long-term care beds | |||||||
| January | 25,464 | 0–0 | 0.00–0.00 | 5162–7489 | 15.67–22.72 | ** | |
| February | 24,606 | 0–0 | 0.00–0.00 | 4223–7188 | 13.28–22.61 | ** | |
| March | 23,329 | 0–0 | 0.00–0.00 | 4595–7672 | 14.82–24.75 | ** | |
| April | 15,976 | 0–0 | 0.00–0.00 | 10,673–13,989 | 35.62–46.68 | ** | |
| May | 15,762 | 0–0 | 0.00–0.00 | 9967–13,379 | 34.20–45.91 | ** | |
| June | 15,398 | 0–0 | 0.00–0.00 | 9583–13,088 | 33.64–45.94 | ** | |
| (3) Average length of hospital stays per patient | |||||||
| (b) Psychiatric care beds | |||||||
| January | 283 | 0–11 | 0.00–4.03 | 0–0 | 0.00–0.00 | ||
| February | 267 | 0–1 | 0.00–0.01 | 0–0 | 0.00–0.00 | ||
| March | 272 | 0–13 | 0.00–4.95 | 0–0 | 0.00–0.00 | ||
| April | 294 | 3–35 | 0.85–13.45 | 0–0 | 0.00–0.00 | * | |
| May | 317 | 28–60 | 10.71–23.24 | 0–0 | 0.00–0.00 | * | |
| June | 265 | 0–11 | 0.00–4.03 | 0–0 | 0.00–0.00 | ||
| (c) Tuberculosis care beds | |||||||
| January | 68 | 0–5 | 0.00–6.36 | 0–0 | 0.00–0.00 | ||
| February | 59 | 0–0 | 0.00–0.00 | 0–5 | 0.00–7.61 | ||
| March | 51 | 0–0 | 0.00–0.00 | 0–12 | 0.00–17.86 | ||
| April | 38 | 0–0 | 0.00–0.00 | 12–27 | 18.13–40.64 | ** | |
| May | 51 | 0–0 | 0.00–0.00 | 0–14 | 0.00–21.16 | ||
| June | 50 | 0–0 | 0.00–0.00 | 1–16 | 0.15–23.23 | ** | |
| (d) Long-term care beds | |||||||
| January | 139 | 0–8 | 0.00–5.40 | 0–0 | 0.00–0.00 | ||
| February | 133 | 0–3 | 0.00–1.69 | 0–0 | 0.00–0.00 | ||
| March | 132 | 0–5 | 0.00–3.51 | 0–0 | 0.00–0.00 | ||
| April | 135 | 0–4 | 0.00–2.89 | 0–0 | 0.00–0.00 | ||
| May | 153 | 0–21 | 0.00–15.82 | 0–0 | 0.00–0.00 | ||
| June | 135 | 0–2 | 0.00–1.47 | 0–0 | 0.00–0.00 | ||
| (e) General beds | |||||||
| January | 17 | 0–1 | 0.00–3.01 | 0–0 | 0.00–0.00 | ||
| February | 17 | 0–1 | 0.00–0.64 | 0–0 | 0.00–0.00 | ||
| March | 16 | 0–1 | 0.00–2.00 | 0–0 | 0.00–0.00 | ||
| April | 17 | 0–2 | 0.00–6.52 | 0–0 | 0.00–0.00 | ||
| May | 19 | 0–3 | 0.00–18.15 | 0–0 | 0.00–0.00 | ||
| June | 16 | 0–1 | 0.00–2.76 | 0–0 | 0.00–0.00 | ||
| (f) LTCI care beds | |||||||
| January | 333 | 0–27 | 0.00–8.59 | 0–0 | 0.00–0.00 | ||
| February | 325 | 0–24 | 0.00–7.78 | 0–0 | 0.00–0.00 | ||
| March | 209 | 0–0 | 0.00–0.00 | 50–82 | 17.03–28.08 | ** | |
| April | 206 | 0–0 | 0.00–0.00 | 58–91 | 19.49–30.61 | ** | |
| May | 375 | 36–72 | 11.76–23.39 | 0–0 | 0.00–0.00 | * | |
| June | 305 | 0–0 | 0.00–0.00 | 0–9 | 0.00–2.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makiyama, K.; Kawashima, T.; Nomura, S.; Eguchi, A.; Yoneoka, D.; Tanoue, Y.; Kawamura, Y.; Sakamoto, H.; Gilmour, S.; Shi, S.; et al. Trends in Healthcare Access in Japan during the First Wave of the COVID-19 Pandemic, up to June 2020. Int. J. Environ. Res. Public Health 2021, 18, 3271. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063271
Makiyama K, Kawashima T, Nomura S, Eguchi A, Yoneoka D, Tanoue Y, Kawamura Y, Sakamoto H, Gilmour S, Shi S, et al. Trends in Healthcare Access in Japan during the First Wave of the COVID-19 Pandemic, up to June 2020. International Journal of Environmental Research and Public Health. 2021; 18(6):3271. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063271
Chicago/Turabian StyleMakiyama, Koji, Takayuki Kawashima, Shuhei Nomura, Akifumi Eguchi, Daisuke Yoneoka, Yuta Tanoue, Yumi Kawamura, Haruka Sakamoto, Stuart Gilmour, Shoi Shi, and et al. 2021. "Trends in Healthcare Access in Japan during the First Wave of the COVID-19 Pandemic, up to June 2020" International Journal of Environmental Research and Public Health 18, no. 6: 3271. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063271